
Abstract
Health-care research relies largely on human materials stored in highly specialised biorepositories. Medical translational research on tissues can be performed using a variety of resources in distinct situations. The best known is the secondary use of pathology archives where paraffin-embedded tissues are stored for diagnostic reasons. Another is collecting and storing frozen material obtained from leftover surgical diagnosis. Such residual tissues can either be used directly in research projects or used in the context of a clinical trial with new interventional medicinal products. The latter can make the regulations governing the use of these materials for medical research much more complicated. The use of residual materials is very distinct from biobanking projects for which tissue is specifically collected. This article describes the consequences of using residual human material from different sources in distinct situations and why signed informed consent is not always the preferred choice of individual countries regarding the use of residual material. In addition, signed informed consent is overdone when using residual tissues in medical research. We maintain that the opt-out system is a balanced choice if certain requirements are met, relating to sufficient transparency about using residual tissue for research, the purpose of such research and to the confidentiality of the data used in that research. Finally, the international exchange of samples can be based on the laws and regulations of the countries of origin. Respecting these form the basis of what can and cannot be done in the country where the research on the samples is being performed.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Today, high-quality collections of human material with accompanying clinical data, especially those with long-term follow-up data are in high demand for medical translational research. Such well-defined high-quality human samples form the basis of finding the answers in personalised medicine as well as molecular target identification. Research on these samples also has the potential to bring prognosis increasingly closer towards prediction, thereby fulfilling the most promising innovations in modern medicine, such as personalised medicine, drug target identification and prediction of progression. Such research, however, requires high statistical power and must therefore be based on large quantities of samples (Foekens et al. 2008; Janssens and van Duijn 2008a, b; Ioannidis 2009; Bates 2010; Diamandis et al. 2010). These quantities can no longer be collected in one institute or research group in a foreseeable amount of time. Hence, samples from different institutes need to be combined in large multi-centre studies. This requires that samples and data be collected in a harmonised or, yet better, standardised way. The custodian of the collection has a pivotal role in this respect. In addition, good research infrastructure as well as a regulatory basis, which is both efficient and acknowledges the interests of donors and their trust in such research, is required (Allen and McNamara 2011; FEDERA 2011). Both are instrumental in enabling an expedient exchange of samples not only at a national, but also at an international level. Most guidelines only cover research with human materials and tissues especially collected and taken from volunteers (such as OECD 2009). However, conditions differ between research based on residual tissue and tissue which is collected directly from the patient in the form of biopsies especially for research purposes only.
A distinct approach is needed to structure research with residual tissue. In this paper, we investigate the preconditions for such research, both from a scientific and more technical point of view and regarding the regulatory and ethical aspects.
Repositories of residual tissue
Collections of fresh frozen tissue and formalin-fixed and paraffin-embedded (FFPE) tissues can be found in both pathology archives derived from surgical resection specimens or during autopsy. The pathology archive consists of FFPE diagnostic material and in most cases, depending on the local law and legislation, may need to be stored for several decades. Such material can be used for medical research, but then the original lesion must be kept and the material returned after the research is performed. The big advantage of FFPE material is that there is a large quantity of samples available. Although formalin fixation can be seen as a standardised method because it is used in most pathology laboratories all over the world, derivatives such as DNA, RNA and proteins are generally of poor quality. In addition, there is a wide variety in quality due to the variation in fixation times and storage conditions. Although today this quality is still adequate for diagnostic purposes mainly because of the high-quality conservation of tissue morphology, it is not suitable for many research purposes. Therefore, pathology departments in academic hospitals with an interest in translational research need to snap freeze and store fresh tissues in freezers and liquid nitrogen tanks for research purposes.
Such tissues are usually taken from surgically removed tissues for curative or diagnostic reasons. Parts of these specimens are necessary for the diagnostic analysis, whereas the rest of the specimens are left over to be destroyed or archived for research if they fit in the inclusion criteria of the collection. If parts of a specimen are stored for research, the diagnostic purpose should come first, requiring that the distinction is made on the fresh surgical specimen at the cutting room under supervision of, or preferably by, a pathologist.
Surgical specimens taken for curative reasons without the need of a pathology diagnosis do not require a pathologist. In this case, the custodian of the collection could make arrangements with the surgeon if those specimens are to be embedded in the collection, to ensure their value for research, such as timelines to arrive at the collection, temperature during that interval, etc. Frozen tissue samples should be dealt with diligently with sufficient annotation of the circumstances under which they were taken from the patient. See Text Box 1 of Appendix on the life cycle of frozen tissue samples.
It should be mentioned that alongside collections of the residual tissue already discussed, other collections of residual tissue can under certain circumstances be considered for tissue banks for medical research as well, such as samples kept at microbiological laboratories. Additionally, the phrase ‘tissue bank’ (with tissue taken from patients) can be confusing. There are also ‘tissue banks’ that store and process tissues for use as transplants or implants. However, due to safety issues a completely different regulatory regime applies here (e.g. European Directive 2004/23/EC).
The scientific advantages and challenges of research via residual tissue
Research with residual tissue can show an impressive track record of valuable results relating to the disease, treatment regime and outcomes of treatment interaction (Foekens et al. 2008; Bates 2010; Diamandis et al. 2010). Research with residual tissue by definition means that research does not have to wait until the donor acquires a medical condition, which is then connected with the analysis of the sample. Research on tissue without accompanying data is senseless. Clinical data or environmental data and lifestyle data, or a combination of the two, are necessary. Clinical data can range from diagnostic to complete follow-up data (Bevilacqua et al. 2010), whereas the environmental data can range over the categories as listed in P3G datashaper (Fortier et al. 2010). All these differences have their purposes in the field of medical research.
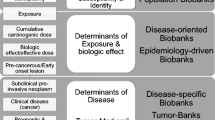
When using residual tissue for research, the medical history of the patient is well recorded and so in general are the outcomes of treatment and disease. Environmental and lifestyle data are usually less known for residual samples in comparison to the population-based biobank samples. The population-based samples mostly do not cover the clinical data acquired from patient records. This might be perceived as limits to the scope of research for both the collections, but in fact illustrates that both types of research are complementary, serving optimally in their research niche. Hence, residual materials collected in a hospital setting offer the optimal opportunity to perform research on the development and progression of disease as well as on the behaviour of disease susceptibility markers in different disease stages. In this way, the potential and the behaviour of a susceptibility marker as biomarker of prediction or progression, and response or drug target can be further investigated. It would be a waste to use such well-documented materials only as validation of susceptibility markers identified in other studies.
Alongside regulatory issues, research with residual tissue faces specific scientific challenges. The repositories of one institution are usually too small to acquire sufficient tissue and data. This requires a research infrastructure by which various institutions can collaborate. That infrastructure can be more or less formal and more or less permanent. Permanent infrastructures require investment in a database that shows which and where a tissue is available and under what conditions it can be used. An example of such an infrastructure is OECI-TuBaFrost (Riegman et al. 2010), as well as NCI-OBBR and BBMRI. (Vaught et al. 2010; The International Cancer Genome Consortium 2010; Moore et al. 2011). The main scientific challenge for collaborative efforts is the lack of standardisation of tissue retrieval and storage as well as data annotation (Moore et al. 2011). Especially in Europe, there is a variation in languages and morphologic and disease coding tables. Networks in such a highly variable field can make use of a slim design as used for OECI-TuBaFrost (Riegman et al. 2010) by making samples visible in a catalogue of biobanks only accessible after controlled registration, where only the aspects of the biobank as well as the collections and only the amount of samples without clinical data are stored. The requestor specifies the samples precisely. In addition, a sample exchange platform can be coupled where participants can work in projects coordinated by one of the participants. The project environments are only accessible by participants after permission of the project coordinator.
Ethical and regulatory issues
Research with residual tissue also faces its own ethical and regulatory challenges. Biobanks based on tissue especially collected (and retrieved from the donor) for research have been set up for such research and have by definition their own specially created governance structure. (see e.g. http://www.p3gobservatory.org or http://www.ukbiobank.ac.uk) Repositories of residual tissue are embedded in the clinical facility and lack such governance structures ab initio. When tissue is retrieved directly from the patient for research purposes only, there is by definition a moment where the nature of the procedure and the project can be explained (and must be explained). That moment is lacking when tissue is taken in the course of the treatment of the patient. Often at that moment, it is even unsure whether a part of that specific sample will be used for research.
Regarding the recent topic of individual feedback of findings or results, there are differences as well. Though that might change in the future, all population biobanks in Europe known to us exclude at the moment individual feedback of results of research. Such results should be distinguished from results obtained by screening, which the volunteer might undergo when enrolling in the project, such as that in the UK Biobank or Lifelines in the Netherlands (http://www.lifelines.nl). Individual feedback of results from research with tissue can only have added value if the validated results can have any practical meaning for the donor or perhaps his or her relatives, in terms of
-
1.
self-management (lifestyle and or screening) to prevent the onset of disease or aid in a timely diagnosis or
-
2.
an increased choice of a treatment regime once the donor has acquired the specific condition (either in terms of medical outcome or in options for informed consent) and
-
3.
which would not have reached the donor in a timely manner without this individual feedback.
Based on those criteria, the difference with residual tissue is apparent. Research with residual tissue is performed when the donor has already acquired the disease, whereas validated results usually only become available years after the donor had been treated for that disease. This difference has to be taken into account, in addition to the usual conditions when considering individual feed-back. The results must have been validated, though it is debatable when results can count as being validated (Dressler 2009) and those results must relate to that specific individual. Research on samples is done for statistical analysis and not by a diagnostic laboratory with a system of quality assurance to avoid swapping from one vial to the other and from one expert to the other. Therefore, a switch or cross-contamination of samples may have taken place during research and results of research can never be translated one to one to an individual. At least a new test based on the material still available at the repository should come first. There might be exceptional cases where feedback of a result might be potentially life saving. Insofar as possible, given the pseudonymisation procedures, such feedback should be tried then. Usually, this will concern an incidental finding and not new scientific findings.
Consent modalities for residual tissue
Several consent modalities have been proposed for research with tissue, ranging from specific consent for each research protocol in which the tissue is used to opt out (Trouet 2003). It seems that at the moment ‘broad consent’ is considered a sufficient consent modality for population biobanks, if the proper governance of such biobanks is sufficiently assured (Campbell 2007; Allen and McNamara 2011). In some countries [such as Denmark, France (van Veen et al. 2006) and recently Belgium (Belgian Act 2008)], the possibility to opt out is considered a sufficient consent modality for the use of residual tissue for research. However, as tissue is always accompanied by data, regulations on the use of tissue should always be read in conjunction with the data protection legislation, which in France is rather strict (van Veen et al. 2006). In a recent consensus document, which included the active participation of patient organisations, the opt-out system has been adopted in the Netherlands as well (FEDERA 2011), however, only if certain conditions are met. These are in brief as follows:
-
There should be full transparency about research with residual tissue. The possibility that residual tissue can be used for research must be made known to the patients visiting the facility. The information should be more than one or two lines ‘hidden’ in the general information leaflet of the hospital. Many university hospitals in the Netherlands have at the moment separate brochures about ‘further use’ of residual tissue for research, which is handed to every patient before undergoing a diagnostic procedure involving taking tissue. Both doctors and the patient information desk at the facility should be prepared to answer additional questions. Though the initiative to object or opt-out must come from the patient, the procedure must have a low threshold. The above-mentioned brochures have a form which the patient can take out and on which he can indicate to opt out. The form can be left at the hospital or sent free of charge later. But simply indicating the wish to opt out to the treating physician or at the patient information desk is possible as well. There should be a procedure at the hospital where opt-outs are administered and notified to the custodians of a collection. The brochure stresses that a patient who has opted out will still receive the best available care.
-
The tissue and accompanying data must be coded-anonymous (van Veen et al. 2006), or in terms of ISO 25237 pseudonymised (ISO 2008) for research, or fully anonymous. However, the latter will usually be impossible for more refined genotype, phenotype, treatment regime and outcomes interaction research. There is considerable confusion about both the concepts of ‘anonymous’. (See Text Box 2 of Appendix for a clarification).
-
The research must be geared towards important health-care questions and hence there must be the reasonable expectation that the results of this research will benefit future patients. Research with residual tissue such as to determine factors influencing criminal behaviour or as an alternative to the use of animals for safety tests of cosmetic products cannot be based on this opt-out system.
-
Insofar as still practically possible, because of the anonymisation procedures, opt-out at a later stage must be honoured.
-
Partnering with commercial parties is not excluded, and neither is the patenting of results when applicable. Yet, the ownership of the tissue must remain within the not-for-profit research groups, which initiated the research and the potential profits of this partnering must strengthen the capacity of these groups to perform more research.
-
The specific protocol, in which the tissue is used for research must have been approved by a research ethics committee, which should ascertain that the above-mentioned conditions have been met.
The ethical basis of this approach is the following:
-
Research on residual samples is observational research (van Veen 2008). Such observational research should be distinguished from research which is ‘interventional’ in the following sense: for research that affects the justifiable expectation of a patient or healthy volunteer, a doctor should always take the patient’s definition and interests in the pursuit of his or her life plan first and should offer the best available treatment if that plan is jeopardised by disease. The origin of all earlier international documents on informed consent is a necessary—but not sufficient—condition to execute medical research related to this interventional research (Bergkamp 1988; Brody 1998; Faunce 2005; Plomer 2005). Medical trials fall in this category, but also taking tissue from the patient by means of biopsies for research purposes only is included. In contrast, the patient’s life plan is not affected by observational research, which is executed in the background of health care and optimal treatment according to present standards. This conclusion makes a huge difference, ethically and legally. In much of the ethical debate, the concept of ‘research involving human subjects’ has been broadened to where already existing tissue and/or data of patients are used for observational research. An example is Lévesque et al. 2009 where the many provisions in (international) documents which indicate that in certain situations the principle of informed consent is not applied are seen as exceptions instead of questioning whether the principle, as derived from the original rationale mentioned, to protect persons against interventional research would be applicable at all in those situations.
-
There can and often should be other good reasons why some form of consent should be applied in those situations. However, these reasons are not that the patient is subjected to research but that data and tissue are submitted to pathology for diagnosis or to follow up the course of treatment, are used for a secondary purpose. These purposes vary greatly and can range from, alongside the examples given already, quality control and teaching of laboratory assistants to the development of a commercial cell line or, as came to light in a Dutch disciplinary court case, to train rescue dogs.
-
Hence the issue here is much more a question about the extent of the patient’s autonomy to decide on secondary uses of tissue (and data) than of protecting patients against research. Without question, the patient’s autonomy should result in explicit consent regarding the last two mentioned purposes. In the context of observational research with tissue as described in the FEDERA Code of Conduct, such autonomy should be first of all seen in the context of the European solidarity-based health-care system. Such health-care systems provide equal access to care, based on need, (Charter 2007; Den Exter 2008) with procedures for quality control and costs containment to assure long-term affordability for all (European Commission 2001). Care for all, as defined by the statutory provisions giving access to health care, should be according to the best professional standards. This standard of care is based on much preceding research to which many have contributed. Just as some members of society contribute within the solidarity-based health-care system financially, it serves the justice of this system if it may be assumed that a patient, who profits from the collective learning capacity of this system based on contributions of many other patients, also contributes to better health care for others as well, as long as and insofar as the conditions mentioned apply. Such an approach does not place ‘autonomy’ regarding ‘further use’ of residual tissue for research first. Autonomy cannot be the only value for societal arrangements (O’Neill 2002) and additionally can be seen as encompassing wider values than pursuing one’s self-interest (O’Neill 2002; Campbell 2011). A balance between research for the public good and private interests must always be struck (The Academy of Medical Sciences 2011). Within that balance there should be—under certain conditions—room for other values such as solidarity (Knoppers and Chadwick 2005; Hoedemaker et al. 2007) or ‘citizenship’ as the basis for contributing to research with residual tissue (Swierstra 2004).
This might not be sufficient reasons not to grant the patient full decision power to the ‘further use’ of residual tissue. However, such a system faces various hindrances and could result in, as has been described elsewhere, the ‘tragedy of the anti-commons’ (Bovenberg 2006).
-
The consulting room would not be the best place to ask for such consent. Contrary to when tissue is specifically taken for research purposes only as in the case of biopsies, there is not a special moment when the nature of research with tissue can be explained. The dialogue between doctor and patient is already sufficiently complicated to arrive at full informed consent and understanding of what really matters in the consulting room: the possible diagnostic and treatment options or sometimes, regretfully, the absence of realistic options, especially when potentially life-threatening diseases are involved.
-
Hence, this consent should be asked at another occasion. To be a true consent, it should be asked, at an interview (see Mancini et al. 2010, where many patients did not remember having given consent based on a simple form) and by someone else than the treating doctor, like a specialised nurse. We made a small calculation of the costs of such a procedure and arrived at 45 min by a staff member for each sample, which will be included. The interview with the patient will be shorter, but the majority of the consented samples will not result in inclusion of the sample in the residual tissue bank. Most samples are too small for that purpose and are completely needed for the original diagnostic purpose, or they arrive after closure of the pathology laboratory and cannot be freshly frozen. Hence, every potential suitable patient will be asked for consent even if it later proves that, when consent has been given, the sample is not suited or used for inclusion. In addition, there will be cancelled appointments, administrative work, etc. Assuming that this staff member does nothing else, like following courses, and based on the overall working time, thus excluding holidays and overall salary costs for the employer of a medium level staff member, it would amount to about Euro 100 for each included sample. Even then, the administrative costs at the residual tissue bank to administer the various options and assure that tissue is released for research according to those options have not been taken into account.
-
There is sufficient evidence that informed consent to use patient data for health research leads to ‘bias’ in the research data (Jacobsen et al. 1999; Wolf et al. 2000; Al-Shahi et al. 2005; Jusilahti et al. 2005). There is no reason why this would not apply to the ‘further use’ of tissue for research and recently the chance of bias has been suggested in this context as well (Mancini et al. 2010).
These practical hindrances will never be allowed to trump the precedence of the well-being of the individual research subject over all other interests, as stated in the Declaration of Helsinki (article A.6, WMA 2008). However, as argued, this is not about endangering in any way the well-being of the research subject. It might even be very well argued that the patient is not a research subject. The patient’s well-being will not be affected, other than the notion that this should not happen with his or her tissue. Balanced against the promises for the public good, a well-organised opt-out system leaves sufficient room for those potential donors. As mentioned, this approach has the full support of the Dutch patient organisations. They have forwarded a new basic right, which should mitigate to some extent the right to autonomy of individual patients regarding ‘further use’ of data and tissue, namely the right to innovation and better treatment (Van der Valk 2010). It follows from the above that some caution must be taken following this approach. Patients must have a reasonable expectation that results will come back as treatment available to all in the health-care system. This expectation only holds in solidarity-based health-care systems, like the western European ones, where patients will have equal access to health care, including new therapies when validated and incorporated in the health-care system based on need and irrespective of income or former contribution to a tissue repository.
What about patient’s preferences?
Much empirical research has been done about preferences of the population at large and of patients regarding the use of tissue for research (amongst many: Wendler 2006 for a meta-study on surveys, Kettis-Lindblad 2005; Kaphingst et al. 2006; Mezuk et al. 2008; Melas et al. 2010; Mancini et al. 2010; Allen and McNamara 2011). All these studies differ in design, such as quantitative surveys or in-depth qualitative interviews, sample size and whether the issue was ‘further use’ of residual tissue for research or participation in population-based biobanks. Especially, purely quantitative surveys should be taken with caution. The responses can also reflect how the questions were framed and will certainly reflect the background cultural values and attitude towards the health-care system, which will be different between the USA and Europe, for example, and might also be different between European countries. Yet, all studies provide valuable insights into points to consider: most studies indicate ‘helping others’ as the prime basis for contribution. The threshold to contribute to ‘commercial’ studies would be much higher, which the FEDERA Code of Conduct addresses, without endorsing the naïve view that academic research should not liaise with commercial parties for the development and marketing of new test kits or pharmaceuticals. The previously mentioned general information to patients must explain this as well. A quantitative study in the Netherlands showed that the general public is by and large unaware of ‘further use’ of tissue (Rathenau Instituut 2009). This is a very important warning sign that much more should be done with respect to transparency about ‘further use’ of tissue. The Wendler 2006 survey seemed to favour demanding more influence than expressed by the patient organisations, which contributed to the FEDERA Code of Conduct and its opt-out system, but yet could lead to such a system as well. A more nuanced, both quantitative and qualitative, study in the Netherlands suggested that most patients would be at ease with an opt-out procedure. They expect research on residual tissue and do want to be informed about it with the possibility to opt out. Yet, in general they do not want to be bothered with consent procedures for possible research taking place in the background (Vermeulen et al. 2009).
Even more important is the “is-ought” divide. Insofar as relevant here, this means that though most people will probably respond, again depending on the framing of the question, but given a simplistic questionnaire, they prefer lower taxes, which does not mean that taxes should become lower. The same applies here. It is ultimately a moral choice, made by a given society, as to how we may use residual tissue for research.
No such choices can lead to a utopian world. In the proposed system, it might happen that a patient did not read the brochure and the tissue was included, while the patient would have opted out if he or she had read it. With written informed consent based on a simple form, a patient might sign assuming that it was necessary for his or her treatment. Even with the interview-based approach, consent might be based on therapeutic misconception, as even happens in clinical trials where informed consent is based on an extensive patient information form and a waiting period (Van Leeuwen 2008). Tissue might have been used for research while the patient regrets this choice. Opt-out at a later stage or withdrawal of consent will come too late for research which has used his or her samples already. Complicated systems have been proposed to allow the donor ‘micromanagement’ of the use of tissue for research through a Web-based interaction with the tissue repository, such as in Nietfeld et al. 2011. Such need for micromanagement does not seem to follow from the above-mentioned empirical research. All Web-based systems for communication between donors and custodians of tissue which involve personal data, such as preferences about use of tissue for research and even more about possible individual feedback, are likely to attract hackers and it seems to us that security leaks can never be fully avoided. Additionally, these more intricate consent systems detract scarce funds from patient care and research.
The assumption of the opt-out system is that patients are willing to contribute to the public good. That assumption can be repudiated, but it will be the patients’ responsibility to do so. It should be mentioned that the FEDERA Code of Conduct, further to the safeguards mentioned in this paper, also has provisions about good research governance for researchers. These will not be discussed here, as the focus in this paper is the consent system and the role of the custodian of residual tissue.
The role of the custodian of the repository
The opt-out system must be organised upfront by the medical facility (Bevilacqua et al. 2010). The collection is held by a ‘custodian’ of the repository of residual tissue (Yassin et al. 2010). (S)he has a pivotal role and acts as the manager of the resource. The life cycle of tissue (Text Box 1 of Appendix) must be assured here, until the tissue is released for research. The first responsibility is that residual tissue remains available to the pathologists to answer additional diagnostic questions at a later stage of the patient’s treatment. The patient’s interests come first and residual tissue for research means surplus residual tissue from that perspective. In the second place, the custodian or biobank manager must arrange that released tissue arrives at the researcher coded-anonymously and that tissue from patients who have objected are not included. Fair and transparent procedures should be in place to handle requests to release tissue for research. Furthermore, it must always be known which tissue is released to whom and in the context of which project. The FEDERA Code of Conduct states that the custodian should draw up an annual report which describes the release of tissue along these lines in the preceding year. That annual report should be submitted to the council of patient representatives, which, according to Dutch law, every Dutch hospital must institute. This council can make comments to which the board of the hospital must respond. If the patient wishes to opt out at a later stage, the tissue must be destroyed if not already used for research. In the latter case, if there is any link between the code and the patient, that link must be removed.
Amongst other things, this means that an investment is needed in a sound sample tracking system for the biobanked samples that not only performs the tracking within the biobank, but is also capable of tracking where the sample is at the moment it is being used for research purposes. The tracking system should also keep track of by whom, what and when changes are made to the database of the tracking system (Mills and Brooks 2010). Furthermore, it should facilitate the two-tiered approach, where a code number can be used in the repository, which still has a link to the patient data, and the biobank manager can remove the hospital code linked to the patient data and add a second code number or pseudonym when the tissue is released for research. Biobank personnel need to be able to work with the hospital coding, so that they can still perform the standardised biobank QA and QC programme on the samples (Moore et al. 2011) and keep the material available for further diagnostic questions.
The challenges to considering research with residual tissue as observational
Research with residual tissue, as described here, is observational research and cannot affect the life plan of the donor, at least not directly or in any negative way. This tenet is challenged by stressing the ‘risks’ of this research (like by CIOMS 2009; Ploem 2010). These risks would fall into two categories. The first is that it cannot be guaranteed that the donor whose data and or tissue are used coded-anonymously (see the Text Box of Appendix) for research will not be re-identified in the research domain. The second is that this research can lead to unwanted social consequences, like discrimination.
The challenge to non-re-identification
This challenge relates to the identifiability of DNA and to the phenotype and other data (exposure, onset of disease, response to treatment, etc.) with which the analyses of the tissue are matched.
The tenet that DNA is always identifiable has been called ‘unnecessarily extreme’ (Lowrance and Collins 2007). That was before it was found that if more than one data bank hold parts of the genomic data of individuals from various studies, they can be uniquely linked to the individuals concerned (Homer et al. 2008), though only under extraordinary circumstances using highly sophisticated analytical tools (Braun et al. 2009). Of course, when tissue is issued to a researcher, in principle, full sequencing would be possible. The idea that the privacy of the donor cannot be guaranteed has been forwarded with new zeal (like Curren et al. 2010).
It is still ‘unnecessarily extreme’. To move from coded DNA data to the identity of the patient, the researcher must access different databases with DNA data to which the identity of the patient is attached. In addition, one would need profound knowledge of what sequences from the total sequence data to compare to the identifying database. Moreover, one should also have profound knowledge on how to compare such data to the identifying database, where (key) information is stored in a completely different way. The other theoretical possibility to re-identify would be linking the phenotype following DNA analysis of the donors to a database holding phenotypes with identities attached, or which can be retrieved using new search tools, and which is shown in that database, (e.g.via Facebook or an Internet group where patients discuss their disease). These are all very abstract, theoretical and unlikely scenarios. If a researcher would consider foul play to identify individuals, easier routes are available.
A more serious challenge is that seemingly anonymous data about a patient in the research domain can be used to re-identify persons through matching with public resources on the Internet, such as the yellow pages, Facebook, etc. This type of re-identification is theoretically much less hypothetical (Ohm 2010). On a practical level, it would still assume bad faith on the side of researchers.
This challenge can be met in two ways. One way is by striving for absolute anonymity in the research domain. Technical solutions have been forwarded in this respect, such as the ‘datashield’ (Wolfson et al. 2010). Though data release to the research domain should always be as minimal as possible for the requested analyses and privacy enhancing techniques are to be used as much as possible (van Veen 2008), the quest for absolute anonymity leads to the impossibility to perform meaningful research (Ohm 2010, van Veen 2011). The other way to meet the challenge would be to ensure the confidentiality of data with a theoretical risk of re-identification within the research domain. Through MTAs and data transfer agreements, researchers must guarantee that tissue and data will only be used for the approved research project and be destroyed or returned afterwards. Trust must also be shown and, though not yet implemented along the whole chain of tissue and data in research, audit procedures and certification, as are existing already in other realms where highly sensitive data and services are being used (like SAS70, in conjunction with applicable norms of the ISO 27002 series), are the way to go forward here (see van Veen 2011 for a fuller description). At this moment, already SAS70 and the implementation of ISO norms of data security should be considered as part of the preconditions for outsourcing sequencing to ‘upcoming markets’ in countries with, in general, a dubious reputation in adhering to basic international human rights standards or for a reliable legal system.
The challenge of possible discrimination
The other possible objection against research with residual tissue not based on full and even reiterative consent is the “risk of uninsurabality, unemployability or genetic discrimination” (Mascalzoni et al. 2008). These risks are then mentioned in an abstract way and no examples are given where research on tissue, as described here, has led to such social exclusion. They do not exist. Apart from the fact that such ‘risks’ cannot be averted by individual consent to genomic research, if such practices are generally applied to all, these ‘risks’ are virtually absent and, if not, remedied in Western societies, all of which have anti-discrimination laws. It must once more be reiterated that the opt-out system is embedded in conditions which in short amount to ‘patients for patients’. Scenarios where minorities are the focus of the research and or where tissue would have been taken for different reasons than their proper disease management (such as described in Mello and Wolf 2010) are by definition excluded from such a system.
International exchange
In the context of the international exchange of samples, the applicable ethical and regulatory standards of the country of origin are decisive for research with those samples in a different country, even if that other country holds different standards, whether more or less strict. The precondition is that the country of origin from where the sample is issued holds the ultimate say about how the sample is used and remains, in terms of Directive 95/46/EC (the data protection Directive), the ‘controller’ of the sample. The MTA should guarantee this. The next condition is that the country of origin has some system of consent, has approval by an ethics committee and that the sample is sent coded-anonymously. This is a simple rule of recognition, which allows research between countries with different regulatory regimes concerning the use of residual tissue for research. This ‘rule of—reciprocal—recognition’ was proposed for exchange in the context of European research projects. It is not necessarily limited to Europe, but the precondition is of course between countries with democratic regimes, the rule of law and trustworthy, accountable institutions participating in the project. The rule of recognition fits perfectly with the idea of inter-operability as proposed by Knoppers (2007). It has been proposed earlier (van Veen et al. 2006) and it is somewhat disappointing to see attempts at harmonisation resulting again in new guidelines. This cannot be due to the fact that the rule of recognition cannot work as it has been proven to work in various cooperative research projects.
Concluding remarks
Designing infrastructure, regulating and harmonising the health-care research biobanking field is a huge effort in which it is very easy to not only overlook a certain type of biobank, but also not to recognise or understand why it is necessary to have differences in approach in collecting human materials for a certain study design. Without such awareness, important and indispensable forms of biobanking are not always included in the design of infrastructure, regulation or attempts in favour of harmonisation in the field. This lack of awareness combined with the urge to describe or design the field at large, starting with the most publicised population biobanks, can actually result in the omission of important forms of biobanks. Hence, a ‘one size fits all approach’ can be detrimental to important resources for research. Residual biobanks start from a different perspective: of tissue repositories as the ‘well guarded treasures in the interests of patients’ (Oosterhuis et al. 2003).
We have presented arguments on how research with residual tissue can benefit from a tailor-made approach based on an opt-out system, if certain conditions are met. A pivotal role is that of the custodian or manager of the biobank as not only QA, but also in releasing the tissue in a coded way for approved projects. Together with Forsberg et al. (2010) we challenge ‘the default setting’ in the debate. We are aware that the opt-out system is not in conformity with most of the nonbinding recommendations issued in this field (e.g.UNESCO 2005; CoE 2006; CIOMS 2009). We have critically discussed this type of quasi law making elsewhere (van Veen et al. 2006) and find support for that criticism when in an international study the phenomenon was described as often amounting to a (rhetorical) ‘race to the top’ (Follesdal et al. 2008), meaning stressing the importance of the organisation concerned by enunciating an even more evocative document on human rights protection. On the possible risks of biobanking, we put forward that theoretical risks should be assessed realistically. It has been demonstrated that these risks exist to a much lesser extent than “hypothetically” mentioned and that they can be controlled and contained. For the international exchange of tissue, we propose a simple ‘rule of—reciprocal—recognition’ (again applicable only if certain conditions are met). We suggest that our approach can be valuable for other biobanking projects as well.
References
Allen J, McNamara B (2011) Reconsidering the value of consent in biobank research. Bioethics 2011(25):155–166
Al-Shahi R, Vousden C, Warlow C, Scottisch Intracranial Vasculkar Malformation Study Steering Committee (2005) Bias from requiring explicit consent from all participants in observational research: prospective, population based study. BMJ 331(7522):942
Bates S (2010) Progress towards personalized medicine. Drug Discov Today 15:115–120
Belgian Act (2008) Wet inzake het verkrijgen en het gebruik van menselijk lichaamsmateriaal met het oog op de geneeskundige toepassing op de mens of het wetenschappelijk onderzoek, as passed by the Parliament of Belgium and given Royal Assent in December 2008, art. 20.2
Bergkamp L (1988) Het proefdier mens, de normering en regulering van medische experimenten met mensen, Alphen aan den Rijn: Samson Uitgeverij
Bevilacqua G, Bosman F, Dassesse T, Höfler H, Janin A, Langer R, Larsimont D, Morente MM, Riegman P, Schirmacher P, Stanta G, Zatloukal K, Caboux E, Hainaut P (2010) The role of the pathologist in tissue banking: European Consensus Expert Group Report. Virchows Arch 456:449–454
Bovenberg JA (2006) Property rights in blood, genes and data, naturally yours?. Martinus Nijhoff Publishers, Leiden
Braun R, Rowe W, Schaefer C, Zhang J, Buetow K (2009) Needles in the haystack: identifying individuals present in pooled genomic data. PLoS Genet 5:e1000668. doi:10.1371/journal.pgen.1000668
Brody BA (1998) The ethics of biomedical research: an international perspective. OUP, New York
Campbell AV (2007) The ethical challenges of genetic databases: Safeguarding altruism and trust. King’s Law J 18:227–245
Campbell AV (2011) Commentary: autonomy revisited—a response to H. Haker. J Int Med 269:380–382
Charter (2007) Charter of Fundamental Rights of the European Union (2007/C 303/01) art. 35
Council for International Organizations of Medical Sciences (CIOMS) (2009) International Ethical Guidelines for Epidemiological Studies, Geneva
Council of Europe (CoE) (2006) Recommendation Rec 4 of the Committee of Ministers to member states on research on biological materials of human origin (adopted by the Committee of Ministers on 15th March 2006)
Curren L, Boddington P, Gowans H, Hawkins N, Kanellopoulou N, Kaye J, Melham K (2010) Identifiability genomics and UK data protection law. Eur J Health Law 17:329–344
den Exter AP (ed) (2008) International health law. Solidarity and justice in health care. Maklu, Apeldoorn
Diamandis M, White NM, Yousef GM (2010) Personalized medicine: marking a new epoch in cancer patient management. Mol Cancer Res 8:1175–1187
Dressler LG (2009) Disclosure of research results from cancer genomic studies: state of the science. Clin Cancer Res 15:4270–4276
Elger BS, Caplan AL (2006) Consent and anonymization in research involving biobanks. EMBO Reports 7(7):661–666
European Commission (2001) The future of health care and care for the elderly: guaranteeing accessibility, quality and financial viability, COM (2001) 723 final
Faunce A (2005) Pilgrims in medicine: conscience, legalism and human rights, Kluwer Law International, The Netherlands
FEDERA (2011) Gedragscode Goed Gebruik (Gedragscode verantwoord omgaan met lichaamsmateriaal ten behoeve van medisch-wetenschappelijk onderzoek)
Foekens JA, Wang Y, Martens JWM, Berns EMJJ, Klijn JGM (2008) The use of genomic tools for the molecular understanding of breast cancer and to guide personolized medicine. Drug Discov Today 13:481–487
Follesdal A, Wessel RA, Wouters J (ed) (2008) Multilevel regulation and the EU: the interplay between global, European and national normative processes, Martinus Nijhoff Publishers, Leiden
Forsberg JS, Eriksson S, Hansson MG (2010) Changing defaults in biobank research could save lives too. Eur J Epidemiol 25:65–68
Fortier I, Burton PR, Robson PJ, Ferretti V, Little J, L’Heureux F, Deschênes M, Knoppers BM, Doiron D, Keers JC, Linksted P, Harris JR, Lachance G, Boileau C, Pedersen NL, Hamilton CM, Hveem K, Borugian MJ, Gallagher RP, McLaughlin J, Parker L, Potter JD, Gallacher J, Kaaks R, Liu B, Sprosen T, Vilain A, Atkinson SA, Rengifo A, Morton R, Metspalu A, Wichmann HE, Tremblay M, Chisholm RL, Garcia-Montero A, Hillege H, Litton JE, Palmer LJ, Perola M, Wolffenbuttel BH, Peltonen L, Hudson TJ (2010) Quality, quantity and harmony: the DataSHaPER approach to integrating data across bioclinical studies. Int J Epidemiol 39:1383–1393
Goodson ML, Vernon BG (2004) A study of public opinion on the use of tissue samples from living subjects for clinical research. J Clin Pathol 57:136–138
Hoedemaker R, Gordijn B, Pijnenburg M (2007) Solidarity and justice as guiding principles in genomics research. Bioethics 21(6):342–350
Homer N, Szelinger S, Redman M, Duggan D, Tembe W, Muehling J, Pearson JV, Stephan DA, Nelson SF, Craig DW (2008) Resolving individuals contributing trace amounts of DNA to highly complex mixtures using high-density SNP genotyping microarrays. PLoS Genet 4:e1000167. doi:10.1371/journal.pgen.1000167
International Conference on Harmonization (2007) Definitions for genomic biomarkers, pharmacogenomics, pharmacogenetics, genomic data and sample coding categories, E15, step 4 version
Ioannidis JPA (2009) Population-Wide Generalizability of Genome-Wide Discovered Associations. JNCI 101(19):1297–1299
ISO (International Organization for Standardization, Health informatics) (2008) Pseudonymization ISO/TS 25237:2008. ISO, Geneva
Jacobsen SJ, Xia Z, Campion ME et al (1999) Potential effect of authorization bias on medical record research. Mayo Clin Proc 74(4):330–338
Janssens AC, van Duijn CM (2008a) Genome-based prediction of common diseases: advances and prospects. Hum Mol Genet 17:R166–R173
Janssens ACJW, van Duijn CM (2008b) Genome-based prediction of common diseases: advances and prospects. Hum Mol Genet 17:R166–R173
Jusilahti P, Salomaa V, Kuulasmaa K et al (2005) Total and cause specific mortality among participants and non-participants of population based surveys: a comprehensive follow-up of 54372 Finnish men and women. J Epedimiol Commun Health 59:310–315
Kaphingst KA, Janoff JM, Harris LN, Emmons KM (2006) Views of female breast cancer patients who donated biologic samples regarding storage and use of samples for genetic research. Clin Genet 69:393–398
Kettis-Lindblad A et al (2005) Genetic research and donation of tissue samples to biobanks. What do potential sample donors in the Swedish general public think? Eur J Public Health 16(4):433–440 (Advanced access published online October 2005)
Knoppers BM, Chadwick R (2005) Human genetic research: emerging trends in ethics. Nat Rev Genet 6(1):75–79
Knoppers BM, Saginur M (2005) The Babel of genetic data terminology. Nat Biotechnol 23:8
Knoppers BM, Abdul MH, Bédard K (2007) Genomic Databases and International Collaboration, 18 KLJ, pp 291–311
Lévesque E, Fraser W, Knoppers BM (2009) Consent to research: exceptional situations. GenEdit 7(3):1–12
Lowrance WW, Collins FS (2007) Ethics identifiability in genomic research. Science 317:600–602
Mancini J et al (2010) Consent for biobanking: assessing the understanding and views of cancer patients. JNCI 103:1–4
Mascalzoni D, Hicks A, Pramstaller P, Wjst M (2008) Informed consent in the genomics era. PLoS Med 5:e192. doi:10.1371/journal.pmed.0050192
Melas P, Sjöholm LK, Forsner T et al (2010) Examining the public refusal to consent to DNA biobanking: empirical data from a Swedish population-based study. J Med Ethics 36:93–98
Mello MM, Wolf LE (2010) The Havasupai Indian tribe case–lessons for research involving stored biologic samples. N Engl J Med 363:204–207
Mezuk B, Eaton WW, Zandi P (2008) Participant characteristics that influence consent for genetic research in a population-based survey: the baltimore epidemiologic catchment area follow-up. Community Genet 11:171–178
Mills FJ, Brooks A (2010) Information systems for Biobanks/Biorepositories: handling information associated with Compliant Sample Management. Biopreservation Biobanking 8:163–165. doi:10.1089/bio.2010.8310
Moore HM, Compton C, Alper J, Vaught JB (2011) International approaches to advancing biospecimen science. Cancer Epidemiol Biomarkers Prev. doi:10.1158/1055-9965.EPI-11-0021
Nietfeld JJ (2007) What is anonymous (letter). EMBO Reports 8(6):518
Nietfeld JJ, Sugarman J, Litton JE (2011) The Bio-PIN: a concept to improve biobanking. Nat Rev Cancer 11:303–308
O’Neill O (2002) Autonomy and trust in bioethics. CUP, Cambridge
OECD (2009) Guidelines for human biobanks and genetic research databases http://www.oecd.org/sti/biotechnology/hbgrd Accessed April 2011
Ohm P (2010) broken promises of privacy: responding to the surprising failure of anonymization (August 13, 2009). UCLA Law Rev vol 57, p 1701 U of Colorado Law Legal Studies Research Paper No. 9–12. Available at SSRN: http://ssrn.com/abstract=1450006
Oosterhuis JW, Coebergh J, van Veen EB (2003) Tumor banks, well guarded treasures in the interests of patients. Nat Rev Cancer 3:73–77
Ploem MC (2010) Gegeven voor de wetenschap; Regulering van onderzoek met gegevens, lichaamsmateriaal en biobanken, in Wetenschappelijk onderzoek in de zorg: Preadvies 2010, Vereniging voor Gezondheidsrecht, Den Haag, SDU: 117–210
Plomer A (2005) The law and ethics of medical research: international bioethics and human rights. Cavendish Publishing, London
Rathenau Instituut (2009) Nader gebruik nader onderzocht: zeggenschap over lichaamsmateriaal (Technology Assessment), Rathenau Instituut Den Haag
Riegman PHJ, de Jong BWD, Llombart-Bosch A (2010) The Organization of European Cancer Institute Pathobiology Working Group and its support of European biobanking infrastructures for translational cancer research. Cancer Epidemiol Biomarkers Prev 19:923–926
SAS 70 (Statement on Auditing Standards (SAS) No. 70 (see http://www.sas70.com)
Swierstra T (2004) Een essay over nader gebruik van lichaamsmateriaal ten behoeve van genomics onderzoek, Nederlandse Vereniging voor Bio-Ethiek Groningen
The Academy of Medical Sciences (2011) A new pathway for the regulation and governance of health research a report from the Academy of Medical Sciences. The Academy of Medical Sciences, London
The International Cancer Genome Consortium (2010) International network of cancer genome projects. Nature 15 464:993–998
Trouet C (2003) Van lichaam naar lichaamsmateriaal, Intersentia Antwerpen
Unesco (2005) The Universal Declaration on Bioethics and Human Rights, adopted by UNESCO in October 2005
van der Valk T (2010) Zeggenschap over lichaamsmateriaal: suggesties vanuit Europa. TvGR 7:562
van Leeuwen E (2008) Ethiek van medisch-wetenschappelijk onderzoek: informed consent en de therapeutische misconceptie. NTvG 12:679–683
van Veen EB (2008) Obstacles to European research projects with data and tissue: solutions and further challenges. Eur J Cancer 44:1438–1450
van Veen EB, Riegman PH, Dinjens WN, Lam KH, Oomen MH, Spatz A, Mager R, Ratcliffe C, Knox K, Kerr D, van Damme B, van de Vijver M, van Boven H, Morente MM, Alonso S, Kerjaschki D, Pammer J, Lopez-Guerrero JA, Llombart Bosch A, Carbone A, Gloghini A, Teodorovic I, Isabelle M, Passioukov A, Lejeune S, Therasse P, Oosterhuis JW (2006) TuBaFrost 3: regulatory and ethical issues on the exchange of residual tissue for research across Europe. Eur J Cancer 42:2914–2923
Vaught J, Kelly A, Hewitt R (2010) A review of International Biobanks and Networks: success factors and key benchmarks. Biopreservation Biobanking 7:143–150. doi:10.1089/bio.2010.0003
Vermeulen E, Schmidt MK, Aaronson NK, Kuenen M, van der Valk P, Sietses C, van den Tol P, van Leeuwen FE (2009) Opt-out plus, the patients’ choice: preferences of cancer patients concerning information and consent regimen for future research with biological samples archived in the context of treatment. J Clin Pathol 62:275–278
Wendler D (2006) One time general consent for research on biological samples. BMJ 332:544–547
Wolf SH, Rothemich SF, Johnson RE, Marsland DW (2000) Selection bias from requiring patients to give consent to examine data for health services research. Arch Fam Med 9(10):1111–1118
Wolfson M et al (2010) DataSHIELD: resolving a conflict in contemporary bioscience-performing a pooled analysis of individual-level data without sharing the data. Int J Epidemiol 39:1372–1382. doi:10.1093/ije/dyq111
Working Party (2007) Opinion 4/2007 on the concept of personal data, Article 29 Data Protection Working Party, Brussels 2007: 0124807/EN, WP 136
World Medical Association. Declaration of Helsinki (2008) article A.6, WMA
Yassin R, Lockhart N, González del Riego M, Pitt K, Thomas JW, Weiss L, Compton C (2010) Custodianship as an ethical framework for biospecimen-based research. Cancer Epidemiol Biomarkers Prev 19:1012–1015
Author information
Authors and Affiliations
Corresponding author
Appendix
Appendix
Text Box 2: Typology of data
There is considerable confusion about the terminology of coded, anonymous or identifiable tissue (Knoppers and Saginur 2005; Elger and Caplan 2006; van Veen et al. 2006; Nietfeld 2007). This confusion also applies to epidemiological data in general, without the context of research with tissue. Several proposals have been put forward (van Veen et al. 2006; Nietfeld 2007, ICH 2007). As tissue is always data as well—data are connected to the tissue and can be derived from the tissue—but not the other way around, the correct terminology following from data protection legislation should be applied. That terminology dates from before research with tissue entered the scene. The terminology should be neutral regarding the admissible use of data or tissue. Such assessment should come later, in view of the applicable privacy, human research protection legislation and the specific ethical assessment when research with tissue is concerned.
Here, we start with the typology of Directive 95/46/EC, which only recognises two kinds of data, namely personal data (falling within its ambit) and anonymous data (not covered by the Directive). Personal data those which are identifiable by the entity having those data, in the terms of the Directive ‘the controller’ or a ‘processor’ working on behalf on the former. Data can be directly or indirectly identifiable. Directly identifiable are data with direct identifiers attached to them, such as name and address. Indirectly identifiable data are those which are identifiable through the attributes attached to a data record, such as profession, age and zipcode.
The Directive states that the criterion whether data are re-identifiable is: ‘the means likely reasonably to be used’ to (re)identify (Recital 26). Obviously, such a criterion leaves room for discussion. The Directive has instituted a so-called ‘Working Party’ composed of members of the European National Data Protection Authorities. In 2007, the Working Party gave an Opinion on the concept of personal data (Working Party 2007). It mentions the high threshold, which must be used before data can be considered not indirectly identifiable. ‘Likely reasonably to be used’ becomes de facto ‘which theoretically could be used’. The Opinion also discusses the data chain and coding at some point in the chain. Coding at one point in the chain does not by itself influence whether data at a later point in the chain are anonymous or not. For that question, it only matters whether the entity holding the data at that later point can re-identify the data subject or not. The Opinion mentions the example of Case Record Forms (CRFs) which are sent to the sponsor of a clinical trial. The Opinion considers them anonymous at the level of the sponsor. CRFs are always two-way coded. Hence it is wrong—as is often assumed—to consider two-way coded data or tissue always to be personal data or tissue at the level of the receiver of the data or tissue, at least in terms of Directive 95/46/EC. But neither are they always anonymous data or tissue. It will depend on the level of security of the pseudonym or code number and again the re-identifiability of the data attached to that pseudonym. Only if those data are sufficiently aggregated (instead of birth date, year or 5-year class, etc.) they can, in combination with the aggregation level of the other data, be considered to be not re-identifiable.
Hence the following typology of data can be made
Anonymous data | Fully anonymous data | |
|---|---|---|
Coded-anonymous (pseudonymised) data | ||
Personal data | Indirectly identifiable data | Coded but either coding insufficiently secure or aggregation level too low |
Not coded, but aggregation level too low | ||
Directly identifiable data | ||
In the text, we come back to the threshold for not considering data not indirectly identifiable. When we use the term ‘absolute anonymity’ we refer to a situation that data are anonymous by all standards instead of not by ‘means likely reasonably to be used’ as mentioned in the data protection Directive or where, in terms of the Sect. 164.514 under b.1 of the US Department of Health and Human Services ‘Privacy Rule’ under HIPAA, the risk for re-identification would not be ‘very small’, but zero.
It might be argued that this terminology is insufficiently nuanced for research with tissue. In that context it matters whether data accompanying the tissue at the research domain (the end of the data chain) are two-way coded or not. Only in the first case is individual feedback possible. If one considers this a relevant factor, one should make a further distinction in the second box on the right-hand side between two-way or reversible coded (at the source) and one-way or irreversible coded (at the source).
Rights and permissions
About this article
Cite this article
Riegman, P.H.J., van Veen, EB. Biobanking residual tissues. Hum Genet 130, 357–368 (2011). https://doi.org/10.1007/s00439-011-1074-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00439-011-1074-x