
Abstract
Background
Endoscopic balloon dilation is the first-line treatment for benign colorectal anastomotic strictures. We aimed to objectively assess its long-term results.
Methods
Gastrointestinal symptoms and health-related quality of life (HRQoL) were assessed at long-term after balloon dilation of anastomotic strictures in 31 consecutive patients (excluding those with inflammatory bowel disease) as well as and controls, using the validated Gastrointestinal Quality of Life Index (GIQLI). Most colectomies had been performed for benign diseases, with anastomoses located at the colorectal junction.
Results
Completed surveys were collected from 81 subjects, including 27 study patients (response rate 87%), 27 surgical controls matched for age, gender, and indication of colectomy, and 27 healthy subjects. At a mean of 3.9 ± 2.3 years after the first endoscopic balloon-dilation, study patients self-reported significantly more gastrointestinal symptoms than controls; these included frequent and urgent bowel movements, bloating, food restriction (p ≤ 0.001, all comparisons), diarrhea, excessive passage of gas through the anus (p < 0.01, all comparisons), constipation, and abdominal pain (p < 0.05, all comparisons). Health-related quality of life was significantly impaired in study patients versus surgical controls and healthy subjects (GIQLI scores, 104 ± 20, 119 ± 24, and 121 ± 16, respectively; p = 0.005). Impaired HRQoL subdimensions included gastrointestinal symptoms (p < 0.001), stress by treatment (p < 0.05), and emotional status (p = 0.08). HRQoL was independent of the delay between stricture dilation and the survey. Follow-up endoscopy (performed in 21/27 [78%] study patients, including the 7 patients with the lowest HRQoL, and 19 [70%] surgical controls) disclosed anastomoses larger than 13 mm in all cases.
Conclusions
Health-related quality of life is significantly impaired at long-term after standard balloon-dilation of benign anastomotic colorectal strictures as a result of gastrointestinal symptoms and stress by treatment. This impairment might be related to the fact that an anastomotic diameter ≥13 mm, although commonly used to define successful endoscopic treatment, is insufficient to provide long-term symptom relief in some patients, or to other, yet to be identified, factors.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Benign anastomotic strictures complicate colorectal surgery in 3%–30% of all cases [11]; this complication is more frequent with stapled compared to handsewn anastomoses [12, 13], possibly because mucosal gaps and areas of necrosis induced by staplers generate overactive inflammatory response and healing by secondary intention [5]. Despite this increased risk, the double stapling technique remains exceedingly popular among colorectal surgeons because it is quick and equivalent to manual suturing in terms of mortality, anastomotic leak, cancer recurrence, and wound infection [12, 13]. The popularity of laparoscopy, together with the development of new staplers, is likely to further increase the proportion of stapled colorectal anastomoses in the foreseeable future.
Endoscopic balloon dilation has become the preferred first-line treatment for benign anastomotic colorectal strictures [7], probably because this therapy is easy to perform at the time of diagnosis during ambulatory endoscopy, and it may avoid reoperation, with the inherent risk of colostomy [7, 17]. The morbidity associated with endoscopic dilation is low, and clinical success at 6–24 months has been reported in > 90% of cases [7]. However, despite widespread use for longer than 20 years, long-term clinical results of hydrostatic balloon dilation have, to our knowledge, never been precisely assessed, excepted in patients affected with inflammatory bowel disease.
The aim of this study was to assess gastrointestinal (GI) symptoms and health-related quality of life (HRQoL) in the long term after endoscopic dilation of benign anastomotic colorectal or colocolonic strictures, and to compare those symptoms with those reported by matched surgical controls and healthy subjects.
Methods
Patient selection
Patients were eligible for the study if they had undergone endoscopic dilation of a symptomatic benign anastomotic stricture complicating partial colectomy between August 1996 and March 2004 at the University Hospitals of Geneva. Exclusion criteria were as follows: malignancy detected at the level of the anastomosis (tissue biopsies were obtained in all patients with a previous history of colorectal cancer), previous diagnosis of inflammatory bowel disease (this was thought to be a potential confounding factor affecting HRQoL), and stricture resection after endoscopic dilation. Data collected prospectively included symptoms at presentation, body mass index, details of surgery and of endoscopic procedures, results of histopathological examination, and response to treatment. These were retrieved retrospectively according to a study protocol approved by the ethics review board at the University Hospital of Geneva (no.04092R). An anastomotic stricture was defined as a narrowed anastomosis through which a 12.8-mm-diameter colonoscope could not be passed associated with obstructive symptoms.
Therapeutic procedures
Strictures were balloon-dilated by one of three senior endoscopists during lower GI endoscopy, using a 12.8-mm-diameter colonoscope (EC-3840L, Pentax, Hamburg, Germany; CF-Q160, Olympus, Hamburg, Germany), generally under conscious sedation. Most recently, dilations were performed using a wire-guided CRE balloon (Boston Scientific, Natick, MA) inserted inside the stricture and filled with water under endoscopic control up to the pressure specified by the manufacturer for the desired dilation diameter; this pressure was maintained for at least 2 min. X-ray control was used only when a guidewire (most recently a 0.035-inch-diameter Jagwire, Boston Scientific) could not easily pass the stricture. During each endoscopy, the dilation diameter was chosen according to the following rule: 18–20 mm, 15 mm, and 12 mm for strictures with a diameter evaluated (using a biopsy forceps) at > 5 mm, ≤ 5 mm, or with a pinpoint orifice, respectively. In cases where a dilation diameter ≥ 18 mm was not achieved, additional endoscopic dilation was scheduled 2–3 weeks later. In all patients, strictures were traversed by a standard colonoscope when endoscopic treatment was considered as finished. In two patients with a persisting/relapsing stricture, pneumatic balloon dilators for achalasia (25-mm-diameter and 30-mm-diameter, Rigiflex; Boston Scientific) were used. Antibioprophylaxis was not routinely administered.
Control groups
Surgical controls matched with study patients for age, gender, and indication for colectomy were selected by an independent gastroenterologist from the hospital database of digestive operations performed over the same period of time (total number of partial colectomies, 1,037); healthy subjects matched with study patients for gender and age were selected from among relatives of patients hospitalized in our institution (they were carefully selected to have no past or present digestive disease).
Quality of life
Health-related quality of life was evaluated with the Gastrointestinal Quality of Life Index (GIQLI) [21]. The GIQLI is a standardized, validated, self-reported questionnaire specifically developed for studying GI diseases. It includes 36 items for which a note is given from 4 (absence of symptoms during the 2 weeks preceding the survey) to 0 (severe symptoms) [6, 15, 21, 26]. The best theoretical score is 144 points; the worst, 0 points. In addition to providing a general score, the questionnaire is divided into five subdimensions: GI symptoms, emotional status, physical functions, social functions, and stress by treatment. This questionnaire was sent to study patients and to surgical controls (it was also given at the end of a short interview to healthy subjects) with a stamped, addressed return envelope; all subjects were asked to complete and return the questionnaire. Patients were also asked if they had undergone any colon investigation in another institution. Health-related quality of life of patients was considered low if the total GIQLI score was 1 SD lower than the mean score observed in matched surgical controls.
Follow-up endoscopy
Study patients and surgical controls who had not recently undergone colonoscopy were offered follow-up endoscopy to assess the height and patency of the anastomosis.
Statistical analysis
Comparisons between study patients and surgical controls were performed with the Pearson χ2 test or Fisher’s exact test for categorical data, and the 2-sample unpaired t-test for continuous variables. Comparisons of GIQLI scores between the three groups were performed using one-way analysis of variance with Dunnett’s correction for multiple comparisons, with healthy subjects as the control group. All p tests were two-sided, and p values less than 0.05 were considered statistically significant. Analyses were performed with JMP software (version 5.1.2, SAS, Cary, NC)
Results
Surveys were sent to 31 consecutive patients who fulfilled our inclusion criteria, and 27 (87%) completed surveys were received (Fig. 1). Demographic, clinical, and pathological characteristics were similar in study patients and matched surgical controls (Table 1), except for use of a stapling device, which was more frequent in study patients (27/27 [100%] versus 21/27 [78%]; p = 0.023). The indication for partial colectomy was a symptomatic diverticulosis in 80% of cases, and none of the study patients or surgical controls had received radiotherapy.

Selection of study patients and controls.
At the time of stricture dilation, study patients were complaining of severe constipation and/or ribbon stools (n = 15; 56%), diarrhea (n = 5; 19%), bloating (n = 2; 7%), and abdominal pain (n = 2; 7%); three (11%) patients presented with ileus. Anastomotic strictures were located at a mean of 14.8 ± 4.6 (range: 10–28) cm from the anal verge. The mean delay between colectomy and the first session of endoscopic stricture dilation was 10.1 ± 10.1 (range: 1.1–45.5) months. Repeat dilation was performed in 15 (56%) patients; a mean of 1.7 ± 0.7 (range, 1–3) dilations per patient were performed. A postdilation perforation (small amount of free gas at computed tomography [CT]-scan) was detected in one (4%) patient; conservative treatment with intravenous antibiotics for 10 days was successful, and the complication was graded as severe [2].
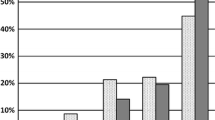
The survey was completed by study patients 46.6 ± 26.5 (range: 14.2–96.9) months after endoscopic stricture dilation. As illustrated in Figure 2, compared to both control groups, study patients self-reported more trouble related to bloating and food restriction (p < 0.001 each), frequent (p < 0.001) and urgent (p = 0.001) bowel movements, excessive passage of gas through the anus (p = 0.003), frustration (p = 0.001) and anxiety (p = 0.003) about their illness, diarrhea (p = 0.006), abdominal pain (p = 0.017), being troubled by medical treatment (p = 0.025), constipation (p = 0.038), and fatigue (p = 0.046). For control items (questions about dysphagia) no difference was detected between groups (p = 0.461 and 0.855 for the comparison between study patients and healthy subjects of GIQLI items 28 and 29, respectively). Compared to healthy subjects, surgical controls self-reported similar scores for all items, except items 8 (eating with pleasure; p = 0.020) and 10 (coping with everyday stresses; p = 0.043).

GIQLI (Gastrointestinal Quality of Life Index) items with the most statistically significant differences for the comparison between groups using Dunnett’s test with healthy subjects as controls. Higher scores indicate better quality of life and p values < 0.05 are indicated
Health-related quality of life was significantly more impaired in study patients compared to surgical controls and healthy subjects (total GIQLI score, 104 ± 20, 119 ± 24, and 121 ± 16, respectively; p = 0.005) (Fig. 3). This lowered HRQoL was found to be independent of the delay between stricture dilation and the survey (total GIQLI score in 13 and 14 study patients with delay > or ≤ 4 years, 106 ± 26 and 102 ± 14, respectively; p = 0.570). Except for social status, all subdimensions of HRQoL were altered in study patients as compared to the two control groups. The difference reached statistical significance for GI symptoms (p < 0.001) as well as stress by treatment (p = 0.025), and it approached statistical significance for emotional status (p = 0.080) (the difference was statistically significant in separate comparisons, with p values of 0.036 and 0.019 for comparison with healthy subjects and with surgical controls, respectively). Surgical controls had values similar to healthy subjects for the total GIQLI score and all of its subdimensions.

Comparison of total GIQLI (Gastrointestinal Quality of Life Index) scores and its five subdimensions between groups. Higher scores indicate better quality of life (each score is presented relative to its maximum theoretical value). Circles are centered on score means and have a diameter proportional to the 95% confidence interval of the mean according to Dunnett’s test for multiple comparison with healthy subjects as controls
Follow-up endoscopy was performed in 21/27 (78%) study patients and 19/27 (70%) surgical controls, at a mean of 45.8 ± 28.1 and 61.9 ± 24.5 months after colon resection, respectively (p = 0.062) (35.1 ± 29.8 months after the first endoscopic dilation in study patients): anastomoses were located at a mean of 14.8 ± 4.7 and 16.6 ± 2.2 cm from the anal verge, respectively (p = 0.149), and were easily traversed by a standard colonoscope in all 40 of these patients.
Nine (33%) study patients self-reported a low HRQoL, defined as a total GIQLI score smaller to the mean of matched surgical controls—1 SD. These patients had undergone one (n = 2), two (n = 5), or three (n = 2) sessions of endoscopic dilation, with the last dilation performed at a diameter of 18 (n = 3), 19 (n = 1), 20 (n = 4), and 30 (n = 1) mm. Three of them had not presented at all for endoscopy during follow-up. The median duration between the last procedure and the survey in these 9 patients was 17 (11–90) months. Follow-up endoscopy was performed after questionnaire collection in 7 of them and disclosed a patent anastomosis that was easily traversed by a standard colonoscope in all cases.
Discussion
Four years after endoscopic stricture dilation, HRQoL was significantly more impaired in study patients compared to healthy subjects as well as matched surgical controls. This alteration in HRQoL was relatively severe because total GIGLI scores reported by study patients were close to those reported in various conditions for which surgery is recommended (e.g., diseases of the GI or biliopancreatic tract) [14, 21]. Abnormal GI symptoms included abdominal pain, alterations in bowel movements, gas bloat, and restriction of food intake. These chronic disorders even tended to affect the patients’ emotional status, a finding that is not surprising, as depression and anxiety are known to complicate chronic GI disorders such as inflammatory bowel disease [1]. Of note, we excluded patients with inflammatory bowel disease (which is known to influence the results of endoscopic dilation) to study a relatively homogeneous group of patients [7], and we elected two control groups to verify (1) if treatment with balloon dilation was restoring HRQoL similar to that observed after uncomplicated partial colectomy, and (2) if uncomplicated partial colectomy decreased HRQoL in our population.
We think that the relatively poor results reported here compared with previous studies (Table 2) reflect differences in methodology for assessing symptoms. No other study has used a HRQoL questionnaire; the GIQLI allows precise assessment of GI symptoms, has been validated for the evaluation of benign as well as malignant colorectal diseases before and after surgery [6, 19, 21], and it is completed by the patients at home without any interference from the investigators. The GIQLI was selected among other instruments available to assess GI symptoms and HRQoL because it has been validated in French, the mother language of the subjects included in this study [6, 19, 21], and it contains both generic and disease-specific HRQoL measures. The use of generic and disease-specific measures complies with guidelines from the European Association for Endoscopic Surgery [10], and their combination in a single questionnaire was thought to avoid the burden of patients having to complete two distinct instruments (and thus to increase response rates). The Fecal Incontinence Quality of Life Scale (FIQL) [10], although recommended by the European Association for Endoscopic Surgery, was not selected, because most study patients had initially presented with constipation, and the FIQL is designed to assess fecal incontinence. On the other hand, our treatment protocol was standard; the proportion of patients who underwent stricture resection after endoscopic dilation (9%) was in the range of published figures, and all follow-up endoscopies (including those performed in study patients with the most severely decreased HRQoL) disclosed anastomoses that were easily traversed by a standard colonoscope.
As no significant difference was found between study patients and surgical controls at baseline or at follow-up endoscopy, we hypothesize that a significant proportion of patients require an anastomosis wider than the 12–13 mm currently used for the definition of benign anastomotic strictures. This conjecture is also supported by (1) the finding, in a series of 36 patients, that the diameter of symptomatic benign anastomotic strictures was comprised between 12 and 20 mm in 58% of cases [23], and (2) a randomized controlled trial that has shown that symptom relief and lumen patency lasted about twice as long after dilation with 35-mm balloons as after dilation with 18-mm balloons [3]. However, based on our data, we cannot exclude that an underlying condition causing the strictures (rather than the anastomosis diameter) is linked to subsequent symptoms. For example, impairments in blood flow could cause both the stricture (ischemia) and subsequent motility disorders (in which case a larger lumen diameter would not lead to better outcomes). This possibility should be further assessed in future studies. Trials comparing standard balloon dilation and other modalities providing larger anastomotic diameters are also warranted to resolve this issue.
Various endoscopic techniques have been described to reach large anastomotic diameters, apparently with no increased risk: two balloons may be inflated side-by-side [4], or strictures may be incised with a sphincterotome before dilation or tissue ablation is performed [8, 18]. Newer guidable stapler systems can be introduced through the anus, parallel to a colonoscope, to divide anastomotic diaphragms under endoscopic control, and enlarge anastomoses up to 3 cm [16]. Redo surgery is also an option, with 89%–100% of patients reported to have normal bowel habits after a mean follow-up of 12–49 months [7]. However, the paucity of data in the literature suggests that, in the majority of cases, patients are not willing to undergo repeat surgery.
It is also important to stress that among the nine patients with the most severely decreased HRQoL, three had not presented at all for endoscopy during follow-up, and six had presented only once. These patients tolerated GI symptoms for long periods of time without seeking specialized medical advice, probably because of the belief that relatively severe GI symptoms are common after colectomy (which proved to be incorrect, as matched surgical controls reported a HRQoL similar to healthy controls), or by fear of reoperation. Based on our results, we would advise use of a validated tool to assess symptoms at regular intervals after stricture dilation, and to explain to patients that partial colectomy does not impair HRQoL. Patients should also be encouraged to seek specialized medical advice in case of symptom recurrence.
In conclusion, treatment of benign anastomotic strictures by standard endoscopic dilation yields poor long-term results. Patients suffer a considerable burden of GI symptoms that contribute, with the stress by treatment, to significantly impair their HRQoL. This finding may be related to the fact that the standard criteria used to define successful dilation (anastomosis ≥ 13 mm in diameter) is insufficient for a significant proportion of patients or to yet unidentified confounding factors. Randomized controlled trials comparing GI symptoms and HRQoL after stricture dilation using either standard balloons or newer techniques providing larger anastomotic diameters are warranted.
References
Addolorato G, Capristo E, Stefanini GF, Gasbarrini G (1997) Inflammatory bowel disease: a study of the association between anxiety and depression, physical morbidity, and nutritional status. Scand J Gastroenterol 32:1013–1021
Cotton PB (1994) Outcomes of endoscopy procedures: struggling towards definitions. Gastrointest Endosc 40:514–518
Di Giorgio P, De Luca L, Rivellini G, Sorrentino E, D’Amore E, De Luca B (2004) Endoscopic dilation of benign colorectal anastomotic stricture after low anterior resection: A prospective comparison study of two balloon types. Gastrointest Endosc 60:347–350
Di ZH, Shin JH, Kim JH, Song HY (2005) Colorectal anastomotic strictures: treatment by fluoroscopic double balloon dilation. J Vasc Interv Radiol 16:75–80
Dziki AJ, Duncan MD, Harmon JW, Saini N, Malthaner RA, Trad KS, Fernicola MT, Hakki F, Ugarte RM (1991) Advantages of handsewn over stapled bowel anastomosis. Dis Colon Rectum 34:442–448
Eypasch E, Williams JI, Wood-Dauphinee S, Ure BM, Schmulling C, Neugebauer E, Troidl H (1995) Gastrointestinal Quality of Life Index: development, validation and application of a new instrument. Br J Surg 82:216–222
Garcea G, Sutton CD, Lloyd TD, Jameson J, Scott A, Kelly MJ (2003) Management of benign rectal strictures: a review of present therapeutic procedures. Dis Colon Rectum 46:1451–1460
Hagiwara A, Sakakura C, Shirasu M, Torii T, Hirata Y, Yamagishi H (1999) Sigmoidofiberscopic incision plus balloon dilatation for anastomotic cicatricial stricture after anterior resection of the rectum. World J Surg 23:717–720
Johansson C (1996) Endoscopic dilation of rectal strictures: a prospective study of 18 cases. Dis Colon Rectum 39:423–428
Korolija D, Sauerland S, Wood-Dauphinee S, Abbou CC, Eypasch E, Caballero MG, Lumsden MA, Millat B, Monson JR, Nilsson G, Pointner R, Schwenk W, Shamiyeh A, Szold A, Targarona E, Ure B, Neugebauer E (2004) Evaluation of quality of life after laparoscopic surgery: evidence-based guidelines of the European Association for Endoscopic Surgery. Surg Endosc 18:879–897
Luchtefeld MA, Milsom JW, Senagore A, Surrell JA, Mazier WP (1989) Colorectal anastomotic stenosis. Results of a survey of the ASCRS membership. Dis Colon Rectum 32:733–736
Lustosa SA, Matos D, Atallah AN, Castro AA (2001) Stapled versus handsewn methods for colorectal anastomosis surgery. Cochrane Database Syst Rev: CD003144
MacRae HM, McLeod RS (1998) Handsewn vs. stapled anastomoses in colon and rectal surgery: a meta-analysis. Dis Colon Rectum 41:180–189
Quintana JM, Arostegui I, Oribe V, Lopez de Tejada I, Barrios B, Garay I (2005) Influence of age and gender on quality-of-life outcomes after cholecystectomy. Qual Life Res 14:815–825
Quintana JM, Cabriada J, Lopez de Tejada I, Varona M, Oribe V, Barrios B, Perdigo L, Bilbao A (2001) Translation and validation of the gastrointestinal Quality of Life Index (GIQLI). Rev Esp Enferm Dig 93:693–706
Reinshagen K, Muldner A, Reinshagen S, Kahler G (2005) Endoscopically controlled strictureplasty for stenotic colorectal anastomosis. Endoscopy 37:873–875
Schlegel RD, Dehni N, Parc R, Caplin S, Tiret E (2001) Results of reoperations in colorectal anastomotic strictures. Dis Colon Rectum 44:1464–1468
Schubert D, Kuhn R, Lippert H, Pross M (2003) Endoscopic treatment of benign gastrointestinal anastomotic strictures using argon plasma coagulation in combination with diathermy. Surg Endosc 17:1579–1582
Schwenk W, Neudecker J, Haase O, Raue W, Strohm T, Muller JM (2004) Comparison of EORTC quality of life core questionnaire (EORTC-QLQ-C30) and gastrointestinal quality of life index (GIQLI) in patients undergoing elective colorectal cancer resection. Int J Colorectal Dis 19:554–560
Skreden K, Wiig JN, Myrvold HE (1987) Balloon dilation of rectal strictures. Acta Chir Scand 153:615–617
Slim K, Bousquet J, Kwiatkowski F, Lescure G, Pezet D, Chipponi J (1999) [First validation of the French version of the Gastrointestinal Quality of Life Index (GIQLI)]. Gastroenterol Clin Biol 23:25–31
Suchan KL, Muldner A, Manegold BC (2003) Endoscopic treatment of postoperative colorectal anastomotic strictures. Surg Endosc 17:1110–1113
Truong S, Willis S, Schumpelick V (1997) Endoscopic therapy of benign anastomotic strictures of the colorectum by electroincision and balloon dilatation. Endoscopy 29:845–849
Venkatesh KS, Ramanujam PS, McGee S (1992) Hydrostatic balloon dilatation of benign colonic anastomotic strictures. Dis Colon Rectum 35:789–791
Virgilio C, Cosentino S, Favara C, Russo V, Russo A (1995) Endoscopic treatment of postoperative colonic strictures using an achalasia dilator: short-term and long-term results. Endoscopy 27:219–222
Yeung SM, Shiu AT, Martin CR, Chu KM (2006) Translation and validation of the Chinese version of the Gastrointestinal Quality of Life Index in patients with gastric tumor. J Psychosom Res 61:469–477
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Nguyen-Tang, T., Huber, O., Gervaz, P. et al. Long-term quality of life after endoscopic dilation of strictured colorectal or colocolonic anastomoses. Surg Endosc 22, 1660–1666 (2008). https://doi.org/10.1007/s00464-007-9679-9
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-007-9679-9