
Abstract
Background
This study aimed to evaluate the long-term impact of laparoscopic Nissen fundoplication on esophageal motility in patients with preoperative esophageal dysmotility.
Methods
This study prospectively followed 580 patients who underwent laparoscopic Nissen fundoplication between 1992 and 1999. Esophageal manometry, 24-h pH monitoring, and symptom score assessment were performed before surgery, then 6 months, 2 years, and 5 years after surgery. Preoperatively, 533 of the patients (93.5%) had normal esophageal contractile pressure (group 1), whereas 38 of the patients (6.5%) had reduced contractile pressure (<30 mmHg) (group 2).
Results
Esophageal contractile pressures increased significantly in the patients with low preoperative values, whereas it remained unchanged in the patients with normal preoperative contractile pressures. Both groups reported a significant reduction in the dysphagia symptom score after surgery.
Conclusion
Nissen fundoplication produces a significant long-lasting increase in esophageal contractile pressures in patients with preoperative esophageal dysmotility (i.e., contractile pressure lower than 30 mmHg). Preoperative esophageal dysmotility is therefore not a contraindication to laparoscopic Nissen fundoplication.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Gastroesophageal reflux disease (GERD) is a common condition, occurring in approximately 7% of the general population on a daily basis, and in up to 30% at least once a month. Proton pump inhibitors usually are the first-line treatment for GERD, but surgery is sometimes required to manage poorly controlled symptoms or to avoid long-term medical therapy.
One of the most popular procedures for the treatment of reflux, described by R. Nissen in 1956 [13], still is the most common surgical option for GERD in North America. However, since it was first reported in 1991 [6], the laparoscopic technique has become the approach of choice.
The basic mechanism of action with these techniques is an increase in lower esophageal sphincter pressure. Some authors, however, advocate that 360° Nissen fundoplication can create an obstacle to esophageal emptying, thus increasing the rate of postoperative dysphagia, esophageal stasis, or gas bloat syndrome, especially in patients with preoperative esophageal dysmotility. When motor disorders of the esophageal body are demonstrated, these authors consider that partial fundoplication is indicated to reduce the postoperative rate of dysphagia. However, conflicting results have been reported in the literature regarding the long-term efficiency of partial fundoplication in controlling GERD, and no clear correlation has ever been demonstrated between preoperative esophageal motility study findings and postoperative results [7, 12].
The aim of this prospective study was to compare the long-term outcomes between patients with preoperative esophageal dysmotility undergoing laparoscopic Nissen fundoplication (LNF) and patients with normal esophageal motility.
Material and methods
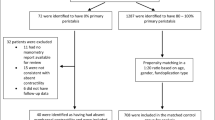
From July 1992 to December 1998, 580 patients with documented GERD underwent LNF performed by a single surgeon (M.A.) at a university medical center (Center for Minimal Access Surgery, McMaster University, Hamilton, Ontario). All the patients who had undergone preoperative esophageal manometry at the same hospital were included in this study. Ethics board approval for collecting these data was obtained.
The following data were collected prospectively, as previously described [2]: demographic data (age, gender, operative time, and duration of hospitalization), esophageal manometry results, 24-h pH recording (number of reflux events, percentage of reflux time during 24 h, and DeMeester score).
Esophageal manometry was performed with a 7-lumen sleeve-sidehole catheter. The basal pressure in the lower esophageal sphincter region was measured with the sleeve sensor (Dent Sleeve Pty Ltd., Adelaide, Australia) in relation to the gastric pressure. All the patients were asked to stop all antireflux medications for 5 days before 24-h pH testing using an ambulatory digitrapper (Synetics, Stockholm, Sweden). The pH probe was positioned 5 cm above the lower esophageal sphincter, as determined earlier by manometry. Gastroesophageal reflux was considered to be a drop in esophageal pH below 4. The percentage of reflux below 4% in 24 h was calculated for each patient.
A detailed questionnaire also was used to assess patients’ GERD-specific symptoms (heartburn, pain, regurgitation, dysphagia, fullness, and cough) and non-GERD symptoms (vomiting, constipation, diarrhea, and loss of appetite). Each symptom was scored as a product of severity from 0 (none) to 3 (severe) and frequency from 0 (none) to 4 (daily). This resulted in a GERD symptoms score ranging from 0 to 60 and a non-GERD symptoms score ranging from 0 to 48. The GERD symptoms score has been previously validated [1].
These data were recorded at the time of surgery, then at 6 months, 2 years, and 5 years. All these data were entered into an electronic database.
The patients with normal esophageal contractions were defined as group 1, and the patients with impaired esophageal motility (defined as a mean amplitude less than 30 mmHg of swallow-induced contractions 5 cm proximal to the lower esophageal sphincter) were defined as group 2. The surgical technique has been described previously [2]. In short, a 2- to 3-cm Nissen fundoplication was performed laparoscopically with selective division of short gastrics. Patients with preoperative esophageal dysmotility had a looser fundoplication. No esophageal bougie was used for calibration of the valve.
The results are expressed as mean ± standard deviation in the Results section, and as mean with standard error of the mean (SEM) in the figures. Statistical analysis was performed using the Student’s t test (with two samples assuming unequal variances), and statistical significance was set at 0.05.
Results
Of the 580 patients (380 women and 200 men with a mean age of 45.8 ± 13.7 years), 533 (93.5%) had a normal preoperative esophageal manometry (group 1), and 38 (6.5%) presented with esophageal dysmotility (group 2).
The mean operative time was 58.2 ± 27.6 min, and the mean hospitalization time was 3.3 ± 5.5 days. There was no significant difference between the two groups in terms of surgical approach or intra- and postoperative outcomes [2]. The mean follow-up time was 37.9 ± 24.9 months. Although attempts were made to carry out follow-up evaluation for all the patients, we could achieve only partial follow-up assessment, because of either patient refusal or inability to contact. Clinical follow-up assessment was performed for 96.4% of the patients at 6 months, 54.9% at 24 months, and 54.1% at 60 months. Esophageal manometry was available for 71.2% of the patients at 6 months, 45.5% at 24 months and 25.9% at 60 months.
Esophageal motility
Lower esophageal sphincter pressures were significantly increased in both groups (Fig. 1a). There was also a significant increase in lower esophageal sphincter nadir pressure in both groups (Fig. 1b).

a Modifications in lower esophageal sphincter pressure. b Modification in nadir lower esophageal pressure.
Whereas no significant change in lower esophageal contractile pressure was observed in patients with normal preoperative values, there was a significant increase in contractile pressure in group 2 patients, which continued to the 5-year follow-up assessment (Fig. 2a and b, Table 1).

a Modification in lower esophageal pressure. b Modifications of lower esophageal pressures in group 2 including details.
The patients with severe preoperative esophageal dysmotility (lower esophageal pressures less than 15 mmHg; n = 9) were compared with the remainder of the dysmotility group (n = 29). There was no significant difference in postoperative lower esophageal pressures between the two groups (9.6 ± 5.7 vs 23.6 ± 3.8 mmHg preoperatively; 48.3 ± 36.0 vs 54.1 ± 28.4 mmHg at 6 months; 95.0 ± 91.8 vs 56.5 ± 25.0 mmHg at 24 months; p > 0.05 for the patients with severe dysmotility vs the rest of the dysmotility group).
Esophageal pH monitoring
The patients in group 2 had a significantly higher percentage of reflux time preoperatively (16.9% vs 9.2%; p < 0.05) and a higher preoperative DeMeester score (85 vs 42; p < 0.05). That difference between the two groups disappeared 6 months after surgery, and the two groups were characterized by similarity in reflux times and DeMeester scores for up to 5 years postoperatively (Fig. 3a and b). There was a significant postoperative- decrease in the percentage of reflux time during 24 h, in the number of reflux events during 24 h, and in the DeMeester score in both groups. One patient in the poor motility group had a GERD recurrence at 2 years, with 50.9% reflux time over 24 h and a DeMeester score of 154. When the median is calculated for the same sample, the percentage of time below pH 4 is 2.2, and the DeMeester score is 7.6. Moreover, the wraps were tailored according to the patient’s motility result. When esophageal dysmotility was present, the patient received a looser fundoplication, which may have affected the long-term results.

a Percentage of reflux time during 24 h. b DeMeester score.
Dysphagia
There was a tendency for a higher preoperative dysphagia score in group 2, but that difference was not statistically significant (3.9 ± 4.6 vs 5.2 ± 4.9; p = 0.11). Both groups experienced a significant reduction in the mean dysphagia score after surgery (p < 0.05, Fig. 4). Importantly, the mean postoperative dysphagia score was not significantly higher in the dysmotility group.

Dysphagia score.
In both groups, GERD- and non-GERD symptom scores were significantly reduced, and there was no significant difference between the two groups (Table 2).
Discussion
Impaired esophageal motility is frequently associated with long-standing GERD, and some have suggested a tailored approach when antireflux surgery is required [8]. It is, however, unclear whether partial fundoplications have a lower rate of postoperative dysphagia than total fundoplication. Moreover, the effectiveness of partial fundoplications in controlling GERD symptoms has been questioned, especially in patients with severe esophagitis. Some authors have reported that partial fundoplication for patients with esophageal dysmotility is associated with a low postoperative dysphagia rate and significantly improves GERD-related symptoms, quality of life, and long-term outcomes [8, 9, 11]. However, the only prospective randomized trial comparing LNF with partial fundoplications in patients with esophageal dysmotility reported a higher rate of postoperative dysphagia only at 3 months after LNF, but that difference disappeared after 12 months [5].
In our study, laparoscopic Nissen fundoplication significantly improved esophageal motility in patients with low preoperative esophageal contractile pressures. The fact that this group had higher preoperative acid exposure time may suggest that chronic esophageal inflammation could play a role. Proton pump inhibitors may be insufficient for total control of acid reflux in these patients with severe GERD and impaired lower esophageal clearance. However, the exact mechanism that improved esophageal contractility remains unclear.
Severe postoperative dysphagia is one of the most troublesome complications of LNF. The factors involved can be related to the surgical technique [14] (such as a tight and long wrap or a tight approximation of the crura) or to postoperative complications (slipping of the wrap or intrathoracic migration). One explanation for postfundoplication dysphagia was described by Chrysos et al. [5] as a distortion of the distal esophagus and a restriction in the anatomic opening of the sphincter by the wrap, which creates a sort of partial outlet mechanical obstruction impeding emptying of the swallowed bolus into the stomach. Usually, adequate esophageal peristalsis overcomes the obstacle, and the bolus eventually empties into the stomach. On the basis of this concept, it was speculated that postfundoplication dysphagia is more likely to develop when peristalsis is impaired, and a partial fundoplication was thus advocated for these patients.
The postoperative dysphagia rate is however highly variable, and the surgical technique does not seem to be the only variable. Some authors [4] have reported a 27% rate of severe dysphagia among patients with esophageal dysmotility who underwent LNF. However, as reported earlier, the only prospective randomized trial comparing LNF with LTF (laparoscopic Toupet fundoplication) did not show any difference in the incidences of dysphagia at 1 year [5]. Beckingham et al. [3] also reported low rates of dysphagia for patients with and without esophageal dysmotility who underwent LNF. This fact was supported by Hunter’s [10] study. Our results support these studies and demonstrate that the effect on esophageal motor function is long-lasting. Moreover, patients with preoperative esophageal dysmotility had a tendency for a higher preoperative dysphagia score that returned to similar levels postoperatively.
In conclusion, Nissen fundoplication produces a significant long-lasting increase in lower esophageal sphincter resting and nadir pressures, which control acid reflux. For patients with preoperative esophageal dysmotility (i.e., contractile pressure lower than 30 mmHg), fundoplication also significantly improves contraction pressures up to 5 years. Preoperative esophageal dysmotility should not be considered a contraindication to LNF.
References
Allen CJ, Parameswaram K, Belda J, Anvari M (2000) Reproducibility, validity, and responsiveness of a disease-specific symptom questionnaire for gastroesophageal reflux disease. Dis Esophagus13: 265–270
Anvari M, Allen CJ (2003) Five-year comprehensive outcomes evaluation in 181 patients after laparoscopic Nissen fundoplication. J Am Coll Surg 196: 51–57
Beckingham IJ, Cariem AK, Bornman PC, Callanan MD, Louw JA (1998) Oesophageal dysmotility is not associated with poor outcome after laparoscopic Nissen fundoplication. Br J Surg 85: 1290–1293
Bessell JR, Finch R, Gotley DC, Smithers BM, Nathanson L, Menzies B (2000) Chronic dysphagia following laparoscopic fundoplication. Br J Surg 87: 1341–1345
Chrysos E, Tsiassouis J, O Zoras, E Athanasakis, A Mantides, A Katsamouris, Xynos E (2003) Laparoscopic surgery for gastroesophageal reflux disease patients with impaired esophageal peristalsis: total or partial fundoplication? J Am Coll Surg 197: 8–15
Dallemagne B, Weerts JM, Jehaes C, Markiewicz S, Lombard R (1991) Laparoscopic Nissen fundoplication: preliminary report. Surg Laparosc Endosc 1: 138–143
Fibbe C, Layer P, Keller J, Strate U, Emmermann A, Zornig C (2001) Esophageal motility in reflux disease before and after fundoplication: a prospective, randomized, clinical, and manometric study. Gastroenterology 121: 5–14
Freys SM, Fuchs KH, Heimbucher J, Thiede A (1997) Tailored augmentation of the lower esophageal sphincter in experimental antireflux operations. Surg Endosc 11: 1183–1188
Granderath F, Kamolz T, Schweiger U, Pasiut M, Wykypiel H, Pointer R (2002) Quality of life and symptomatic outcome three to five years after laparoscopic Toupet fundoplication in gastroesophageal reflux disease patients with impaired esophageal motility. Am J Surg 183: 110–116
Hunter J (2004) Invited commentary. J Am Coll Surg 198: 869
Lund RJ, Wetcher GJ, Raiser F, Glaser K, Perdikis G, Gadenstatter M, Katada N, Filipi CJ, Hinder RA (1997) Laparoscopic Toupet fundoplication for gastroesophageal reflux disease with poor esophageal body motility. J Gastrointest Surg 1: 301–308
Mathew G, Watson DI, Myers JC, Holloway RH, Jamieson GG (1997) Oesophageal motility before and after laparoscopic Nissen fundoplication. Br J Surg 84: 1465–1469
Nissen R (1956) Eine einfache Operation zur Beeinflussung der Refluxoesophagitis. Schweiz Med Wochenschr 86: 590–592
Watson DI, Pike GK, Baigrie RJ, Mathew G, Devitt PG, Britten-Jones R, Jamieson GG (1997) Prospective double-blind randomised trial of laparoscopic Nissen fundoplication with division and without division of short gastric vessels. Ann Surg 226: 642–652
Author information
Authors and Affiliations
Corresponding author
Additional information
Presented at the Society of American Gastrointestinal and Endoscopic Surgeons (SAGES) meeting, Fort Lauderdale, FL, 13–16 April 2005
Rights and permissions
About this article
Cite this article
Biertho, L., Sebajang, H. & Anvari, M. Effects of laparoscopic Nissen fundoplication on esophageal motility. Surg Endosc 20, 619–623 (2006). https://doi.org/10.1007/s00464-005-0256-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-005-0256-9