
Abstract
Background
Laparoscopic ventral hernia repair may be an alternative to open mesh repair as it avoids a large abdominal incision, and thus potentially reduces pain and hospital stay. This review aimed to assess the safety and efficacy of laparoscopic ventral hernia repair in comparison with open ventral hernia repair.
Method
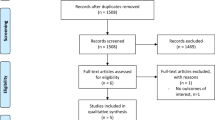
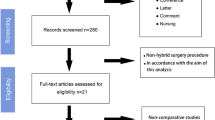
A systematic review was conducted, with comprehensive searches identifying six randomised controlled trials (RCTs) and eight nonrandomised comparative studies.
Results
The laparoscopic approach may have a lower recurrence rate than the open approach and required a shorter hospital stay. Five RCTs (Barbaros et al., Hernia 11:51–56, 2007; Misra et al., Surg Endosc 20:1839–1845, 2006; Navarra et al., Surg Laparosc Endosc Percutan Tech 17:86–90, 2007; Moreno-Egea et al., Arch Surg 137:266–1268, 2002; Carbajo et al., Surg Endosc 13:250–252, 1999) reported no conversion (0%) to open surgery, and four nonrandomised studies reported conversions to open surgery ranging from 0% to 14%. Open approach complications generally were wound related, whereas the laparoscopic approach reported both wound- and procedure-related complications and these appeared to be less frequently reported.
Conclusion
Based on current evidence, the relative safety and efficacy of the laparoscopic approach in comparison with the open approach remains uncertain. The laparoscopic approach may be more suitable for straightforward hernias, with open repair reserved for the more complex hernias. Laparoscopic ventral hernia repair appears to be an acceptable alternative that can be offered by surgeons proficient in advanced laparoscopic techniques.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Ventral hernias are the second most common type of abdominal hernias, after inguinal hernias [1], and account for approximately 10% of all hernias [2]. Ventral hernia, also known as abdominal wall hernia or incisional hernia, is defined as protrusion of a portion of an organ or tissue through the abdominal wall [3]. The inner lining of the abdomen pushes through the abdominal wall that has been weakened due to either a congenital defect or previous surgical incision (e.g. alimentary surgery, vascular surgery, genital tract surgery, or laparoscopy). The resulting balloon-like sac may trap or incarcerate a loop of intestine or other abdominal contents, which could cause potentially serious problems requiring emergency surgery [4].
Ventral hernias are an important long-term morbidity of conventional surgery [5, 6] as they usually develop within 5 years after laparotomy. Risk factors for incisional ventral hernia include wound infection, abdominal distension, pulmonary complications, male sex, age, obesity, emergency procedures, early reoperation, jaundice, underlying disease process, type of closure, suture material used in closure and choice of original incision [7]. They may also result from too much tension with the initial closure of the abdominal incision, which creates poor healing, swelling and wound separation [8]. Hernia sizes vary from very small to very large and complex. A hernia left untreated may enlarge with time and become progressively symptomatic. Surgery is the preferred treatment [5] with a choice of two methods: open repair (with sutures or mesh) and laparoscopic mesh repair.
Laparoscopic ventral hernia repair (LVHR) was first introduced in 1993 by LeBlanc and Booth [9]. After pneumoperitoneum is established for exploration of the abdomen, at least three trocars are placed as far laterally as possible from the hernia defect. The number of trocars required and the placement of ports will depend on the size and location of the hernia. Intra-abdominal adhesions are broken down with sharp and blunt dissection and the hernia sac can be reduced, if necessary. Mesh is cut to overlap the defect by approximately 3–5 cm, and is then inserted through a trocar site and fixed to the abdominal wall. The mesh is usually placed intraperitoneally and a range of mesh and suture combinations have been used. Full-thickness mattress sutures (2-0 or 0) spaced at 4–5-cm intervals around the circumference of the mesh are usually used to anchor the mesh and hold it in place [10]. Spiral tacks or staples are then placed in between the mattress sutures at 1-cm intervals to secure the mesh [10].
The open approach is the standard technique for repair of ventral hernias. However, the rate of hernia recurrence is high, especially if the hernia defect has been repaired with sutures. The laparoscopic repair of ventral hernias is an emerging technique that has been applied with potential to replace open repair. Recurrence rates have been reported to be similar to open repair with mesh but with shorter hospital stay [5] as it does not require the wide dissection area or routinely require the subcutaneous drains which accompany open repair [11]. A summary of the evidence of the efficacy, safety and cost-effectiveness of laparoscopic repair compared with open repair is lacking. It is unclear whether one technique may be more appropriate for a particular type of hernia and if the severity and types of complications differ for each technique. The efficacy and safety of laparoscopic ventral hernia repair in comparison with open ventral hernia repair needs to be considered, as do costs and resource use.
The aim of this review was to assess the safety and efficacy of laparoscopic surgery in comparison to open surgery for the treatment of ventral hernia repair, through a systematic review of the literature.
Materials and methods
Search strategy
A systematic search of MEDLINE, EMBASE, Current Contents, PubMed and the Cochrane Library (Issue 3, 2005) was conducted, from the inception of the databases until July 2005. The York (UK) Centre for Reviews and Dissemination databases, relevant online journals and the Internet were searched in July 2005. In addition Clinicaltrials.gov and the National Research Register were searched for ongoing trials in this area, and located a number of trials which have been included as Appendix 1. Updated searches were performed in October 2007 to include any new RCTs. Searches were conducted without language restriction. The search terms were “laparoscopic ventral hernia repair” or “LVHR”, “laparoscopy” and “hernia, ventral laparosco*” and “(ventral hernia or incisional hernia or abdominal wall hernia)”, where the asterisk is a truncation symbol in several databases and retrieves terms with a common word stem, e.g. “laparoscope”, “laparoscopy”, “laparoscopic”, and “laparoscopies”.
Inclusion criteria
Articles were obtained on the basis of the abstract containing safety and efficacy data on the laparoscopic approach to ventral hernia repair in the form of RCTs and other controlled or comparative studies. Conference abstracts and manufacturer’s information were included if they contained relevant safety and efficacy data. The English-language abstracts from foreign-language articles were also included if they met the study inclusion criteria and contained safety and efficacy data. In the case of duplicate publications, the latest and most complete study was included.
Data extraction and analysis
Data were extracted by one researcher and checked by a second using standardised data extraction tables developed a priori. Included studies were assigned a level of evidence according to the hierarchy of evidence table developed by the National Health and Medical Research Council of Australia [12], and examined for design or execution factors that may have introduced bias. Assessment of study quality considered a number of factors, including quality of the reporting of study methodology, methods of randomisation and allocation concealment (for RCTs), any blinding of patients or outcome assessors; and attempts made to minimise bias.
Results
Description of studies and critical appraisal
A total of 14 studies met the inclusion criteria: six RCTs (level II) and eight nonrandomised comparative studies (six level III-2 and two level III-3). Table 1 provides a descriptive summary of the included studies.
There was a relative homogeneity to the patient pool, as the included studies had similar inclusion and exclusion criteria for patient recruitment. The patient pool typically included those with a diagnosis of ventral hernia (primary and incisional) with a minimum and maximum defect size, who were eligible for an open or laparoscopic surgical procedure. Excluded patients were those with a need for emergency surgery, a high risk for general anaesthesia or whose hernia repair was performed concurrently with another surgical procedure.
One RCT reported significant differences in patient sex and hernia type [11], whilst the comparative studies reported significant differences in patient age and defect size [13], proportion of patients with recurrent ventral hernias [6], and hernia size [14]. None of the other studies reported statistically significant differences between patient characteristics for the laparoscopic and open repair groups. Possible confounding factors identified in the studies included the number of previous ventral hernia repairs, fixation technique (sutures, staples or tacks) and location and aetiology of the hernias. Misra et al. [15] noted that, for the majority of patients in both groups, ventral hernia followed lower abdominal gynaecologic operation.
Comorbidities were reported in four RCTs. Misra et al. [15] included some patients with a higher body mass index (BMI) and chronic obstructive pulmonary disease, although numbers were not reported. Olmi et al. [16] reported one patient with coeliac disease, and Barbaros et al. [11] reported one patient who had prosthetic heart valves. Navarra et al. [17] reported on two patients who had additional multiple small defects that were discovered intraoperatively; however, these were not described.
Four RCTs described their randomisation process: by computerised program [11, 17, 18] and by random numbers derived from the website www.randomization.com [15]. Two of these RCTs stated the method of allocation concealment: numbers in sequential order were kept in sealed envelopes which were opened only in theatre before surgery after the patient had already been enrolled [17] and slips were kept in sealed envelopes which were picked at random after patient’s consent had been received, then opened to reveal the type of repair [15]. Blinding of investigators, outcome assessors or patients was not possible due to the nature of surgery. Follow-up times ranged from 2 to 55 months. Nine patients in the Misra et al. [15] study were lost to follow-up, comprising five patients from the open repair group and four patients from the laparoscopic repair group. The final number of patients assessed by Misra et al. was unclear. Thirty-three patients were originally randomised to each group, then five open and four laparoscopic repair patients were reported as lost to follow-up. However, postoperative complications were reported for group sizes of 30 (open) and 32 (laparoscopic). There were no other reported losses to follow-up in the included studies.
Methods for patient allocation in the nonrandomised comparative studies varied. In three studies patient allocation was based on surgeon preference [1, 6, 19]. Methods of patient allocation in Robbins et al. [20], Holzman et al. [13] and Zanghi et al. [14] may have introduced selection bias, which is likely to have favoured the laparoscopic method, since patient comorbidities and hernia anatomy were the basis of patient allocation in these studies. DeMaria et al. [6] intentionally allocated patients with more complex hernias to receive laparoscopic repair. Chari et al. [21] matched patients in the laparoscopic group to patients in the open group, allowing comparisons to be made between patients with similar characteristics. However, due to the retrospective study design, there was potential for error and bias in the collection and interpretation of information. Park et al. [22] and Zanghi et al. [14] used historical controls, so valid comparisons could not be made between the laparoscopic and open groups in these studies due to differences in the duration of follow-up. Two of the studies reported small to moderate losses to follow-up [13, 14], but the remaining eight studies appeared to have retained all patients.
Efficacy of laparoscopic repair compared with open repair
Rate of hernia recurrence
RCTs
Four RCTs reported on hernia recurrence [11, 15, 16, 23]. Two RCTs reported hernia recurrence in the laparoscopic repair group: Olmi et al. [16] reported 2.3% (2/85) 1 and 3 months after surgery, and Misra et al. [15] reported 6.3% (2/32) with mean follow-up of 13.7 months.
For open repair, one RCT [23] reported hernia recurrence in 7% (2/30) of patients at mean follow-up of 27 months, whilst another RCT [11] reported recurrence in 4% (1/23) of patients at mean follow-up of 20 months. All three patients required reoperation (Table 2). The third RCT [16] reported hernia recurrence in 1.1% (1/85) of open repair patients 1 month after surgery and Misra et al. [15] reported hernia recurrence in 3.3% (1/30) of open repair patients with mean follow-up of 13 months; however, reoperation for these patients was not reported.
Nonrandomised comparative studies
Three of the six nonrandomised comparative studies with concurrent controls [1, 6, 13] reported hernia recurrence with at least 2 years mean follow-up. Lower recurrence rate was reported in the laparoscopic group in two of the three studies [1, 13]. DeMaria et al. [6] reported a lower recurrence rate in the open group. In the two comparative studies with historical controls, 13% recurrence rate after mean follow-up of 24 months in the laparoscopic group and 61% recurrence rate in the open group after mean follow-up of 53 months was reported in one study [22], and no recurrences after mean follow-up of 18 months for the laparoscopic group and mean follow-up of 40 months for the open group was reported in the second (Table 2) [14].
Reasons for recurrences were not reported in any of the studies. However, hernia recurrences in two of the patients undergoing the open procedure in Ramshaw et al. [1] later turned out to be missed hernias from the original operation.
Length of hospital stay
RCTs
In all six RCTs hospital stay was significantly shorter for patients in the laparoscopic group (Table 3) [11, 15–18, 23].
Nonrandomised comparative studies
No significant difference between the two groups for hospital stay was reported in the six nonrandomised comparative studies [1, 6, 14, 19, 21, 22]. However, the variability in the duration of hospital stay for the laparoscopic and open groups resulted in wide ranges, which may have been due to some patients requiring aspiration drains, thus prolonging their stay in hospital (Table 3).
Operating time
RCTs
Operating time was significantly shorter for the laparoscopic approach in three RCTs [11, 16, 23], however Moreno-Egea et al. [18] reported similar operating times for laparoscopic and open approaches. Neither Navarra et al. [17] nor Misra et al. [15] found a significant difference in mean operating time (Table 4).
Nonrandomised comparative studies
The ranges in operating time reported from six of the nonrandomised comparative studies [1, 13, 14, 19, 21, 22] were similar for both groups (Table 4). However, the operating time for the laparoscopic approach appeared to be longer.
Conversions to open
RCTs
Five RCTs [11, 15, 17, 18, 23] reported no conversions from laparoscopic to open surgery and the remaining RCT [16] did not report on conversion (Table 5).
Nonrandomised comparative studies
Conversion rates were reported in four nonrandomised comparative studies and ranged from 0% to 14% (median 5%) (Table 5) [13, 14, 19, 20]. Reasons for conversion included enterotomy, obesity (which resulted in the inability to reduce the hernia contents), multiple defects, severe adhesions and abscess.
Safety of laparoscopic repair compared with open repair: complications
More complications were reported for open repair patients than for laparoscopic repair patients in four of the six RCTs (Table 6) [15, 16, 18, 23]. Moreno-Egea et al. [18] reported no complications for laparoscopic patients, while 18% (2 of 11) of open repair patients required aspiration drains and 36% (4 of 11) had postoperative haematomas. In Carbajo et al. [23], 3% (1/30) of laparoscopic patients had postoperative incarceration requiring reoperation and 13% (4/30) had mild seroma, while 7% (2/30) of open patients had accidental intestinal perforations during surgery, 50% (15/30) had mild seroma, 17% (5/30) had massive seroma, 10% (3/30) had abscess (one patient requiring reoperation), 10% (3/30) had mild haematoma, 10% (3/30) had moderate haematoma and 3% (1/30) had intestinal occlusion requiring reintervention.
Olmi et al. [16] reported complications in 16.4% of laparoscopic repair patients and in 29.4% of open repair patients. In the laparoscopic repair group 19% (6/85) of patients developed persistent seroma longer than 4–6 weeks and 1.2% (1/85) developed seroma infection 1 month after surgery, requiring laparoscopic removal of the mesh and suture of the abdominal wall. Seven months later this patient developed a small bowel obstruction due to adhesions, requiring a further laparoscopic procedure. Five percent (4/85) of patients developed neuralgia thought to be due to tack placement and, of these, two had tacks removed laparoscopically. One patient who developed faecal obstruction was treated by water enema. In the open repair group 20 patients had minor complications: six wound infections, one seroma, two persistent serous secretions, one faecal obstruction, two cases of occlusion (which occurred 6 and 12 months after operation and were treated conservatively) and eight cases of neuralgia. Four patients had major complications: one severe wound infection (leading to sepsis), one caval thrombosis (requiring a caval filter placement and 103 days of hospitalisation), one pulmonary embolism (requiring intensive therapy unit) and one postoperative haemorrhage (requiring reintervention).
Misra et al. [15] reported more wound-related infectious complications in the open repair group (33%) than in the laparoscopic repair group (6%). These complications included superficial wound infection (nine in the open and two in the laparoscopic group), deep wound infection, mesh infection and flap necrosis (one each reported in the open group) and seroma (one in the open and four in the laparoscopic group). Urinary retention was reported in two patients (one per repair group), together with one recurrence in the open repair group and two recurrences in the laparoscopic repair group.
The remaining two RCTs [11, 17] reported more complications for laparoscopic repair patients than for open repair patients. Navarra et al. [17] reported postoperative complications in 16.6% of laparoscopic repair patients and in 8.3% of open repair patients. Sixteen percent (2/12) of laparoscopic repair patients suffered from seroma formation, which resolved spontaneously. Eight percent (1/12) of open repair patients suffered a wound infection which healed without requiring mesh removal.
Barbaros et al. [11] reported that 17% (4/23) of laparoscopic repair patients had seroma, and haematoma, cellulitis, ileus and mesh removal due to rejection were each suffered by 4% (1/23) of patients. One patient (4%) had enterotomy, and this same patient also had mesh removed due to infection. The only postoperative complication for the open repair patients was mesh removal due to infection occurring in 17% (4/23) of patients.
The nonrandomised comparative studies reported more complications from the open approach. The most commonly reported complications for open repair were wound infection, seroma and prolonged ileus. For the laparoscopic approach, seroma and enterotomy were the most frequently reported outcomes. More patients in the open group required aspiration drains than those in the laparoscopic group. A small number of complications such as nausea/vomiting, pulmonary embolism, stroke and urinary retention, were also reported in both groups (Tables 7 and 8).
No deaths were reported in either group.
Discussion
Laparoscopic ventral hernia repair is an emerging technique with the potential to replace open repair. The safety and efficacy of laparoscopic repair of ventral hernias in comparison with open repair is uncertain due to a lack of high-level comparative evidence. However, the data from the included studies suggest that the laparoscopic approach may have some advantages over open repair.
The laparoscopic approach may have a lower recurrence rate and require a shorter hospital stay, with conversion to open surgery ranging from 0% to 14% in four nonrandomised comparative studies, 0% in five RCTs and not reported upon in the remaining studies.
Two RCTs [16, 23] reported significantly shorter operating time for laparoscopic repair, whilst one RCT [11] reported a significantly longer operating time for laparoscopic repair. The operating times from the other RCTs [15, 17, 18] and the ranges in operating time from the nonrandomised comparative studies were either not significant, or were similar for both laparoscopic and open approaches.
Variability in the data across the studies may have been influenced by the size and complexity of the hernia and the surgeon’s level of experience. These factors may also have influenced the duration of the operation and whether a conversion to open was required.
Complications from the open approach tended to be wound related, whereas the laparoscopic approach reported wound-related and procedure-related complications such as enterotomy. The variability in the complications reported may be due to differences in operative techniques across studies, for both laparoscopic and open, and the level of the surgeon’s experience with the technique. Complications appeared to be less frequent in laparoscopic repair; however, the sequelae may be more severe, for example, an unrecognised enterotomy could potentially lead to abdominal contamination and sepsis. It is also possible that fewer complications were reported after laparoscopic surgery in the nonrandomised comparative studies because patients with less complex hernias were allocated to the laparoscopic group, while those with more complex hernias were treated with the open approach [13, 14]. Furthermore, complex and large hernias may have been reserved for open repair due to limitations in the laparoscopic technique. Holzman et al. [13] found extremely large hernias difficult to approach laparoscopically due to inability to place functional trocars, which resulted in a tendency to perform open repair for the larger and more complex hernias.
No cost-effectiveness analyses have been published to date. The surgical appliances for the laparoscopic approach are more expensive, but this cost may be balanced by the shorter hospital stay [6, 13].
As there is still uncertainty on whether an open or laparoscopic approach should be used, it is important that patients are well informed of the risks and benefits of each technique.
Further research
To determine long-term safety and recurrence rates, there is a need for more rigorous studies with adequate sample sizes and longer follow-up (longer than 2 years). Other factors that may influence the evaluation of the laparoscopic approach include: the surgeon’s level of experience with the techniques (to ascertain any correlations with the main outcome measures), the reasons for recurrence (as it is unclear whether the recurrence rates reported in the included studies are due to the technique or the noncompliance of patients with postoperative instructions) and postoperative pain (as it is often assumed that minimally invasive procedures are less painful, but few studies testing this assumption have been published).
Conclusions
There is no conclusive evidence that the laparoscopic approach is better or worse than the open approach in terms of safety and efficacy. However, results from the included studies suggest that laparoscopic repair may have a lower recurrence rate, shorter hospital stay and fewer complications. The implications for practice arising from these findings are:
-
The laparoscopic approach may be more suitable for straightforward hernias, with open repair reserved for more complex hernias.
-
Laparoscopic ventral hernia repair appears to be an acceptable surgical operation that can be offered by surgeons proficient in advanced laparoscopic techniques with access to high-technology equipment.
Abbreviations
- RCT:
-
Randomised controlled trial
References
Ramshaw BJ, Esartia P, Schwab J, Mason EM, Wilson RA, Duncan TD, Miller J, Lucas GW, Promes J (1999) Comparison of laparoscopic and open ventral herniorrhaphy. Am Surg 65:827–831
Hernias (1997) In: Sabiston DC Jr, Lyerly HK (eds) Textbook of Surgery. Pocket Companion, WB Saunders, Pennsylvania, pp 418–421
Dorland’s Pocket Medical Dictionary (1995) WB Saunders, Pennsylvania
Society of American Gastrointestinal Endoscopic Surgeons (SAGES) (2003) Laparoscopic ventral hernia repair. http://www.sages.org/pi_ventral_hernia.html [September 2003]
Cassar K, Munro A (2002) Surgical treatment of incisional hernia. Br J Surg 89:534–545
DeMaria EJ, Moss JM, Sugerman HJ (2000) Laparoscopic intraperitoneal polytetrafluoroethylene (PTFE) prosthetic patch repair of ventral hernia. Prospective comparison to open prefascial polypropylene mesh repair. Surg Endosc 14:326–329
Millikan KW (2003) Incisional hernia repair. Surg Clin North Am 83:1223–1234
Luijendijk RW, Hop WCJ, van den Tol P, de Lange DCD, Braaksma MMJ, IJzermans JNM, Boelhouwer RU, de Vries BC, Salu MKM, Wereldsma JCJ, Bruijninckx CMA, Jeekel J (2000) A comparison of suture repair with mesh repair for incisional hernia. N Engl J Med 343:392–398
LeBlanc KA, Booth WV (1993) Laparoscopic repair of incisional abdominal hernias using expanded polytetrafluoroethylene: preliminary findings. Surg Laparosc Endosc 3:39–41
Larson GM (2000) Ventral hernia repair by the laparoscopic approach. Surg Clin North Am 80:1329–1340
Barbaros U, Asoglu O, Seven R, Erbil Y, Dinccag A, Deveci U, Ozarmagan S, Mercan S (2007) The comparison of laparoscopic and open ventral hernia repairs: a prospective randomised study. Hernia 11:51–56
NHMRC (2000) How to use the evidence: assessment and application of scientific evidence. NHMRC, Canberra
Holzman MD, Purut CM, Reintgen K, Eubanks S, Pappas TN (1997) Laparoscopic ventral and incisional hernioplasty. Surg Endosc 11:32–35
Zanghi A, Di Vita M, Lomenzo E, De Luca A, Cappellani A (2000) Laparoscopic repair vs open surgery for incisional hernias: a comparison study. Ann Ital Chir 71:663–667
Misra MC, Bansal VK, Kulkarni MP, Pawar DK (2006) Comparison of laparoscopic and open repair of incisional and primary ventral hernia: results of a prospective randomized study. Surg Endosc 20:1839–1845
Olmi S, Scaini A, Cesana GC, Erba L, Croce E (2007) Laparoscopic versus open incisional hernia repair. Surg Endosc 21:555–559
Navarra G, Musolino C, De Marco ML, Bartolotta M, Barbera A, Centorrino T (2007) Retromuscular sutured incisional hernia repair: a randomised controlled trial to compare open and laparoscopic approach. Surg Laparosc Endosc Percutan Tech 17:86–90
Moreno-Egea A, Carrasco L, Girela E, Martin JG, Aguayo JL, Canteras M (2002) Open vs laparoscopic repair of spigelian hernia: a prospective randomised trial. Arch Surg 137:266–1268
McGreevy JM, Goodney PP, Birkmeyer CM, Finlayson SR, Laycock WS, Birkmeyer JD (2003) A prospective study comparing the complication rates between laparoscopic and open ventral hernia repairs. Surg Endosc 17:1778–1780
Robbins SB, Pofahl WE, Gonzalez RP (2001) Laparoscopic ventral hernia repair reduces wound complications. Am Surg 67:896–900
Chari R, Chari V, Eisenstat M, Chung R (2000) A case controlled study of laparoscopic incisional hernia repair. Surg Endosc 14:117–119
Park A, Birch DW, Lovrics P (1998) Laparoscopic and open incisional hernia repair: a comparison study. Surgery 124:816–821
Carbajo MA, Martin del Olmo JC, Blanco JI, de la CC, Toledano M, Martin F, Vaquero C, Inglada L (1999) Laparoscopic treatment vs open surgery in the solution of major incisional and abdominal wall hernias with mesh. Surg Endosc 13:250–252
Acknowledgements
We would like to thank Drs. Rebecca Tooher and Tabatha Griffin for their editing assistance in this assessment. The full Australian Safety and Efficacy Register of New Interventional Procedures—Surgical (ASERNIP-S) accelerated systematic review of this technique with data extraction tables can be found at the ASERNIP-S website: www.surgeons.org/asernip-s/.
Author information
Authors and Affiliations
Corresponding author
Appendix 1
Appendix 1
Randomised controlled trials in progress
Itani KMF, Neumayer L, Reda D, Kim L, Anthony T. Multicentre trial—Massachusetts, USA: Repair of ventral incisional hernia. Start Date: March 2004. End Date: December 2007.
Malmö University Hospital, SWEDEN: Prospective randomised evaluation of open vs. laparoscopic operation of ventral incisional eventrations—a Swedish multicenter study. Start date: November 2005. End date: December 2008 Study Type: Observational.
Melvin WS. Cincinnati, USA: Prospective, randomised trial of laparoscopic versus open ventral hernia repair. Start Date: April 2000. Randomisation began January 2002.
O’Dwyer P Glasgow, SCOTLAND: Laparoscopic versus open ventral hernia repair using a classical versus collagen mesh (surgisis gold): a European multicentre two factorial randomized controlled trial. Start date: October 2005. End date: October 2007.
Taylor RS London, UK: Prospective randomised comparison of laparoscopic extra-peritoneal and open Lichtenstein hernia repair. Start date: July 1995. End date: July 1998. Results not yet published.
Weber G and Horvath OP. Pecs, HUNGARY: Ventral hernia repair: comparison of suture repair with mesh implantation (onlay versus sublay) using open and laparoscopic approach—prospective, randomised, multicentre study. Start Date: March 2002. The study will run for five years.
Rights and permissions
About this article
Cite this article
Pham, C.T., Perera, C.L., Scott Watkin, D. et al. Laparoscopic ventral hernia repair: a systematic review. Surg Endosc 23, 4–15 (2009). https://doi.org/10.1007/s00464-008-0182-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-008-0182-8