
Abstract
Background
Several studies have shown the efficacy and effectiveness of the combined endoscopic–laparoscopic “rendezvous” technique for treatment of gallbladder and bile duct stones without complications, particularly pancreatitis. The so-called rendezvous technique consists of laparoscopic cholecystectomy standards with intraoperative cholangiography followed by endoscopic sphincterotomy (EST). The sphincterotome is driven across the papilla through a guidewire inserted by the transcystic route. This method allows easier and faster cannulation, thus avoiding papillary edema and pancreatic trauma. The aim of this study was to evaluate whether this method is effective in eliminating ductal stones and to verify whether the risk of postprocedure pancreatitis is diminished.
Methods
From January 2002 to September 2004, we enrolled 256 patients with cholecystocholedolithiasis detected by transabdominal ultrasound and magnetic resonance cholangiopancreatography. One hundred and twenty of these had one or more patient-related risk factors for post-endoscopic retrograde cholangiopancreatography (ERCP) pancreatitis, so they were randomized into two groups of 60 patients. In group A, the patients were treated in a single step with videolaparoscopic cholecystectomy, intraoperative cholangiography, and EST during the surgical procedure with the rendezvous technique. In group B, preoperative ERCP and EST were performed by using a traditional method of bile duct cannulation.
Results
No cases of post-ERCP pancreatitis were observed in group A, whereas six cases of acute post-ERCP pancreatitis occurred in group B (five mild and one moderate) (p = 0.0274). No procedure-related mortality was recorded.
Conclusion
In cholecysthocholedocholithiasis, the combined laparoscopic–endoscopic approach prevents post-ERCP pancreatitis in cases with patient-related risk factors for this complication.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
In Western countries, choledocholithiasis is associated with symptomatic gallstones in 8–18% of cases [16]. There are several approaches for the management of this situation: (a) endoscopic treatment of bile duct stones without subsequent cholecystectomy [29, 30], (b) preoperative endoscopic retrograde cholangiopancreatography (ERCP) followed by cholecystectomy [4], (c) cholecystectomy and laparoscopic treatment of the bile duct [4], or (d) cholecystectomy followed by postoperative ERCP [4]. The final choice among the therapeutic strategies generally available depends on expertise and experience. Pre- and postoperative ERCP and laparoscopic bile duct stones treatment (LBDT) are preferable according to the findings of a consensus development conference of the European Association for Endoscopic Surgery [7]. The transcystic (choledochoscopy) and transductal (choledodochotomy) LBTD are demanding techniques and, apart from a few centers [22], they are not widely used.
The challenged and proven method for the treatment of biliary duct stones remains the ERCP with sphincterotomy, but it is burdened with serious complications such as acute pancreatitis that occur in 2–9% of cases and moderate to severe complications in approximately 1% of cases [11, 12]. The rate of these complications increases dramatically with a relevant mortality when there are patient-related risk factors for post-ERCP pancreatitis [11]. In recent years, some reports have shown the effective use of the one-step combined laparoscopic–endoscopic “rendezvous” technique in the gallbladder and biliary duct lithiasis [6, 9, 14, 15]. This involves a standard laparoscopic cholecystectomy with intraoperative cholangiography followed by endoscopic sphincterotomy (EST) in which the sphincterotomy is driven across the papilla through a guidewire inserted through the transcystic route. In these studies, bile duct clearance was obtained in 90–94% of cases with a low complication rate and with no cases of post-ERCP acute pancreatitis. The guidewire most likely allows easier and faster bile duct cannulation, thus avoiding papillary edema and pancreatic trauma.
In the current study, we evaluated the effectiveness and safety of the laparoscopic–endoscopic rendezvous technique compared to the traditional preoperative ERCP/EST in cases of both gallbladder and main bile duct stones with patient-related risk factors for post-ERCP acute pancreatitis.
Patients and methods
Between January 2002 and September 2004, in 256 consecutive hospitalized patients gallbladder and main bile duct stones were detected by both transabdominal ultrasound (US) and magnetic resonance cholangiopancreatography (MRCP). One hundred and twenty of these patients (52 men and 68 women; mean age, 54.2 years; range, 22–60) were considered as having one or more of the following patient-related risk factors for post-ERCP pancreatitis: age ≤60 years (120 cases) [20], female gender (68 cases) [10], history of relapsing pancreatitis (36 cases) [19], and bile duct diameter ≤8 mm (15 cases) [10, 19, 20] (Table 1). These patients were randomized into two groups (A and B) by a computer program; each group was composed of 60 patients. In designing the study, a power analysis was conducted for detecting differences at a 5% level of significance between a group with a 15% rate of postprocedure pancreatitis (ERCP performed with standard technique in cases with patient-related risk factors, according to published data [10–12] and a group with a less than 2% rate of postprocedure pancreatitis (ERCP performed in an operative laparoscopic setting, based on preliminary data). The analysis indicated that a sample of 60 patients in each arm of the study would provide a power of 80%.
Exclusion criteria were the refusal or inability to provide informed consent, age <18 years, chronic use of opoid drugs, pregnancy, allergy to propofol and/or fentanyl, the presence of a choledochoduodenal anastomosis, chronic pancreatitis, and previous sphincterotomy. Written informed consent was obtained from all patients, and the study, carried out in accordance with the Helsinki Declaration, was approved by the ethics committee of our institute.
In all patients in group A, the severity of any concomitant disease was graded according to the American Society of Anesthesiologists (ASA) physical status classification [8]. General anesthesia was obtained with fentanyl 50–100 μg/ml i.v., propofol 0.5 μg/ml (with target concentration ranging between 2 and 5 μg/ml), and vecuronium bromide 4 mg/ml. All drugs used for the anesthesia had a rapid washout and did not relieve possible abdominal pain in the postoperative period. All patients were positioned supine on the operating table, and after creating the pneumoperitoneum, intraoperative cholangiography was obtained by using a 5-Fr catheter kept in place with one or more clips on the cystic duct to confirm the duct stones already detected by US and MRCP.
After a partial deflation of the pneumoperitoneum, a videoduodenoscope (ED 3410, Pentax, Hamburg, Germany) and monitor were placed behind the anesthesia drapes at the patient’s head. Duodenoscope manipulation through the stomach and maneuvers to reach the papilla were identical to those for ERCP with the patient in the prone position. The major differences from standard ERCP were as follows: (a) the endoscopist worked with his back toward the patient from the left side of the operating table; (b) the introduction of the duodenoscope was sometimes difficult due to the presence of the tracheal–laryngeal anesthetic tube; and (c) there was rapid cannulation of the papilla because a soft-tipped guidewire (450 cm, 0.035 in., Zebra Exchange, Microvasive, Boston Scientific, Genoa, Italy) had been passed through the cystic duct and papilla into the duodenum by the surgeon before removal of the gallbladder. The guidewire, gripped with a snare, was pulled through the accessory channel of the duodenoscope. Then the 6-Fr papillotome (Cotton cannulotome II PC PreCurved Double Lumen Sphincterothome, Wilson–Cook Medical, Winston-Salem, NC, USA) was inserted endoscopically over the guidewire. The sphincterotomy was performed in all patients using a bland electrosurgical current. After the extraction of the wire through the accessory channel of the duodenoscope, the stones were removed with a Dormia basket or balloon. Cholecystectomy was then performed.
In group B, the standard technique was used for cannulation of the bile duct with a papillotome and injection of contrast medium. After an overnight fast, all patients were given standard premedication (pentazocine chloride 30 mg i.v. and hioscine N-butyl bromide 20 mg i.v.). Pharyngeal anesthesia was induced with a topical anesthetic. The antibiotic gentamicine was diluted to a concentration of 2 mg/ml in iopamidol (Iopamir, Bracco, Milan, Italy), a low-osmolality contrast medium that was used to opacify the ducts. Blood oxygen saturation was monitored by using an automed device during all procedures. All patients in group B were scheduled for videolaparoscopic cholecystectomy within 24–48 h after ERCP.
No drugs for the prophylactic prevention of post-ERCP pancreatitis were administered before the two procedures. In the event of postlaparoscopic pain, the patients in group A received no more than 100 mg i.v. tramadol to avoid biases in the diagnosis of pancreatitis. All endoscopic procedures in both groups were performed by the same endoscopist (F.L.). During the 7 years before the study, this endoscopist performed more than 200 ERCPs per year.
At the end of each procedure, the endoscopist recorded the details of the maneuvers performed, particularly the ease or difficulty of cannulation and the number of pancreatic duct injections in group B. The duration of the overall procedures and hospital stay were also registered for all patients.
In both groups, the serum amylase level and the white blood cell count were measured before the endoscopic procedure and 2, 4, 8, and 24 h thereafter. Hyperamylasemia was defined when there was an increase in serum amylase above the upper normal value (220 IU/L); leukocytosis was defined when the white cell count was >10,000 cells/mm³ [2, 27]. Pancreatic-like pain was defined as a persistent epigastric pain, often radiating to the back [13]. The presence/absence of pancreatic-like pain was recorded before the procedure and 2, 4, 8, and 24 h afterwards by an endoscopist or a surgery staff member who was unaware of the serum amylase and white blood cell count values.
Clinical features considered to be consistent with acute pancreatitis were pancreatic-like pain that persisted for at least 24 h after the procedure associated with serum amylase levels more than five times the upper normal limit, with or without leukocytosis [12, 13]; CT was used to confirm pancreatic inflammation. These features have been proposed by us as the most reliable indicators of post-ERCP pancreatitis [25, 26].
Statistical analysis
The occurrence of post-ERCP pancreatitis in the two groups was analyzed using the Fisher’s exact test. The parameter “hyperamylasemia greater than five times the upper normal limit” was evaluated in patients of the two groups and its occurrence was analyzed by the chi-square test with continuity correction. The duration of the procedures and hospital stay were evaluated by the Student’s t-test for continuous variables. Two-tailed p values were computed.
Results
No episode of acute pancreatitis was detected in group A, whereas six patients in group B developed acute pancreatitis after the endoscopic procedure (p = 0.0274). In five patients, the pancreatitis was mild, and in one it was moderate. In the five patients with mild acute pancreatitis, cholecystectomy was performed after 5 days; for the patient with moderate acute pancreatitis, the surgical approach was delayed 7 days.
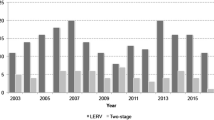
The serum amylase was more than five times the upper normal limit during the 24 h after the endoscopic procedure in one patient in group A and in 15 patients in group B (p < 0.001). The highest 24-h serum amylase values of all patients in groups A and B are reported in Fig. 1. Neither the occurrence of post-ERCP pancreatitis nor the rise in serum amylase levels more than five times the upper normal limit correlated with the prevalence of a single risk factor.

Highest 24-h serum amylase values in each patient of the two groups.
In group A, the bile duct was cannulated in 59 patients on whom we performed EST by extracting the biliary stones with a Dormia basket or balloon. In one patient, the guidewire did not pass through the papilla, so it was necessary to make a precut. In two patients, conversion to open surgery with choledochotomy was needed: in one case for prepapillary giant impacted stones and in the other case for a technical problem (loss of the wire in the intestinal loops). The latter patient did not undergo the endoscopic procedure and was therefore excluded from the statistical analysis. No biliary anatomy changes that could alter the procedures were observed. Laparoscopic cholecystectomies were not made more difficult by intraoperative endoscopic procedures using a device for adequate bowel disinflation before the probe extraction. In group B, clearing of the biliary duct was obtained in 58 patients; in one patient, the precut technique was needed, whereas other maneuvers such as guidewire cannulation or pancreatic stenting were never used. In two patients, the cholangiogram was normal and they did not undergo EST.
In group A, the median duration of the endoscopic procedure was 30 min, whereas in group B it was 35 min. The median time for the combined procedure was 70.5 min (range, 59–160) compared to 38.5 min (range, 28–115) for simple laparoscopic cholecystectomy (p < 0.001).
In group B, 22 patients had an accidental main pancreatic duct injection, with a median of 4 (range, 2–6). Among these patients were the six cases of acute post-ERCP pancreatitis. In group A, the main pancreatic duct was never cannulated or contrasted. The median hospital stay for group A was 3 days (range, 2–4), and that for group B was 6 days (range, 5–11) (p < 0.001). Other complications related to the two procedures were recorded in four cases. In group A, one patient had post-EST hemorrhage and one had delayed retroperitoneal post-EST perforation—the patient was discharged after 4 days and readmitted a week later for septic fever. The former patient was successfully treated with submucosal epinephrine infiltration. The latter received antibiotic therapy and subsequent percutaneous drainage of a retroperitoneal fluid collection associated with endoscopic biliary stenting; then, because clinical conditions did not improve, the patient underwent surgical intervention with gastrojejunostomy plus hepatic–jejunostomy and the outcome was favorable. In group B, two patients experienced an episode of post-ERCP cholangitis treated with i.v. antibiotics. Fifteen patients in group A experienced transient postlaparoscopic abdominal pain, not irradiated to the back, that was relieved within 6 h after tramadol administration. None of these patients had hyperamylasemia during the 24 h after the combined procedure.
No late complications were recorded. No cases of procedure-related mortality were observed.
Discussion
In approximately 15% of patients with lithiasis of the gallbladder, a symptomatic choledocholithiasis is associated, and it is the most frequent indication of ERCP. The common approach is the sequential method—that is, ERCP with papillosphincterotomy followed 24–48 h later by laparoscopic cholecystectomy. The diagnosis of lithiasis of the gallbladder is achieved by transabdominal US, whereas the main biliary duct is studied by US and, where possible, MRCP since in referral centers diagnostical ERCP has been abandoned in order to avoid the additional risk of acute post-ERCP pancreatitis [3]. This clinical event remains the most common complication, occurring after 1–30% of procedures with pancreatic necrosis in 0.3–0.6% of patients and with a related mortality of 0.4% [6]. In the past few decades, several studies have considered different strategies to reduce the occurrence of post-ERCP pancreatitis but with uncertain results. Pharmacological prophylaxis [1, 5, 21, 28] as well as the insertion of pancreatic stents [24] were tested. Multivariate analyses have delineated patient- and procedure-related risk factors for this complication so that post-ERCP pancreatitis is now largely predictable [11].
The concept that derives from these studies is that, especially in young patients with Sphincter of Oddi (SO) dysfunction and with a history of relapsing pancreatitis or with previous post-ERCP pancreatitis, we have to limit the manipulation of Vater’s papilla with repeated cannulations as much as possible to avoid the main pancreatic duct injection that can cause pressure duct trauma and pancreatic infections.
In a recent report, we showed that in nonselected patients with main biliary duct lithiasis the cannulation of the papilla with a guidewire avoids acute post-ERCP pancreatitis compared to the 4.1% complication rate seen with the traditional method [17]. Nevertheless, in the current series we chose the standard technique of papillary cannulation in the control group since at the time of the test the guidewire access to the bile duct had still not been validated.
A model of guidewire cannulation to reduce the risk of papillary injury during ERCP is well expressed in the context of the so-called rendezvous technique, a method developed in the 1980s as an endoscopic–radiological approach to facilitate common bile duct access through the abdomen [18, 23]. The use of a guidewire inserted by the surgeon through the cystic duct, common duct, and the papilla into the duodenum, where it is retrieved by the endoscopist with a polipectomy snare catheter through the endoscopy operatory channel, allows easier cannulation of the main bile duct without accidental Wirsung injection. In this context, the EST is performed in the right axis and the cut of the sphincter is fast. After extraction of the stones using a Dormia basket and/or balloon, the surgeon performs the cholecystectomy in a single step.
By adopting this combined approach in patients with gallbladder and main bile duct lithiasis, papillary trauma is avoided since this can be caused if the traditional catheter is used to detect the main biliary duct. In this regard, data reported in the literature show that no case of acute pancreatitis has been recorded after the combined technique [6, 9, 14, 15].
In the current study, we observed that in patients with cholecystocholedocholithiasis and with risk factors for acute post-ERCP pancreatitis, the single-step endoscopic–laparoscopic rendezvous technique allows clearance of the biliary duct and gallbladder removal at the same time and with no pancreatic complications. On the other hand, when an accidental contrast injection in the pancreatic duct was recorded (group B), acute post-ERCP pancreatitis occurred and the incidence of this complication was significantly different in the two treatment arms (p = 0.0274). This evidence, associated with a 24- to 48-h delay of laparoscopic cholecystectomy in the sequential approach, may account for the prolonged hospital stay in group B that was unrelated to other factors, such as concomitant illnesses or the need for further examinations.
In our study, the rendezvous technique required open surgery in three cases (two direct conversions and one delayed for a septic complication). However, only the conversion due to loss of the wire in the bowel loops was a direct consequence of the technique, and it occurred at the beginning of our learning curve. In the other cases, open surgery was adopted either for the failure of endoscopic treatment (giant stone) or for the management of a septic complication of EST, which are not related to the single-step approach but may also occur with the sequential method.
Despite clinical advantages, the combined endoscopic–laparoscopic approach to cholecystocholedocholithiasis proposed in our study presents some logistic problems, such as coscheduling laparoscopic cholecystectomy and ERCP, training of surgical and endoscopic staff, and prolonged use of the operative room. These aspects make the “all-in-one” management of gallbladder and bile duct stones difficult to perform in an urgent setting and in patients with only suspected choledocholithiasis, for whom the traditional therapeutic algorithm [22] should be considered. On the other hand, when bile duct stones have been previously diagnosed by US and/or MRCP, the rendezvous technique may play an important role as a therapeutic choice in place of the sequential method.
In conclusion, the favorable results in the clearance of the biliary duct, the short hospital stay, and the low morbidity make the rendezvous technique a promising strategy, in expert hands and in equipped centers, for the treatment of the gallbladder and main biliary duct lithiasis, particularly in cases with patient-related risk factors for acute post-ERCP pancreatitis.
References
Andriulli A, Leandro G, Niro G, Mangia A, Festa V, Gambassi G, et al. (2000) Pharmacologic treatment can prevent pancreatic injury after ERCP: a meta-analysis. Gastrointest Endosc 51: 1–7
Arcidiacono R, Gambitta P, Rossi A, Grosso C, Bini M, Zanasi G (1994) The use of a long-acting somatostatin analogue (Octreotide) for prophylaxis of acute pancreatitis after endoscopic sphincterotomy. Endoscopy 26: 715–718
Baillie J, Paulson EK, Vitellas KM (2003) Biliary imaging: a review. Gastroenterology 124: 1686–1699
Carr-Locke DL (2002) Therapeutic role of ERCP in the management of suspected common bile duct stones. Gastrointest Endosc 56: 170–174
Cavallini G, Tittobello A, Frulloni L, Masci E, Mariani A, Di Francesco V, et al. (1996) Gabexate for the prevention of pancreatic damage related to endoscopic retrograde cholangiopancreatography. N Engl J Med 335: 919–923
Davis WZ, Cotton PB, Arias RS, Williams DM, Onken JE (1997) ERCP and sphincterotomy in the context of laparoscopic cholecystectomy; academic and community practice patterns and results. Am J Gastroenterol 92: 597–601
European Association for Endoscopic Surgery Committee (1998) Diagnosis and treatment of common bile duct stones (CBDS). Surg Endosc 12: 856–864
Fanti L, Agostoni M, Casati A, Guslandi M, Giollo P, et al. (2004) Target-controlled propofol infusion during monitored anaesthesia in patients undergoing ERCP. Gastrointest Endosc 60: 361–366
Frazee RC, Robert J, Symmonds R, Hendricks JC, Snyder S, et al (1993) Combined laparoscopic and endoscopic management of cholelithiasis and choledocholithiasis. 166: 702–705
Freeman ML, DiSario JA, Nelson DB, Fennerty B, Lee JG, Bjorkman DJ, et al. (2001) Risk factors for post ERCP pancreatitis: a prospective multicenter study. Gastrointest Endosc 54: 425–434
Freeman ML, Guda N (2004) Prevention of post-ERCP pancreatitis: a comprehensive review. Gastrointest Endosc 59: 845–864
Freeman ML, Nelson DB, Sherman S, Haber GB, Herman ME, Dorsher PJ, et al. (1996) Complications of endoscopic biliary sphincterotomy. N Engl J Med 335: 909–918
Gottlieb K, Sherman S, Pezzi J, Esber E, Lehman GA (1996) Early recognition of post-ERCP pancreatitis by clinical assessment and serum pancreatic enzymes. Am J Gastroenterol 91: 1553–1557
Huntigton TR, Bohlman TW (1997) Laparoscopic biliary guidewire: a simplified approach to choledocholithiasis. Gastrointest Endosc 45: 295–297
Iodice G, Giardello C, Francica G, Sarrantonio G, Angelone G, Cristiano S, et al. (2001) Single-step treatment of gallbladder and bile duct stones: a combined endoscopic–laparoscopic technique. Gastrointest Endosc 53: 336–338
Ko CW, Lee SP (2002) Epidemiology and natural history of common bile duct stones and prediction of disease. The NIH State-of-the Science Conference: ERCP for diagnosis and therapy. Gastrointest Endosc 56(Suppl): 165–169
Lella F, Bagnolo F, Colombo E, Bonassi U (2004) A simple way of avoiding post-ERCP pancreatitis. Gastrointest Endosc 59: 830–834
Long WB, Shwarz W, Ring EJ (1984) Endoscopic sphincterotomy assisted by catheterization antegrade. Gastrointest Endosc 30: 36–39
Loperfido S, Angelini GP, Benedetti G, Chilovi F, Costan F, De Berardinis F, et al. (1998) Major early complications from diagnostic and therapeutic ERCP: a prospective multicenter study. Gastrointest Endosc 48: 1–10
Masci E, Toti G, Mariani A, Curioni S, Lomazzi A, et al. (2001) Complications of diagnostic and therapeutic ERCP: a prospective multicenter study. Am J Gastroenterol 96: 417–423
Pasha TM, Therneau T, Petersen BT (1997) Economic analysis of gabexate mesilate in post-ERCP pancreatitis [Abstract]. Gastroenterology 112: A471
Petelin JB (2002) Surgical management of common bile duct stones. Gastrointest Endosc 56(Suppl): 183–189
Shorvon PJ, Cotton PB, Mason RR (1985) Percutaneous transhepatic assistance for duodenal sphincterotomy. Gut 26: 1373–1376
Singh P, Das A, Isemberg G, Wong RCK, Sivak MV, Agrawal D, Chak A (2004) Does prophylactic pancreatic stent placement reduce the risk of post-ERCP acute pancreatitis? A meta-analysis of controlled trial. Gastrointest Endosc 60: 544–550
Testoni PA, Bagnolo F (2001) Pain at 24 hours associated with amylase levels 5 times greater than the upper normal limit as the most reliable indicator of post-ERCP pancreatitis. Gastrointest Endosc 53: 33–39
Testoni PA, Bagnolo F, Caporuscio S, Lella F (1999) Serum amylase measured four hours after endoscopic sphincterotomy is a reliable predictor of postprocedure pancreatitis. Am J Gastroenterol 94: 1235–1241
Testoni PA, Caporuscio S, Bagnolo F, Lella F (1999) Twenty-four hour amylase predicting pancreatic reaction after endoscopic sphincterotomy. Endoscopy 31: 131–136
Testoni PA, Lella F, Bagnolo F, Caporuscio S, Cattani L, Colombo E, et al. (1996) Long-term prophylactic administration of octreotide reduces the rise in serum amylase after endoscopic procedures on Vater’s papilla. Pancreas 13: 61–65
Tham TCK, Carr-Locke DL (1999) Endoscopic treatment of bile duct stones in elderly people. Br Med J 318: 617–618
Tham TC, Vandrvoort J, Wong RC, Carr-Locke DL (1996) Endoscopic sphincterotomy with gallbladder left in situ versus open surgery for common bile duct calculi. Lancet 348: 264
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Lella, F., Bagnolo, F., Rebuffat, C. et al. Use of the laparoscopic–endoscopic approach, the so-called “rendezvous” technique, in cholecystocholedocholithiasis. Surg Endosc 20, 419–423 (2006). https://doi.org/10.1007/s00464-005-0356-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-005-0356-6