
Abstract
Background
The role of laparoscopic appendectomy for perforated appendicitis remains controversial. This study aimed to compare laparoscopic and open appendectomy outcomes for children with perforated appendicitis.
Methods
Over a 36-month period, 111 children with perforated appendicitis were analyzed in a retrospective review. These children were treated with either laparoscopic (n = 59) or open appendectomy. The primary outcome measures were operative time, length of hospital stay, time to adequate oral intake, wound infection, intraabdominal abscess formation, and bowel obstruction.
Results
The demographic data, presenting symptoms, preoperative laboratory values, and operative times (laparoscopic group, 61 ± 3 min; open group, 57 ± 3 were similar for the two groups (p = 0.3). The time to adequate oral intake was 104 ± 7 h for the laparoscopic group and 127 ± 12 h for the open group (p = 0.08). The hospitalization time was 189 ± 14 h for the laparoscopic group, as compared with 210 ± 15 h for the open group (p = 0.3). The wound infection rate was 6.8% for the laparoscopic group and 23% for the open group (p < 0.05). The wounds of another 29% of the patients were left open at the time of surgery. The postoperative intraabdominal abscess formation rate was 13.6% for the laparoscopic group and 15.4% for the open group. One patient in each group experienced bowel obstruction.
Conclusions
Laparoscopic appendectomy for the children with perforated appendicitis in this study was associated with a significant decrease in the rate of wound infection. Furthermore, on the average, the children who underwent laparoscopic appendectomy tolerated enteral feedings and were discharged from the hospital approximately 24 h earlier than those who had open appendectomy.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Appendicitis is the most common surgical emergency in childhood [1]. Perforation is a typical complication in children [2]. In fact, 55% to 80% of patients younger than 6 years present to the surgeon with perforation, and perforated appendicitis remains a highly morbid condition [3]. For decades, open appendectomy has been the standard treatment for both acute and perforated appendicitis and has been proved safe and effective [4, 5]. Semm’s [6] application of laparoscopy for the treatment of appendicitis has introduced an element of controversy into an otherwise well-established treatment.
Laparoscopic appendectomy has the intrinsic appeal shared by all minimal access surgery. This includes the potential for decreased postoperative pain, more rapid return to full activity, and improved cosmesis. However several studies have suggested that the laparoscopic approach results in a possible longer operating time and more postoperative complications than the open approach. These observation have been reported for both adults and children [7–14].
Despite these reported potential disadvantages, laparoscopic appendectomy has become a popular operation for acute and perforated appendicitis in children [7, 9–11, 15, 16]. Our study aimed to compare the outcomes of laparoscopic and open appendectomy for children with perforated appendicitis in a busy pediatric surgical center that commonly performs advanced minimally invasive procedures for children.
Patients and methods
Over a 36-month period, 111 children with perforated appendicitis were seen at the Children’s Hospital of Alabama, University of Alabama at Birmingham. These patients were analyzed in a retrospective chart review. Appendectomy was performed by either open or laparoscopic technique on the basis of individual surgeon preference.
This retrospective chart review was performed by examining the reports of six pediatric surgeons at the University of Alabama at Birmingham, Children’s Hospital. Three of these pediatric surgeons are advocates of laparoscopic surgery. They prefer to treat every acute appendicitis case via a laparoscopic approach. These surgeons are well experienced in the field of pediatric laparoscopic surgery, including the most complex operations such as laparoscopic colectomy, Roux-en-Y, porto-enterostomy, and the like. The other three surgeons were in the favor of open appendectomy, and performed all their appendectomies in open fashion. Consequently, 59 (53%) of the children were treated with a laparoscopic approach, and 52 (47%) had open appendectomy. The cases were analyzed on the basis of intent to treat. Therefore, the laparoscopic group included three patients for whom laparoscopic appendectomy was attempted before conversion to open appendectomy. The open group included three patients for whom laparoscopy was used only to confirm the diagnosis of perforated appendicitis before open appendectomy. Children who had perforated appendicitis managed with intravenous antibiotics and drainage followed by interval appendectomy were not included in the study.
The diagnosis of perforated appendicitis was established by the surgeon at the time of surgery, then confirmed later with histopathologic reports. Open appendectomy was performed through a right lower quadrant muscle-splitting incision. The appendix was ligated at the base and divided with or without inversion of the appendiceal stump. Irrigation was based on the surgeon’s preference. The abdominal fascia was closed in layers. The skin incision was either left open (15/52) or closed with interrupted nylon sutures (37/52), as determined by the surgeon’s preference. Laparoscopic appendectomy was performed using a Veress needle for abdominal insufflation and placement of three abdominal access trocars. The meso-appendix was divided with an endo-GIA stapler or electrocautery. The appendix was laparoscopically mobilized and divided at the base using an endoscopic stapling device (32/59) or tied at the base with endoloops (27/52) and then divided. The appendix then was removed from the abdomen in an endocatch bag (46/59) or via the 12-mm umbilical trocar (13/59). The entire abdomen was inspected for contamination and typically irrigated vigorously.
Postoperatively, all the patients received intravenous (IV) fluid and parenteral broad-spectrum antibiotics. Children received either a triple antibiotic regimen or a single broad-spectrum antibiotic, typically for 7 to 10 days. Oral antibiotics such as Augmentin were frequently prescribed at the time of discharge for an additional week. Oral feeding was initiated and advanced as tolerated by the child. In addition to demographic data, particular attention was given to the operative time, the time to adequate oral intake, and the length of hospital stay. The operation length was calculated from skin incision to completion of wound closure. The time to adequate oral intake was specifically defined as the postoperative period required for the child to tolerate two-thirds of daily maintenance fluid by mouth. The hospital length of stay was defined as the time from admission until the time of discharge. The primary outcome measures for this study were development of a wound infection, intraabdominal abscess formation, and bowel obstruction. Wound infection was defined as purulent drainage from the wound or a change in antibiotics secondary to inflammatory changes in the wound. Computerized tomography or ultrasonography reports were used to establish the diagnosis of intraabdominal abscess formation. Bowel obstruction was defined as the patient requiring readmission for gastrointestinal decompression or reoperation. The frequencies of complications in the two groups were compared using the chi-square test. Student’s t-test was used for comparison of other continuous variables.
Results
The presenting symptoms and preoperative laboratory values were similar for the two groups (Table 1). Gender distribution also was similar in the open and laparoscopic appendectomy groups, with a male-to-female ratio of 1.8:1. In both populations, the patients ranged in age from 2 to 18 years. The mean age for the open group was 8.6 ± 0.5 years, as compared with 10.2 ± 0.5 years for the laparoscopic group (p < 0.05). The weight of the children ranged from 10 to 90 kg. The mean weight for the open group was 36 ± 3 kg, as compared with 43 ± 3 kg for the laparoscopic group, and this difference also was statistically significant (p < 0.05) (Table 2).
The mean operative time was 57 ± 3 min for the open appendectomy group and 60 ± 3 min for the laparoscopic group. This difference was not statistically significant (p > 0.05). The mean time to adequate oral intake was 127 ± 11 postoperative hours for the open group and 104 ± 7 postoperative hours for the laparoscopy group (p = 0.06). The children who underwent open appendectomy were hospitalized 210 ± 15 h on the average, whereas the laparoscopic appendectomy patients stayed 189 ± 15 h (Table 2).
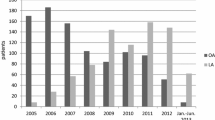
The incidences of postoperative complications for the two groups are summarized in Fig. 1. The most common complication observed in the group of children that underwent open appendectomy was wound infection. Superficial wound infection developed in 23% of the patients in this group. In the laparoscopic appendectomy group, a wound infection developed in only three patients. Each infection was located at the umbilical trocar site, and one of the patients had removal of appendix via this trocar. There seems to be no statistically significant difference between the two groups with regard to removal of the appendix. A postoperative intraabdominal abscess developed in 15.4% (8/52) of the patients undergoing open appendectomy. Three of these patients experienced intraabdominal abscess formation during the initial admission. Three of the patients were rehospitalized and treated with IV antibiotics. Five patients required reoperation for drainage. In the laparoscopic group, 8 (13.6%) of 59 patients experienced an intraabdominal abscess. Ligation with endoloops was performed for four of these eight patients (odds ratio [OR], 1.22; 95% confidence interval [CI], 0.27–5.41), whereas the appendix was removed via the umbilical trocar without using an endo-catch bag for three patients (OR, 2.46; 95% CI, 0.50–12.05).

Postoperative complication rates for the groups studied.
These data clearly show that there was no statistically significant difference between stapling the appendiceal stump and using endoloops in the presented series. Three of these patients were treated in hospital with an IV antibiotic. One patient was treated at home with oral antibiotics. Percutaneous drainage with ultrasonographic guidance was performed for one patient, and three patients required reoperation. There was no statistical difference between the two groups with regard to the prevalence of an intraabdominal abscess formation. One patient in each group experienced a postoperative bowel obstruction as a complication. The incidence of this condition was 1.9% in the open group and 1.7% in laparoscopic group.
Discussion
Most of the controlled trials comparing laparoscopic and open appendectomy in adults and children report significant advantages of the laparoscopic technique in terms of a reduced wound infection rate. This can be explained by the almost complete avoidance of abdominal wall contamination during laparoscopic procedures. This is especially true for all forms of perforated appendicitis with local formation of pus [7, 10, 16–18].
Our results for laparoscopic appendectomy confirm the significantly lower rate of wound healing complications (p < 0.05). Only three patients experienced a superficial wound healing impairment at the umbilical trocar. On the other hand, about one-fourth of the patients who underwent open appendectomy for perforated appendicitis experienced a superficial wound infection. This difference exists despite the fact that this rate of wound infection underrates the total wound morbidity associated with open appendectomy. In addition to the 25% in whom wound infections developed, the wounds of another 29% were left open at the time of operation. Considering this, less than half the children who underwent open appendectomy healed without a complicated wound. These results were comparable with other published infection rates, which reach up to 45% [12, 19]. Risk factors for the formation of intraabdominal abscess remain controversial. Several reports suggest that the incidence of this complication is higher after laparoscopic appendectomy than after open appendectomy among patients with perforated appendicitis [20]. Classic open appendectomy data have identified three factors crucial to minimizing intraabdominal abscess rates including adequate preoperative resuscitation, appropriate perioperative antibiotics, and good surgical technique [20–22].
The results of the presented study showed no increase in the incidence of postoperative intraabdominal abscess after laparoscopic appendectomy (p > 0.05). It has been suggested that the ligation of the appendiceal base with staples rather than an endoloop reduces the risk of spillage [23]. Four of eight patients in the presented group who experienced a postoperative intraabdominal abscess had their appendiceal stump ligated with endoloops (OR, 1.22; 95% CI, 0.27–5.41). Placement of the detached appendix into an endobag before its removal from the abdominal cavity reduces contact with visceral or fascial surfaces, minimizing intraabdominal contamination. Of the 13 children whose appendix was removed via the 12-mm umbilical trocar, 23% experienced an intraabdominal abscess, as compared with 10% of the endobag group (OR, 2.46; 95% CI, 0.50–12.05). On the basis of this data, we suggest removal of the appendix from the abdomen in an endobag.
Ortega et al. [23] have reported that the incidence of bowel obstruction is higher in laparoscopic appendectomy for perforated appendicitis than with the open approach. The incidence of postoperative bowel obstruction for perforated appendicitis in our study did not differ between the laparoscopic and open approaches.
One purported disadvantage of laparoscopic appendectomy is the longer operative time [18]. Our results refute this notion. This study is one of the first to demonstrate similar operating times for laparoscopic and open appendectomy used to manage perforated appendicitis. In most of the published data, the time until the start of postoperative oral intake was not found to be different in children and adults between laparoscopic and open appendectomy [24, 25]. Reintroduction of a normal diet occurred earlier after laparoscopic than after open appendectomy in a few studies [26]. In our series, the children in the laparoscopic appendectomy group usually started taking adequate oral intake on postoperative day 4, as compared with postoperative day 5 for the open appendectomy group. The magnitude of the difference between these means was large. There was almost a full 24-h time difference between the groups. Using Student’s t test, the difference fell just short of statistical significance, with a p value of 0.06. We believe this finding is a result of sample size. One major advantage of laparoscopic procedures reported is the faster recovery and shorter length of hospital stay. Several reports have suggested that the hospitalization was significantly shorter when the patient was treated using laparoscopic appendectomy [12, 16–18, 27].
The mean length of hospital stay for the laparoscopic appendectomy group in the current series was 20 h less than for the open appendectomy group. However, given the variance in these data, the difference between these two groups did not reach statistical difference.
In summary, perforated appendicitis in children continues to be a common and morbid condition. The incidence of perforation in children who presented with appendicitis was 40% at the Children’s Hospital of Alabama during the study period. Postoperative complications occurred in 27% of our patients, and 12% of these complications were superficial wound infections. In our series, laparoscopic appendectomy did not increase the operative time. Laparoscopic appendectomy in children with perforated appendicitis in this study was associated with a significant decrease in the rate of wound infection. Total wound morbidity decreased approximately 10-fold. The higher incidence of intraabdominal abscess formation after laparoscopic appendectomy suggested in other series was not observed in our study. It can be concluded that laparoscopic appendectomy is a safe alternative to the traditional open approach and could be the procedure of choice for perforated appendicitis in childhood.
References
Addiss DG, Shaffer N, Fowler BS, Tauxe RV (1990) The epidemiology of appendicitis and appendectomy in the United States. Am J Epidemiol 132: 910–925
Surana R, Puri P (1994) Primary wound closure after perforated appendicitis in children. Br J Surg 81: 440. No abstract available
Brender JD, Marcuse EK, Koepsell TD, Hatch EI (1985) Childhood appendicitis: factors associated with perforation. Pediatrics 76: 301–306
Pearl RH, Hale DA, Molloy M, Schutt DC, Jaques DP (1995) Pediatric appendectomy. J Pediatr Surg 30: 173–178
Fishman SJ, Pelosi L, Klavon SL, O’Rourke EJ (2000) Perforated appendicitis: prospective outcome analysis for 150 children. J Pediatr Surg 35: 923–926
Semm K (1983) Endoscopic appendectomy. Endoscopy 15: 59–64
Paya K, Fakhari M, Rauhofer U, Felberbauer FX, Rebhandl W, Horcher E. (2000) Open versus laparoscopic appendectomy in children: a comparison of complications. Journal of the Society of Laparoendoscopic Surgeons 4: 121–124
Frazee RC, Bohannon WT (1996) Laparoscopic appendectomy for complicated appendicitis. Arch Surg 131: 509–511
Canty TG Sr, Collins D, Losasso B, Lynch F, Brown C (2000) Laparoscopic appendectomy for simple and perforated appendicitis in children: the procedure of choice? J Pediatr Surg 35: 1582–1585
Kokoska ER, Murayama KM, Silen ML, Miller TA, Dillon PA, Weber TR (1999) A state-wide evaluation of appendectomy in children. Am J Surg 178: 537–540
Steyaert H, Hendrice C, Lereau L, Hayem C, el Ghoneimi A, Valla JS (1999) Laparoscopic appendectomy in children: sense or nonsense? Acta Chir Belg 99: 119–124
Stoltzing H,Thon K (2000) Perforated appendicitis: is laparocopic operation advisable? Dig Surg 17: 610–616
Little DC, Custer MD, May BH, Blalock SE, Cooney DR (2002) Laparoscopic appendectomy: An unnecessary and expensive procedure in children? J Pediatr Surg 37: 310–317
Lavonius MI, Liesjarvi S, Ovaska J, Pajulo O, Ristkari S, Alanen M (2001) Laparoscopic versus open appendectomy in children: a prospective randomised study. Eur J Pediatr Surg 11: 235–238
Lintula H, Kokki H, Vanamo K (2001) Single blind randomized clinical trial of laparoscopic versus open appendicectomy in children. Br J Surg 88: 510–514
Meguerditchian AN, Prasil P, Cloutier R, Leclerc S, Peloquin J, Roy G (2002) Laparoscopic appendectomy in children: A favorable alternative in simple and complicated appendicitis. J Pediatr Surg 37: 695–698
Paya K, Rauhofer U, Rebhandl W, Deluggi S, Horcher E (2000) Perforating appendicitis. An indication for laparoscopy? Surg Endosc 14: 182–184
Chung RS, Rowland DY, Li P, Diaz J (1999) A meta-analysis of randomized controlled trials of laparoscopic versus conventional appendectomy. Am J Surg 177: 250–256
Jess P (1983) Acute appendicitis: epidemiology, diagnostic accuracy, and complications. Scand J Gastroenterol 18: 161–163
Katkhouda N, Friedlander MH, Grant SW, Achanta KK, Essani R, Paik P,Velmahos G, Campos G, Mason R, Mavor E (2000) Intraabdominal abscess rate after laparoscopic appendectomy. Am J Surg 180: 456–459; discussion 460–461
Reid RI, Dobbs BR, Frizelle FA (1999) Risk factors for postappendicectomy intraabdominal abscess. Aust NZ J Surg 69: 373–374
Temple LK, Litwin DE, McLeod RS (1999) A metaanalysis of laparoscopic versus open appendectomy in patients suspected of having acute appendicitis. Can J Surg 42: 377–383
Ortega AE, Hunter JG, Peters JH, Swanstrom LL, Schirmer B (1995) A prospective, randomized comparison of laparoscopic appendectomy with open appendectomy. Laparoscopic Appendectomy Study Group. Am J Surg 169: 208–212
Lejus C, Delile L, Plattner V, Baron M, Guillou S, Heloury Y, Souron R (1996) Randomized, single-blinded trial of laparoscopic versus open appendectomy in children: effects on postoperative analgesia. Anesthesiology 84: 801–806
Ure BM, Spangenberger W, Hebebrand D, Eypasch EP, Troidl H (1992) Laparoscopic surgery in children and adolescents with suspected appendicitis: results of medical technology assessment. Eur J Pediatr Surg 2: 336–340
Tate JJ, Chung SC, Dawson J, Leong HT, Chan A, Lau WY, Li AK (1993) Conventional versus laparoscopic surgery for acute appendicitis. Br J Surg 80: 761–764
Khalili TM, Hiatt JR, Savar A, Lau C, Margulies DR (1999) Perforated appendicitis is not a contraindication to laparoscopy. Am Surg 65(10): 965–967
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Yagmurlu, A., Vernon, A., Barnhart, D.C. et al. Laparoscopic appendectomy for perforated appendicitis: a comparison with open appendectomy. Surg Endosc 20, 1051–1054 (2006). https://doi.org/10.1007/s00464-005-0342-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-005-0342-z