
Abstract
Background
The purpose of this study was to analyze the published perioperative results and outcomes of laparoscopic (LVHR) and open (OVHR) ventral hernia repair focusing on complications and hernia recurrences.
Methods
Data were compiled from all English-language reports of LVHR published from 1996 through January 2006. Series with fewer than 20 cases of LVHR, insufficient details of complications, or those part of a larger series were excluded. Data were derived from 31 reports of LVHR alone (unpaired studies) and 14 that directly compared LVHR to OVHR (paired sudies). Chi-squared analysis, Fisher’s exact test, and two-tailed t-test analysis were used.
Results
Forty-five published series were included, representing 5340 patients (4582 LVHR, 758 OVHR). In the pooled analysis (combined paired and unpaired studies), LVHR was associated with significantly fewer wound complications (3.8% vs. 16.8%, p < 0.0001), total complications (22.7% vs. 41.7%, p < 0.0001), hernia recurrences (4.3% vs. 12.1%, p < 0.0001), and a shorter length of stay (2.4 vs. 4.3 days, p = 0.0004). These outcomes maintained statistical significance when only the paired studies were analyzed. In the pooled analysis, LVHR was associated with fewer gastrointestinal (2.6% vs. 5.9%, p < 0.0001), pulmonary (0.6% vs. 1.7%, p = 0.0013), and miscellaneous (0.7% vs. 1.9%, p = 0.0011) complications, but a higher incidence of prolonged procedure site pain (1.96% vs. 0.92%, p = 0.0469); none of these outcomes was significant in the paired study analysis. No differences in cardiac, neurologic, septic, genitourinary, or thromboembolic complications were found. The mortality rate was 0.13% with LVHR and 0.26% with OVHR (p = NS). Trends toward larger hernia defects and larger mesh sizes were observed for LVHR.
Conclusions
The published literature indicates fewer wound-related and overall complications and a lower rate of hernia recurrence for LVHR compared to OVHR. Further controlled trials are necessary to substantiate these findings and to assess the health care economic impact of this approach.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Incisional hernia is one of the most common major complications of abdominal surgery. In recent series with careful followup, the rate of incisional hernia after midline laparotomy has been 20% or higher [23, 26, 29, 33]. Because of their frequent recurrence, these hernias are associated not only with significant morbidity, but they also represent millions of dollars in yearly health care expenditures [10, 11]. Over the last 15 years, mesh repair techniques have replaced primary suture repair for the majority of incisional hernia repairs because of the high failure rate associated with primary repair [1, 6, 18, 19]. However, open incisional hernia repair can be a major operation with associated risks of wound- and mesh-related infections and hernia recurrence. As an alternative approach, laparoscopic incisional hernia repair was first reported in 1991 [16]. This technique is now being used increasingly in the management of patients with uncomplicated and more complex incisional hernias.
To date, close to 100 studies on laparoscopic ventral hernia repair (LVHR) have been published, although most represent small series of patients in uncontrolled and nonrandomized trials from single institutions. The aggregate data from these studies has not been carefully analyzed on a large scale and only a single meta-analysis involving a total of eight studies has been published [13]. To better understand the current status of LVHR and critically compare it to more traditional open techniques, we chose to examine the published literature and evaluate those studies that deal with either LVHR alone or in conjunction with open ventral hernia repair (OVHR). After surveying over 300 potential abstracts and critically evaluating 78 published reports, we performed an analysis of the pooled data from 45 studies with a focus on outcomes, complications, and recurrences.
Methods
Study selection
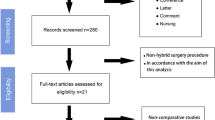
A Medline search was performed to identify all publications involving laparoscopic ventral hernia repair from January 1996 through January 2006. Publications containing the keywords ventral hernia, incisional hernia, umbilical hernia, and diastasis recti were identified and pooled; a similar search was also performed on the broad-based keyword laparoscopy. These two large groups were then combined to isolate those references common to both and were further limited to studies conducted in humans and published in English. This final limitation produced a total of 330 publications and their accompanying abstracts. A manual review of the bibliographies of several recent publications dealing with LVHR did not identify any additional citations within the defined time frame that were missed. Studies were excluded from consideration after review of the abstract if they contained fewer than 20 laparoscopic cases or if LVHR was not the primary focus of the work. This process produced a total of 78 published series that appeared to contain at least 20 subjects each and dealt primarily with LVHR.
These 78 studies were separated into series that compared patients who had undergone LVHR and OVHR within a given institution (“paired” studies) and series that described only patients who had undergone LVHR (“unpaired” studies). If a single group or institution had published multiple studies, then the largest series from the group was chosen for inclusion unless the studies involved distinct, nonoverlapping patient populations. If a group had published both a paired and an unpaired study, then the paired study was chosen for analysis. Each of the 78 studies was then independently evaluated by two of three reviewers for topical focus and completeness. Data extracted from each selected report included patient demographics, hernia etiology characteristics, perioperative details, postoperative complications, and hernia recurrence. All studies that provided sufficient detail regarding complications and recurrences were included in the analysis, even if other variables (i.e., mean hernia size) were missing. Any discrepancies were resolved by consensus after re-review of the primary data. This process led to the final selection of 45 total studies—14 paired and 31 unpaired. The studies used in this analysis are listed in Appendices 1 and 2.
Intraoperative parameters collected included operative time, hernia and mesh size, mesh vs. primary suture repair (for open cases), conversion to open repair (for laparoscopic cases), and complications such as bleeding and enterotomy. Postoperatively, data on length of hospital stay, complications, duration of followup, hernia recurrences, mortality, and cost of hospitalization were all examined. Information on complications related to the surgical procedure included wound problems, mesh infection, trocar site hernia, seroma, and need for early reoperation. Other postoperative complications were classified into the following categories: cardiac, pulmonary, gastrointestinal, genitourinary, thromboembolic, septic, neurologic/psychiatric, prolonged pain, and a miscellaneous category. Perioperative mortality rate was analyzed independently, but the principal cause of death was also included as a complication.
Statistical methods
Statistical analysis was performed by an independent statistician with two separate data sets because of the two different study types (paired studies that compared LVHR to open VHR and unpaired studies that involved LVHR only). Data from the paired studies were analyzed as the primary evaluation designated the paired analysis. In addition, data from the unpaired LVHR studies were combined with the LVHR data from the paired studies to create a “pooled LVHR” group. Pooled LVHR data were then compared to the open VHR data from the paired studies, which is designated as the pooled analysis. In three instances, a given group had published both a paired study and a more recent, larger, unpaired study that appeared to incorporate the LVHR cases from the smaller paired study. In these situations, the LVHR cases in the paired study were included in the paired analysis but were excluded from the combined analysis in lieu of the larger unpaired cohort.
The strategy behind this dual analysis (paired and pooled), was twofold: First, the paired analysis should have the greatest amount of internal validity because the same groups of surgeons were performing both the open and the laparoscopic cases. In addition, it is much more likely that the patients undergoing either LVHR or OVHR in these studies would have been drawn from the same respective patient populations. Second, comparing the results of the paired analysis to those derived from the tenfold larger LVHR group used for the pooled analysis allows for external validation and extrapolation to a more global patient population.
In several series, the patient populations were split into smaller subpopulations and mean values were given for these subgroups. In these instances, a conglomerate weighted mean was calculated and used in the final analysis. Likewise, many of the studies did not report standard deviations in their statistical analyses and thus weighted means were used to perform the calculations. Accordingly, a two-tailed t test was used to compare differences in these weighted means, and any studies that had missing data points were taken into account when performing the analysis.
Given that the raw numbers of complications, recurrences, and deaths were available in all the studies that were evaluated, these parameters were amenable to more thorough statistical analyses. Thus, totals for these data points were calculated for both the LVHR and OVHR groups and differences between them were determined using chi-squared analysis. Alternatively, Fisher’s exact test was used in the event that the number of data points was too small to allow for the use of a chi-squared algorithm.
Results
A total of 45 reports met the criteria for inclusion, including 14 paired studies (both LVHR and OVHR included) and 31 unpaired (LVHR alone). The majority of these studies were retrospective (n = 33, 73%), while three of the paired and nine of the unpaired studies were done in a prospective fashion (12 total, 27%). These reports encompassed a total of 5340 patients, including 4582 (86%) who had undergone LVHR and 758 (14%) who had OVHR. Of those 4582 patients who underwent LVHR, 619 (14%) were reported in paired studies and 87% were from unpaired studies.
Demographic data from the 45 included studies are shown in Table 1. In those studies that reported gender distribution, 44% of the patients undergoing LVHR in the pooled studies were male and 49% were male in the paired studies. Fifty-one percent of the open repairs were in males. The mean age of patients was 55.3 years in the LVHR pooled studies group, 52.9 years in the LVHR paired studies, and 56.1 years in the open VHR patients. (p = NS). Only 19 series reported body mass indices (BMI) for their patients, five of which were paired studies. In the five paired series, the weighted mean BMI was 30.5 for laparoscopic cases and 29.5 for the open cases (p = NS). In the pooled group, the LVHR patients had a somewhat higher mean BMI of 32.6 when compared to OVHR patients (p = 0.0026).
Each study was also examined for the numbers of primary vs. incisional hernias and recurrent hernias. Few series included all three data points, however, 12 of the 14 paired and 27 of the 31 unpaired studies documented the number of recurrent hernias that were operated on. Among the open group, 25.2% of the hernias were recurrent compared to 27.5% of those done laparoscopically in only the paired studies or 28.5% of cases from the combined laparoscopic group. Two paired studies [12, 34] that focused solely on umbilical hernias were included in the analysis. Both were paired studies and all of their open repairs were done using a mesh prosthetic. Conversely, two other paired studies [15, 28] reported repairing some of their smaller ventral hernias using a primary sutured technique. However, these 24 cases of primary closure represented only 4.4% of the total number of open repairs. All laparoscopic repairs were done using intraperitoneal mesh.
Operative data are shown in Table 2. The average operating time for the laparoscopic cases in the paired studies was 119.6 min, and 100.3 min when all the laparoscopic procedures are considered. The mean OR time for open repairs falls between these two times at 104.5 min. The hernia defect size (70.8 cm2) and size of the mesh used for repair (175.5 cm2) were smallest in the patients undergoing open herniorraphy. The values are somewhat larger (87.9 cm2 and 260.9 cm2) when compared directly to the patients undergoing laparoscopic repair in the same set of paired studies. However, the larger hernia and mesh sizes become even more apparent when all the laparoscopic cases in the pooled group are considered: 103.4 cm2 and 295.2 cm2 (p = 0.025 and 0.009), respectively. The enterotomy rate was significantly higher in paired LVHR cases compared to open VHR (2.9% vs. 1.2%). Postoperative length of stay was significantly shorter for the laparoscopic repairs, averaging 2.4 days in both paired and pooled LVHR groups compared to 4.3 days after open VHR (p = 0.015 and 0.0004, respectively).
The results of the complication analysis are shown in Tables 3 and 4 and in Fig. 1. Total complication rates were significantly higher with open VHR (41.6%) compared to LVHR for both pooled (22.7%) and paired (25.5%) analyses (p < 0.0001). In the analysis of complications by organ system in Table 3, the pooled LVHR studies reported significantly fewer wound, pulmonary, and GI complications compared to the open VHR series. Only total and wound complication rates were significantly different in the paired study comparison. No significant differences were noted for rates of cardiac, thromboembolic, urologic, or neurologic complications between any of the study groups. In the pooled LVHR group, prolonged postoperative pain was reported in a significantly greater percentage of patients (1.9%) compared to the open VHR group (0.92%); however, prolonged pain rates were similar for the open and LVHR paired series. Mortality rates were also similar between groups.

Total complications.
Wound complications were analyzed in more detail as shown in Table 4. Wound infection rates were 4.6–8-fold higher in the open vs. LVHR series for both pooled and paired study comparisons and accounted for most of the wound-related complications. The number of mesh infections was also significantly higher with open VHR for all comparisons. Interestingly, the incidence of postoperative seroma was similar for both open and laparoscopic series.
The rate of hernia recurrence (Fig. 2) was significantly lower with LVHR for both the pooled (4.3%) and the paired (3.1%) study cohorts compared to the paired open VHR series (12.1%, both p < 0.0001). Small variations existed in the length of followup reported in the three groups of studies (25.5 months for pooled LVHR, 16.9 months for paired LVHR, 20.2 months for OVHR), but these differences were not significant. The reported incidence of trocar site hernia in the laparoscopic series was only 0.35%.

Hernia recurrence.
Discussion
Although originally first described in 1991 [16], it is only in the last few years that laparoscopic incisional hernia repair has been increasingly utilized in the management of incisional hernias. Several large single and multi-institutional series have reported excellent results with few complications and recurrence rates generally less than 10% [3, 4, 8, 14, 17, 22, 27, 32]. However, to date there is only one prospective randomized controlled trial that compares laparoscopic to open incisional hernia repair [7] and one that looks at laparoscopic vs. open repair of Spigelian hernias [21]. Despite the growing body of knowledge in the field of LVHR, published overviews of the topic are largely review papers that have not pooled the data and critically analyzed it as a whole [9]. To date only a single meta-analysis encompassing eight studies and looking at three data sets (perioperative complications, operative time, and hospital LOS) has been published [13]. The current work, therefore, represents the first large-scale analysis of the published data on this topic.
The most stringent statistical method for analyzing any published data from multiple sources is a meta-analysis, which requires the studies under review to be complete and uniform in their data-reporting methods. Any studies that lack a data point of interest or fail to report standard deviations along with their means must be excluded from analysis. Such an approach in the area of ventral hernia repair would exclude many potentially informative studies because of the variable reporting methods used in these reports. We thus chose to perform a pooled-data analysis of LVHR to encompass a broad range of topical papers and thereby achieve a more complete overview of the results and outcomes of this procedure. Dividing the study population into “paired” and “pooled” groups allowed us to examine one cohort that should have a high degree of internal consistency for comparison with open ventral hernia repair (the paired studies only), and a significantly larger group (the pooled studies) that should give a broader view of the field as a whole, as has proven useful in similar past analyses [33].
In our analysis, we found the patient populations in both the pooled and paired laparoscopic groups, as well as in the open surgery group, to be demographically similar. All cohorts showed a similar gender distribution and the mean patient ages across the groups of studies showed little variation, with a minimum of 52.9 and a maximum of 56.1 years. Patient BMIs also fell within a narrow range of between 29.5 and 32.6, indicating that the vast majority of patients in the reported series were clinically overweight or obese. This finding is not surprising given that obesity is a strong predicative factor in hernia formation and recurrence [24, 30, 31].
The analysis of perioperative data showed that operative times were not significantly different for open or laparoscopic approaches. However, there was considerable variation across studies in the laparoscopic operative technique used, with some groups employing transfixion sutures routinely and others using them in a limited fashion or using only tacks. The variability in laparoscopic technique and the fact that most series included cases that were a part of the institution’s early experience limit any definite conclusions about operative time comparisons. The measured size of the hernia defect and the size of mesh used were, however, greater in the laparoscopic reports than the open patients, although these differences were significant for the pooled laparoscopic studies only. Possible explanations for these findings are that patients with larger defects are being selected for laparoscopic repair, the laparoscopic series are measuring sizes of all the combined defects whereas open reports describe the size of the largest defect only, additional defects are being detected and repaired with LVHR, or a combination of these variables. Similarly, it is not surprising that a larger mesh size was used with LVHR because of the coverage of all defects with a single piece of mesh without the need to dissect large tissue flaps as with open VHR. The identification of these additional defects and the ability to cover “Swiss-cheese”-type lesions with a single large piece of mesh are cited as benefits of the laparoscopic approach.
Postoperative length of stay (LOS) for both the pooled and the paired laparoscopic groups averaged only 2.4 days compared to 4.3 days for the open group. The reasons for the shorter hospitalization with the laparoscopic approach are unclear but could be related to fewer complications, as discussed below, among other variables. A shorter hospitalization could also be a factor in the potential economic impact of LVHR as recently addressed by Earle et al. [11].
The primary focus of this study was on perioperative complications and hernia recurrences. The analysis clearly shows that laparoscopic VHR was associated with a significantly lower overall complication rate compared to open VHR (25.5% LVHR vs. 41.7% OVHR in the paired analysis). This difference was primarily a result of more wound complications in the open VHR series, which were predominantly wound and/or mesh infections. Some differences were also seen in other organ system complications when the pooled LVHR data were compared to open VHR for GI, pulmonary, and miscellaneous other complications such as fever and thrombophlebitis; however, these differences did not reach statistical significance in the paired comparison because of the smaller sample size. Another explanation for the differences in other organ system complications in the pooled analysis is that groups reporting only on their laparoscopic experiences (i.e., studies included only in the pooled analysis) may have accumulated a more extensive experience and achieved better outcomes with the laparoscopic procedure. For example, one of the studies included in the pooled data set consisted of 850 patients from one multicenter trial of LVHR conducted by laparoscopic experts with very low complication rates [14]. Furthermore, the average number of patients undergoing LVHR in the unpaired studies was 132, but it was only 44 in the paired studies and 105 if the pooled group is considered. These differences hold true even if the aforementioned 850-patient study is excluded.
One of the main advantages of laparoscopic incisional hernia repair touted by proponents of this procedure is the potential for reduced wound complications and mesh infections. The results of this meta-analysis from the published literature give strong support to this contention. The difference in wound complications rates between laparoscopic versus open cases is largely a reflection of the decreased number of wound infections seen in the former group (1.3% laparoscopic vs. 9.5% open). There are likely two major factors contributing to this reduction in infection rate. First, open incisional hernia repair typically involves extensive lateral dissection of tissue planes with a large subcutaneous dead space and potentially altered blood flow and the need to drain the wound bed postoperatively. The mesh is often exposed to the subcutaneous space with the potential for increased infection risk of the mesh if a superficial wound infection occurs. With the laparoscopic approach, there is no flap dissection and the mesh is placed totally intraperitoneally. Second, during open repair there is a greater likelihood of the prosthetic mesh coming in contact with the patient’s skin with the potential for seeding by residual dermal flora. In the laparoscopic approach, however, the mesh is rolled up tightly before passing it into the abdomen, thus minimizing contact with the patient’s skin. In addition, the use of an iodine-impregnated adhesive surgical drape is one strategy that may reduce this potential contamination and resultant wound infection. Despite these advantages, some mesh infections were reported in the laparoscopic series (1.45% of paired laparoscopic series and 0.85% of pooled studies), which often resulted in removal of the mesh. Of note is that no differences in rate of seroma formation were found between laparoscopic vs. open repairs. While this could be because of variability in reporting of seroma as a complication, it would appear that clinically significant seroma is not a significant disadvantage for the laparoscopic approach.
One complication that occurred somewhat more frequently in the laparoscopic group in the paired analysis was enterotomy (2.9% laparoscopic vs. 1.2% open). Enterotomy during attempted ventral hernia repair is a major complication with potentially life-threatening consequences if unrecognized at the time of injury. The enterotomies recorded in this analysis included both those that were recognized at the time of surgery and those discovered later as a result of a subsequent complication. The occurrence of enterotomy is likely related to multiple variables, including surgeon experience, but the primary risk variable is the extent of intra-abdominal adhesions. The presence of prior mesh hernia repair may also be a factor in the risk for enterotomy during laparoscopic incisional hernia repair. In one recent series, the incidence of enterotomy during LVHR in patients with prior mesh placed was 11.4% compared to no enterotomies in patients who had not had previous mesh repairs [25]. Limiting use of cautery during adhesiolysis and avoiding the placement of uncoated macroporous meshes where they may come in contact with the abdominal viscera are strategies that should be undertaken to minimize this risk.
Early postoperative pain was not evaluated in this analysis, but prolonged procedure-related pain was recorded in a somewhat higher percentage of patients in the pooled laparoscopic series compared to open but not in the paired analysis. These differences could be accounted for in part by variable reporting methods of prolonged pain as a “complication.” However, unlike most other laparoscopic procedures where incisional pain is typically minimal and relatively short lived, laparoscopic incisional hernia repair is associated with substantially more pain in the postoperative period because of the methods of mesh fixation. Specifically, the use of transfixion sutures for the mesh has been associated with increased pain after laparoscopic ventral hernia repair but this issue was not addressed in our analysis.
The most important measure of an effective hernia operation is a low recurrence rate. The results of our analysis show that for both the paired and the pooled data sets, LVHR was associated with significantly fewer hernia recurrences overall. In fact, the hernia recurrence rates in the paired and the pooled laparoscopic studies of 3.1% and 4.3%, respectively, are some of the lowest recurrence rates for incisional hernia yet reported in the literature. These results do not appear to be explained on the basis of an inadequate or a short followup period, which averaged between 17 and 25 months across the reported series, although longer-term studies with exam followup will ultimately be necessary to verify these claims. Among the possible explanations for the lower recurrence rate with LVHR are that wide areas of tissue/prosthetic overlap can be obtained, as evidenced by the larger mesh sizes used in these cases compared to the open cases. This broad interface should allow for better tissue/mesh integration and thus a stronger repair and lower recurrence rate. LVHR may also be better at identifying all hernia defects, some of which could be missed with an open approach. Finally, variability in the mesh placement and fixation for open VHR could also be a factor in the higher recurrence rate. The low hernia recurrence rates reported to date with LVHR, therefore, should be taken into consideration when selecting an operative approach for patients with uncomplicated incisional hernias.
It is important to consider some of the limitations of the data analysis reported herein. One potential shortcoming of this study is the lack of complete statistical analysis of all data points studied. This, however, is largely due to inconsistent reporting of these data points across the studies evaluated. All the examined series reported their total number of patients, greater than 95% reported mean patient age, and approximately 85%–90% gave information on gender breakdowns, operative times, hospital length of stay, and duration of followup. In contrast, only about one-half to two-thirds of the studies gave information on hernia and mesh size, and fewer than 50% reported patient BMI values. Furthermore, only six reports, all of them paired studies, gave any information on the costs associated with the operative procedure and/or the hospital stay [2, 5, 10, 15, 20, 35]. Even in instances in which these parameters were reported, the values were sometimes given as means, sometimes as medians, and they often did not include standard deviations. Lack of such detailed information limits the statistical analyses that can be applied and precludes any formal meta-analysis of the data points unless a large number of studies with incomplete data are excluded.
Because they are reported as absolute numbers rather than means or percentages, the data on complications and recurrences are more amenable to formal statistical analysis. While we were able to identify 45 studies with complete recurrence and complication data, an additional 33 studies that were reviewed were excluded primarily because of incomplete outcomes data. This again highlights the importance of complete data reporting in studies of LVHR. We feel that we have identified a comprehensive, yet manageable list of data points that should be reported in all studies dealing with laparoscopic and open ventral hernia repair. Furthermore, values that are amenable to being reported as means (such as age, BMI, operative time, and length of stay) should be recorded as such, but standard deviations must be included to allow for better pooled-data or meta-analysis at a later point in time. Such meticulous data reporting, along with an increase in the amount of level 1 data, would certainly help to better define the role of new approaches to ventral hernia repair and should provide meaningful data that could lead to improvements in the surgical treatment of this important clinical problem.
Conclusions
Our analysis of the published literature on laparoscopic ventral hernia repair shows that this procedure is associated with lower total complication rates and fewer wound and mesh infections than seen with open mesh repair. In addition, hernia recurrence rates as reported in short- to medium-term followup are acceptably low and are significantly less than that reported in paired open ventral hernia cases. Further studies with longer-term followup will be necessary to verify these results. Despite the limitations of this pooled-data analysis, it would appear that there are several distinct advantages of laparoscopic incisional hernia repair over open approaches. Laparoscopic repair should be strongly considered by surgeons with appropriate advanced laparoscopic expertise for most patients with noncomplex incisional hernias.
References
Anthony T, Bergen PC, Kim LT, Henderson M, Fahey T, Rege RV, Turnage RH (2000) Factors affecting recurrence following incisional herniorrhaphy. World J Surg 24: 95–100
Beldi G, Ipaktchi R, Wagner M, Gloor B, Candinas D (2006) Laparoscopic ventral hernia repair is safe and cost effective. Surg Endosc 20: 92–95
Ben-Haim M, Kuriansky J, Tal R, Zmora O, Mintz Y, Rosin D, Ayalon A, Shabtai M (2002) Pitfalls and complications with laparoscopic intraperitoneal expanded polytetrafluoroethylene patch repair of postoperative ventral hernia. Surg Endosc 16: 785–788
Bencini L, Sanchez LJ (2004) Learning curve for laparoscopic ventral hernia repair. Am J Surg 187: 378–382
Bencini L, Sanchez LJ, Boffi B, Farsi M, Scatizzi M, Moretti R (2003) Incisional hernia: repair retrospective comparison of laparoscopic and open techniques. Surg Endosc 17: 1546–1551
Burger JW, Luijendijk RW, Hop WC, Halm JA, Verdaasdonk EG, Jeekel J (2004) Long-term follow-up of a randomized controlled trial of suture versus mesh repair of incisional hernia. Ann Surg 240: 578–583
Carbajo MA, Martin del Olmo JC, Blanco JI, de la CC, Toledano M, Martin F, Vaquero C, Inglada L (1999) Laparoscopic treatment vs open surgery in the solution of major incisional and abdominal wall hernias with mesh. Surg Endosc 13: 250–252
Carbajo MA, Martin del Olmo JC, Blanco JI, Toledano M, de la CC, Ferreras C, Vaquero C (2003) Laparoscopic approach to incisional hernia. Surg Endosc 17: 118–122
Cobb WS, Kercher KW, Heniford BT (2005) Laparoscopic repair of incisional hernias. Surg Clin North Am 85: 91–103, ix
DeMaria EJ, Moss JM, Sugerman HJ (2000) Laparoscopic intraperitoneal polytetrafluoroethylene (PTFE) prosthetic patch repair of ventral hernia. Prospective comparison to open prefascial polypropylene mesh repair. Surg Endosc 14: 326–329
Earle D, Seymour N, Fellinger E, Perez A (2006) Laparoscopic versus open incisional hernia repair: a single-institution analysis of hospital resource utilization for 884 consecutive cases. Surg Endosc 20: 71–75
Gonzalez R, Mason E, Duncan T, Wilson R, Ramshaw BJ (2003) Laparoscopic versus open umbilical hernia repair. JSLS 7: 323–328
Goodney PP, Birkmeyer CM, Birkmeyer JD (2002) Short-term outcomes of laparoscopic and open ventral hernia repair: a meta-analysis. Arch Surg 137: 1161–1165
Heniford BT, Park A, Ramshaw BJ, Voeller G (2003) Laparoscopic repair of ventral hernias: nine years’ experience with 850 consecutive hernias. Ann Surg 238: 391–399
Holzman MD, Purut CM, Reintgen K, Eubanks S, Pappas TN (1997) Laparoscopic ventral and incisional hernioplasty. Surg Endosc 11: 32–35
LeBlanc KA, Booth WV (1993) Laparoscopic repair of incisional abdominal hernias using expanded polytetrafluoroethylene: preliminary findings. Surg Laparosc Endosc 3: 39–41
LeBlanc KA, Booth WV, Whitaker JM, Bellanger DE (2000) Laparoscopic incisional and ventral herniorrhaphy in 100 patients. Am J Surg 180: 193–197
Luijendijk RW, Hop WC, van den Tol MP, de L, Braaksma MM, IJzermans JN, Boelhouwer RU, de Vries BC, Salu MK, Wereldsma JC, Bruijninckx CM, Jeekel J (2000) A comparison of suture repair with mesh repair for incisional hernia. N Engl J Med 343: 392–398
Luijendijk RW, Lemmen MH, Hop WC, Wereldsma JC (1997) Incisional hernia recurrence following “vest-over-pants” or vertical Mayo repair of primary hernias of the midline. World J Surg 21: 62–65
McGreevy JM, Goodney PP, Birkmeyer CM, Finlayson SR, Laycock WS, Birkmeyer JD (2003) A prospective study comparing the complication rates between laparoscopic and open ventral hernia repairs. Surg Endosc 17: 1778–1780
Moreno-Egea A, Carrasco L, Girela E, Martin JG, Aguayo JL, Canteras M (2002) Open vs laparoscopic repair of spigelian hernia: a prospective randomized trial. Arch Surg 137: 1266–1268
Moreno-Egea A, Torralba JA, Girela E, Corral M, Bento M, Cartagena J, Vicente JP, Aguayo JL, Canteras M (2004) Immediate, early, and late morbidity with laparoscopic ventral hernia repair and tolerance to composite mesh. Surg Laparosc Endosc Percutan Tech 14: 130–135
Mudge M, Hughes LE (1985) Incisional hernia: a 10 year prospective study of incidence and attitudes. Br J Surg 72: 70–71
Novitsky YW, Cobb WS, Kercher KW, Matthews BD, Sing RF, Heniford BT (2006) Laparoscopic ventral hernia repair in obese patients: a new standard of care. Arch Surg 141: 57–61
Perrone JM, Soper NJ, Eagon JC, Klingensmith ME, Aft RL, Frisella MM, Brunt LM (2005) Perioperative outcomes and complications of laparoscopic ventral hernia repair. Surgery 138: 708–715
Read RC, Yoder G (1989) Recent trends in the management of incisional herniation. Arch Surg 124: 485–488
Rosen M, Brody F, Ponsky J, Walsh RM, Rosenblatt S, Duperier F, Fanning A, Siperstein A (2003) Recurrence after laparoscopic ventral hernia repair. Surg Endosc 17: 123–128
Salameh JR, Sweeney JF, Graviss EA, Essien FA, Williams MD, Awad S, Itani KM, Fisher WE (2002) Laparoscopic ventral hernia repair during the learning curve. Hernia 6: 182–187
Sorensen LT, Hemmingsen UB, Kirkeby LT, Kallehave F, Jorgensen LN (2005) Smoking is a risk factor for incisional hernia. Arch Surg 140: 119–123
Sugerman HJ (1998) Increased intra-abdominal pressure in obesity. Int J Obes Relat Metab Disord 22: 1138
Sugerman HJ (2001) Effects of increased intra-abdominal pressure in severe obesity. Surg Clin North Am 81: 1063–1075, vi
Ujiki MB, Weinberger J, Varghese TK, Murayama KM, Joehl RJ (2004) One hundred consecutive laparoscopic ventral hernia repairs. Am J Surg 188: 593–597
Winslow ER, Fleshman JW, Birnbaum EH, Brunt LM (2002) Wound complications of laparoscopic vs open colectomy. Surg Endosc 16: 1420–1425
Wright BE, Beckerman J, Cohen M, Cumming JK, Rodriguez JL (2002) Is laparoscopic umbilical hernia repair with mesh a reasonable alternative to conventional repair? Am J Surg 184: 505–508
Wright BE, Niskanen BD, Peterson DJ, Ney AL, Odland MD, VanCamp J, Zera RT, Rodriguez JL (2002) Laparoscopic ventral hernia repair: are there comparative advantages over traditional methods of repair? Am Surg 68: 291–295
Acknowledgments
The authors thank Dr. Yan Yan in the Division of Urologic Surgery for performing the statistical analyses in this study. They also acknowledge the support of the Washington University Institute for Minimally Invasive Surgery, which is supported by educational grants from Ethicon EndoSurgery, Inc., and Stryker Endoscopy, Inc.
Author information
Authors and Affiliations
Corresponding author
Appendices
Appendix 1. Paired Series Included in Study
-
1.
Beldi G, Ipaktchi R, Wagner M, Gloor B, Candinas D (2006) Laparoscopic ventral hernia repair is safe and cost effective. Surg Endosc 20: 92–95
-
2.
Bencini L, Sanchez LJ, Boffi B, Farsi M, Scatizzi M, Moretti R (2003) Incisional hernia: repair retrospective comparison of laparoscopic and open techniques. Surg Endosc 17: 1546–1551
-
3.
Carbajo MA, Martin del Olmo JC, Blanco JI, de la CC, Toledano M, Martin F, Vaquero C, Inglada L (1999) Laparoscopic treatment vs open surgery in the solution of major incisional and abdominal wall hernias with mesh. Surg Endosc 13: 250–252
-
4.
DeMaria EJ, Moss JM, Sugerman HJ (2000) Laparoscopic intraperitoneal polytetrafluoroethylene (PTFE) prosthetic patch repair of ventral hernia. Prospective comparison to open prefascial polypropylene mesh repair. Surg Endosc 14: 326–329
-
5.
Gonzalez R, Mason E, Duncan T, Wilson R, Ramshaw BJ (2003) Laparoscopic versus open umbilical hernia repair. JSLS 7: 323–328
-
6.
Holzman MD, Purut CM, Reintgen K, Eubanks S, Pappas TN (1997) Laparoscopic ventral and incisional hernioplasty. Surg Endosc 11: 32–35
-
7.
McGreevy JM, Goodney PP, Birkmeyer CM, Finlayson SR, Laycock WS, Birkmeyer JD (2003) A prospective study comparing the complication rates between laparoscopic and open ventral hernia repairs. Surg Endosc 17: 1778–1780
-
8.
Park A, Birch DW, Lovrics P (1998) Laparoscopic and open incisional hernia repair: a comparison study. Surgery 124: 816–821
-
9.
Raftopoulos I, Vanuno D, Khorsand J, Kouraklis G, Lasky P (2003) Comparison of open and laparoscopic prosthetic repair of large ventral hernias. JSLS 7: 227–232
-
10.
Ramshaw BJ, Esartia P, Schwab J, Mason EM, Wilson RA, Duncan TD, Miller J, Lucas GW, Promes J (1999) Comparison of laparoscopic and open ventral herniorrhaphy. Am Surg 65: 827–831
-
11.
Salameh JR, Sweeney JF, Graviss EA, Essien FA, Williams MD, Awad S, Itani KM, Fisher WE (2002) Laparoscopic ventral hernia repair during the learning curve. Hernia 6: 182–187
-
12.
van’t Riet RM, de Vos van Steenwijk PJ, Bonthuis F, Marquet RL, Steyerberg EW, Jeekel J, Bonjer HJ (2003) Prevention of adhesion to prosthetic mesh: comparison of different barriers using an incisional hernia model. Ann Surg 237: 123–128
-
13.
Wright BE, Beckerman J, Cohen M, Cumming JK, Rodriguez JL (2002) Is laparoscopic umbilical hernia repair with mesh a reasonable alternative to conventional repair? Am J Surg 184: 505–508
-
14.
Wright BE, Niskanen BD, Peterson DJ, Ney AL, Odland MD, VanCamp J, Zera RT, Rodriguez JL (2002) Laparoscopic ventral hernia repair: are there comparative advantages over traditional methods of repair? Am Surg 68: 291–295
Appendix 2. Unpaired Series Included in Study
-
1.
Aura T, Habib E, Mekkaoui M, Brassier D, Elhadad A (2002) Laparoscopic tension-free repair of anterior abdominal wall incisional and ventral hernias with an intraperitoneal Gore-Tex mesh: prospective study and review of the literature. J Laparoendosc Adv Surg Tech A 12: 263–267
-
2.
Bageacu S, Blanc P, Breton C, Gonzales M, Porcheron J, Chabert M, Balique JG (2002) Laparoscopic repair of incisional hernia: a retrospective study of 159 patients. Surg Endosc 16: 345–348
-
3.
Bamehriz F, Birch DW (2004) The feasibility of adopting laparoscopic incisional hernia repair in general surgery practice: early outcomes in an unselected series of patients. Surg Laparosc Endosc Percutan Tech 14: 207–209
-
4.
Ben-Haim M, Kuriansky J, Tal R, Zmora O, Mintz Y, Rosin D, Ayalon A, Shabtai M (2002) Pitfalls and complications with laparoscopic intraperitoneal expanded polytetrafluoroethylene patch repair of postoperative ventral hernia. Surg Endosc 16: 785–788
-
5.
Berger D, Bientzle M, Muller A (2002) Postoperative complications after laparoscopic incisional hernia repair. Incidence and treatment. Surg Endosc 16: 1720–1723
-
6.
Bingener J, Kazantsev GB, Chopra S, Schwesinger WH (2004) Adhesion formation after laparoscopic ventral incisional hernia repair with polypropylene mesh: a study using abdominal ultrasound. JSLS 8: 127–131
-
7.
Birgisson G, Park AE, Mastrangelo MJ Jr, Witzke DB, Chu UB (2001) Obesity and laparoscopic repair of ventral hernias. Surg Endosc 15: 1419–1422
-
8.
Bower CE, Reade CC, Kirby LW, Roth JS (2004) Complications of laparoscopic incisional-ventral hernia repair: the experience of a single institution. Surg Endosc 18: 672–675
-
9.
Carbajo MA, Martp del Olmo JC, Blanco JI, Toledano M, de la CC, Ferreras C, Vaquero C (2003) Laparoscopic approach to incisional hernia. Surg Endosc 17: 118–122
-
10.
Chelala E, Gaede F, Douillez V, Dessily M, Alle JL (2003) The suturing concept for laparoscopic mesh fixation in ventral and incisional hernias: preliminary results. Hernia 7: 191–196
-
11.
Chowbey PK, Sharma A, Khullar R, Mann V, Baijal M, Vashistha A (2000) Laparoscopic ventral hernia repair. J Laparoendosc Adv Surg Tech A 10: 79–84
-
12.
Eid GM, Prince JM, Mattar SG, Hamad G, Ikrammudin S, Schauer PR (2003) Medium-term follow-up confirms the safety and durability of laparoscopic ventral hernia repair with PTFE. Surgery 134: 599–603
-
13.
Franklin ME Jr, Gonzalez JJ Jr, Glass JL, Manjarrez A (2004) Laparoscopic ventral and incisional hernia repair: an 11-year experience. Hernia 8: 23–27
-
14.
Heniford BT, Park A, Ramshaw BJ, Voeller G (2003) Laparoscopic repair of ventral hernias: nine years’ experience with 850 consecutive hernias. Ann Surg 238: 391–399
-
15.
Kannan K, Ng C, Ravintharan T (2004) Laparoscopic ventral hernia repair: local experience. Singapore Med J 45: 271–275
-
16.
Kua KB, Coleman M, Martin I, O’Rourke N (2002) Laparoscopic repair of ventral incisional hernia. ANZ J Surg 72: 296–299
-
17.
Kyzer S, Alis M, Aloni Y, Charuzi I (1999) Laparoscopic repair of postoperation ventral hernia. Early postoperation results. Surg Endosc 13: 928–931
-
18.
LeBlanc KA, Whitaker JM, Bellanger DE, Rhynes VK (2003) Laparoscopic incisional and ventral hernioplasty: lessons learned from 200 patients. Hernia 7: 118–124
-
19.
Mizrahi S, Lantsberg L, Kirshtein B, Bayme M, Avinoah E (2003) The experience with a modified technique for laparoscopic ventral hernia repair. J Laparoendosc Adv Surg Tech A 13: 305–307
-
20.
Moreno-Egea DA, Martinez JA, Cuenca GM, Miquel JD, Lorenzo JG, Albasini JL, Jordana MC (2004) Mortality following laparoscopic ventral hernia repair: lessons from 90 consecutive cases and bibliographical analysis. Hernia 8: 208–212
-
21.
Muysoms F, Daeter E, Vander MG, Claeys D (2004) Laparoscopic intraperitoneal repair of incisional and ventral hernias. Acta Chir Belg 104: 705–708
-
22.
Parker HH III, Nottingham JM, Bynoe RP, Yost MJ (2002) Laparoscopic repair of large incisional hernias. Am Surg 68: 530–533
-
23.
Perrone JM, Soper NJ, Eagon JC, Klingensmith ME, Aft RL, Frisella MM, Brunt LM (2005) Perioperative outcomes and complications of laparoscopic ventral hernia repair. Surgery 138: 708–715
-
24.
Reitter DR, Paulsen JK, Debord JR, Estes NC (2000) Five-year experience with the “four-before” laparoscopic ventral hernia repair. Am Surg 66: 465–468
-
25.
Rosen M, Brody F, Ponsky J, Walsh RM, Rosenblatt S, Duperier F, Fanning A, Siperstein A (2003) Recurrence after laparoscopic ventral hernia repair. Surg Endosc 17: 123–128
-
26.
Sanchez LJ, Bencini L, Moretti R (2004) Recurrences after laparoscopic ventral hernia repair: results and critical review. Hernia 8: 138–143
-
27.
Szymanski J, Voitk A, Joffe J, Alvarez C, Rosenthal G (2000) Technique and early results of outpatient laparoscopic mesh onlay repair of ventral hernias. Surg Endosc 14: 582–584
-
28.
Toy FK, Bailey RW, Carey S, Chappuis CW, Gagner M, Josephs LG, Mangiante EC, Park AE, Pomp A, Smoot RT Jr, Uddo JF Jr, Voeller GR (1998) Prospective, multicenter study of laparoscopic ventral hernioplasty. Preliminary results. Surg Endosc 12: 955–959
-
29.
Tsimoyiannis EC, Siakas P, Glantzounis G, Koulas S, Mavridou P, Gossios KI (2001) Seroma in laparoscopic ventral hernioplasty. Surg Laparosc Endosc Percutan Tech 11: 317–321
-
30.
Ujiki MB, Weinberger J, Varghese TK, Murayama KM, Joehl RJ (2004) One hundred consecutive laparoscopic ventral hernia repairs. Am J Surg 188: 593–597
-
31.
Verbo A, Petito L, Pedretti G, Lurati M, D’Alba P, Coco C (2004) Use of a new type of PTFE mesh in laparoscopic incisional hernia repair: the continuing evolution of technique and surgical expertise. Int Surg 89: 27–31
Rights and permissions
About this article
Cite this article
Pierce, R.A., Spitler, J.A., Frisella, M.M. et al. Pooled data analysis of laparoscopic vs. open ventral hernia repair: 14 years of patient data accrual. Surg Endosc 21, 378–386 (2007). https://doi.org/10.1007/s00464-006-9115-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-006-9115-6