
Abstract
Background
Distorted haptic feedback by the surgical instrumentation is a major problem in minimally invasive surgery (MIS). Friction force generated by the rubber seal in the trocars masks the haptic information needed to perceive the properties and structure of the target tissue, resulting in an increased haptic perception threshold in naïve subjects. This can lead to over application of forces in surgery.
Objective
This paper examines the effect of surgical experience on the psychophysics of force perception and force application efficiency in MIS.
Method
A controlled experiment was conducted using a mixed design, with friction and vision as independent within-subjects factors, experience as a between-subjects factor, and applied force and detection time as dependent measures. Fourteen subjects (eight novices and six experienced surgeons) performed a simulated tissue probing task. Performance data were recorded by a custom-built force-sensing system.
Results
When friction was present, higher thresholds and longer detection times were observed for both experienced and inexperienced subjects. In all cases, experienced surgeons applied a greater force than novices, but were quicker to detect contact with tissue, resulting in higher force application efficiency.
Conclusion
Surgeons seem to have adapted to the higher threshold in haptic perception by reacting faster, even while applying more force to the tissue, keeping within the limits of safety.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
It is very important for surgeons to be able to touch and feel the tissue while operating since the sense of touch is one of the primary sources of information that guides the surgeon during surgery [1]. However, in minimally invasive surgery, direct contact is replaced by long instruments between the tissue and fingers [2], resulting in reduced and distorted haptic (kinesthetic and tactile) feedback [3]. This can lead to changes in how the surgeon interacts with the tissue, especially in the application of forces while manipulating tissue.
One contributing factor to the distortion of haptic feedback in MIS is the trocar. The rubber seal within the trocar fits tightly around the instrument to maintain pressure within the insufflated body cavity. It also generates friction forces when the surgical instrument rubs against the rubber. These friction forces are detrimental to the utility of force feedback, especially during rapid tool movements [4, 5, 6]. The friction forces are also dependent on the type of trocar, the movement velocity, and the movement direction. A recent study [7] showed that, for most trocars, large fluctuations in forces occur at the beginning of tool movement or when the movement direction reverses. Specifically, trocars with narrow or thick sealing caps generate a high amount of friction. At movement reversals, high variance of friction fluctuation can deteriorate surgical performance during high-precision tasks, which typically involve many changes in movement direction (e.g., tissue manipulation).
For a surgeon to get useful force information from the surgical site during probing and dissecting, he or she must be able to accurately differentiate between seal friction and tissue contact forces. According to Weber’s law [8], the just-noticeable difference in a stimulus is proportional to the magnitude of the original stimulus. Because the contact forces between tool and tissue are on the same order of magnitude as the amount of friction in the system [6,9], the surgeon would have to press harder in order to perceive a difference in tissue resistance above the level of the friction force.
With experience, MIS surgeons have learned to compensate, to a limited extent, for the distorted haptic feedback by relying primarily on visual cues. However, visual feedback in MIS is also distorted, with only two-dimensional (2D) views of a restricted surgical site. Furthermore, processing the haptic information through the visual channel is not only inefficient, but may be overloading the already limited resources for the visuospatial tasks in surgery [10]. Data in the literature indicate that injury to the bile ducts during cholecystectomy occurs at a rate of 0.41–1.1% [11], compared to 0–0.4% in open surgery [12], which is three times higher than in open surgery [13, 14, 15]. Therefore, a conservative estimate of 500,000 annual laparoscopic surgeries means that there are 2,000 bile duct injuries per year [16]. Other research suggests that injury rates have not improved with time or experience [11]. A recent study [17] suggests that the misidentification of biliary anatomy stems principally from misperception, not errors of skill, knowledge, or judgment. Way et al. believe that loss of haptic perception is the most important contributor to such errors and that the restoration of haptic cues can help guide the surgeon to the cystic duct when it is otherwise difficult to see or identify.
Our previous research [18] showed that, in simulated tissue probing and differentiation tasks, higher force perception threshold, longer detection time, and more errors were observed when force feedback from tissue was masked by trocar friction. However, these studies observed only naïve subjects who had no prior experience in medicine or surgical simulators. There is conflicting evidence in the literature of whether experience in laparoscopic surgery affects the psychophysics of force perception. One study showed that surgeons perform better than non-surgeons when differentiating soft tissue [19], while another showed no significant differences between the two groups [20]. A third study showed that the performance of experienced surgeons was superior to that of interns when identifying shapes and determining tissue consistency, but that there was no difference in texture identification [21]. Generally, these results suggest that the superior performance seen in the experienced surgeons represents learning. Although it is true that experienced surgeons may have acquired strategies to overcome, to varying degrees, the effects of friction in the system, these tactics employ the visual system to sense haptic information, two independent modalities with separate processing areas in working memory [10]. These adaptations demand additional processing that is ill-suited to the inherent abilities of the visual sense and may be unnecessarily overburdening the visual system while leaving the more-suitable haptic sense underutilized [18].
The objective of this research was to determine whether experience in laparoscopic surgery affects the psychophysics of force perception. We hypothesized that experience would improve surgeons’ performance in tissue contact detection when visual feedback is available, such that their force perception threshold would be lower and force perception would be more efficient. However, experienced surgeons’ pure force perception (without visual feedback) threshold would be similar to novices. A controlled experiment was conducted, using simple tissue probing task in a psychophysical paradigm. Force perception threshold is defined as the minimum force required to perceive contact with target tissue. Force application efficiency is defined as the inverse of the amount of time from making physical contact to when the subject perceives contact.
Methods
Subjects
Fourteen subjects with varying levels of surgical experience participated in this study. The eight novices were undergraduate students at Tufts University, while the six experts were surgical residents (two PGY1s, two PGY2s, one PGY4, and one PGY5) from the Tufts New England Medical Center. All subjects provided informed consent.
Simulated surgical environment
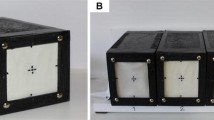
A wooden box was used to simulate the patient’s abdomen. A 10-mm US Surgical Surgiview Laparoscope set at 37° from vertical and a Stryker 777 camera were used to visualize the inside of the box. A 5/12-mm Origin convertible trocar set at 5 mm was mounted on a guide board (see Fig. 1). A 5-mm-diameter US Surgical AutoSuture Endo Clinch II grasper, inserted through the trocar (friction condition), was used to probe target tissue. The trocar was removed in half the trials to simulate the frictionless condition. The abdomen (box) was illuminated by an intrinsic laparoscope optical fiber and an auxiliary lamp. A video monitor, positioned at eye level in front of the subject (not shown in Fig. 1) was turned on in the visual condition and off in the blind condition.

Experimental set up
Three sets of visually identical, homogeneous silicone gels (GE Silicones) were used to simulate organic tissue with different softness: hard, medium, and soft. The hardest gel approximated the compliance of liver tissue at 15 kPa, the medium gel was two times softer, and the soft gel approximated fatty tissue and was four times softer than the hardest gel.
Force-sensing device and data acquisition
A custom-built strain-gauge force sensing device with an accuracy of ±0.003 N was used to record force as a function of time. A force sensor was embedded in a cantilever bridge on which the gels were placed. Data were sampled at 100 Hz, processed by a data-acquisition card, and displayed in LabView.
Test protocol and experimental design
Subjects were allowed to become familiar with the apparatus prior to testing. They were given three practice trials at the beginning of each new condition. Subjects were instructed to behave as though the tissue probing task were actual surgery, probing with only enough force to just perceive contact (i.e., as little as possible) and minimizing the time in contact with the sample. They were presented with a single simulated tissue sample during each trial and instructed to move the grasper vertically toward the sample until contact was made. As soon as contact was felt, the subject was to cease pushing, retract the grasper, and return it to the supporting stand. The height of the sample was then altered by a random amount between trials to prevent the subjects from relying on their memory of sample position. A short break was given between conditions.
A 2 vision × 2 friction × 3 softness × 2 experience mixed design was used. Each subject completed 10 trials per condition for a total of 120 trials. The order of tissue softness was randomized, and the order of vision and friction conditions was counterbalanced.
Dependent measures and analysis
Applied force and contact time were recorded. Applied force was defined as the maximum force applied to the sample, equivalent to the force perception threshold. Contact time was defined as the elapsed time from initial contact until final withdrawal began.
A four-way analysis of variance was performed using an alpha value of 0.05. Preplanned paired sample t-tests were performed on individual pairs of means in the four vision × friction conditions: extreme conditions — blind-friction (BF) and vision-no-friction (VNF); blind conditions — BF and blind-no-friction (BNF); vision conditions — vision-friction (VF) and VNF; and intermediate conditions — BNF and VF. In BF, subjects had no visual feedback (blind) and trocar friction was present. In BNF, subjects were blind but trocar friction was removed. In VF, subjects had the benefit of vision but trocar friction was present. In VNF, subjects had visual feedback but trocar friction had been removed. Preplanned paired sample t-tests were also conducted on two pairs of means for novices and experienced surgeons in each of the four conditions mentioned above. Tukey’s honestly significant difference (HSD) was used as the post hoc test.
Results
Applied force
There were significant main effects of vision [F(1, 138) = 143.0, p < 0.001], friction [F(1, 138) = 134.2, p < 0.001], softness (F(2, 276) = 39.4, p < 0.001] and experience [F(1, 138) = 108.5, p < 0.001] on the maximum applied force (see Fig. 2). Post hoc analysis of the softness main effect showed a significant difference between hard and soft conditions (p < 0.001) but not between hard and medium, or soft and medium conditions. There was a significant interaction between vision and friction [F(1, 138) = 22.3, p < 0.001], with a larger increase in applied force in the blind conditions than in the visual conditions when friction was present compared to no friction. There was also a significant interaction between friction and experience [F(1, 138) = 12.9, p < 0.001], softness and experience [F(2, 276) = 10.1, p < 0.001]. Significant three-way interactions among vision, friction, and experience [F(1, 138) = 11.0, p < 0.001], vision, softness, and experience [F(2, 276) = 3.5, p < 0.04] were also observed.

Applied force of novice and experienced subjects under different vision and friction conditions
Paired sample t-tests of the vision and friction conditions across experience levels showed a significant difference between each of the four pairs of means that were considered: extreme conditions: BF and VNF, t(419) = 21.3, p < 0.001, BF and BNF, t(419) = 14.4, p < 0.001, VF and VNF, t(419) = 7.1, p < 0.001, BNF and VF, t(419) = 4.6, p < 0.001.
Paired-sample t-tests of the experience conditions showed a significant difference between novice and experienced surgeon in all four vision × friction conditions. In BF, t(179) = 12.4, p < 0.001; in BNF, t(179) = 12.1, p < 0.001; in VF, t(179) = 13.0, p < 0.001; and in VNF, t(179) = 9.8, p < 0.001.
Contact time
There were significant main effects of vision [F(1, 138) = 71.6, p < 0.001], friction [F(1, 138) = 168.5, p < 0.001], softness [F(2, 276) = 87.3, p < 0.001], and experience [F(1, 138) = 48.2, p < 0.001] on contact time (see Fig. 3). Post hoc analysis of the softness main effect showed a significant difference between the soft and hard conditions (p < 0.001), soft and medium conditions (p < 0.001), but not between the hard and medium conditions. There was a significant interaction between vision and friction [F(1, 138) = 75.4, p < 0.001], with longer detection time in the blind conditions than in the visual conditions when friction was present compared to no friction. There were also significant interactions between vision and experience [F(1, 138) = 66.6, p < 0.001], friction and experience [F(1, 138) = 49.0, p < 0.001], softness and experience [F(2, 276) = 17.4, p < 0.001], vision and softness [F(2, 276) = 67.6, p < 0.001], and friction and softness [F(2, 276) = 9.4, p < 0.001]. Significant three-way interactions were found among vision, friction, and experience [F(1, 138) = 45.7, p < 0.001], vision, friction, and softness [F(2, 276) = 37.2, p < 0.001]. A significant four-way interaction was found among vision, friction, softness, and experience [F(2, 276) = 33.6, p < 0.001].

Contact time of novice and experienced subjects under different vision and friction conditions
Paired-sample t-tests of the vision and friction conditions across experience levels showed a significant difference between each of the four pairs of means for contact time; BF and VNF, t(419) = 12.3, p < 0.001; BF and BNF, t(419) = 13.0, p < 0.001; VF and VNF, t(419) = 8.3, p < 0.001; and BNF and VF, t(419) = 6.8, p < 0.001.
Paired sample t-tests of the experience conditions showed a significant difference between novices and experienced surgeons in all four vision × friction conditions. In BF, t(179) = 9.9, p < 0.001; in BNF, t(179) = 8.0, p < 0.001; in VF, t(179) = 4.4, p < 0.001; and in VNF, t(179) = 4.3, p < 0.001.
Discussion
In this simple probing task, our results showed that, in general, experienced surgeons were faster at detecting contact with tissue than novices. However, they also applied a higher maximum force than novices, suggesting a higher force perception threshold. The latter result was unexpected, as we presumed that better performance is characterized by a lower maximum applied force.
Data reported in the literature showed that when manipulating tissue, novice surgeons applied higher force/torque than experienced surgeons [22]. This was attributed to insufficient dexterity of the novice surgeons, and represented a potential for tissue damage. The same study showed lower force/torque being applied by novice surgeons than by experienced surgeons during tissue dissection, which might indicate excessive caution to avoid irreversible tissue damage [22]. Since the probing task used in our study could be considered more similar to tissue dissection than manipulation, our results are consistent with those reported in the literature. That is, the task required subjects to advance the tool until the tip is in contact with tissue, as in dissection. Additionally, the higher force application during tissue dissection/probing may be due to the fact that surgeons have learned from experience the extent to which they can load the tissue without causing damage. Indeed, the documented tool tip – tissue interaction force with a trocar ranges from 0.1 to 10 N [6]. The force data in our experiment were well below the upper limit of this range, at an average of 3.6 N applied by the experienced surgeons.
In general, experienced surgeons applied 1.83 N more force (p < 0.001) and made contact with tissue 0.45 s shorter (p < 0.001) than novices in blind conditions; but they applied 1.51 N more force (p < 0.001) and made contact with tissue only 0.1 s shorter (p < 0.001) than novices in vision conditions. Also, when friction was present in the blind condition, experienced surgeons applied greater force and took longer in detection, even though the increases were smaller than for novices. Interestingly, and contrary to expectation, the effect of friction was more pronounced in vision conditions for experienced surgeons, whereas for novices, the effect of friction was more pronounced in blind conditions. When friction was present, experienced surgeons applied 63% more force in vision conditions and 41% more force in blind conditions. A possible explanation could be that experienced surgeons have become accustomed to using vision to process partial haptic information. Klatzky, Lederman and Reed have shown that the hardness of an object was relatively slowly encoded by joint haptic and visual exploration, and that visual explorers tended to perform minimal manual exploration, relying instead on visual cues [23]. Accordingly, the availability of vision may have substantially reduced hand movements and thus severely decreased the data available to the haptic modality for the experienced surgeons.
Of practical significance is the fact that the blind condition is representative of real situations in surgery in which the target tissue is obscured from view among other anatomy. In such visually impoverished conditions, the ability to detect tissue contact in spite of the masking friction would be important. Our results suggest that, with experience and practice, subjects have learned to overcome the poor perceptual conditions in minimally invasive surgery to some degree. Experienced surgeons are able to balance the criteria of speed and accuracy in force application to optimize efficiency, applying more force to complete the task quickly, without damaging the tissue.
Conclusion
Experience does seem to affect force detection threshold in laparoscopic surgery. Compared to novices, experienced surgeons have a higher force perception threshold than novices. However, they seem to be able to process the force information more quickly. Experience may also have resulted in a greater reliance on visual information to guide their force application. Nevertheless, the applied forces are within safety limits of tissue interaction.
References
Plinkert PK, Baumann I, Flemming E, Loewenheim H (1998) The use of a vibrotactile sensor as an artificial sense of touch for tissues of the head and neck. Minim Invasive Ther Allied Technol 7:111–115
Claus GP, Sjoerdsma W, Jansen A, Grimbergen CA (1995) Quantitative standardized analysis of advanced laparoscopic surgical procedures. End Surg 3:210–213
Den Boer KT, Herder JL, Sjoerdsma W, Meijer DW, Gouma DJ, Stassen HG (1999) Sensitivity of laparoscopic dissectors: what can you feel? Surg Endosc 13:869–873
Dubois P, Thommen Q, Jambon AC (2002) In vivo measurement of surgical gestures. IEEE Trans Biomed Eng 49:49–54
Lamata P, Gomez EJ, Sanchez-Margallo FM, Lamata F, Antolin M, Rodriguez S, Oltra A, Uson J (2006) Study of laparoscopic forces perception for defining simulation fidelity. Stud Health Technol Inform 14:288–292
Picod G, Jambon AC, Vinatier D, Dubois P (2005) What can the operator actually feel when performing a laparoscopy? Surg Endosc 19:95–100
van den Dobbelsteen JJ, Schooleman A, Dankelman J (2006) Friction dynamics of trocars. Surg Endosc Dec. 13, 2006
Boff KR, Lincoln JE (eds) (1988) Vibrotactile stimulation: Detectability of intensity differences. In Engineering data compendium: Human perception and performance. Wright-Patterson Air Force Base, OH: Harry G. Armstrong Aerospace Medical Research Laboratory 730–731
Rosen J, Hannaford B, MacFarlane MP, Sinanan MN (1999) Force controlled and teleoperated endoscopic grasper for minimally invasive surgery: experimental performance evaluation. IEEE Trans Biomed Eng 46:1212–1221
Baddeley AD (1996) Exploring the central executive. Q J Exp Psychol 49A:5–28
Adamsen PS, Hansen OH, Funch-Jensen P, Schulze S, Stage JG, Wara P (1997) Bile duct injury during laparoscopic cholecystectomy: A prospective nationwide series. J Am Coll Surg 184:571–578
Denzeil D, Millikan KW, Economou SG, Doolas A, Ko ST, Airan MC (1993) Complications of laparoscopic cholecystectomy: a national survey of 4,292 hospitals and an analysis of 77,604 cases. Am J Surg 165:9–14
Archer SB, Brown DW, Smith CD, Branum GD, Hunter JG (2001) Bile duct injury during laparoscopic cholecystectomy: results of a national survey. Ann Surg 234:549–559
Strasber SM, Hertl M, Soper NJ (1995) An analysis of the problem of biliary injury during laparoscopic cholecystectomy. J Am Coll Surg 180:101–125
Traverso LW (1999) Risk factors for intraoperative injury during cholecystectomy: An ounce of prevention is worth a pound of cure. Ann Surg 229:458–459
Hugh TB (2002) New strategies to prevent laparoscopic bile duct injury – Surgeons can learn from pilots. Surgery 132:826–835
Way LW, Stewart L, Gantert W, Liu K, Lee CM, Whang K, Hunter J (2003) Causes and prevention of laparoscopic bile duct injuries – Analysis of 252 cases from a human factors and cognitive psychology perspective. Ann Surg 237:460–469
Perreault JO, Cao CGL (2006) Effects of vision and friction on haptic perception. Human Factors 48:574–586
Bicchi A, Canepa G, De Rossi D, Iacconi P, Scilingo EP (1996) A sensorized minimally invasive surgery tool for detecting tissutal elastic properties. Proceedings IEEE International Conference on Robotics and Automation 1:884–888
MacFarlane M, Rosen J, Hannaford B, Pellegrini C, Sinanan M (1999) Force feedback grasper helps restore the sense of touch in minimally invasive surgery. J Gastrointest Surg 3:278–285
Bholat S, Haluck RS, Murray WB, Gorman PJ, Krummel TM (1999) Tactile feedback is present during minimally invasive surgery. J Am Coll Surg 189:349–355
Richards C, Rosen J, Hannaford B, Pellegrini C, Sinanan M (2000) Skills evaluation in minimally invasive surgery using force/torque signatures. Surg Endosc 14:791–798
Klatzky RL, Lederman SJ, Reed C (1987) There’s more to touch than meets the eye: The salience of object attributes for haptics with and without vision. J Exp Psychol 116:356–369
Acknowledgment
This work was supported by a career award from the National Science Foundation (#0238284) and the Tufts University graduate research fund. We would like to thank Tuan Nguyen for his assistance in collecting data. We also acknowledge J. O’Leary’s helpful guidance in building the force-sensing instrument.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Zhou, M., Perreault, J., Schwaitzberg, S.D. et al. Effects of experience on force perception threshold in minimally invasive surgery. Surg Endosc 22, 510–515 (2008). https://doi.org/10.1007/s00464-007-9499-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-007-9499-y