
Abstract
The effects of age and gender on the upper esophageal sphincter’s (UES) and pharyngeal manometric parameters were investigated in 84 healthy subjects (45 men, 39 women, mean age=44 years, range = 18–91). Manometric recordings were performed with solid-state circumferential transducers. Subjects older than 60 years (n = 23) showed a significant lower UES resting pressure. In addition, during water swallows they had a higher UES residual pressure, shorter UES relaxation interval and UES relaxation duration, and a decreased UES relaxation rate. Furthermore, pharyngeal contraction had significant higher amplitude and longer duration in subjects older than 60 years during water swallows. Some of these findings were also observed during cookie and pudding swallows. Women had a higher UES resting pressure and a longer UES relaxation interval than men. The observed changes with increasing age indicate loss of basal tone and decreased compliance of the UES. Increased pharyngeal contraction amplitude and its prolonged duration in the elderly might be compensatory to this. These physiologic effects of age and gender on UES and pharyngeal parameters should be taken into account during analysis of manometric studies.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Problems with swallowing and complaints of globus sensation are quite often reported [1,2]. Manometry is a valuable method to investigate intraluminal pressure changes caused by pharyngeal muscle action and pharyngeal shortening [3]. To accurately interpret the pharyngeal and upper esophageal sphincter (UES) motility of patients, it is important to know if any parameters are changed by age and/or gender. Until now the effects of age and gender on UES and pharyngeal parameters have not been well established. Only a small number of studies have been performed and most of these studies have limitations. These limitations include a small number of subjects, relatively young subjects, studies performed with a sleeve sensor or other unidirectional pressure transducer, and evaluation of only a restricted number of parameters of the swallowing mechanism [4,5,6,7,8,9,10,11,12,13,14]. Both pharyngeal and UES pressures have been shown to have radial asymmetry [15,16,17]. Therefore, it is difficult to interpret studies in which the measurement is performed with a sleeve or unidirectional pressure transducers, since both are able to record pressures in one direction only [15,16,17].
The aim of this study was to investigate the effect of age and gender on UES and pharyngeal manometric parameters in 84 healthy subjects by using circumferential pressure transducers.
Materials and Methods
Subjects
Manometric studies of the pharynx and UES were obtained from 84 healthy subjects (45 male, 39 female, mean age = 44 y, (range = 18–91)). Based on age and gender, subjects were divided into the following groups: age < 60 y (n = 61, 31 male, 30 female, mean age = 33.7 y, (range = 18–59) vs. age > 60 y (n = 23, 14 male, 9 female, mean age = 71.3 y, (range = 61–91); men (n = 45, mean age = 47.1 y, range = 21–91) vs. women (n = 39, mean age = 40.4 y, range = 18–73). No statistical differences in age between men and women was found in the total group (p = 0.15), in the group subjects < 6 y (p = 0.19), and in the group subjects > 60 y (p = 0.15).
None of the subjects had swallowing problems, gastroesophageal reflux disease, diabetes mellitus, neurologic disease, or muscular disorders. Subjects did not use any drug that would affect the gastrointestinal motility. The study was approved by the Institutional Review Board of the Graduate Hospital. Written informed consent was obtained from each subject.
Studies were performed in the Esophageal Function Laboratory of the Graduate Hospital, Philadelphia, Pennsylvania, and the Florida College of Medicine in Jacksonville, Florida.
Equipment
Pharyngeal and UES manometric recordings were performed using an intraluminal solid-state transducer system. The solid-state manometry catheter incorporated two circumferential transducers spaced 3 cm apart and one unidirectional transducer situated 2 cm proximal to the proximal circumferential transducer (Koningsberg instruments, Pasadena, CA). The circumferential transducers sense pressures over 360° which allows accurate measurements of the radial asymmetric UES and pharynx [15,17]. The system is characterized by a low volumetric compliance (7 × 10−6 mm3/mmHg) and an increase in pressure at the rate of more than 2000 mmHg/s [15]. The overall probe diameter was 4.6 mm, and the circumferential transducers had a diameter of 5.2 mm. Pressures were sampled at a frequency of 128 Hz.
Study Protocol
After a 6-h fast, the manometric study was performed with the patient in the sitting position. The manometric assembly was passed through the nose into the esophageal body. A slow pull through at 0.5-cm increments across the UES was carried out to determine UES resting pressure. At each station the catheter was left in place for at least 15 s to allow pressures to stabilize before a measurement was taken. The distal circumferential transducer was then anchored approximately 1 cm proximal to the highest pressure zone of the UES. This position of the catheter compensates for laryngeal elevation during swallowing, allowing the high-pressure zone of the UES to elevate onto the transducer prior to relaxation. The duration of UES relaxation measured with the catheter in this position has been shown to have the best correlation with the opening of the sphincter as measured radiographically [18]. Proper positioning of the catheter is verified by an “M” configuration of the pressure tracing during swallowing [3]. The other two transducers were located in the hypopharynx and pharynx. Pharyngeal and UES manometric parameters were subsequently measured during three series of at least four swallows each of 5 ml of water, 5 ml (1 tablespoon) of pudding, and one-quarter pieces of cookie.
Data Analysis
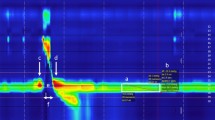
The analysis of pharyngeal and UES pressure tracings was done by computer (Polygram UpperGI, Medtronic Functional Diagnostic, Shoreview, MN). Parameters of pharyngeal and UES mechanics were calculated for each swallow separately (Fig. 1). To determine the pharyngeal mechanics, the onset of the pharyngeal contractions was manually estimated by extrapolating the pharyngeal clearing contraction to baseline (Fig. 1). The onset and end of the pharyngeal contraction were defined as the times that the contraction cuts the level of 5 mmHg above the pharyngeal baseline. The pharyngeal contraction propagation rate was defined as the time difference from the onset of the proximal to the onset of the distal pharyngeal contraction divided by the distance between these transducers (2 cm). The distal pharyngeal circumferential transducer, which was positioned in the pharynx, was used to analyze the remaining pharyngeal parameters [17]. Pharyngeal contraction interval and duration were defined as the time between the onset and the peak of the pharyngeal contraction and as the time between the onset and the end of the pharyngeal contraction, respectively. The amplitude of the pharyngeal contraction was defined as the highest pressure of the contraction with the pharyngeal baseline as reference, and the pharyngeal contraction rate was defined as the pharyngeal amplitude divided by the pharyngeal contraction interval. UES resting pressure and UES residual pressure were measured by using the esophageal baseline pressure as reference. UES residual pressure was defined as the difference in pressure between the nadir of the UES relaxation and the esophageal baseline. The onset and end of the UES relaxation were taken at the times that the UES relaxation cuts the level of 50% of the UES resting pressure. UES relaxation interval and duration were defined as the time differences between the onset and the nadir and between the onset and the end of the UES relaxation. The velocity of the UES relaxation was defined as the difference in pressure between the onset and nadir of the UES relaxation divided by LIES relaxation interval. The coordination between pharyngeal contraction and UES relaxation was studied by taking the time difference between the onset of the pharyngeal contraction and the onset of the UES relaxation and by taking the time difference between the time of pharyngeal peak and onset of UES relaxation.

Schematic of the pharynx contraction and UES relaxation during swallowing. Pharynx proximal: manual estimation by extrapolating the pharyngeal clearing contraction to baseline onset. Pharynx distal: 1 = start of contraction, 2 = peak of contraction, 3 = end of contraction. UES: 4 = start of UESR, 5 = nadir UESR, 6=end of UESR. AP = amplitude pharyngeal contraction, DP = duration pharyngeal contraction, DU = duration UES relaxation, RP = residual pressure UES relaxation.
Statistical Analysis
The results of pharyngeal and UES parameters of each set of four swallows were averaged. Data showed a nonparametrical distribution. Results are presented as medians and the normal range (95% of all data values, 2.5% of highest and lowest values omitted). Mann–Whitney U test was used to analyze the effect of age and gender on pharyngeal and UES mechanics. The effect of gender was studied in the total group and subsequently in the age groups above 60 and below 60 years separately.
Results
Manometric parameters were successfully measured in all subjects for water swallows. In two subjects no cookie swallows were done and in one subject no pudding swallows were done.
Effect of Age
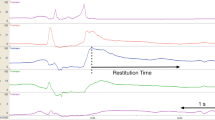
Medians of UES and pharynx mechanics during water swallows for both age groups are shown as a schematic in Figure 2.

A simplified representation of pharynx contraction and UES relaxation based on computer analysis of pressure dynamics for water swallows. This figure shows the significantly decreased UES resting pressure (p < 0.001), increased UES residual pressure (p = 0.001), shorter UES relaxation interval (p = 0.025) and duration (0.046), and a delayed UES relaxation rate in the elderly (p < 0.001). It shows also the significantly higher pharyngeal contraction amplitude (p = 0.028) and longer pharyngeal contraction interval and duration (p = 0.007 and p = 0.012, respectively).
Resting UES pressure was significantly lower in the >60 age group [45.7 (20.3–116.3) vs. 77.8 (33.9–164.7) mmHg, p < 0.001] and showed an inverse correlation with age (Fig. 3). UES residual pressure was significantly higher in subjects >60 y compared with those <60 y during water and cookie swallows [2.5 (−8.4–14.5) vs. −3 (−9.6–12.0) mmHg, p = 0.001 and 1.7 (−13.3–16.3) vs. −4.6 (−15.6–5.0) mmHg, p = 0.002, respectively]. In addition, UES relaxation interval and duration were shorter in the elderly during water and cookie swallows [water: 220.8 (75.0–379.2) vs. 260.1 (132.5–534.7) ms, p = 0.025 and 515.8 (298.2–1087.9) vs. 602.4 (415.3–890.6) ms, p = 0.046; cookie: 140.4 (57.7–236.9) vs. 183.5 (118.8–317.4) ms, p = 0.001 and 415.1 (197.6–788.9) vs. 523.1 (384.9–813.0) ms, p = 0.004].

The association of UES resting pressure with gender and age. A significant (p < 0.001) trend of diminished UES resting pressure by increasing age is shown. UES resting pressure showed a large variety in men and women, but it was significantly higher in women.
UES relaxation rate was significantly lower in the elderly during water, cookie, and pudding swallows [0.09 (0.03–0.21) vs. 0.16 (0.07–0.32) mmHg/ms, p < 0.001, 0.19 (0.03–0.28) vs. 0.25 (0.1–0.48) mmHg/ms, p < 0.001, and 0.14 (0.05–0.37) vs. 0.21 (0.09–0.50) ms, p = 0.001, respectively]. No significant effect of age on UES residual pressure, UES relaxation interval, and UES relaxation duration was observed during pudding swallow [>60 y vs. <60 y: 5.7 (−9.3–21.4) vs. 1.6 (−7.0–15.3) mmHg, 144.6 (60.6–485.7) vs. 184.7 (94.1–346.2) ms, and 488.5 (351.0–1314.5) vs. 544.3 (298.0–835.5) ms, respectively].
Table 1 presents the manometric data of pharyngeal contraction for both age groups during water, pudding, and cookie swallows. Pharyngeal pressures were also affected by age. The elderly had significantly higher pharyngeal contraction amplitude during water and pudding swallows compared with the younger people. A similar trend was observed during cookie swallows but statistical significance was not reached. Pharyngeal interval and duration for all food types were significantly longer in the >60 y group. The onset of the UES relaxation relative to the onset of the pharyngeal contraction pressure was significantly delayed in the elderly during cookie swallows, but not during water and pudding swallows.
Effect of Gender
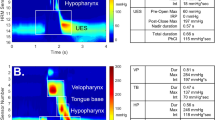
Medians of UES and pharynx mechanics during water swallows for men and women are illustrated in Figure 4. Females had a significantly higher UES resting pressure [85.1 mmHg (23.4–165.1) vs. 56.7 mm Hg (22.4–152.3), p = 0.01] and, during water swallow, a longer UES relaxation interval [281.4 ms (123.1–453.1) vs. 228.9 ms (82.4–445.0), p = 0.003] than males. Similar significant differences between men and women were observed in the <60 y age group but not in the >60 y age group. The young women had a higher resting pressure [90.8 (58.2–167.7) vs. 66.6 (28.8–157), p = 0.006] and a longer UES relaxation interval [283.4 (194.3–509.6) vs. (230.6 (113.3–491.3), p = 0.006] than the young men.

A simplified representation of pharynx/UES mechanics based on computer analysis of pressure dynamics for water swallows of men and women. Females had a significantly higher UES resting pressure (p = 0.01) and longer UES relaxation interval (p = 0.003) than men.
Discussion
The aim of this study was to investigate the effect of age and gender on UES and pharyngeal manometric parameters in 84 healthy subjects. Since both the pharyngeal and UES pressures showed radial asymmetry, in the present study we used circumferential pressure transducers [15,16,17].
This study shows for the first time that all manometric parameters of the UES are affected by age during both water and cookie swallows. UES resting pressure falls, UES residual pressure rises, UES relaxation interval and duration get shorter, and the UES relaxation rate decreases as people age.
UES resting pressure is the most frequently studied manometric parameter of the swallowing mechanism. The current study showed a significantly lower UES resting pressure in the older subjects and a significant inverse relationship between UES resting pressure and age. This phenomenon has been previously described [4,5,6,7,12]. However, Wilson et al. [8] observed only a weak inverse association between UES pressure and age in healthy subjects with an age up to 77 years and no significant difference was found between the 47 people with an age below 60 and the 20 subjects with an age over 60. Two other studies in which UES resting pressure was measured unidirectionally using a perfused sleeve did not detect an effect of age on UES pressure [9,11]. The limited number of subjects used in the Shaw et al. study [9] (n = 23) might be another factor explaining the discrepancy with our study.
The present study shows that subjects older than 60 have a higher UES residual pressure compared with subjects younger than 60. The three previously performed studies on the effect of age on UES residual pressure showed conflicting results. Two studies, performed with a sleeve and which might underrecord UES residual pressure, were not able to detect a significant effect of age on UES residual pressure [9,11]. In addition, one of these studies was performed in only 23 subjects and in the other study UES residual pressure was established during dry swallows. McKee et al. [7] recorded UES residual pressure using a circumferential solid-state transducer and, in agreement with our study, they observed increased UES residual pressure in subjects over the age of 60.
Previous data from our lab showed evidence of a delayed UES relaxation in the elderly [12]. This conclusion was based on the shortened interval from the pharyngeal contraction peak to the nadir of the UES relaxation. The present study confirmed our previous observation as the UES relaxation rate was delayed in the elderly during swallows with all the food types.
Shaw et al. [9] performed simultaneous manometric and fluoroscopic measurements and, based on a higher hypopharyngeal intrabolus pressure combined with a diminished opening of the UES without changes in hololaryngeal elevations in the elderly, they concluded that the UES loses compliance when people get older. No other manometric evidence was observed to support this theory. However, in the present study we observed lower UES resting pressure, shorter UES duration, higher UES residual pressure, and lower UES relaxation rate in the older subjects. These findings reinforce the theory that age affects the compliance of the UES. We agree with Shaw et al. that the most likely reason for this is degeneration of the cricopharyngeal muscle combined with replacement of fibroadipose tissue. This theory is based on similar changes in the cricopharyngeal muscle structure observed in subjects with Zenker’s diverticulum, a group of patients also characterized by an increased intrabolus pressure and diminished UES compliance [19,20]. In addition, the findings that age does not affect the response of UES relaxation to esophageal distention by air nor the increase of UES pressure during esophageal distention by a balloon support the idea that the differences in UES mechanics observed in older subjects are more likely to be a result of changes in the cricopharyngeal muscle than changes in the neurological component of the swallowing mechanism [6].
Data concerning the effect of age on pharyngeal manometric features are contradictory [6,7,8,9,11,12,13,14]. Various studies did not find any effect of age on pharyngeal manometry [9,11,12,13]: One study observed decreased pharyngeal contraction amplitudes in the elderly [14], and three other studies found, in agreement with our study, increased pharyngeal contractions in the elderly [6,7,8]. Confounding factors for these discrepancies are the limited number of subjects, the relatively young age of the subjects, different localization of the pressure transducers, and the use of unidirectional pressure transducers. To overcome pharyngeal radial and longitudinal asymmetry, we used a circumferential solid-state transducer which was placed in the hypopharynx, the position shown to have the highest pharyngeal contractions along the pharynx [17]. Higher pharyngeal contractions were observed in the older subjects compared with the younger subjects during both water and pudding swallows. However, the association between age and the pharyngeal contraction amplitude was quite weak (data not shown). Interestingly, in the older subjects the pharyngeal amplitude shows a larger variability compared with the younger subjects. It might be that some people are able to increase their pharyngeal amplitude in order to overcome the negative changes of the UES mechanics. During cookie swallows no significant effect of age was noted on the pharyngeal contraction amplitude. This is comparable with the results of Shaker et al. [6] who showed a significant increase of pharyngeal contraction amplitude during water swallows but not during swallows with mashed potato. Our overall pharyngeal contraction amplitudes during cookie swallows were significantly higher than those during water and pudding swallows. This might suggest that during cookie swallows the contraction amplitude had already reached its physiological limit and subsequently could not be increased further in the older people.
Oropharyngeal dysphagia is presented more frequently by older than by younger subjects [21,22,23]. Obviously, one reason is that diseases with oropharyngeal dysphagia as a contributing factor are more common in the elderly [21,22]. In addition, it is possible that the decreased UES function in the elderly makes them more sensitive to small changes in swallow function and thus they more readily develop symptoms of dysphagia. Possibly those elderly patients who are unable to compensate by increasing pharyngeal contraction will experience difficulties with swallowing as the UES function diminishes with age.
One interesting finding is that females have higher UES resting pressure than males. This was observed in both the total group and in the age group <60 years old. In contrast, this difference was not observed in the elderly. This could be a reflection of the overall lower UES resting pressure in this age group or it might be a type two (β) error. In addition, in the total group but not in the individual age groups, women had an increased velocity of the UES relaxation compared with men during pudding and cookie swallows. This might be a compensatory mechanism to the increased UES pressure to prevent coordination problems between UES relaxation and pharynx.
A limited number of studies have been performed on the effect of gender on UES pressure, and a gender-related effect was not found in any of these studies [7,8,9,10,11]. Again, this might be due to the limited number of subjects investigated or the fact that the UES was measured without using a circumferential transducer.
In summary, the described changes of manometric parameters of the UES with increasing age indicate a loss of basal tone and a decrease of compliance of the UES. The improvement of pharyngeal function in the elderly might be a compensatory mechanism to this decreased function of the UES. Manometric parameters of the UES and to a lesser extent, of the pharynx are influenced by gender. These physiologic effects of age and gender should be taken into account during analysis of normal values of UES and pharyngeal parameters, since this may affect regular patient care and research design.
References
S Lindgren L Janzon (1991) ArticleTitlePrevalence of swallowing complaints and clinical findings among 50–79-year-old men and women in an urban population. Dysphagia 6 187–192 Occurrence Handle1:STN:280:By2C3snosVA%3D Occurrence Handle1778094
ME Groher R Bukatman (1986) ArticleTitleThe prevalence of swallowing disorders in two teaching hospitals. Dysphagia 1 13–16
JA Castell DO Castell (1993) ArticleTitleModern solid state computerized manometry of the pharyngoesophageal segment. Dysphagia 8 270–275 Occurrence Handle1:STN:280:ByyA28rjtFc%3D Occurrence Handle8359050
W Pelemans G Vantrappen (1985) ArticleTitleEsophageal disease in elderly. Clin Gastroenterol 14 635–656 Occurrence Handle1:STN:280:BimC3cnotlM%3D
TR Weihrauch P Vallerius H Alpers (1980) ArticleTitleAssessment of various factors influencing esophageal pressure measurements. II. Significance of physiological factors in intraluminal manometry. Klin Wochenschr 58 287–292 Occurrence Handle1:STN:280:Bi%2BC1crpsVM%3D Occurrence Handle7374097
R Shaker J Ren B Podvrsan W Dodds WJ Hogan M Kern R Hoffmann J Hintz (1993) ArticleTitleEffect of aging and bolus variables on pharyngeal and upper esophageal sphincter motor function. Am J Physiol 264 G427–G432 Occurrence Handle1:STN:280:ByyB3M3otFw%3D Occurrence Handle8460698
GJ McKee BT Johnston GB McBride WJ Primrose (1998) ArticleTitleDoes age or sex affect pharyngeal swallowing? Clin Otolaryngol 23 100–106 Occurrence Handle1:STN:280:DyaK1c3lvFGltA%3D%3D Occurrence Handle9597278
JA Wilson A Pryde CCA Macintyre AGD Maran RC Heading (1990) ArticleTitleThe effects of age, sex and smoking on normal pharyngeal motility. Am J Gastroenterol 85 686–691 Occurrence Handle1:STN:280:By%2BB1c3itV0%3D Occurrence Handle2353687
DW Shaw IJ Cook M Gabb RH Holloway ME Simula V Panagopoulos J Dent (1995) ArticleTitleInfluence of normal aging on oral-pharyngeal and upper esophageal sphincter function during swallowing. Am J Physiol 268 G389–G396 Occurrence Handle1:CAS:528:DyaK2MXkslKiu7c%3D Occurrence Handle7900799
IJ Cook J Dent SM Collins (1989) ArticleTitleUpper esophageal sphincter tone and reactivity to stress in patients with a history of globus sensation. Dig Dis Sci 34 672–676 Occurrence Handle1:STN:280:BiaB3s7jtFc%3D Occurrence Handle2714142
J Robbins JW Hamilton GL Lof GB Kempster (1992) ArticleTitleOropharyngeal swallowing in normal adults of different ages. Gastroenterology 103 823–829 Occurrence Handle1:STN:280:By2A28zhsFM%3D Occurrence Handle1499933
SR Fulp CB Dalton JA Castell DO Castell (1990) ArticleTitleAging-related alterations in human upper esophageal sphincter function. Am J Gastroenterol 12 1569–1572
JA Wilson A Pryde CCA Macintyre RC Heading (1989) ArticleTitleNormal pharyngoesophageal motility: a study of 50 healthy subjects. Dig Dis Sci 34 1590–1599 Occurrence Handle1:STN:280:By%2BD3cvnvV0%3D Occurrence Handle2791811
JF Tracy JA Loggemann PJ Kahrilas P Jacob M Kobara C Krugler (1989) ArticleTitlePreliminary observations on the effect of age on oropharyngeal deglutition. Dysphagia 4 90–94 Occurrence Handle1:STN:280:By%2BA383ot1A%3D Occurrence Handle2640185
JA Castell CB Dalton DO Castell (1990) ArticleTitlePharyngeal and upper esophageal sphincter manometry in humans. Am J Physiol 258 G173–G178 Occurrence Handle1:STN:280:By%2BC28vns1M%3D Occurrence Handle2305883
CS Winans (1972) ArticleTitleThe pharyngoesophageal closure mechanism: a manometric study. Gastroenterology 63 768–777 Occurrence Handle1:STN:280:CSyD38vjt1c%3D Occurrence Handle5079487
VW Sears JA Castell DO Castell (1991) ArticleTitleRadial and longitudinal asymmetry of human pharyngeal pressures during swallowing. Gastroenterology 101 1559–1563 Occurrence Handle1955121
PJ Kahrilas WJ Dodds J Dent JA Logeman R Shaker (1988) ArticleTitleUpper esophageal sphincter function during deglutition. Gastroenterology 95 52–62 Occurrence Handle1:STN:280:BieB38rptlY%3D Occurrence Handle3371625
FMS McConnel D Hood K Jackson A O’Connor (1994) ArticleTitleAnalysis of intrabolus forces in patients with Zenker’s diverticulum. Laryngoscope 104 571–580 Occurrence Handle1:STN:280:ByuB2cjitlA%3D Occurrence Handle8189989
IJ Cook P Blumbergs K Cash GG Jamieson DJ Shearman (1992) ArticleTitleStructural abnormalities of the cricopharyngeus muscle in patients with pharyngeal (Zenker’s) diverticulum. J Gastroenterol Hepatol 7 756–562
N Sheth WC Diner (1988) ArticleTitleSwallowing problems in the elderly. Dysphagia 2 209–215 Occurrence Handle1:STN:280:BiaB1cbhsVM%3D Occurrence Handle3251696
DO Castell (1990) ArticleTitleEsophageal disorders in the elderly. Gastroenterol Clin North Am 19 235–252 Occurrence Handle1:STN:280:By%2BA3cjhs1A%3D Occurrence Handle2194944
H Siebens E Trupe A Siebens (1986) ArticleTitleCorrelates and consequences of eating dependency in institutionalized elderly. J Am Geriatr Soc 34 192–198 Occurrence Handle1:STN:280:BimC2c7jslw%3D Occurrence Handle3950287
Author information
Authors and Affiliations
Corresponding author
Additional information
The first author was financially supported by the Netherlands Digestive and Disease Foundation and the Netherlands Organization for Scientific Research (NWO).
Rights and permissions
About this article
Cite this article
van Herwaarden, M.A., Katz, P.O., Matthew Gideon, R. et al. Are Manometric Parameters of the Upper Esophageal Sphincter and Pharynx Affected by Age and Gender? . Dysphagia 18, 211–217 (2003). https://doi.org/10.1007/s00455-002-0099-7
Issue Date:
DOI: https://doi.org/10.1007/s00455-002-0099-7