
Abstract
Background
Assessing cancer margins, lymph nodes, and small cancer deposits intraoperatively can be challenging. A new device has become available that allows the detection of positron emission tomography (PET) radiotracers through both high-energy gamma and short-range beta emissions. These PET probes are handheld, allowing for real-time evaluation of cancer using a tool that provides surgeons with better intraoperative assessment of tumor sites.
Methods
Within the context of two institutional review board (IRB)-approved protocols investigating new applications of antibody-labeled PET scanning, 124I-labeled humanized monoclonal antibodies specific for colorectal cancer (huA33) and renal tumors (cG250) were constructed. Patients underwent preoperative PET scans, approximately seven days post-tracer infusion, when tumor-to-nontumor ratios were high. Suspected tumor deposits were evaluated intraoperatively with handheld beta and gamma PET probes.
Results
Handheld PET probes detected emissions from all tumors. Count rates from the gamma probe on tumor ranged from 48 to 306 cps, and for the beta probe ranged from 18 to 190 cps. Gamma and beta emissions exhibited a strong positive correlation. The ratio of gamma and beta counts was at least twice that of the background counts for all tumors evaluated.
Conclusions
This study is the first to demonstrate the utility of beta probes for the intraoperative detection of radiolabeled antibodies targeting cancer. Importantly, the recorded beta count rates from the beta probe correlate with the count rates from the high-energy gamma probe. Furthermore, the beta probe may offer superior specificity for real-time localization of small tumor deposits, compared to gamma probes. The intraoperative portable PET probe may prove a valuable bridge to combining tumor biology and PET technology to guide surgical therapy.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Positron emission tomography (PET) has increased the sensitivity for identifying occult sources of cancer and thereby improved the staging of patients with a number of potentially curable cancers. However, difficulty remains in pinpointing the specific sites of tumor, and in particular identifying small cancer deposits that approach the resolution of the current nuclear medicine instrumentation, currently about 1 cm3 [1]. PET images are formed by the coincident detection of the pair of opposed 511 keV photons, created by the annihilation of an emitted positron with an electron in the body tissue, thus detecting sites of high-energy gamma emissions to form an image that locates sites of cancer. However, correlating the preoperative PET image to intraoperative findings remains a challenge. Most clinical applications using PET scans for detection of cancer have been with 18F-labeled fluorodeoxyglucose (FDG), which evaluates sites of high glucose metabolic activity, such as tumors, inflammation, and infection. A newer, promising application of PET is in the detection of cancer through the use of tumor-specific antibodies, radiolabeled with long-lived positron-emitting radionuclides, such as iodine 124, with a half-life of 4.2 days. However, even with potential improved tumor specificity of radioimmune PET, the surgeon must visualize how a preoperative tomographic image translates into a three-dimensional location during surgery.
The development of handheld PET probes has assisted in this translation by allowing the real-time intraoperative detection of tumor and tumor deposits from sites with radiolabeled antibodies that are detectable by PET. Because PET radioisotopes initially emit a positively charged beta particle (positron), followed by high-energy annihilation, possibly with other gamma rays, this gives the opportunity to combine a dedicated beta detector with a gamma ray probe. Beta particles travel distances ranging from only millimeters to several centimeters from a radiolabeled source. This property makes beta particles undetectable with PET scanners, but potentially detectable at close range, such as intraoperatively during resection of a tumor, or for assessment of lymph nodes or small deposits of cancer. A significant advantage of a beta detector probe is its high sensitivity to local radioactivity distribution, which provides a much greater change in signal when moving from tumor to background. In contrast, gamma-ray probes sum contributions from radioactivity over a much greater depth of tissue, and therefore are less able to discriminate between surface tumor and deeper-seated normal tissue. A further advantage of beta probes is that they are responsive only to sources within 1–2 mm distance from the probe tip, and do not require the extensive collimation needed by a high-energy 511-keV gamma probe. This allows the design of probe sizes that are small enough to be used in minimally invasive surgery, and are potentially usable through a 5-mm port site.
As such, we aimed to evaluate, for the first time, the utility of these handheld high-energy gamma and beta detectors for identifying cancer deposits with 124I-labeled antibodies specific for colorectal and renal cell tumors. We furthermore aimed to assess whether beta and gamma emissions would correlate with detection of tumor deposits.
Materials and methods
Clinical study
All studies were carried out under protocols approved by the institutional review board (IRB) of Memorial Sloan-Kettering Cancer Center (MSKCC) and by the protocol review committee of the Ludwig Institute for Cancer Research (LICR), which provided the antibodies for these studies. The LICR has submitted an investigational new drug (IND) application for each agent and all protocols are being carried out under this IND, and are approved by the Food and Drug Administration (FDA).
For this study, PET probes were evaluated in the context of two ongoing, IRB-approved clinical trials at MSKCC, testing ways of improving PET scanning using antibody-labeled radioisotopes that are specific for various types of cancer. The first involves 124I-labeled-huA33 antibody, which targets the A33 transmembrane glycoprotein antigen, and is being evaluated for PET specificity in a trial of patients with colorectal cancer. The second study involves 124I-labeled cG250, an antibody directed against a carbonic anhydrase IX, which is found in the conventional clear cell carcinoma that is a distinct histological subtype of renal cell carcinoma. This is being evaluated for PET specificity in a trial of patients with newly diagnosed renal masses, in order to identify clear cell renal carcinoma preoperatively.
Specifically, patients received a single intravenous (IV) infusion of 4 mCi/10 mg 124I-huA33 in 30 mL of 5% human serum albumin (HSA) over ten minutes, or 5mCi/10 mg 124I-cG250 over 20 minutes. Blood samples were then obtained for pharmacokinetic analysis at 5, 15, 60 and 120 minutes after completion of the IV infusion. PET scans were performed within four hours post-radiolabeled-antibody infusion, and then again on the day of operation (around seven days later), when patients underwent a PET scan of the abdomen and pelvis less than three hours prior to surgery. Tumor and normal tissue (colon, liver or kidney) obtained at surgery (or biopsy), as well as serum, were measured for estimation of percentage-injected-dose (%ID) per gram of tumor and serum. Tissue samples were obtained for autoradiography and immunohistochemistry as an additional assessment of tumor targeting.
PET probes
The handheld PET probes, measuring high-energy gamma and beta emissions, that were used in this study, were obtained from IntraMedical Imaging LLC (Los Angeles, CA) and detect 511-keV photons from positron-emitting sources (gamma probe) and positrons (or beta rays) directly (beta probe). These instruments allow the connection of both probes simultaneously via separate input ports on the front face of a PC-based read-out console. The monitor records the counts per second (cps), and allows automatic background subtraction and the setting of a threshold count rate, above which an audible signal can be heard if desired. The monitor displays the instantaneous count rate, but also the highest count rate over the previous second (or user-selectable number of seconds). A single mouse click selects between the active probe, either beta or gamma. High-energy gamma and beta probes are all calibrated to a point source of 124I-Ab, and the count rate determined, in order to optimize detection of the respective emissions. All probe readings can be recorded within a data file on the PC for later analysis.
Radiolabeled 124I tracer
MSKCC has produced 124I, a positron emitter with a half-life of 4.2 days, in our cyclotron, using a reusable 124Te-tellurium dioxide solid-state target. This isotope is ideal for imaging with intact immunoglobulin. The nuclide has been used clinically in patients with thyroid cancer, as well as labeled with antibodies under an FDA-approved drug master file (no. 13227). Our institution has also carried out extensive characterization of the optimal imaging characteristics of 124I with a variety of PET cameras.
Intraoperative gamma- and beta-probe methods
Four patients were evaluated with the gamma and beta probes, two patients with colorectal metastases and two patients with clear cell renal cancer. Once the patients were in the operating room and anesthetized, the high-energy gamma and beta probes were used to evaluate counts in areas of suspected tumor versus background tissue (correlated from the preoperative PET scan), and these were recorded in triplicate. Excised tissue was then evaluated ex vivo with the high-energy gamma and beta probes in areas of tumor, tumor necrosis, surrounding normal tissue and background. Results were then correlated with noninvasive PET scan results (i.e., PET positivity and standardized uptake value) and with final pathology of the specimen.
Results
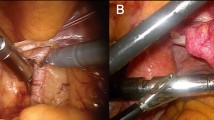
Representative 124I radioimmuno-PET scans are shown in Fig. 1, alongside photographs of the corresponding excised tumor specimens from one patient with colorectal cancer and one with clear cell renal carcinoma. Figure 1a shows a PET coronal slice where background uptake in the colon can be seen, as well as the area of uptake in the right lateral lobe of the liver. The excised liver metastasis is shown in the corresponding photograph (Fig. 1b). Figure 1c demonstrates 124I-cG250 targeting, on the PET scan, of a clear cell renal carcinoma. In Fig. 1d, the corresponding gross photograph is shown.

Representative 124I-antibody-labeled PET scan and gross photo of patient with a colorectal tumor (a and b) and patient with a renal tumor (c and d)
After tumor excision, all specimens were photographed, as shown in a representative case from a patient with a colorectal metastasis to the liver and lymph node in Fig. 2. This patient presented with a colorectal metastasis to the liver two years after initial surgery for primary colon cancer. In addition, the patient was noted to have internal iliac lymph node sites that were equivocal on preoperative PET scanning, but were detectable with intraoperative assessment with PET probes. Sections of tumor within the liver and lymph node disease, as well as a segment of surrounding normal liver tissue that was excised as part of the specimen, were evaluated as shown by autoradiography, hematoxylin and eosin (H&E) staining, and with PET probes for high-energy gamma and beta counts per second. Readings were obtained in triplicate from the tissue samples shown. The autoradiographs (Figs. 2d–f) show the highest uptake of radiolabeled antibody in the liver metastasis (Fig. 2d), followed by slightly lower uptake in the lymph node (Fig. 2e). H&E staining of the specimens demonstrated a higher tumor burden in the liver specimen than in the lymph node. Use of the PET probes for the colorectal liver metastasis demonstrated the highest number of counts per second at 125 ± 11, followed by detectable, but lower counts in an excised lymph node of 45 ± 2 cps. The background tissue readings obtained from a segment of normal liver are included for reference. Beta counts over the colorectal liver metastasis and lymph node were about half that seen for gamma counts, at 63 ± 12 versus 125 ± 11, respectively, over tumor; and 27 ± 8 versus 45 ± 2 over the internal iliac lymph node, respectively. Beta counts over sites of tumor were 2.7–6.3 times higher than background counts, whereas gamma counts were only 1.5–3.7 times higher than background counts, demonstrating the expected higher tumor specificity of the beta probe.

Patient with a colorectal cancer metastasis to the liver and distant metastatic lymph node showing tumor sites and corresponding autoradiographs, hematoxylin and eosin (H&E) staining, and high-energy gamma and beta counts
Figure 3 demonstrates actual gamma and beta counts obtained as the resected tissue from a renal cell carcinoma is scanned from end and end, readings being recorded at 1-cm intervals. This data demonstrates the range of detectability and specificity of the gamma and beta probes over the different tissue regions within the excised specimen, i.e., normal tissue, necrotic and viable tumor tissue. It is important to note that the necrotic tumor sites demonstrated very high gamma counts (due to contribution from radioactivity at deeper tissue layers), but low beta counts, when compared to counts over viable tumor. Normal tissue expressed background counts that were about half those seen for viable tumor, rendering detection of tumor sites possible.

High-energy gamma and beta counts, obtained from a renal cell carcinoma specimen, over tumor, necrotic center, and normal renal tissue. All counts represent triplicate readings ± standard error on the mean (SEM)
After obtaining high-energy gamma and beta counts from the tumors of all four patients studied, the relative correlation of the gamma counts and beta counts was assessed. A strong correlation between the gamma and beta counts over 37 separate readings was observed from measurements over the various sites of tumor from both colorectal and renal cell tumors, as shown in Fig. 4.

Correlation of 37 high-energy gamma counts and correlating beta counts obtained from the tumors of the four patients studied. This demonstrates the relationship of each individual high-energy gamma count to its correlating beta count at that point on the tumor
The absolute counts are reported for both beta and gamma probes. Of greater importance may be the detectability expressed as the counts from tumor sites in relation to background normal tissue counts for each patient studied. The ratio of gamma and beta counts detected in relation to background counts was also analyzed and the results are shown in Fig. 5. For patients 1 and 2, with metastatic colorectal cancer, beta tumor/background count ratios were higher than those obtained with the counts from the gamma probe. This was not observed in patients 3 and 4, with clear cell renal carcinoma, where the ratio of counts from the gamma probe (tumor/background) was higher than (in one patient) or equal to the counts obtained with the beta probe. This suggests that the benefits of the beta probe may be contingent upon the configuration of the tumor specimen, with the beta probe being advantageous for superficial tumor deposits.

Ratio of high-energy gamma and beta emissions over background counts in normal tissue, measured in tumors excised from patients with colorectal cancer (n = 2, patients 1 and 2) and renal cell cancer (n = 2, patients 3 and 4). All counts were obtained in triplicate ± standard error on the mean (SEM)
Discussion
Handheld PET probes for the detection of positrons were first described and developed by Daghighian et al. in 1994 as a novel method to direct intraoperative tumor localization [2]. Unlike low-energy gamma probes that allow for detection of markers such as 99mTc (used for sentinel node mapping, but not for identification of tumor cells), the new PET probe device allows either the direct detection of the positron emission, which in this study arose from radiolabeled antibody targeting of tumor cells, or by detecting the same high-energy 511-keV gamma rays using a highly collimated photon probe, which forms the basis of the camera signal in positron emission tomography. This technology provides a unique combination of detection devices that, in a small handheld form, can be used in the operating room to detect smaller foci of tumor than is possible using conventional PET scanning. In addition, the ability to use this technology as a real-time device, before, during and after resection of tumor, to identify additional tumor deposits, lymph nodes and clear resection margins, would provide a valuable and feasible tool to improve cancer resections.
The gamma probe, although useful for open resections, cannot be reduced below a 12-mm diameter, due to the heavy collimation needed to shield side scatter from the high-energy photons. For this reason, the beta probe is of particular interest, because of its potential to be produced in a small form that can be introduced through a 5-mm laparoscopic port site.
Several authors have addressed the use of the high-energy gamma probe for the detection of tumor deposits with FDG during surgery [3–6]. The purpose of this study was to establish for the first time that the positron-detecting beta probe is able to detect tumor sites with equivalent reliability to that of the more bulky gamma probe, in humans. The results of our study demonstrate that the beta probe appears to be more specific than the gamma probe, and correlates reliably with readings obtained from the gamma emissions.
In Fig. 2, we show that the gamma and beta probes are useful for detecting positron emissions from tissue with tumor and that these counts are distinct from background counts obtained over normal liver tissue. Interestingly, the counts obtained correlate with increasing amounts of tumor, as seen on H&E staining, suggesting that the probes are reliable and able to differentiate tumor-containing tissue from normal tissue.
Data from Fig. 3 show a representative patient with a clear cell renal cell carcinoma, using the G250-labeled antibody specific for clear cell renal carcinoma [7], again demonstrating the relative ability of the gamma and beta probes to detect sites of tumor over necrotic sites and viable sites, in comparison to normal renal parenchyma. Beta counts were able to differentiate necrotic from viable tumor, whereas gamma probes were not, due to the scatter from nearby viable tumor contributing to the gamma probe signal.
Figure 4 demonstrates the correlation between the counts from gamma and beta probes from the tumor sites of the four patients studied. This is an important observation, since it connects the photon signal, which forms the basis of the PET image, with the intraoperative signal detected by both gamma and beta probes. Clearly, further studies with more patients will need to fully confirm the findings from this pilot study.
Lastly, the specificity of the gamma and beta probes, i.e., the ability to differentiate between viable tumor from background nontumor or necrotic tissue, was evaluated by the ratio of counts for each probe between tumor and background for all four patients studied. For both patients with colorectal carcinoma metastases, the tumor/background ratio was five for the beta probe, compared to only 2.5 for the gamma probe, suggesting a potential advantage for the beta detector. However, there was no significant difference in the ratio of tumor/background counts for the two probes compared in the two renal cell carcinoma patients.
In summary, this pilot study demonstrates for the first time the feasibility of intraoperative beta probes, with a potential advantage for selected tumor deposits over conventional gamma-type probes. If further studies confirm this finding, then the utility of real-time intraoperative beta detectors may improve the sensitivity of tumor detection beyond that of conventional PET scans, where the limit of detectable is approximately 6–10 mm. We have yet to establish the lowest detectable limit of beta intraoperative probes in vivo, but this study is underway. Further studies of this promising technology are warranted and will establish the role of handheld PET probes in the resection of cancer.
References
Alazraki NP, Mishkin FS (1991) Fundamentals of nuclear medicine, 2nd edition. The Society of Nuclear Medicine, Inc., ISBM? 0-932004-29-6, p 85
Daghighian F, Mazziotta JC, Hoffman EJ, Siegel S, Shenderov P, Eshaghian B, Phelps ME (1994) Intraoperative beta probe: A device for detecting tissue labeled with positron- or electron-emitting isotopes during surgery. Med Phys 21:153–157
Essner R, Daghighian F, Giuliano A (2002) Advances in FDG PET probes in surgical oncology. Cancer J8:100–108
Gulec SA, Dahgighian F, Essner R (2006) PET Probe: Evaluation of technical performance and clinical utility of a handheld high-energy gamma probe in oncologic surgery. Ann Surg Oncol 1–8
Essner R, Hsueh E, Haigh P, Glass E, Huynh Y, Daghighian F (2001) Application of an 18F fluorodeoxyglucose-sensitive probe for the intraoperative detection of malignancy. J Surg Res 96:120–126
Franc B, Mari C, Johnson D, Leong S (2005) The role of a positron and high-energy gamma photon probe in intraoperative localization of recurrent melanoma. Clin Nucl Med 30:787–791
Divgi CR, Pandit-Taskar N, Jungbluth AA, Reuter VE, Gonen M, Ruan S, Pierre C, Nagel A, Pryma DA, Humm J, Larson SM, Old LJ, Russo P (2007) Preoperative characterisation of clear-cell carcinoma using iodine-124-labelled antibody chimeric G250 (124I-cG250) and PET in patients with renal masses: a phase I trial. Lancet Oncol 8:304–310
Acknowledgments
Supported in part by a grant from the Society of American Gastrointestinal Endoscopic Surgeons (V.S.), and in part by the Ludwig Center for Cancer Immunotherapy and 5 PO1 Ca33049.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Strong, V.E., Humm, J., Russo, P. et al. A novel method to localize antibody-targeted cancer deposits intraoperatively using handheld PET beta and gamma probes. Surg Endosc 22, 386–391 (2008). https://doi.org/10.1007/s00464-007-9611-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-007-9611-3