
Abstract
Background
Laparoscopic cholecystectomy is one of the most common operations in general surgery. It is performed by surgeons with a specialist interest in biliary disease as well as by surgeons with other specialist interests.
Methods
This retrospective audit of all cholecystectomies was conducted in a single hospital over a 10-year period from 1996 to 2005. Data were extracted from two independent electronic databases and supplemented by a full note review of cases with extended postoperative stay or unplanned readmission. The outcomes for cases under the care of specialist upper gastrointestinal (GI) consultants were compared with outcomes for cases of general surgery consultants from other firms.
Results
Data from 4,139 cholecystectomies were obtained. More cholecystectomies performed by upper GI firms were completed laparoscopically (96.2% vs 80.1%) with a higher rate of intraoperative cholangiograms (83.4% vs 16.9%). The mean operating time was shorter for upper GI cases (69 vs 84 min), as was the postoperative hospital stay (2 vs 3.6 days). There also was a significantly lower incidence of bile duct injury in upper GI cases (0.1% vs 0.9%).
Conclusion
In their institution, the authors found evidence of improved outcomes when laparoscopic cholecystectomy was performed under the care of surgeons with a specialist interest in upper GI or hepatopancreaticobiliary surgery.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Laparoscopic cholecystectomy was first performed by Muhe in Germany in 1986 [15] and subsequently developed independently by Mouret in France and McKernan in the United States [14]. Over the following decade it became the operation of choice for symptomatic gallbladder disease. Laparoscopic cholecystectomy is now one of the most common procedures performed by general surgeons, with more than 45,000 operations performed annually in England (Hospital Episode Statistics data). In the United Kingdom, laparoscopic cholecystectomy is performed both by surgeons with a special interest in upper gastrointestinal (GI) and/or hepatopancreaticobiliary (HPB) surgery and surgeons who specialize in other areas of general surgery.
This study aimed to audit the practice and outcomes of cholecystectomies performed in one unit over a 10-year period (1996 to 2005), and to determine whether the consultant specialty had any influence on surgical outcome.
Patients and methods
A retrospective audit was conducted at a large district hospital serving a population of 525,000. The electronic operating theater database was searched for all operations in which a cholecystectomy was entered into the database as one of the procedures performed. The information extracted from this database included basic patient details, the consultant responsible for the care of the patient, the surgeon and assistants who performed the operation, the procedures performed, and the times at which the patient entered and left the operating theater. Data included whether the procedure was completed laparoscopically, but in cases for which the procedure was not coded as laparoscopic, it often was not clear whether the operation was started laparoscopically and converted or planned as an open procedure. Information extracted from this database was checked manually by case note review where appropriate. Cases were coded into two groups: operations performed under the care of an upper GI surgeon (upper GI) and those performed under the care of a surgeon with no specialist upper GI/HPB interest (other firm). Operations performed by pediatric surgeons and operations for which it was clear that cholecystectomy was not the primary procedure performed (e.g., cases in which pancreaticoduodenectomy or hemicolectomy also was performed) were excluded from the audit.
The included cases then were matched to information in the electronic hospital coding database. This allowed data on the method of admission (elective or emergent), date of discharge, and date of death to be extracted. Combined data from both the theater database and the hospital coding database were stored in an Excel spreadsheet (Microsoft Corp. Redmond, WA, USA).
To gain further information on surgical complications, a review of clinical notes was attempted in all cases for which the postoperative stay exceeded 4 days or death occurred within 30 days of surgery. In addition, a list of patients readmitted to the hospital on an emergency basis within 30 days of surgery also was obtained from an electronic hospital database (this information was available only for cases since 2000), and notes on these patients also were reviewed. If after full review of the case notes it was clear that cholecystectomy was not the primary procedure, the case was excluded from the audit. Data regarding perioperative and postoperative complications were added to the Excel spreadsheet.
Statistical analysis was performed using SPSS 13.0 software (SPSS Inc. Chicago, IL, USA). Continuous data, reported as mean ± standard deviation or median and interquartile range, were compared between groups using the unpaired t-test or the Mann–Whitney U test. Categorical data were compared using Fisher’s exact test. All p values less than 0.05 were considered statistically significant.
Results
In 1996, the hospital employed eight consultant general surgeons, one of whom specialized in upper GI/HPB surgery, and all of whom performed laparoscopic cholecystectomy. By the end of 2005, 16 consultant general surgeons were on the staff (including 3 upper GI/HPB surgeons), 12 of whom were performing laparoscopic cholecystectomy.
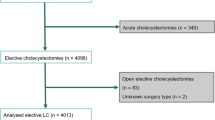
Between 1996 and 2005, 4,139 cholecystectomies were performed in which cholecystectomy was the primary procedure. Data were available from both the theater and the coding electronic databases for these procedures (Fig. 1). The number of cholecystectomies performed annually ranged from 307 to 487 during this period. Of the 423 cholecystectomies performed in 1996, 161 (38%) were performed under the care of the specialist upper GI surgeon. In 2005, 455 cholecystectomies were performed, 292 (64%) under the care of one of three upper GI/HPB surgeons.

Flow chart describing audit methodology.
Overall, 89% of the cases were elective admissions, and this proportion did not significantly differ over the 10-year period (p = 0.136, chi-square test). There was no significant difference in the proportion of elective admissions between the cases managed by the upper GI firm and those managed by the other firms (Table 1). The proportion of female patients was 74%, and this did not differ significantly between upper GI and other firms. The mean age of patients treated by the upper GI firm was 54 years as compared with 56.2 years for patients treated by the other firms (p < 0.001).
Overall, 89% of the cases were completed laparoscopically. Significantly more cases managed under the upper GI firm were completed laparoscopically than cases managed under the other firms. Elective admissions were significantly more likely to be managed laparoscopically than emergency admissions. Among cholecystectomies performed by the upper GI team, 97.1% of the elective admissions were managed laparoscopically, compared with 89.1% of the emergency admissions, and these rates remained fairly steady throughout the 10-year period. For the other firms, 43.3% of the emergency admissions were managed laparoscopically, compared with 84.6% of the elective admissions overall, although this rate improved significantly over the 10-year period (Fig. 2).

Trends with time in the proportion of cholecystectomies completed laparoscopically by the firm group and the method of admission.
The mean theater time was 75.6 min overall. The theater time was significantly shorter for upper GI cases than for other firm cases. On the average, cholecystectomy for emergency admissions took 17 min longer than surgery for elective admissions. Cholangiograms were performed and recorded on the theater database for 54.1% of the cases overall. The upper GI firm performed a cholangiogram in a significantly higher proportion of cases than the other firms.
Over the 10-year period, the mean postoperative stay fell from 3.8 days in 1996 to 2.1 days in 2005 (Fig. 3). The overall mean postoperative stay was 2.7 days, and was significantly shorter for upper GI cases than for other firm cases. The postoperative stay was shorter in upper GI cases for both elective (1.7 vs 3 days; p < 0.001) and emergency admissions (3.9 vs 8.7 days; p < 0.001). The postoperative stay also was shorter for upper GI cases if the analysis included only the cases managed laparoscopically (1.8 vs 2.3 days; p < 0.001).

Trends with time in the postoperative hospital stay by the firm group.
The overall 30-day mortality rate was 0.6% and did not differ significantly between upper GI cases and cases managed by other firms. The case notes for the patients who had a postoperative stay longer than 4 days after a primary cholecystectomy or who died within 30 days of surgery were sought to discover perioperative complications. The notes for 519 of these patients (87.6%) were found and reviewed. Details are shown in Table 2.
Between 2000 and 2005, 121 patients were readmitted for an emergency in the month after a cholecystectomy. The case notes of these patients were reviewed, and the results are shown in Table 3. Overall, patients were readmitted at a rate of 4.6%. There was a trend toward a higher readmission rate among upper GI patients, but this trend was not statistically significant. Of the patients who were readmitted, 57.9% needed no interventional radiologic or surgical treatment.
Complications discovered from the note reviews of patients who had an extended postoperative stay and those readmitted were combined (Table 4). The patients treated before 2000 are excluded from Table 4 because readmission data were not available for this period.
Overall, the rate of bile duct injury (unintentional damage to the common bile duct or major hepatic ducts) was 0.4% during this period and significantly lower for upper GI patients. A postoperative bile leak was experienced by 1.9% of the patients, which prolonged the hospital stay or caused readmission, whereas 1.2% of the patients had a bile leak that required either surgical or radiologic intervention. There was no significant difference in the incidence of bile leak between upper GI and other firm patients. Significantly fewer upper GI patients experienced an intraabdominal collection (causing a prolonged hospital stay or readmission and confirmed radiologically, but with no evidence of a bile leak) than other firm patients. There was no significant difference in the rate of complications requiring further surgery between the groups.
Discussion
Over the 10-year period of this audit, the number of cholecystectomies performed in the studied unit has remained relatively steady, as has the proportion managed as emergency admissions. However, as a result of consultant appointments during the 10-year period and a greater degree of specialization within the general surgical department, a larger proportion of cholecystectomies currently are performed under the care of consultants with a declared specialist interest in upper GI or HPB surgery.
Overall, we have found that cases managed under the upper GI firm had a shorter theater time and were more likely to be completed laparoscopically than cases performed by other firms. There also was a lower rate of bile duct injury, and the postoperative hospital stay was significantly shorter. Although the proportion of emergency admissions was similar between the groups, the average age of upper GI patients was slightly more than 2 years less. Because this was a retrospective audit, it is likely that there was some degree of heterogeneity between the two groups of patients. However, any difference in case mix is likely to be biased against the upper GI firm because potentially more complicated patients likely were referred to the surgeons specializing in biliary surgery. In addition, more operations in the upper GI group were performed by consultant surgeons. However, univariate analysis suggested that although the mean operating time was shorter when a consultant was the primary surgeon (by 19 min), this was independent of a significant effect of the firm on the operating time.
Although there has been a progressive reduction in the conversion rate for elective laparoscopic cholecystectomies performed by non–upper GI firms, over the period of the audit, the overall conversion rate was significantly higher, and this partly explains the difference in postoperative stay between the groups.
Overall, there was a difference of 1.6 days in the mean postoperative hospital stay between the two groups. This represents a significant economic cost for an operation performed as frequently as laparoscopic cholecystectomy. In the other firms group, a large proportion of patients with an extended hospital stay did not have any specific complications, but were only recovering normally from an open procedure. However, even when analysis of postoperative stay is confined to cases managed laparoscopically, there still is a significant difference between the groups. More upper GI cases were managed on a day case basis, and it is also likely that for inpatient cases, the upper GI firm was more confident discharging patients earlier than other firms, who managed these patients on a less regular basis. Despite the earlier discharge of patients by the upper GI firm, the unplanned readmission rate was not significantly higher.
The findings of our audit are based on two parallel third-party collected databases and thus were not likely influenced by the surgeon’s input into cases. By covering a 10-year period and more than 4,000 cholecystectomies, we have been able to highlight small but significant differences such as bile duct injury rates that are infrequent but serious complications of laparoscopic cholecystectomy.
By selecting patients with an extended postoperative stay or readmission for detailed manual note review, we aimed to discover the majority of the major complications in the group of patients as a whole without relying on specific diagnostic codes in an electronic database. However, it is possible that some patients with complications were discharged within 4 days of the operation, or presented later than 1 month after the operation. Also, because we were unable to review all the notes we sought (because of notes destroyed, lost, tracked incorrectly, or in use by different departments), it is possible that some major complications may have been missed by this audit.
Another source of error in this audit was the quality of the information on the databases we used. All the cases included in this audit were on both the theater database and the hospital coding database. It is clear that there were cases available only on one of these databases (e.g., due to incorrect coding of the procedure, incorrect entry of patient details, or technical failure), and these cases were not included. However, there is no reason to suspect that these errors affected the one group of patients more than the other.
Bile duct injury after cholecystectomy is often a serious complication associated with significant morbidity and should be regarded as preventable [1]. Population-based studies have suggested a significant increase in the incidence of bile duct injuries related to performance of laparoscopic rather than open cholecystectomy [4, 5]. In this audit, we discovered 17 major bile duct injuries over the whole 10-year period (0.4%), with 10 in the period 2000–2005 (0.4%). All bile duct injuries occurred during operations attempted laparoscopically. Of all bile duct injuries, 13 were discovered intraoperatively, with 10 repaired primarily and 3 managed using a hepaticojejunostomy.
Four major bile duct injuries (all of them non-Upper GI firm cases) presented postoperatively. It is possible that the significantly lower rate for bile duct injury in upper GI cases reflects the higher use of perioperative cholangiogram in this group. Although still controversial, there is substantial evidence to suggest that by defining abnormal anatomy, the routine use of intraoperative cholangiography may reduce both the incidence and severity of bile duct injuries [2, 4, 5, 11, 12].
It has been shown that routine use of cholangiography is cost effective, particularly in the hands of inexperienced surgeons and in high-risk operations [6]. Although routine cholangiography was performed in all four cases of bile duct injury under the upper GI firm, cholangiogram ensured that these injuries were identified intraoperatively and repaired without significant long-term sequelae. In contrast, cholangiography had not been performed in any of the four cases of bile duct injury with delayed presentation, three of which required extensive reconstructive surgery and involved extended hospital stays with significant morbidity.
Although there was a significant difference between the groups, the overall rate of bile duct injury in this unit are line with previously published data. A metaanalysis of 83 single-institution studies in 1996 showed a common bile duct injury rate of 0.47% [16], whereas a prospective audit of laparoscopic cholecystectomies performed in the Rome area between 1999 and 2001 showed an average bile duct injury rate of 0.22%, with individual institutions having injury rates between 0% and 0.8% [8].
Our findings add to the growing evidence that the outcome for laparoscopic cholecystectomy may be influenced by expertise and special interest. Hobbs et al. [9] recently showed that both intraoperative cholangiography and surgeon experience are associated with fewer bile duct injuries. They found that surgeons who had performed fewer than 200 laparoscopic cholecystectomies in the previous 5 years were more likely to have complications than those who had performed more than this number of procedures.
Several other large population-based studies also have shown decreased rates of bile duct injuries associated with increased surgical experience [5, 7, 13]. Our findings agree with these results because cholangiography was much more likely to take place in the upper GI firm, with most surgeons in the other firms performing fewer than 40 procedures per year. However, other studies have not found a direct correlation between the number of procedures performed by a surgeon or team and the rate of bile duct injury [3, 8, 10], and these authors suggest that complications are related more to surgical technique than to crude surgical volume.
The question of who should perform laparoscopic cholecystectomy remains. Data from this audit suggest that when performed under the care of a surgeon with a specialist interest in upper GI or HPB surgery, the operations were performed more quickly with fewer conversions and bile duct injuries, and patients spent a shorter time in hospital. However, this audit was limited to a single unit, and care must exercised in generalizing these data to other institutions. Also, this is a historical audit and may not represent the current situation. Because more laparoscopic procedures are being performed by general surgeons for a variety of both elective and emergency operations, it is likely that surgeons with specialties other than upper GI are more skilled in laparoscopic surgery than they were at the beginning of the audit period in 1996.
In addition, it is difficult to ascertain whether the better results of the upper GI surgeons were attributable to their specialized training or solely to the larger number of cases they managed. It is possible that surgeons who are not specialists in biliary disease could achieve equally good results if they were allowed to increase their case load to that of the specialist surgeons.
We are not advocating that laparoscopic cholecystectomy be performed only by upper GI or HPB surgeons because this would significantly limit opportunities for other surgeons to gain the advanced skills necessary for performing laparoscopic colorectal or endocrine surgery. However, we do suggest as a minimum that surgeons who offer laparoscopic cholecystectomy should perform the operation regularly, should have an interest in laparoscopic surgery, and should be competent in performing techniques that may be necessary, including laparoscopic suturing and intraoperative cholangiogram. It also is necessary for a regular audit to be undertaken locally to ensure that in each hospital, patients are receiving optimal treatment.
References
Connor S, Garden OJ (2006) Bile duct injury in the era of laparoscopic cholecystectomy. Br J Surg 93: 158–168
Debru E, Dawson A, Leibman S, Richardson M, Glen L, Hollinshead J, Falk GL (2005) Does routine intraoperative cholangiography prevent bile duct transection? Surg Endosc 19: 589–593
Diamantis T, Tsigris C, Kiriakopoulos A, Papalambros E, Bramis J, Michail P, Felekouras E, Griniatsos J, Rosenberg T, Kalahanis N, Giannopoulos A, Bakoyiannis C, Bastounis E (2005) Bile duct injuries associated with laparoscopic and open cholecystectomy: an 11-year experience in one institute. Surg Today 35: 841–845
Fletcher DR, Hobbs MS, Tan P, Valinsky LJ, Hockey RL, Pikora TJ, Knuiman MW, Sheiner HJ, Edis A (1999) Complications of cholecystectomy: risks of the laparoscopic approach and protective effects of operative cholangiography: a population-based study. Ann Surg 229: 449–457
Flum DR, Dellinger EP, Cheadle A, Chan L, Koepsell T (2003) Intraoperative cholangiography and risk of common bile duct injury during cholecystectomy. JAMA 289: 1639–1644
Flum DR, Flowers C, Veenstra DL (2003) A cost-effectiveness analysis of intraoperative cholangiography in the prevention of bile duct injury during laparoscopic cholecystectomy. J Am Coll Surg 196: 385–393
Flum DR, Koepsell T, Heagerty P, Sinanan M, Dellinger EP (2001) Common bile duct injury during laparoscopic cholecystectomy and the use of intraoperative cholangiography: adverse outcome or preventable error? Arch Surg 136: 1287–1292
Gentileschi P, Di Paola M, Catarci M, Santoro E, Montemurro L, Carlini M, Nanni E, Alessandroni L, Angeloni R, Benini B, Cristini F, Dalla Torre A, De Stefano C, Gatto A, Gossetti F, Manfroni S, Mascagni P, Masoni L, Montalto G, Polito D, Puce E, Silecchia G, Terenzi A, Valle M, Vita S, Zanarini T (2004) Bile duct injuries during laparoscopic cholecystectomy: a 1994–2001 audit on 13,718 operations in the area of Rome. Surg Endosc 18: 232–236
Hobbs MS, Mai Q, Knuiman MW, Fletcher DR, Ridout SC (2006) Surgeon experience and trends in intraoperative complications in laparoscopic cholecystectomy. Br J Surg 93: 844–853
Krahenbuhl L, Sclabas G, Wente MN, Schafer M, Schlumpf R, Buchler MW (2001) Incidence, risk factors, and prevention of biliary tract injuries during laparoscopic cholecystectomy in Switzerland. World J Surg 25: 1325–1330
Ludwig K, Bernhardt J, Steffen H, Lorenz D (2002) Contribution of intraoperative cholangiography to incidence and outcome of common bile duct injuries during laparoscopic cholecystectomy. Surg Endosc 16: 1098–1104
Nickkholgh A, Soltaniyekta S, Kalbasi H (2006) Routine versus selective intraoperative cholangiography during laparoscopic cholecystectomy: a survey of 2,130 patients undergoing laparoscopic cholecystectomy. Surg Endosc 20: 868–874
Nuzzo G, Giuliante F, Giovannini I, Ardito F, D’Acapito F, Vellone M, Murazio M, Capelli G (2005) Bile duct injury during laparoscopic cholecystectomy: results of an Italian national survey on 56 591 cholecystectomies. Arch Surg 140: 986–992
Perissat J (1999) Laparoscopic cholecystectomy, a treatment for gallstones: from idea to reality. World J Surg 23: 328–331
Reynolds W Jr (2001) The first laparoscopic cholecystectomy. JSLS 5: 89–94
Shea JA, Healey MJ, Berlin JA, Clarke JR, Malet PF, Staroscik RN, Schwartz JS, Williams SV (1996) Mortality and complications associated with laparoscopic cholecystectomy: a meta-analysis. Ann Surg 224: 609–620
Author information
Authors and Affiliations
Additional information
Presented in part at the 10th World Congress of Endoscopic Surgery, Berlin, September 2006
Rights and permissions
About this article
Cite this article
Boddy, A.P., Bennett, J.M.H., Ranka, S. et al. Who should perform laparoscopic cholecystectomy? A 10-year audit. Surg Endosc 21, 1492–1497 (2007). https://doi.org/10.1007/s00464-007-9291-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-007-9291-z