
Abstract
Background
This study aimed to investigate the impact of manipulation angles and instrument length on task performance and muscle workload in hand-assisted laparoscopic surgery.
Methods
The standard task was to close a 5-cm enterotomy of porcine small bowel inside a hand-assisted laparoscopic trainer. Surgeons were instructed to place the sutures 3 to 5 mm apart and from the enterotomy edge. Ten surgeons participated in each experiment. In the first experiment, each surgeon performed one task for each of the following manipulation angles: 45°, 60°, 75°, and 90°. In the second experiment, each surgeon performed two sessions of three tasks using either standard-length (330 mm) or short (250 mm) needle holders in the external hand. Outcome measures were execution time (s), placement error score (mm deviation from exact placement), leaking pressure (mmHg), and muscle workload by upper extremities as measured by integrated electromyography (mV s).
Results
In the first experiments, the mean execution time was significantly longer with 90° angles than with 45° and 60° manipulation angles (1,074.9 vs 715.9 s and 657.9 s with p < 0.05 and p < 0.01, respectively). The 90° manipulation angle had the greatest muscle workload by the deltoid and trapezius of the extracorporeal and intracorporeal limbs and the extracorporeal dominant arm extensor and flexor groups. In the second experiment, the short instruments had a shorter mean execution time than the standard-length instrument (572.05 vs 618.75 s; p < 0.01). There was less muscle workload with the short than with the standard-length instrument by the extracorporeal dominant forearm extensor and flexor muscle groups and the deltoid of extracorporeal dominant and intracorporeal limbs. There were no significant differences in leaking pressure or placement error score between the different manipulation angles and instrument lengths.
Conclusion
The best ergonomic setup in hand-assisted laparoscopic surgery entails a manipulation angle of 45° to 60° and use of an instrument with a shorter shaft than standard laparoscopic length.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Hand-assisted laparoscopic surgery (HALS) has been introduced as a hybrid approach to overcome the mechanical constraints of total laparoscopic surgery while maintaining its benefits. The technique allows the surgeon to use the best available instrument (i.e., the hand) for exploration, exposure, finger dissection, palpation, and immediate effective hemostasis.
In ergonomic terms, the hand access device replaces the assisting port but is substantially larger to accommodate the intracorporeal hand. However, the ergonomic setup in HALS has two main constraints. First, there is a significant reduction of the internal and external workspace compared with the total laparoscopic approach. The size of the intracorporeal hand encroaches on the workspace in the peritoneal cavity, whereas the external workspace is reduced by the size of the hand access device and the proximity of surgeon’s trunk, with the surgeon becoming anchored to the abdomen of the patient by his or her intracorporeal hand. The reduction in workspace creates difficulty in port placement. Applying the definition of the manipulation angle to HALS, it refers to the angle between the axis of the inserted forearm–hand and the axis of the external instrument. To date, no ergonomic studies on the optimum location of the hand access device in HALS have been reported.
Second, there is a discrepancy in the hand-to-target distance between the extracorporeal and intracorporeal limbs in HALS. This results in an awkward posture of the surgeon, who adopts a lordotic position, resulting in discomfort to the upper limbs. The problem is heightened by the static posture of the surgeon, with the forearm anchored to the hand port device for long periods during complex procedures. Consequently, during HALS, many surgeons experience back strain and muscle fatigue of the upper limbs.
Although this problem can be addressed by using the assistant’s hand intracorporeally or by having the assistant manipulate the instrument from outside, this approach depends heavily on the availability of an experienced assistant. An alternative approach is to use shorter instruments in the extracorporeal hand to reduce the discrepancy in the hand-to-target distance between the extra- and intracorporeal limbs. This allows the leading surgeon to control the movement of both the intracorporeal and extracorporeal instruments while minimizing the lordotic posture and muscle discomfort to the extracorporeal limb.
This study addressed the preceding two problems in two laboratory-based experiments by investigating the impact of different manipulation angles and extracorporeal instrument lengths on task performance and muscle workload for hand-assisted laparoscopic bowel suturing.
Materials and methods
Two experiments were carried out to investigate the influence of manipulation angle and instrument length on task performance. Ten right-handed surgeons with different clinical experience participated in each study. Each surgeon was instructed to close a 50-mm enterotomy of non-live porcine bowel inside a hand-assisted laparoscopic trainer. The quality of the task was assessed by the leaking pressure and suture placement error score. Efficiency of performance was measured by the execution time. Muscle recruitment was measured by surface electromyography (EMG).
Task
The standardized task consisted of closure via continuous suturing of 50-mm enterotomy of porcine bowel inside a dedicated hand-assisted laparoscopic trainer using a 3–0 18-cm braided polyester mounted on a 23-mm ESK needle (EL-415, Polysorb; United States Surgical Corporation, Norwalk, Connecticut, USA). A 10-cm-long porcine bowel with its attached fan-shaped mesentery was cleansed thoroughly with tap water. The bowel was fixed on a wooden block covered with a nonreflective cloth, with the surface of the block angulated 30° to the horizontal plane. The center of the enterotomy corresponded to the center of the block, with the longitudinal axis of the bowel and the block aligned.
Video endoscopic equipment
The videoendoscopic system (Karl Storz, Tuttlingen, Germany) consisted of a forward-viewing endoscope 10 mm in diameter coupled to a single-chip camera (Endovision 9050-PB; Karl Storz, Tuttlingen, Germany) and a high-resolution monitor (Model PVM-1443MD; Sony, Tokyo, Japan). A cold light source (Model 450-V) was connected to a fiberoptic light cable 3.5 mm diameter and 180 cm in length (Model 495NL). The hand access device was the Omniport (Advanced Surgical Concepts Ltd, Dublin, Ireland).
Variables for investigation
In the first experiment, 45°, 60°, 75° or 90° manipulation angles were studied, whereas in the second experiment, two shaft lengths were investigated: short shaft (250 mm) and standard-length shaft (330 mm).
Control measures
The ergonomics of the setup was standardized in all the experiments:
-
1.
The monitor was placed on a stand of adjustable height so that the center of the monitor corresponded to the eye level at a distance of 50 in.
-
2.
The trainer was placed on a table with adjustable height so that the table surface was 10 cm below the elbow level of the subject’s extracorporeal limb and the enterotomy lay along the sagittal plane.
-
3.
A forward-viewing 0° endoscope (Karl Storz) was introduced to subtend an optical axis-to-target angle of 90° with a 75-mm distance between the end of the endoscope and the bowel specimen. The endoscope was readjusted as required by the assistant to maintain the area of interest in the middle of the field as suturing progressed.
The ideal manipulation angle identified in the first experiment was used in the second study to place the needleholder and the hand port so that the angle between the needleholder-to-target axis and the hand-to-target axis equaled 60°. The location of each port was calculated using the AutoCAD 2002 software (Autodesk Inc., San Rafael, CA, USA), which gave the exact location of each port in (x,y,z) coordinate.
Experimental procedure
Before the start of each experiment, each surgeon had a familiarization session. All the participants completed all tasks within the same day, with a 10-min rest interval between each task. The nondominant hand was inserted through the Omniport, which was inflated to a pressure of 12 mmHg, and a standard plain forceps was used by the intracorporeal hand for assistance. The participants were instructed to use the standard seromuscular continuous technique, starting and finishing with a three-throw, square intracorporeal knot. They also were instructed to obtain a watertight closure and to place the suture exactly 3 to 5 mm apart and from the enterotomy edge.
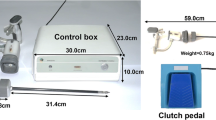
During task performance, each participant was attached by surface electromyography electrodes (3M Red Dot; 3M United Kingdom PLC, Bracknell, UK) to the extracorporeal dominant forearm extensor, forearm flexor, arm extensor, arm flexor, and deltoid and trapezius muscle groups as well as to the nondominant trapezius and deltoid muscle groups of the intracorporeal limb. The EMG signals were collected using the MT8 Biomedical Radio Telemetry system (MIE Medical Research Ltd, Leeds, UK). The signals gained then were full-wave rectified, low-pass filtered, and integrated over the total execution time by the dedicated software (MyoDat 5.0; MIE Medical Research Ltd, Leeds, UK). These represent the area under the curve, which can be translated into the work done by each muscle group.
In the first experiment, each participant carried out one task with each of the manipulation angles (45°, 60°, 75°, and 90°) and an equal azimuth angle in a random sequence. The participants used instruments of standard shaft length with the extracorporeal dominant hand.
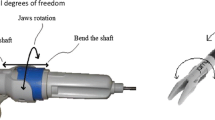
In the second experiment, the participants used the dominant hand to manipulate the Szabo-Berci needleholder “Parrot Jaws” (26173SC, Karl Storz) with a ringed pistol-grip handle but no ratchet. Two shaft lengths were investigated: the short shaft (250 mm) and a standard-length shaft (330 mm). Each participant completed six tasks with each instrument length in two sessions. The sequence of the instrument length was randomized for each participant, for a total of three tasks with every instrument length in each session.
Outcome measures
Execution time (s) was defined as the interval from the time the subject started to drive the needle for the first stitch until the instruments were released at task completion.
Leaking pressure (mmHg) was measured by using a simple colored water manometry U-tube system with an inflow tap at one end of the sutured enterotomy, at which colored water started to leak from any part of the suture line.
The suture placement error score (mm) was the summation of the vertical and horizontal deviation in millimeters from exact suture placement.
Integrated electromyography (mV s) was the summation of EMG signals from the muscle during the test after they had been full-wave rectified and low-pass filtered.
Statistical analysis
In the first experiment, the Friedman test was used for statistical analysis except for the execution time data, which were analyzed by repeated measures analysis of variance (ANOVA). In the second experiment, univariate ANOVA was used for analysis of the execution time data, and the Wilcoxon signed rank test was used to compare the remainder of the data. The significance level was set at a p value less than 0.05.
Results
Experiment 1
The mean execution time was significantly shorter when the 45° and 60° manipulation angles were used (p < 0.05), as compared with the 90° angle (p < 0.01). There were no significant differences in leaking pressures or suture placement error scores among the manipulation angles of 45°, 60°, 75°, and 90° (Table 1).
The median workload by the deltoid of the extracorporeal dominant limb and the intracorporeal nondominant limb was higher with the 90° manipulation angle than with the 45° and 60° manipulation angles. Also, the median work done by the arm extensor and flexor muscle groups of the extracorporeal dominant limb was greater with the 90° manipulation angle. Moreover, the median work done by the trapezius of the extracorporeal dominant limb was greater with the 90° angle than with the 75° angle. There was no significant difference in the workload of the other muscle groups between the different manipulation angles (Table 2).
Experiment 2
The mean execution time ± standard error of the mean was significantly shorter when the short instrument was used (572.05 ± 28.87 s vs 618.75 ± 30.25 s, respectively; p < 0.01). However, there were no significant differences between the short and standard instruments in the leaking pressures (11.76 ± 12.50 vs 11.03 ± 10.29 mmHg; p = 0.833) or in the suture placement error scores (18.05 ± 17.45 mm vs 17.50 ± 16.25 mm; p = 0.192).
The muscle workload of the extracorporeal dominant forearm extensor, forearm flexor, and deltoid as well as the deltoid of the intracorporeal nondominant limb was significantly lower with the use of the short instrument than with the standard-length instrument (p < 0.05, p < 0.05, p < 0.01, and p < 0.05, respectively) (Table 3).
Discussion
Although HALS enhances task performance by use of the intracorporeal hand as an instrument with tactile feedback and 21 degrees of freedom of movement, the reduction in workspace and the surgeon’s awkward posture impose considerable ergonomic constraints on the surgeon. This study showed that the best ergonomic setup in HALS entails a manipulation angle of 45° to 60° and use of a shorter shaft instrument than standard laparoscopic length.
The first experiment found that the shortest execution time was achieved using the manipulation angles of 45° and 60° without compromising the quality of task performance. Moreover, the greatest workload by the extracorporeal dominant deltoid and trapezius and the nondominant deltoid and trapezius of the intracorporeal limb was encountered with the 90° manipulation angle. There also was an increase in the muscle work of the extracorporeal dominant arm extensor and flexor as a consequence of the wider manipulation angle.
Research on the choreography of surgeons’ movement using motion analysis showed different patterns of shoulder movements adopted by experts and trainees for intracorporeal endoscopic knot tying [2]. Expert surgeons had a higher angular velocity and a wider movement with more adduction at the dominant shoulder joint than trainees. This choreography of movements by experts was associated with better task quality and efficiency than demonstrated by trainees. Apparently, limiting the abduction of the shoulder joint enabled the experts to use their arms more efficiently.
In our experiments, a wide manipulation angle resulted in more abduction of the surgeon’s shoulder joints. As a consequence, the movement of the arms was restricted with more workload at the deltoids, and subjects became more easily fatigued than with the more adducted shoulders.
In addition to the ergonomics of instrument angles that governs port location, the optimum port placement and the position of the operating team around the table depends on the role of the surgical team members in undertaking the procedure. The incision of the hand access port should be placed to allow easy reach of the intracorporeal hand to the operating target and ability to extend the wound for carrying out the procedure through the conventional open approach.
It is important to avoid placing the hand access device over the operative field. Otherwise, the internal hand may obstruct the view. In general, a peripheral location (in a specific quadrant) should be chosen if the manipulations of an operation are largely restricted to one quadrant, whereas the central (transverse or midline) location is preferable if the component steps of the operation involve more than one quadrant of the abdomen.
Also, the location of the optical port depends on whether the principal surgeon or the assistant inserts the hand into the abdominal cavity. When the principal surgeon uses the nondominant hand inside the abdomen while manipulating with the dominant hand externally, the workspace between the hands does not allow easy operation of the camera and the endoscope. In this case, one option is to place the optical port to one side of the principal surgeon’s hand. This represents off-optical axis work because both “instruments” are on one side of the laparoscope and its optical axis. The alternative is to place the laparoscope between the internal hand and the dominant external hand, but with the optical port further back from the hand access device.
There is less of a problem when the assistant inserts his or her hand inside the peritoneal cavity through the hand access device and the surgeon manipulates with both hands externally. In this instance, the workspace between the instruments permits insertion of the optical port in accordance with the ideal setup (i.e., the optical port lies between the two instrument ports and equidistant from them).
The second experiment demonstrates the benefits of using a short extracorporeal instrument in hand-assisted laparoscopic procedures to reduce the mismatch in the hand-to-target distance by the extracorporeal and intracorporeal limbs. This translates into a reduction in execution time and muscle workload without compromise in the quality of the task performance, as indicated by the suture placement error score and the leaking pressure.
Manipulation of standard instrument length by the extracorporeal hand imposes more muscle recruitment by the forearm flexor and extensor muscle groups. This higher muscle workload than with the shorter instrument is due to the awkward wrist position in the handling of long instruments. The increased abduction of the shoulder joint with standard instrument length results in more recruitment by the deltoid muscle of the extracorporeal limb. There also is more muscle recruitment in the deltoid of the intracorporeal limb because of the difficulty in shoulder movement incurred by the lordotic position imposed by the standard-length instrument.
In addition to the effect of extracorporeal instrument length on muscle workload, instrument length also determines the intracorporeal-to-extracorporeal instrument ratio. It is known that an intracorporeal-to-extracorporeal instrument length ratio of less than 1 impairs task performance in addition to being associated with a wider range of elbow and shoulder movement and a higher shoulder angular velocity [3].
In the current study, the standard-length instrument resulted in a lower intracorporeal-to-extracorporeal instrument ratio than the short instrument. This may account for the decrease in task efficiency, as indicated by the increased execution time.
Another method that can improve surgeons’ posture during HALS is use of the articulating handle [1] that permits adjustment of the angle between the handle and the shaft of the instrument (Rocker adjustable universal handle; Karl Storz). With this handle, the surgeon can adjust the angle between the instrument axis and the forearm–hand axis by altering the angle between the handle and instrument shaft. Further work is needed to investigate the optimum extracorporeal instrument length and its relation to the surgeon’s build and the height of the operating table.
References
Emam TA, Frank TG, Hanna GB, Stockham G, Cuschieri A (1999) Rocker handle for endoscopic needle drivers: technical and ergonomic evaluation by infrared motion analysis system. Surg Endosc 13:658–661
Emam TA, Hanna GB, Kimber C, Cuschieri A (2000) Differences between experts and trainees in the motion pattern of the dominant upper limb during intracorporeal endoscopic knotting. Dig Surg 17:120–123
Emam TA, Hanna GB, Kimber C, Dunkley P, Cuschieri A (2000) Effect of intracorporeal–extracorporeal instrument length ratio on endoscopic task performance and surgeon movements. Arch Surg 135:62–65
Acknowledgments
The author is grateful to all surgeons who participated in the study and thanks Mrs. Lorna Christie, Miss Susan Farrell, and Mr. William Davie from the Cuschieri Skills Centre, Ninewells Hospital and Medical School, Dundee for their support. The author also thanks the Royal Thai Government for providing support.
Author information
Authors and Affiliations
Corresponding author
Additional information
The study of manipulation angle was presented at the 12th International Congress of the European Association for Endoscopic Surgery (EAES) and Other Interventional Techniques, Barcelona, June 2004; the experiment on instrument length was presented at the Technology Award Session, the 13th International Congress of the EAES, Venice, June 2005.
Rights and permissions
About this article
Cite this article
Manasnayakorn, S., Cuschieri, A. & Hanna, G.B. Ideal manipulation angle and instrument length in hand-assisted laparoscopic surgery. Surg Endosc 22, 924–929 (2008). https://doi.org/10.1007/s00464-007-9520-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-007-9520-5