
Abstract
Increased life expectancy has led to an overall aging of the population and greater numbers of elderly people. Therefore, the number of people with osteoporosis has increased substantially, accompanied with an epidemic of hip fractures. Osteoporosis is an age-related systemic condition that naturally occurs, among mammals, only in humans. Osteoporosis is known to be highly heritable. However, assuming a genetic determinant for this post-reproductive disease to be transmitted from one generation to the next is counter-intuitive, based on the principles of human evolution, I will attempt to provide an explanation of the phenomenon from the point of view of evolution, selection, and changed environment in humans, which contributed to human longevity, while on other hand, contribute to diseases of civilization, including osteoporosis. There is a need to delve into evolution of human species in search for adaptive patterns to a specific environment that humans are operating in the last couple of millennia, to clarify whether “good” and “bad” genes exist, and how to find and correct them. The answer to the above questions will help us to identify causes of the current epidemic of osteoporosis and to pin-point a tailored treatment.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Increased life expectancy has led to an overall aging of the population and greater numbers of elderly people. Therefore, the number of people with age-related osteoporosis has increased substantially as well. Osteoporosis is defined as a disease characterized by low bone mass and structural deterioration of bone tissue, leading to bone fragility and an increased susceptibility to fractures (http://www.nof.org/osteoporosis/diseasefacts.htm 2008). Osteoporosis is estimated to affect about 75 million people in Europe, the US, and Japan. According to the International Osteoporosis Foundation, the total direct cost of osteoporotic fractures is €31.7 billion in Europe and €17.5 billion in the US (2002 figure). There are over 1.5 million osteoporotic fractures annually in the US. Fracture risk increases with age, and as the world’s population ages, an epidemic of hip fractures has been prophesized for the years to come; an estimated 30 million US women face an increased risk of fracture (Melton 1995).
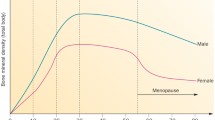
Osteoporosis is an age-related systemic condition that naturally occurs, among mammals, mainly in humans (Latimer 2005). It affects mostly women in their late-life years and results from a failure to acquire optimal peak bone mass during growth, and/or to maintain bone mass in later years (Bonjour et al. 1994). Osteoporosis originates in two ways: a rapid bone loss after menopause as a result of estrogen withdrawal (“menopausal” osteoporosis), and a gradual age-related bone loss in older persons, in both men and women (“senile”, or aging-related osteoporosis) (Burger et al. 1998; Hannan et al. 2000).
Osteoporosis is known to be highly heritable. However, assuming a gene(s) for this disease is transmitted from one generation to the next is counter-intuitive, based on the principles of human evolution. Here, I will attempt to provide an explanation of the phenomenon from the physical anthropological (as well as Darwinian medicine’s) perspective, focusing on processes of evolution, selection, and changed environment in humans, which contributed, on one hand, to human longevity, while on another, to diseases of civilization, including osteoporosis. I will regress into evolution of human species in search for “mistakes” in adaptive patterns, as well as for a specific environment we humans are operating in the last couple of millennia, for clues. Finally, there is a need to immerse into the notion of a deterministic view of DNA code, which prescribes how the whole organism should behave, to clarify whether “good” and “bad” genes exist, and how to find and correct them. Answer to the above questions will help to identify causes of the current epidemic of osteoporosis (http://www.surgeongeneral.gov/library/bonehealth/).
What the bones are for?
There are more than 200 bones in the skeleton; however, there are three times as many (~650) skeletal muscles. Approximately 80% of the adult skeleton is composed of cortical (compact) bone and 20% is cancellous (or trabecular), but the relative proportions of the two types of bone vary considerably at different skeletal sites. As mentioned, muscles are more numerous than bones; therefore, the most obvious function of the bones is mechanical: to serve as a lever for the muscles, such as in locomotion and mastication. Similar to a turtle’s shell, there is a protective function, as well as a “body shaping” (e.g., pelvis, cranium, rib cage) role. There are two additional important functions of the bone that are less obvious: bone marrow holder (for hematopoiesis, the new blood production) and, particularly relevant to this review, a minerals’ storage. Bones store ~97% of the body’s calcium and phosphorus, serve as a biochemical accessory: the increase of blood acidosis caused by the sulfur requires a buffer, which is provided by dissolving bones for calcium as this buffer.
Unlike nerves or muscles, bones possess a remarkable ability to regenerate continuously, an ability called remodeling. Remodeling replaces “old” fatigued bone with new, mechanically sound bone (thus maintaining mechanical strength and re-structuring to withstand changing strains) and preserves the body’s mineral homeostasis by providing access to the skeletal stores of calcium and phosphorus. This role becomes acutely relevant during pregnancy and nursing (lactation), when mother’s skeletal deposits are used to build the baby’s new bones. When remodeling is unbalanced (too much old bone is removed, too little is replaced by a new tissue), net bone loss occurs.
Evolution of osteoporosis
Although bone loss has been observed even in earlier populations (Karasik et al. 1998; Mays 2001), clinically recognized osteoporosis and especially the postmenopausal osteoporosis, was not evident in the past. Specifically, osteoporotic fracture typically seen in modern osteoporosis was absent in past populations (Mays 2000). Nowadays, this may be partly attributed to the increased life expectancy, which tends to increase the incidence of clinically recognizable fractures. Despite low bone mass and unfavorable bone geometry are expected to be a universal phenomenon (Nowlan and Prendergast 2005), our ancestors most probably did not live long enough for the osteoporosis to begin to manifest as fractures in genetically predisposed individuals.
Evolution science may provide us clues as all major evolutionary adaptations are compromises between selective advantages and disadvantages (Latimer 2005). For example, bipedality (two-leg walking) in general created many problems, including the human’s need for midwives. The shift to upright human-like walking is quite ancient with fossil evidence suggesting that it occurred somewhere between 6 and 8 million years ago (Latimer 2005). Freeing the upper extremity contributed to our fine motor skills and, as a consequence, brain development. It also caused common human-only maladies such as fractured hips, hernias, torn menisci, herniated intervertebral disks, fractured vertebrae, scoliosis, and kyphosis, just to name a few. [Indeed, human walking places stress upon our lower limbs that are normally shared by both hind and forelimbs in quadrupedal animals (Latimer 2005), thus overloading them.]
Some evidence exists that bipedality could have developed for energy efficiency. Sockol and colleagues (Sockol et al. 2007) demonstrated the energy benefit of bipedal locomotion in chimpanzee. The study linked the energy cost to biomechanical design, namely a straighter knee-hip configuration and the longer leg in humans, the same factors that largely contribute to the risk of falls and hip fracture (Rauch and Rittweger 2007). Even in Homo neanderthalensis, a more robust skeleton, a peculiar thorax, smooth lumbar lordosis, and pelvic girdle construction strongly suggest significant gait differences from the H. sapiens, therefore confirming the view that human ability to walk for long distances and quickly run comes at a cost of gracile bones.
Clearly, our ancestors did not live long enough for this to have become an issue. However, current demographic trends will have the effect of altering what was once a positive adaptation for distinctive human bipedality into a serious set of “collateral” pathology among the modern elderly (Latimer 2005). Alexander (2001) suggests that the modern humans’ pattern of bone loss is a result of chronic under-use of movement range, a by-product of a bipedal lifestyle. For example, exercise that uses all of the available movement range, would better prepare the skeleton to adjust to other factors hostile to bone maintenance. Indeed, studies conducted by Reeve and colleagues demonstrated life-long thinning of the superolateral femoral neck cortex, which they explained by insufficient loading during walking (Mayhew et al. 2005).
The environment triggers evolution; there is ongoing interaction between a species’ genome and its environment over the course of many generations (Cordain et al. 2005). A change in environment can lead to maladaptations, which are reflected in chronic diseases (Booth and Lees 2007; Cordain et al. 2005). So what aspect of the environment causes our failing bones? Is it the Western diet and/or the hypodynamia (sedentary lifestyle) of western people?
In their review, Booth and Lees (2007) argue that physical inactivity is an “actual cause” of common diseases. Today, we are not as physically active as our “stone age” ancestors, or even our ancestors from a hundred years ago (Booth and Lees 2007). Similarly, with the advent of agriculture, novel foods were introduced for which the archaic Homo genome had little experience and “tools” to deal with (Cordain et al. 2005).
Today, indigenous cultures continue some of the protective traditions (Batchelder 2005), including a traditional diet and strenuous physical activity. However, during the last two million years, societal changes have brought technological sophistication and advances, while biological mechanisms, improving bone strength, have decreased (Beck et al. 2000). One example of “modernization” that impacted bone strength is the decline of breast-feeding, which began in Western countries has spread to the less developed countries (Batchelder 2005). Breast milk provided an important source of nutrients in the traditional diet of young humans, which has been replaced by inferior processed foods in modern societies (Batchelder 2005).
Adaptations to new food and osteoporosis risk
Darwinian theory states that organisms that possess the most advantageous genes will survive longer and produce more offspring than the rest of the population; in other words, have “greater reproductive fitness”. Therefore, evolutionary forces are expected to produce different effects before, during, and after the fertile period, which is sometimes evident as antagonistic pleiotropy (Kirkwood and Rose 1991). There are multiple examples of the transmission of genes advantageous early in life, including the gene for lactose tolerance. Milk is rich with many important nutrients, including vitamin D and disaccharide lactose; lactase is an enzyme that splits the disaccharide to the glucose and galactose. Milk is the primary food source not only for human infants but for all newborn mammals. As the young grow, they are weaned away from breast-feeding. The onset of lactose intolerance may aid in this process; it occurs in most mammals, even some adult cats cannot effectively digest cow’s milk. At some point in history, humans discovered that they could continue to drink milk past infancy and into adulthood, and not only human milk but milk from other species. The invention of dairy herding 10–12 thousands years ago (Cordain et al. 2005; Karasik et al. 2000) was thus one of the decisive steps for making adaptive superiority. Natural selection was therefore involved as the ability to digest dairy products, which is advantageous and contributes to our general fitness, especially for the improved calcium intake.
We need vitamin D to facilitate calcium absorption, as calcium is not absorbed efficiently if it is not accompanied by vitamin D. An effective way to produce vitamin D is to sun-bathe; however, when humans left Africa, sunshine became unreliable. The improved vitamin D nutrition facilitated by a depigmented skin (easier to sun-bathe) or diets of ocean fish (the only meaningful nutritional source of vitamin D) would have been essential for human survival at northern latitudes (Vieth 2003). It has been argued that a high calcium in diet was also needed (Vieth 2003). To achieve this, human populations in northern Europe adapted to permit consumption of milk into adulthood by selecting for high intestinal lactase activity beyond childhood (Fuller 2000). Therefore, Africans more frequently have lactose intolerance, probably because they do not need as much vitamin D and calcium to maintain their (relatively strong) skeletons. On the contrary, skin depigmentation and high consumption of dairy products do not seem to protect Northern Europeans from fractures.
As follows, the invention of dairy herding helped to select for the ability to digest milk sugars. However, as the negative by-product of consuming domesticated animals (rich on “marbled” meats), the Western diet generally contains excessive saturated and trans fatty acids and has too little omega-3 polyunsaturated fatty acids (PUFAs) than omega-6 PUFAs (Cordain et al. 2005). Thus, healthy adults consuming the standard Western diet sustain a chronic, low-grade pathogenic metabolic acidosis that worsens with age as kidney function declines. Similarly, displacement of vegetables and fruit (consumed by hunters-gatherers) by whole grains and milk products, which are poor for potassium concentrations, aggravates the disbalance (Cordain et al. 2005). In uncorrected acidosis, the deposition of alkaline mineral in bone by osteoblasts is reduced, and osteoclast resorptive activity is increased in order to maximize the availability of hydroxyl ions in solution to buffer protons (Brandao-Burch et al. 2005).
Physical activity and bones (Back to hunting and gathering?)
Researchers and the general public have long known that an active lifestyle, including regular and intense exercise, correspond to stronger bones. Unfortunately, for those over 40, this should already have happened. Adult bone is less sensitive to exercise-induced changes in peak muscle strain than younger, growing bone (Turner et al. 1995).
Robust and well-designed study of Michaelsson and colleagues (2007) should receive quite some attention. This 35 year follow-up study in men ages 49–51 at baseline showed that recreational participation in exercise is by far the most powerful protective factor among the list of the behaviors linked to bone health (e.g., vitamin D, calcium intake, smoking, alcohol use, and joint diseases). Regular physical exercise can reduce the risk of fracture by amounts that are comparable or even greater than pharmacological interventions. The authors think that one-third of all hip fractures could be prevented by regular exercise. What is the mechanism,—local or central; general fitness, better muscles, or neural responses—remains enigmatic (Rauch and Rittweger 2007). However, it is known that even extremely small strains on the bone, if induced at a sufficiently high frequency, are strong determinants of bone strength (Rubin et al. 2001). This suggests that the bone tissue depends as much on the persistent, low magnitude strains that arise through common activities such as standing as it does on the relatively large, but rare strain events of strenuous muscular activity (Adams et al. 1997). From this perspective, the bone loss of those confined to long-term bed rest (or space flight), may result not only from diminished numbers of high-strain magnitude cycles, but also diminished numbers of low-strain magnitude cycles due to low muscular activity. Thus, exercise is an inexpensive and effective way to prevent fractures, at least for the young.
The evolutionary view on menopause: the ‘stopping-early’ and ‘grandmother’ hypotheses
Despite sharing up to 99% of the DNA with higher primates, apes are not our direct ancestors. There is a list of features in humans that are different from great apes. We all know about brain size, the opposable thumb, and body hair. However, some of us may not be aware of the skeletal muscle strength, the descended larynx, (absence of) the penis bone, handedness, different chromosome number, ear lobes, third molar (wisdom tooth) impaction, and so on. This is just a part of a very long list [see review by (Varki and Altheide 2005)]. And of course, the list also includes helplessness of the newborn, prolonged helplessness of young, and the need of extended care of the young. Along with these, there is the human-only trait of menopause.
Menopause and post-menopausal longevity of human females presents a puzzle from an evolutionary perspective. Two theories attempt to explain these phenomena. The ‘stopping-early hypothesis’ states that because human infants are so under-developed at birth, it is beneficial for women to cease reproduction at the age at which the risk of maternal death reaches a certain threshold. In contrast, ‘the grandmother hypothesis’ states that survival long past the age of menopause has been selected for because grandmothers significantly improve their daughter’s children survival (Grainger and Beise 2004), by helping them with child-raising chores.
In their numerical study, the authors (Grainger and Beise 2004) tested both “the stopping-early hypothesis” and “the grandmother hypothesis”. They found some support for grandmaternal facilitation of infant survival. Therefore, there is an advantage for women to first, stop making new babies when they are already grandmothers, and second, to survive past their “normal” reproductive years to invest in their grandchildren. Some further hypothesize that “grandmothering is an adaptation facilitating increased longevity, and menopause is a byproduct” (Peccei 2001).
The above presents a paradox of osteoporosis: why does the risk of osteoporosis not track with longevity? Why don’t men with their stronger bones live longer? Longevity in men involved in parallel with that in women: there was a huge benefit for at least one wise hunter or tool-maker to stay around longer to share the newly acquired skills with the younger tribesmen. This might happen even if genes for men’s longevity were selected for as a by-product of women’s longevity: i.e., if a gene on chromosome X was responsible for the survival of grandmothers; by virtue of inheriting one copy of X men also enjoyed its benefits. However, if there exists an X-linked, frequent and dominant allele associated with osteoporosis, then having a second X chromosome would afford the extra probability of liability to an XX female compared to an XY male (Karasik and Ferrari 2008). Indeed, men do die at a relatively younger age than women. Therefore, the selective advantage of being female persists at the cost of increasing the incidence of age-related disorders, such as to become osteoporotic. Men die from complications of fracture, at the rates comparable with female (Berry and Kiel 2007); but women fracture more frequently. It seems accurate to assume that if osteoporosis has a genetic determinant, its genetics will share peculiarity with the aging per se, being an example of “post-reproductive” genetics (Capri et al. 2008), which is difficult to explain by a selection process.
Is natural selection unlikely cause of osteoporosis?
Since osteoporosis occurs after the reproductive years, natural selection could not have a role to prevent it. Natural selection works on genes on the basis of benefits they provide in early life (Harris and Malyango 2005). Although researchers often considered bone an optimal structure for withstanding loading, it has not attained an optimum for a variety of stresses (running, walking, jumping, habitual for H. sapiens), because of the slow speed of adaptation (Bagge 2000). Recent empirical and theoretical work suggests that there is no single optimal bone architecture; instead many different architectures produce adequate bone strength (Nowlan and Prendergast 2005; Turner 2002). Therefore, natural selection probably has not played a dominant role in optimizing bone structure since the beginning of H. sapiens. This again confirms the notion that mutation-selection balance is responsible for maintaining genetic variance in human population. In a human society, both physically strong and weak children survived into adulthood to give progeny. There was not a clear benefit of having strong bones in childhood [which is known to be a prerequisite to avoid fractures later in life (Ferrari 2005)]. Therefore, children with a “pro-osteoporotic” bone architecture and lower bone mineralization were not selected against—which means, they were able to transfer their genes further on.
In search of a possible culprit: “Stone Age” genes?
There are a couple hundreds of genes that were suggested as possible regulators of bone mass, calcium, and collagen metabolism, which variations are implicated in osteoporosis [recently reviewed in (Ferrari and Rizzoli 2005; Karasik and Ferrari 2008; Ralston and de Crombrugghe 2006)]. Genes from multiple pathways, including inflammatory, growth hormone, and steroid metabolism, were studied by multiple groups, and several dozens were replicated by well-powered studies (Langdahl et al. 2008; Ralston et al. 2006; van Meurs et al. 2008). Majority of the candidate genes might be described as “stone age”, or archaic, genes (Booth and Lees 2007), which were properly functioning in our ancestors under the challenging environment before the dawn of civilization, but became affected by the recent post-industrial change of environment.
Two prominent examples can be mentioned here. Nuclear receptors, especially sex hormones—androgens and estrogens—are obvious candidates for regulation of musculoskeletal system since the sexual dimorphism in bone mass and muscle strength is pronounced. The skeletal actions of androgens may result from direct activation of the androgen receptor (AR), or may alternatively depend on stimulation of the estrogen receptors (ESRs) following aromatization of androgens into estrogens; the enzyme aromatase (coded by CYP19) catalyzes this conversion (Gennari et al. 2004). Especially relevant is the role of sex hormones in adaptation of bone structure to the mechanical impulses on the skeleton; therefore, they act in response to exercise (Ferretti et al. 1998; Frost 1999; Sievänen 2005).
Regulation of calcium in bone homeostasis through the vitamin D endocrine system is well known (Ferrari and Rizzoli 2005). Even more interesting is reduction in the number of falls and fractures with vitamin D supplementation and an improvement in muscle strength (Bischoff-Ferrari et al. 2004; Bischoff et al. 2001), which indicates an alternative mechanism on fracture prevention via vitamin D receptor (VDR) pathway. VDR polymorphisms were indeed associated with bone geometry (Fang et al. 2007), fractures (Uitterlinden et al. 2006), and muscle mass/strength (Grundberg et al. 2004; Windelinckx et al. 2007). The taxonomic tree constructed by Gurel and Livshits (2003) of the entire set of vertebrate sequences of nuclear receptor genes conformed to known vertebrate evolution; in general, the authors noted a slow rate of evolution of these genes. They attribute this fact, along with Baker (2001), to the relatively short divergence time of mammals, with not many neutral or expressed changes being accumulated in the human protein in relation to other mammals. Therefore, our “stone age” genes are not much different from the amphibian or reptilian genes.
Obviously, any list of genes associated with osteoporosis is not comprehensive; it needs to be added by genome-wide association studies, refined by bioinformatic search of expression databases, and confirmed via functional studies. Similarly important is to understand how environment exerts its effect via these genes.
The promise of genomic research to treat osteoporosis
By definition, natural selection should favor “good” genes; since it seems not to be a case for osteoporosis, let us try to evaluate what is wrong with the perception of gene determinism. Common diseases, such as diabetes, osteoporosis, or cancer, are the result of the complex interplay between genetic and environmental factors. Moreover, there are many indications that virtually all human diseases result from the interaction of genetic susceptibility factors and environmental factors (Khoury et al. 2003). Even expression of some rare Mendelian diseases long thought to be the result of a deficiency in a single gene product, may depend on the modifying effects of environment (a simplest example is phenylketonuria, which occurs only when the mutation, phenylalanine hydoxylase deficiency, and the environmental exposure, dietary phenylalanine, are both present). Similarly, in many complex diseases, penetrance of risk genotypes is often incomplete unless specific environmental factors and/or other gene variants are also present.
Genome-wide association studies promise to find genes regulating osteoporosis (Kiel et al. 2007a), however, it is a gene–environment interaction that has to be studied. This task is achievable only within the large consortia of comparable studies. However, most genetics research is still focused on identifying single causative factors (a “reductionist” approach) and has not overcome a deterministic interpretation of complex disorders. Although there has been some progress lately in the field of gene–environment interactions (Ferrari et al. 2004; Kiel et al. 2007b), the results themselves have exposed the immense complexity that is involved. There is a need to develop a new approach to integrate this type of knowledge into existing methods, including enhancements from a statistical point of view (Karasik and Ferrari 2008).
Adaptations to the environment should lead to an altered gene expression (Fig. 1). According to Booth and Lees (2007), one strategy for adaptation to a new environment is to change DNA sequence; however, this is a process requiring many generations (Gurel and Livshits 2003), more than elapsed since the industry-driven environment change began. The time frame for the current environment of physical inactivity is too short to have selected polymorphisms, enabling to “tolerate” physical inactivity (Booth and Lees 2007). Similarly, it is not reasonable to expect that genetic drift (guided largely by chance) will be responsible for a directional change in gene pool (Nowlan and Prendergast 2005; Turner 2002). Rather, it is the altered expression of existing genes that produces maladaptations to unusual environment, such as metabolic syndrome (Booth and Lees 2007; Harris and Malyango 2005).

Simplification of a paradigm proposed by Booth and Lees (2007): gene-by-environment interaction leads most probably, to an altered gene expression, and rather unlikely, to a change in DNA sequence
The second strategy for adaptation to a new environment is through epigenetic modifications, which results in changes of chromatin structure and do not alter nucleotide sequence. Epigenetic effects, primarily methylation, should play a role in osteoporosis. This is a novel and promising area in the complex diseases, and to date almost unexplored in comparison to the ample knowledge of genome-wide polymorphic and structural variation (Conrad and Hurles 2007).
Pleiotropy and epistasis
Any complex system needs to be regulated by a concerted action of genes; also, it is very improbable that bone tissue homeostasis would be maintained by means of a single, simple mechanism. There is a need for genetic mechanisms to be redundant, pleiotropic, and polygenic, to avoid perturbation triggered by the environment (Ho et al. 2008; Sievänen 2005; Wolf et al. 2006). Since the same genes seem to affect multiple chronic diseases, such as coronary artery disease, hypertension, breast and prostate cancer, Type 2 diabetes, and osteoporosis (Booth and Lees 2007; Karasik and Kiel 2008), there is no need to explore vast numbers of genes; pleiotropic approach will pin-point those hubs that are important for several diseases. On the other hand, most chronic diseases are polygenic; perturbing a single gene may not produce a preclinical phenotype (Booth and Lees 2007). Therefore, a winning approach to decipher a genetic architecture seems to be an epistatic pleiotropy (Wolf et al. 2006).
There are several parallel and partly complementary physiological feedback systems involving intertwined hormonal functions for the muscle–bone interaction (Sievänen 2005; Wolf et al. 2006). A great example of the epistatic pleiotropy and its role in structuring the genetic composition of a complex phenotype are genes belonging to sex hormones and IGF1 pathways that are interacting in processes of muscle and bone development and maintenance and functioning in older age [reviewed in (Karasik and Kiel 2008)].
The dawn of H. futurensis
In conclusion, all modern people employ (at least some) technology as our primary means of adaptation to the environment (Beck et al. 2000). Humans brought physical inactivity, fatty foods, smoking and alcohol consumption, into their lifestyle, which has had the adverse effect of increasing incidence of chronic diseases (Booth and Lees 2007; Cordain et al. 2005). Leading explanations of the origins of diseases of civilization, such as type 2 diabetes, obesity, metabolic syndrome (Cordain et al. 2005; Harris and Malyango 2005), and probably osteoporosis are evolutionary. Technological change has clearly driven natural selection in the past. The invention of dairy herding, as we saw above, selected for the lactase gene that gives adults the ability to digest milk sugars; it also contributed to metabolic acidosis and fatty acids disbalance. It seems correct to agree that “the ultimate factor underlying diseases of civilization is the collision of our ancient genome with the new conditions of life in affluent nations, including the nutritional qualities” (Cordain et al. 2005) and lack of physical activity (Booth and Lees 2007).
Human evolution has brought immense advances, but everything comes at a cost. By freeing the upper extremities we got tools, but overloaded lower extremities; by living longer, we increased the chance to break our bones; by developing agriculture and technology, we created the environment for osteoporosis, but also created a possibility for treatment, such as stem cells, gene replacement and durable prostheses. Thus, what has made us H. sapiens, can provide ways to fight our diseases, including osteoporosis.
Understanding gene-by-modifiable environment interactions will afford more opportunities to effectively target intervention strategies, by providing the molecular evidence to improve prevention of chronic diseases through physical activity or dietary interventions, to identify those molecules that will allow early disease detection and deliver individual therapy (Booth and Lees 2007; Karasik and Ferrari 2008). However, will treatment of bone fractures via sophisticated bio-prostheses, gene delivery/tissue engineering, or grafting of stem-cell bone tissue be a step on the road for humans to become bio-robots? Is natural selection still a driving force in humans, given that our survival is often less dependent on genes than on technology? To what extent might a changing genome lead to changes in our future appearance (big skull/thin legs)? What might our species look like 1,000 years from now? There are still more questions than answers. This is an exciting time to live and work.
References
Adams DJ, Spirt AA, Brown TD, Fritton SP, Rubin CT, Brand RA (1997) Testing the daily stress stimulus theory of bone adaptation with natural and experimentally controlled strain histories. J Biomech 30:671–678
Alexander C (2001) Idiopathic osteoporosis: an evolutionary dys-adaptation? Ann Rheum Dis 60:554–558
Bagge M (2000) A model of bone adaptation as an optimization process. J Biomech 33:1349–1357
Baker ME (2001) Adrenal and sex steroid receptor evolution: environmental implications. J Mol Endocrinol 26:119–125
Batchelder T (2005) The stories bones tell. The Townsend Letter Group
Beck TJ, Looker AC, Ruff CB, Sievanen H, Wahner HW (2000) Structural trends in the aging femoral neck and proximal shaft: analysis of the Third National Health and Nutrition Examination Survey dual-energy X-ray absorptiometry data. J Bone Miner Res 15:2297–2304
Berry SD, Kiel DP (2007) Absolute risk for subsequent fracture was similar in women and men. ACP J Club 147:22
Bischoff HA, Borchers M, Gudat F, Duermueller U, Theiler R, Stahelin HB, Dick W (2001) In situ detection of 1, 25-dihydroxyvitamin D3 receptor in human skeletal muscle tissue. Histochem J 33:19–24
Bischoff-Ferrari HA, Borchers M, Gudat F, Durmuller U, Stahelin HB, Dick W (2004) Vitamin D receptor expression in human muscle tissue decreases with age. J Bone Miner Res 19:265–269
Bonjour JP, Theintz G, Law F, Slosman D, Rizzoli R (1994) Peak bone mass. Osteoporos Int 4:7–13
Booth FW, Lees SJ (2007) Fundamental questions about genes, inactivity, and chronic diseases. Physiol Genomics 28:146–157
Brandao-Burch A, Utting JC, Orriss IR, Arnett TR (2005) Acidosis inhibits bone formation by osteoblasts in vitro by preventing mineralization. Calcif Tissue Int 77:167–174
Burger H, de Laet CE, van Daele PL, Weel AE, Witteman JC, Hofman A, Pols HA (1998) Risk factors for increased bone loss in an elderly population: the Rotterdam Study. Am J Epidemiol 147:871–879
Capri M, Salvioli S, Monti D, Caruso C, Candore G, Vasto S, Olivieri F, Marchegiani F, Sansoni P, Baggio G, Mari D, Passarino G, De Benedictis G, Franceschi C (2008) Human longevity within an evolutionary perspective: the peculiar paradigm of a post-reproductive genetics. Exp Gerontol 43:53–60
Conrad DF, Hurles ME (2007) The population genetics of structural variation. Nat Genet 39:S30–S36
Cordain L, Eaton SB, Sebastian A, Mann N, Lindeberg S, Watkins BA, O’Keefe JH, Brand-Miller J (2005) Origins and evolution of the Western diet: health implications for the 21st century. Am J Clin Nutr 81:341–354
Fang Y, van Meurs JB, Rivadeneira F, van Schoor NM, van Leeuwen JP, Lips P, Pols HA, Uitterlinden AG (2007) Vitamin D receptor gene haplotype is associated with body height and bone size. J Clin Endocrinol Metab 92:1491–1501
Ferrari S (2005) Osteoporosis: a complex disorder of aging with multiple genetic and environmental determinants. In: Simopoulos A (ed) Nutrition and fitness: mental health, aging, and the implementation of a healthy diet and physical activity lifestyle, vol 95. Karger, Basel, pp 35–51
Ferrari SL, Rizzoli R (2005) Gene variants for osteoporosis and their pleiotropic effects in aging. Mol Aspects Med 26:145–167
Ferrari SL, Karasik D, Liu J, Karamohamed S, Herbert AG, Cupples LA, Kiel DP (2004) Interactions of interleukin-6 promoter polymorphisms with dietary and lifestyle factors and their association with bone mass in men and women from the Framingham Osteoporosis Study. J Bone Miner Res 19:552–559
Ferretti JL, Capozza RF, Cointry GR, Garcia SL, Plotkin H, Alvarez Filgueira ML, Zanchetta JR (1998) Gender-related differences in the relationship between densitometric values of whole-body bone mineral content and lean body mass in humans between 2 and 87 years of age. Bone 22:683–690
Frost HM (1999) On the estrogen-bone relationship and postmenopausal bone loss: a new model. J Bone Miner Res 14:1473–1477
Fuller K (2000) Lactose, rickets, and the coevolution of genes and culture. J Hum Ecol 28:471–477
Gennari L, Masi L, Merlotti D, Picariello L, Falchetti A, Tanini A, Mavilia C, Del Monte F, Gonnelli S, Lucani B, Gennari C, Brandi ML (2004) A polymorphic CYP19 TTTA repeat influences aromatase activity and estrogen levels in elderly men: effects on bone metabolism. J Clin Endocrinol Metab 89:2803–2810
Grainger S, Beise J (2004) Menopause and post-generative longevity: testing the ‘stopping-early’ and ‘grandmother’ hypotheses. MPIDR Working Papers Vol http://www.demogr.mpg.de/papers/working/wp-2004-003.pdf
Grundberg E, Brandstrom H, Ribom EL, Ljunggren O, Mallmin H, Kindmark A (2004) Genetic variation in the human vitamin D receptor is associated with muscle strength, fat mass and body weight in Swedish women. Eur J Endocrinol 150:323–328
Gurel I, Livshits G (2003) Phylogeny of vertebrate nuclear receptors—analysis of variance components in protein sequences. Coll Antropol 27:599–610
Hannan MT, Felson DT, Dawson-Hughes B, Tucker KL, Cupples LA, Wilson PW, Kiel DP (2000) Risk factors for longitudinal bone loss in elderly men and women: the Framingham Osteoporosis Study. J Bone Miner Res 15:710–720
Harris EE, Malyango AA (2005) Evolutionary explanations in medical and health profession courses: are you answering your students’ “why” questions? BMC Med Educ 5:16
Ho AM, Marker PC, Peng H, Quintero AJ, Kingsley DM, Huard J (2008) Dominant negative Bmp5 mutation reveals key role of BMPs in skeletal response to mechanical stimulation. BMC Dev Biol 8:35
http://www.nof.org/osteoporosis/diseasefacts.htm (2008) National Osteoporosis Foundation
Karasik D, Ferrari SL (2008) Contribution of gender-specific genetic factors to osteoporosis risk. Ann Hum Genet 72:696–714
Karasik D, Kiel DP (2008) Genetics of the musculoskeletal system: a pleiotropic approach. J Bone Miner Res 23:788–802
Karasik D, Arensburg B, Tillier A-M, Pavlovsky O (1998) Skeletal age assessment of fossil hominids. J Archaeol Sci 25:689–696
Karasik D, Arensburg B, Pavlovsky OM (2000) Age assessment of Natufian remains from the land of Israel. Am J Phys Anthropol 113:263–274
Khoury MJ, McCabe LL, McCabe ER (2003) Population screening in the age of genomic medicine. N Engl J Med 348:50–58
Kiel DP, Demissie S, Dupuis J, Lunetta KL, Murabito JM, Karasik D (2007a) Genome-wide association with bone mass and geometry in the Framingham Heart Study. BMC Med Genet 8(Suppl 1):S14
Kiel DP, Ferrari SL, Cupples LA, Karasik D, Manen D, Imamovic A, Herbert AG, Dupuis J (2007b) Genetic variation at the low-density lipoprotein receptor-related protein 5 (LRP5) locus modulates Wnt signaling and the relationship of physical activity with bone mineral density in men. Bone 40:587–596
Kirkwood TB, Rose MR (1991) Evolution of senescence: late survival sacrificed for reproduction. Philos Trans R Soc Lond B Biol Sci 332:15–24
Langdahl BL, Uitterlinden AG, Ralston SH (2008) Large-scale analysis of association between polymorphisms in the transforming growth factor beta 1 gene (TGFB1) and osteoporosis: the GENOMOS study. Bone. Available online 3 December 2007
Latimer B (2005) The perils of being bipedal. Ann Biomed Eng 33:3–6
Mayhew PM, Thomas CD, Clement JG, Loveridge N, Beck TJ, Bonfield W, Burgoyne CJ, Reeve J (2005) Relation between age, femoral neck cortical stability, and hip fracture risk. Lancet 366:129–135
Mays S (2000) Age-dependent cortical bone loss in women from 18th and early 19th century London. Am J Phys Anthropol 112:349–361
Mays S (2001) Effects of age and occupation on cortical bone in a group of 18th–19th century British men. Am J Phys Anthropol 116:34–44
Melton LJ (1995) How many women have osteoporosis now? J Bone Miner Res 10:175–177
Michaelsson K, Olofsson H, Jensevik K, Larsson S, Mallmin H, Berglund L, Vessby B, Melhus H (2007) Leisure physical activity and the risk of fracture in men. PLoS Med 4:e199
Nowlan NC, Prendergast PJ (2005) Evolution of mechanoregulation of bone growth will lead to non-optimal bone phenotypes. J Theor Biol 235:408–418
Peccei JS (2001) A critique of the grandmother hypotheses: old and new. Am J Hum Biol 13:434–452
Ralston SH, de Crombrugghe B (2006) Genetic regulation of bone mass and susceptibility to osteoporosis. Genes Dev 20:2492–2506
Ralston SH, Uitterlinden AG, Brandi ML, Balcells S, Langdahl BL, Lips P, Lorenc R, Obermayer-Pietsch B, Scollen S, Bustamante M, Husted LB, Carey AH, Diez-Perez A, Dunning AM, Falchetti A, Karczmarewicz E, Kruk M, van Leeuwen JP, van Meurs JB, Mangion J, McGuigan FE, Mellibovsky L, del Monte F, Pols HA, Reeve J, Reid DM, Renner W, Rivadeneira F, van Schoor NM, Sherlock RE, Ioannidis JP (2006) Large-scale evidence for the effect of the COLIA1 Sp1 polymorphism on osteoporosis outcomes: the GENOMOS study. PLoS Med 3:e90
Rauch F, Rittweger J (2007) Recent literature review: new studies on bone material, fractures, walking and running. J Musculoskelet Neuronal Interact 7:368–371
Rubin CT, Sommerfeldt DW, Judex S, Qin Y (2001) Inhibition of osteopenia by low magnitude, high-frequency mechanical stimuli. Drug Discov Today 6:848–858
Sievänen H (2005) Hormonal influences on the muscle-bone feedback system: a perspective. J Musculoskelet Neuronal Interact 5:255–261
Sockol MD, Raichlen DA, Pontzer H (2007) Chimpanzee locomotor energetics and the origin of human bipedalism. Proc Natl Acad Sci U S A 104:12265–12269
Turner CH (2002) Biomechanics of bone: determinants of skeletal fragility and bone quality. Osteoporosis Int 13:97–104
Turner CH, Takano Y, Owan I (1995) Aging changes mechanical loading thresholds for bone formation in rats. J Bone Miner Res 10:1544–1549
Uitterlinden AG, Ralston SH, Brandi ML, Carey AH, Grinberg D, Langdahl BL, Lips P, Lorenc R, Obermayer-Pietsch B, Reeve J, Reid DM, Amedei A, Bassiti A, Bustamante M, Husted LB, Diez-Perez A, Dobnig H, Dunning AM, Enjuanes A, Fahrleitner-Pammer A, Fang Y, Karczmarewicz E, Kruk M, van Leeuwen JP, Mavilia C, van Meurs JB, Mangion J, McGuigan FE, Pols HA, Renner W, Rivadeneira F, van Schoor NM, Scollen S, Sherlock RE, Ioannidis JP (2006) The association between common vitamin D receptor gene variations and osteoporosis: a participant-level meta-analysis. Ann Intern Med 145:255–264
van Meurs JB, Trikalinos T, Ralston SH, GENOMOS C (2008) Large-scale analysis of association between polymorphisms in the LRP-5 and -6 genes and osteoporosis: the GENOMOS study. JAMA
Varki A, Altheide TK (2005) Comparing the human and chimpanzee genomes: searching for needles in a haystack. Genome Res 15:1746–1758
Vieth R (2003) Vitamin D deficiency affecting genetic selection for lighter skin color. In: Agarwal SC, Stout SD (eds) Bone loss and osteoporosis: an anthropological perspective. Kluwer Academic Publications, New York
Windelinckx A, De Mars G, Beunen G, Aerssens J, Delecluse C, Lefevre J, Thomis MA (2007) Polymorphisms in the vitamin D receptor gene are associated with muscle strength in men and women. Osteoporos Int 18:1235–1242
Wolf JB, Pomp D, Eisen EJ, Cheverud JM, Leamy LJ (2006) The contribution of epistatic pleiotropy to the genetic architecture of covariation among polygenic traits in mice. Evol Dev 8:468–476
Acknowledgments
We are thankful to Genevieve Ferrick of Harvard Extension School and Catherine Gauthier of Hebrew SeniorLife for their critical reading, as well as to two anonymous reviewers for their useful comments. This review was supported, in part, by National Institute of Health/NIAMS grant (R01 AR050066).
Conflict of interest statement
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Karasik, D. Osteoporosis: an evolutionary perspective. Hum Genet 124, 349–356 (2008). https://doi.org/10.1007/s00439-008-0559-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00439-008-0559-8