
Abstract
The majority of patients with Saethre-Chotzen syndrome have mutations in the TWIST gene, which codes for a basic helix-loop-helix transcription factor. Of the genetic alterations identified in TWIST, nonsense mutations, frameshifts secondary to small deletions or insertions, and large deletions implicate haploinsufficiency as the pathogenic mechanism. We identified three novel intragenic mutations and six deletions in our patients by using a new strategy to screen for TWIST mutations. We used polymerase chain reaction (PCR) amplification with subsequent sequencing to identify point mutations and small insertions or deletions in the coding region, and real-time PCR-based gene dosage analysis to identify large deletions encompassing the gene, with confirmation by microsatellite and fluorescence in situ hybridization (FISH) analyses. The size of the deletions can also be analyzed by using the gene dosage assay with "PCR walking" across the critical region. In 55 patients with features of Saethre-Chotzen syndrome, 11% were detected to have deletions by real-time gene dosage analysis. Two patients had a translocation or inversion at least 260 kb 3' of the gene, suggesting they had position-effect mutations. Of the 37 patients with classic features of Saethre-Chotzen syndrome, the overall detection rate for TWIST mutations was 68%. The risk for developmental delay in patients with deletions involving the TWIST gene is approximately 90% or eight times more common than in patients with intragenic mutations.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
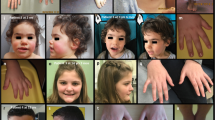
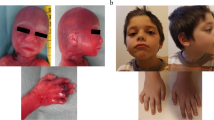
Saethre-Chotzen syndrome (acrocephalosyndactyly type III; MIM 101400; Saethre 1931; Chotzen 1932) is one of the most commonly inherited craniosynostosis conditions, the hallmarks of which are premature fusion of the calvarial bones and limb abnormalities. The notable craniofacial features of this syndrome are facial asymmetry, low frontal hairline, hypertelorism, and blepharoptosis, whereas the most common limb abnormalities are brachydactyly, large broad toes, and cutaneous syndactyly. Saethre-Chotzen syndrome is an autosomal dominant disease with high penetrance and variable expressivity, which leads to diagnostic difficulties among the craniosynostosis syndromes.
The TWIST gene has been demonstrated to have mutations in Saethre-Chotzen patients (El Ghouzzi et al. 1997; Howard et al. 1997). The TWIST gene, originally identified in Drosophila melanogaster, is highly conserved from Caenorhabditis elegans, D. melanogaster, Xenopus laevis, Mus musculus, to humans. It is localized at human chromosome 7p21 and has two exons and one intron of 538 bp. The first exon, which is 772 bp long, contains the entire coding region. The mRNA is at least 1396 bp long, and the transcription initiation site is unknown. The 202-amino-acid protein encoded by the TWIST gene is a basic helix-loop-helix (HLH) motif-containing transcription factor. The HLH region of this motif is important for homo- or heterodimerization, whereas the basic domain is essential for the binding of the dimer complex to a target DNA-binding sequence(s). TWIST is thought to be a negative transcriptional regulator that acts by direct binding to the PCAF and EP300 domain of histone acetyltransferases and by inhibiting their acetyltransferase activities (Hamamori et al. 1999). It is also involved in osteoblast and myoblast differentiation and maturation by negative transcriptional regulation (Funato et al. 2001; Jabs 2001). The pathway of molecular components involved in craniofacial and limb development includes not only TWIST, but also fibroblast growth factor receptors (FGFRs), which may be negatively regulated by TWIST (Rice et al. 2000).
Currently, at least 69 different intragenic mutations have been described for TWIST in unrelated Saethre-Chotzen patients (Gripp et al. 2000a, 2000b; Boeck et al. 2001; Dollfus et al. 2001; Elanko et al. 2001; Seto et al. 2001; Chun et al. 2002; Cai et al. 2003). Significant intra- and interfamilial phenotypic variability can be present, and no significant phenotype-genotype correlation has been observed. The nature of these mutations suggests that haploinsufficiency, the complete loss of function of one copy, can cause the condition, which implies that the normal function of the TWIST protein is critically sensitive to dosage. This hypothesis is further supported by studies on a Twist-knockout mouse model (Chen and Behringer 1995; Bourgeois et al. 1998). Whereas homozygous Twist-null mouse embryos exhibit failure of neural tube closure, heterozygosity for Twist-null mutations results in a viable phenotype including skull and limb anomalies consistent with those of the Saethre-Chotzen syndrome.
Therefore, in a TWIST mutation screen, it is very important that not only point mutations and small insertions/deletions are detected, but deletions spanning the gene must also be examined to detect dosage changes of the TWIST gene. Various strategies combining sequencing, microsatellite, Southern blot, and fluorescence in situ hybridization (FISH) analyses have been proposed (Johnson et al. 1998; Gripp et al. 2001; Chun et al. 2002). We report the development of a new screening method based on real-time PCR to detect TWIST gene deletions. We have also analyzed a cohort of patients for point mutations and small insertions/deletions and for large deletions.
Materials and methods
Patients and samples
All probands and family members were clinically examined by a medical geneticist/dysmorphologist, and tissues samples were collected after informed consents (protocol approved by the institutional review boards) were obtained. Genomic DNA was isolated from blood samples from these patients or from tissue cultures (lymphoblast, osteoblast, or fibroblast) established from these patients by means of the Blood and Cell Culture DNA Kit (Qiagen).
Mutation analysis by sequencing
The coding region of the TWIST gene was amplified and sequenced. PCR primers used for amplification were: forward 5'-GAGGCGCCCCGCTCTTCTCC-3' and reverse 5'-AATCGAGGTGGACTGGGAACCG-3', which yield an expected amplicon of 797 bp. PCRs were performed in 40-μl volumes that contained 200 ng genomic DNA, 1× High Fidelity PCR buffer, 0.2 mM each dATP, dCTP and dTTP, 0.15 mM 7-deaza-dGTP, 0.05 mM dGTP, 0.25 μM each primer, 2 mM MgSO4, and 1 U Platinum Taq High Fidelity (Invitrogen). PCR parameters were: 94°C for 6 min; 38 cycles of 94°C for 1 min, 66°C for 15 s, and 68°C for 45 s; followed by 68°C for 7 min. The PCR products were directly sequenced in both directions at the Johns Hopkins University Genetics Resource Core Facility. If insertions or deletions were suspected, the PCR products were then cloned into pCR-Blunt vector (Invitrogen), and clones containing different alleles were sequenced in both directions.
Real-time PCR analysis
Gene dosage analysis was performed by using the LightCycler (Roche). PCRs were carried out in a 20-μl volume with 5 μl DNA (various concentrations, ranging from 500 to 4000 copies), 0.5 μM forward primers, 0.5 μM reverse primers, and 1× QuantiTect SYBR Green PCR Master Mix (Qiagen). The primer sequences were: TWIST: forward 5' CGGGAGTCCGCAGTCTTA 3', reverse 5'CTTGAGGGTCTGAATCTTGCT 3'; ACTIN: forward 5'TGCGTGACATTAAGGAGAAG3', reverse 5'GCTCGTAGCTCTTCTCCA 3'; BETA-GLOBIN: forward 5'GGCTTCCTAGAGACCAATCA3', reverse 5'AACCAAGACAGCCAGTTCAC3'; HDAC9: forward 5' CAGCAACAAATCCAGAAGCA 3', reverse 5' CGGTGCAGACTCCTGAGTAA 3'; FERD3L: forward 5' GAAAGGAAGCGGATGTTCAA 3', reverse 5' GCCGCTTTCCTTCTTCTCAC 3'. PCR parameters were: a pre-incubation step of 95°C for 15 min; a quantitation step of 40 cycles of 95°C for 20 s, 57°C for 20 s, and 72°C for 8 s, at the end of which, the fluorescent reading of the F1 channel was taken; a melting curve step of 1 cycle of 95°C for 20 s and 65°C for 20 s, and slowly ramping to 95°C, with the fluorescent reading of the F1 channel being taken continuously; a cooling step of 1 cycle of 40°C for 30 s. The ramp rate was set at 20°C/s, except during the melting curve step from 65°C to 95°C when the ramp rate was set at 0.2°C/s. Human Genomic DNA (Roche) was diluted to 4000, 2000, 1000, 500, or 250 copies per 5 μl, and these were used for external standardization. All standards were amplified in triplicate, and a linear standard curve was constructed. Sample concentrations were inferred based on this standard curve by LightCycler 3 software (Roche) with second-derivative maximum algorithm and default settings. Sample concentrations were diluted to lie within the range of standards. All patient DNA samples were measured in four replicates, and the results were accepted only if they were within less than 10% of the standard deviation for the four replicates. Melting curve analysis was performed to confirm the presence of the specific PCR products, and the size of the amplicons was checked by gel electrophoresis.
Microsatellite analysis
Twenty-nine microsatellite markers spanning a region of approximately 19 Mb around the TWIST gene (from 13 Mb telomeric to 6 Mb centromeric to TWIST) were selected to detect loss of heterozygosity. These markers were highly informative with an average heterozygosity rate of 74%. Based on a sequence from the Genome Database (http://www.gdb.org), PCR primers were synthesized and fluorescently labeled with either 6-FAM, TET, or HEX at the 5' end (Johns Hopkins University Genetics Resource Core Facility) for the following markers: D7S481, D7S2514, D7S641, D7S2547, D7S2464, D7S513, D7S620, D7S664, D7S2557, D7S2508, D7S507, D7S488, D7S638, D7S2532, D7S2559, D7S503, D7S815, D7S654, D7S2551, D7S2535, D7S2562, D7S493, D7S1795, D7S2458, D7S2510, D7S629, D7S682, D7S673, D7S2444 (oriented from chromosome 7p22.1 to 7p15.3). The TWIST gene is between D7S2532 and D7S2559. Genotyping was performed and analyzed on a Model 373 DNA Sequencer and Genescan software (Applied Biosystem).
FISH analysis
Metaphase chromosome spreads were prepared by standard methods. Cosmid DNA (1 μg) was labeled with digoxigenin (Roche) by nick translation. For each hybridization, an aliquot (200 ng) of labeled probe was co-precipitated with 5 μg of human Cot-1 DNA onto slides and then resuspended in 10 μl hybridization solution consisting of 50% formamide in 2×SSC (1×SSC=150 mM NaCl, 15 mM sodium citrate, pH 7.0), 10% dextran sulfate. The probe solution was denatured for 5 min at 75°C and pre-annealed at 37°C for 20–40 min. Samples on slides were denatured for 3 min at 75°C before hybridization at 37°C for 18 h. The slides were washed twice at 42°C in 50% formamide/2×SSC for 7 min, twice at 42°C in 2×SSC for 5 min, and then once in 4×SSC/0.05% Tween-20 for 1 min at room temperature. The cosmid signals were detected by using rhodamine-conjugated anti-digoxigenin according to the manufacturer's instructions (Ventana). Metaphase chromosomes were counterstained with the A-T binding fluorochrome 4',6-diamidino-2-phenylindole (DAPI) and viewed by using a Zeiss AxioSkop equipped with the appropriate filters, a SenSys cooled charge-coupled device camera (Photometrics), and Quips SmartCapture VP imaging software (Applied Imaging).
Results
Detection of mutations by sequence analysis
Thirty-nine patients with Saethre-Chotzen syndrome-like features were studied. Four of these patients had abnormal karyotypes (46,XY,del(7)(p15.1p21.3); 46,XY,t(2;7)(p23;p22); 46,XX,inv(7)(p21.3q34); 46,XY,del(7)(p15.3p21.3)). Sixteen patients were karyotypically normal by standard G-banding. For the remaining 19, chromosomal analysis data were not available. By sequence analysis, all patients were negative for mutations of exon IIIa of FGFR1, exons IIIa and IIIc of FGFR2, and exon IIIa of FGFR3, in which mutations have been reported for syndromic craniosynostosis conditions (Paznekas et al. 1998).
Heterozygous mutations were identified in nine patients (Table 1), including three novel mutations (Fig. 1). Two of these new mutations were located 5' to the DNA-binding domain of the TWIST gene: an 11-bp heterozygous deletion (128_138del11) resulting in a frameshift at codon 44 and a termination codon at 233, and a single nucleotide deletion (309delC), resulting in a premature stop codon at codon 103. A novel 7-bp deletion in the helix II domain (482_488del7) was found, resulting in a frameshift at codon 161 and termination codon at position 228. These changes occurred at conserved amino acids and were not detected in at least 100 alleles from control individuals. We also detected six different mutations in TWIST that have been described elsewhere: 7C>T, 309C>G, 364C>T, 416_417dup21, 420_421dup21, 445C>T (El Ghouzzi et al. 1997; Howard et al. 1997; Rose et al. 1997; Johnson et al. 1998; Paznekas et al. 1998; Elanko et al. 2001).

New TWIST mutations identified by sequencing (top normal allele, bottom mutant allele). A Normal and mutant 128_138del11 alleles. B Normal and mutant 309delC alleles. C Normal and mutant 482_488del7 alleles
Detection of TWIST deletion by real-time PCR
To detect a two-fold difference in copy number, we applied a quantitative PCR assay. The measured copy number of ACTIN, a housekeeping gene, was compared with the actual copy number from human genomic DNA at various concentrations by using the LightCycler (Fig. 2). The assay was very accurate in detecting DNA from 250 to 4000 copies with no overlap between the neighboring data points for samples that differed two-fold in copy number. We also tested the accuracy with BETA-GLOBIN, another housekeeping gene that yielded similar results. Thus, we were able to accurately detect two-fold differences between two samples.

Accuracy of the real-time PCR method. The relationship between the mean value with the standard error of the number of computed gene copies and the actual number of gene copies is shown. Two-fold differences in copy number can be detected without ambiguity
To detect a heterozygous deletion of the TWIST gene in DNA samples from patients, the copy number of TWIST was compared with the copy number of a control gene in the same individual by using the LightCycler. TWIST gene copy, and control gene copy measurements were carried out individually on successive LightCycler runs. We chose not to co-amplify TWIST and a control gene in the same reaction with gene-specific probes to measure copy number, because the high GC content of the TWIST gene prohibited the design of satisfactory probes. Instead, we utilized SYBR green, which is capable of generating fluorescence after binding DNA, and measured the total DNA present. We first used ACTIN as a control gene. Since the amplification efficiencies for both TWIST and ACTIN were similar, the need to correct for different amplification efficiencies when comparing different genes was avoided. Similar results were obtained by using BETA-GLOBIN as a control gene.
We hypothesized that if there was a heterozygous deletion of the TWIST gene in the DNA of a patient, the ratio of gene copy number between TWIST and ACTIN would be close to 0.5, whereas if there was no deletion of the TWIST gene, the ratio would be close to 1.0. To test this hypothesis, we performed this gene copy number analysis on patients with known deletions of one allele as determined by karyotype analysis and controls with two normal alleles. Patient B2459M, who was shown to have a large deletion including TWIST (46,XX,del(7)(p15.1–21.1)) by karyotype and FISH (Hoover-Fong et al. 2003), and patient SA, who was previously shown to have a deletion of one TWIST allele (Johnson et al. 1998), had ratios of 0.47 and 0.50, respectively, whereas two human genomic DNA controls had a ratio of 0.93 and 1.02, respectively. In addition, three samples (R1945P, K2557J, J1887S) with heterozygous mutations detected by sequencing had a ratio from 0.92 to 1.10. These results validated our method and showed that the ratio of gene copy number as determined by real-time PCR could be used to detect heterozygous deletions of TWIST.
We proceeded to analyze for TWIST deletions in the 30 Saethre-Chotzen syndrome-like patients, who failed to show a mutation in the TWIST coding region by sequence analysis. Of the 26 patients who were not known to have chromosomal abnormalities, four cases (G1160D, S2517D, F2519T, and S2518C) showed heterozygous TWIST gene deletions (Fig. 3). We verified the presence of these deletions by FISH by using cosmid IIIA9 containing TWIST (Krebs et al. 1997) in two patients (S2517D and F2519T) (Fig. 4). Cell lines for the other patients were unavailable.

Heterozygous TWIST deletions identified by real-time PCR. Thirty Saethre-Chotzen syndrome cases negative for intragenic mutations were screened for deletions. Of the 26 patients not known to have chromosomal abnormalities, four were found to have a heterozygous deletion, with a gene copy number ratio TWIST/ACTIN of approximately 0.5. Of the four patients with chromosomal abnormalities, two were also found to have a deletion. Two heterozygous deletion controls had a ratio of approximately 0.5, whereas three patients with heterozygous mutations detected by sequencing (cross-hatched bars) and two normal controls had a ratio of approximately 1.0. Gray bars Data from patients with an abnormal karyotype

TWIST deletion in patient S2517D confirmed by FISH. Hybridization signal for cosmid IIIA9 probe is detected on one chromosome 7 but not on the other, indicating a deletion
Analysis of size of TWIST deletion by microsatellites and FISH
To confirm that the TWIST gene was indeed deleted in these four patients and to estimate further the extent of the deletion, we employed a microsatellite genotyping method of markers on 7p. Patient S2517D was demonstrated to have only paternal alleles for multiple microsatellite loci that extended from at least 600 kb to less than 8.7 Mb (between markers D7S513 and D7S2551). Patient F2519T was found to carry only maternal alleles from 5.5 Mb to 7.8 Mb (between markers D7S664 and D7S2562). Patient S2518C was homozygous for all markers in a region of less than 1.6 Mb (between D7S488 and D7S654), suggestive of a deletion. For patient G1160D, two markers flanking the TWIST gene were homozygous, but no DNA samples was available for further genotyping, and thus the extent of the deletion could not be estimated. Non-paternity was not observed in these patients.
We also used this microsatellite genotyping method to estimate the extent of the deletion for two patients with a deletion detected by both chromosomal analysis and real-time PCR gene dosage assay. We determined that the deletion for patient W63P (46,XY,del(7)(p15.3p21.3)) was less than 14.4 Mb between markers D7S2514 and D7S2510. We also determined that the deletion for patient C2535J (46,XY,del(7)(p15.1p21.3)) was less than 16 Mb between markers D7S481 and D7S2510.
To estimate the breakpoint location in our patients with a translocation or inversion, we made overlapping probes of about 10 kb in length at the suspected regions, and FISH analysis was performed to determine whether the breakpoints were within the region of the probe. For patient N1339D (46,XX,inv(7)(p21.3q34)), we narrowed the 7p21.3 breakpoint to a 10-kb region about 260 kb 3' of the TWIST gene (between D7S2532 and TWIST; data not shown). This 10-kb probe was generated by long-range PCR with primers: forward 5'-CTATAGGAGCAGCTACTCAGCAATGCCTTCTTCGC-3' and reverse 5'-GAGGGACTTTCCTTGCCTAAGATGTGTCACG-3'. With the same probe, we located the 7p22 breakpoint at more than 260 kb 3' of TWIST gene in patient M1389S (46,XY,t(2;7)(p23;p22)) reported in Lewanda et al. (1994). As expected, no TWIST deletions were detected in these two patients by real-time PCR analysis (Fig. 3).
Refinement of size of TWIST deletion by real-time PCR
From our results, patient S2518C had a heterozygous TWIST deletion of less than 1.6 Mb, which was the minimal region shared by all of our patients with large deletions and by three cases previouly published (Johnson et al. 1998). In addition to TWIST, two flanking genes, HDAC9 (480 kb 3' of TWIST) and FER3DL (30 kb 5' of TWIST), were identified in the critical region (http://genome.ucsc.edu). We applied the real-time PCR gene dosage assay further to refine the extent of the deletion in patient S2518C. The results showed that these two genes were not deleted in patient S2518C (ratio of HDAC9/ACTIN =0.92, FERD3L/ACTIN =0.89), thus narrowing the extent of the deletion to a 510-kb region between HDAC9 and FER3DL. For patients known to have larger deletions (S2517D, F2519T, W63P, C2535J), both genes were indeed deleted.
Discussion
Craniosynostosis syndromes have in the past been classified into several categories on the basis of clinical findings. Of the common craniosynostosis syndromes, Saethre-Chotzen syndrome is one of the most difficult to diagnose. The identification of mutations in the coding region of the TWIST gene as the cause of Saethre-Chotzen syndrome has proved invaluable for the diagnosis of this disorder and for genetic counseling. However, phenotypic variability and overlap among syndromes have complicated the classification of craniosynostosis conditions. For example, TWIST mutations have also been found in Robinow-Sorauf syndrome (Kunz et al. 1999; Cai et al. 2003) and Baller-Gerold syndrome (Seto et al. 2001), indicating that these two disorders may not be clinically and molecularly distinct and may lie within the spectrum of Saethre-Chotzen syndrome.
We screened for TWIST mutations in craniosynostosis patients with features of Saethre-Chotzen syndrome. Given the small size of the TWIST gene and the low cost of sequencing, it was straightforward to sequence the whole coding region to detect mutations. We identified nine intragenic mutations, three of which were novel. Of these, three nonsense and three deletion/frameshift mutations are clearly pathogenic. Both types of mutations are likely to abolish normal function by nonsense-mediated decay leading to haploinsufficiency, truncation of the protein resulting in loss of the functional helix-loop-helix region, and/or dominant negative effect attributable to the formation of abnormal proteins. The other three mutations, viz., two in-frame insertions and one missense, were previously reported as being pathogenic. These mutations are predicted to cause this dominant disease by reducing the functional activity of TWIST. For example, P139_S140insKIIPTLP significantly alters dimer formation (El Ghouzzi et al. 2000).
Besides intragenic mutation detection by sequencing, we have addressed the question of heterozygous deletions of the TWIST gene, because the syndrome can be caused by haploinsufficiency. We have developed a quantitative real-time PCR-based method to detect heterozygous deletion of the TWIST gene. Southern blot, microsatellite, and FISH analyses are often used for the detection of gene dosage change, but they are laborious and time consuming, utilize large amounts of genomic DNA, and are not sufficiently sensitive. Analysis of microsatellite and other polymorphic markers also requires parental DNA, confirmation of paternity, and informative genotypes. Southern blot hybridization can only detect deletions or rearrangements of several kilobases in size. FISH analysis can only detect large chromosomal deletions or rearrangements of several megabases in size. These problems can be overcome by real-time PCR, which offers major advantages, such as the large dynamic range of quantification and the exclusion of post-PCR manipulations, which minimizes the risk of carry-over contamination. The real-time PCR system usually allows quantitation of gene expression by employing labeled oligonucleotide probes, which generate sequence-specific signals. Some studies have made use of the real-time PCR method with gene-specific probes to study gene dosage (Ruiz-Ponte et al. 2000, Wilke et al. 2000). In contrast, we have used SYBR Green in the quantitative method in our study. Our method is fast (results usually being obtained within 2 h) and requires only minimal quantities of genomic DNA. Our data show that deletions can be reliably detected by using as low as 250 copies (less than 1 ng) of human genomic DNA. Our method is very sensitive because it can detect deletions less than 500 bp in length. Southern blot hybridization, microsatellite analysis, and FISH would miss such small deletions.
This real-time PCR based gene dosage analysis has broad applications. It not only can be used to detect deletions, but can also be applied to the detection of duplication or amplification. Similar techniques have been used to detect OA1 gene deletions in congenital nystagmus (Faugere et al. 2003), to analyze SMN1 and SMN2 quantitatively in spinal muscular atrophy (Feldkotter et al. 2002), and to investigate MYCN gene amplification in neuroblastoma (De Preter et al. 2002). We have also demonstrated that this method can be utilized to refine the extent of a deletion by "PCR walking" across the critical region. Theoretically, with a series of PCRs, the size of either small or large deletions and amplifications can be determined. As real-time PCR machines are becoming more and more common in diagnostic labs, they are being used in clinical applications, such as point mutation detection, rearrangement detection, and virus load quantification. We envision that real-time PCR will and can be used in clinical settings to screen for gene deletion or duplication. A secondary or comfirmatory technique (FISH or microsatellite genotyping) will eventually become unnecessary, given the accuracy and sensitivity of the real-time PCR method in detecting deletions.
Four of our Saethre-Chotzen patients, despite being karyotypically normal, have been shown, by our real-time PCR methodology, to have TWIST gene deletions. Two patients, who were previously suspected to have deletions in the region of TWIST by their abnormal karyotypes, were confirmed. To date, in the 55 patients whom we have investigated (this study; Howard et al. 1997; Paznekas et al. 1998), TWIST gene deletions have been detected in 6/55, an 11% improvement in detection rate. By combining real-time PCR and direct sequencing, we have detected mutations (including intragenic mutations and deletions) in 31/55 or 56% of our patient population. However, only 37 of the 55 patients have the classical features of Saethre-Chotzen syndrome, and the overall detection rate for these patients is higher at 25/37 or 68%. The other 18 craniosynostosis patients, including the four patients with abnormal karyotypes and four patients with deletions detected by real-time PCR, have few Saethre-Chotzen findings and/or in some cases additional features.
Of interest, it has been proposed that haploinsufficiency of the genes that neighbor TWIST contributes to significant learning difficulties (Johnson et at. 1998). All six of our patients (Table 2) and five out of six previously reported patients (Johnson et al. 1998; Gripp et al. 2001) with large deletions have developmental delay. Indeed, the flanking genes HDAC9 and FERD3L are expressed in the developing central nervous system (Zhou et al. 2001; Verzi et.al. 2002). However, our results showing deletion of the TWIST gene alone in patient S2518C with developmental delay implies that deletion of TWIST, without the deletion of neighboring genes, can cause developmental delay in Saethre-Chotzen patients. Furthermore, patient R1945P, who has a nonsense mutation in TWIST, and 4/39 of our previous series of Saethre-Chotzen patients with intragenic mutations (Paznekas et al. 1998) were also developmentally delayed. These results suggest that only 10% of patients with intragenic mutations, whereas approximately 90% of patients with large deletions, have developmental delay.
In two of our patients with chromosomal abnormalities, the breakpoints were located at 260 kb or more 3' of the TWIST gene. No intragenic mutations were found in the TWIST coding region. One can speculate that, in these two patients, a translocation or inversion occuring at a distance 3' of TWIST disrupts important regulatory elements. Scherer et al. (2003) have compiled a list of clinical cases with breakpoints on chromosome 7. They have noted position-effect mutations for the TWIST gene in Saethre-Chotzen syndrome (up to 100 kb 5' of the gene). Taking these data together, it seems that regulatory regions of TWIST may be located both 5' and 3' of the gene and act at a distance. The interruption of these regulatory regions may cause Saethre-Chotzen syndrome by position-effect mutations. Since only 68% of Sathre-Chotzen patients carried intragenic mutations or deletions, it is conceivable that some portion of the remaining patients have still-to-be-identified mutations in these critial 5' and 3' regulatory regions.
Johnson et al. (1998) also observed that TWIST deletions were of paternal original in three of three cases. However, in our study, patient S2517D inherited only the paternal allele. Therefore, our case is the first to show that a deletion of maternal origin can also occur in Saethre-Chotzen syndrome. Consistent with our results is the finding that none of the deletion syndromes to date has been found to be exclusively of either paternal or maternal origin, even though some recurrent point mutations are exclusively of paternal origin (Crow 2000).
To conclude, as an addition to conventional sequenced-based mutational analysis, we have developed a method based on quantitative real-time PCR to detect TWIST gene dosage change. We propose a step-wise strategy for screening TWIST mutations in order to achieve a higher detection rate in Saethre-Chotzen syndrome: PCR amplification with subsequent sequencing to identify intragenic mutations, followed by real-time PCR based gene dosage analysis to identify deletions encompassing the gene and the extent of the deletions. The detection of TWIST gene deletions has important prognostic implications for genetic counseling with regard to developmental delay in Saethre-Chotzen patients.
References
Boeck A, Kosan C, Ciznar P, Kunz J (2001) Saethre-Chotzen syndrome and hyper IgE syndrome in a patient with a novel 11 bp deletion of the TWIST gene. Am J Med Genet 104:53–56
Bourgeois P, Bolcato-Bellemin AL, Danse JM, Bloch-Zupan A, Yoshiba K, Stoetzel C, Perrin-Schmitt F (1998) The variable expressivity and incomplete penetrance of the Twist-null heterozygous mouse phenotype resemble those of human Saethre-Chotzen syndrome. Hum Mol Genet 7:945–957
Cai J. Shoo BA, Sorauf T, Jabs EW (2003) A novel mutation in the TWIST gene, implicated in Saethre-Chotzen syndrome, is found in the original case of Robinow-Sorauf syndrome. Clin Genet (in press)
Chen ZF, Behringer RR (1995) Twist is required in head mesenchyme for cranial neural tube morphogenesis. Genes Dev 9:686–699
Chotzen F (1932) Eine eigenartige familiaere Entwicklungsstoerung (Akrocephalosyndaktylie, Dysostosis craniofacialis und Hypertelorismus). Monatsschr Kinderheilk 55:97–122
Chun K, Teebi AS, Jung JH, Kennedy S, Laframboise R, Meschino WS, Nakabayashi K, Scherer SW, Ray PN, Teshima I (2002) Genetic analysis of patients with the Saethre-Chotzen phenotype. Am J Med Genet 110:136–143
Crow JF (2000) The origins, patterns and implications of human spontaneous mutation. Nat Rev Genet 1:40–47
De Preter K, Speleman F, Combaret V, Lunec J, Laureys G, Eussen BH, Francotte N, Board J, Pearson AD, De Paepe A, Van Roy N, Vandesompele J (2002) Quantification of MYCN, DDX1 and NAG gene copy number in neuroblastoma using a real-time quantitative PCR assay. Mod Pathol 15:159–166
Den Dunnen JT, Antonarakis SE (2000) Mutation nomenclature extensions and suggestions to describe complex mutations: a discussion. Hum Mutat 15:7–12
Dollfus H, Kumaramanickavel G, Biswas P, Stoetzel C, Quillet R, Denton M, Maw M, Perrin-Schmitt F (2001) Identification of a new TWIST mutation (7p21) with variable eyelid manifestations supports locus homogeneity of BPES at 3q22. J Med Genet 38:470–472
Elanko N, Sibbring JS, Metcalfe KA, Clayton-Smith J, Donnai D, Temple IK, Wall SA, Wilkie AO (2001) A survey of TWIST for mutations in craniosynostosis reveals a variable length polyglycine tract in asymptomatic individuals. Hum Mutat 18:535–541
El Ghouzzi V, Le Merrer M, Perrin-Schmitt F, Lajeunie E, Benit P, Renier D, Bourgeois P, Bolcato-Bellemin AL, Munnich A, Bonaventure J (1997) Mutations of the TWIST gene in the Saethre-Chotzen syndrome. Nat Genet 15:42–46
El Ghouzzi V, Legeai-Mallet L, Aresta S, Benoist C, Munnich A, Gunzburg J de, Bonaventure J (2000) Saethre-Chotzen mutations cause TWIST protein degradation or impaired nuclear location. Hum Mol Genet 9:813–819
Faugere V, Tuffery-Giraud S, Hamel C, Claustres M (2003) Identification of three novel OA1 gene mutations identified in three families misdiagnosed with congenital nystagmus and carrier status determination by real-time quantitative PCR assay. BMC Genet 4:1
Feldkotter M, Schwarzer V, Wirth R, Wienker TF, Wirth B (2002) Quantitative analyses of SMN1 and SMN2 based on real-time LightCycler PCR: fast and highly reliable carrier testing and prediction of severity of spinal muscular atrophy. Am J Hum Genet 70:358–368
Funato N, Ohtani K, Ohyama K, Kuroda T, Nakamura M (2001) Common regulation of growth arrest and differentiation of osteoblasts by helix-loop-helix factors. Mol Cell Biol 21:7416–7428
Gripp KW, Zackai EH, Stolle CA (2000a) Mutations in the human TWIST gene. Hum Mutat 15:150–155
Gripp KW, Zackai EH, Stolle CA (2000b) Erratum—mutations in the human TWIST gene. Hum Mutat 15:479
Gripp KW, Kasparcova V, McDonald-McGinn DM, Bhatt S, Bartlett SP, Storm AL, Drumheller TC, Emanuel BS, Zackai EH, Stolle CA (2001) A diagnostic approach to identifying submicroscopic 7p21 deletions in Saethre-Chotzen syndrome: fluorescence in situ hybridization and dosage-sensitive Southern blot analysis. Genet Med 3:102–108
Hamamori Y, Sartorelli V, Ogryzko V, Puri PL, Wu HY, Wang JY, Nakatani Y, Kedes L (1999) Regulation of histone acetyltransferases p300 and PCAF by the bHLH protein twist and adenoviral oncoprotein E1A. Cell 96:405–413
Hoover-Fong JE, Cai J, Cargile CB, Thomas GH, Patel A, Griffin CA, Jabs EW, Hamosh A (2003) Facial dysgenesis: a novel facial syndrome with chromosome 7 deletion p15.1–21.1. Am J Med Genet 117A:47–56
Howard TD, Paznekas WA, Green ED, Chiang LC, Ma N, Ortiz de Luna RI, Garcia Delgado C, Gonzalez-Ramos M, Kline AD, Jabs EW (1997) Mutations in TWIST, a basic helix-loop-helix transcription factor, in Saethre-Chotzen syndrome. Nat Genet 15:36–41
Jabs EW (2001) A TWIST in the fate of human osteoblasts identifies signaling molecules involved in skull development. J Clin Invest 107:1075–1077
Johnson D, Horsley SW, Moloney DM, Oldridge M, Twigg SR, Walsh S, Barrow M, Njolstad PR, Kunz J, Ashworth GJ, Wall SA, Kearney L, Wilkie AO (1998) A comprehensive screen for TWIST mutations in patients with craniosynostosis identifies a new microdeletion syndrome of chromosome band 7p21.1. Am J Hum Genet 63:1282–1293
Krebs I, Weis I, Hudler M, Rommens JM, Roth H, Scherer SW, Tsui LC, Fuchtbauer EM, Grzeschik KH, Tsuji K, Kunz J (1997) Translocation breakpoint maps 5 kb 3' from TWIST in a patient affected with Saethre-Chotzen syndrome. Hum Mol Genet 6:1079–1086
Kunz J, Hudler M, Fritz B (1999) Identification of a frameshift mutation in the gene TWIST in a family affected with Robinow-Sorauf syndrome. J Med Genet 36:650–652
Lewanda AF, Green ED, Weissenbach J, Jerald H, Taylor E, Summar ML, Phillips JA 3rd, Cohen M, Feingold M, Mouradian W, Clarren SK, Jabs EW (1994) Evidence that the Saethre-Chotzen syndrome locus lies between D7S664 and D7S507, by genetic analysis and detection of a microdeletion in a patient. Am J Hum Genet 55:1195–1201
Paznekas WA, Cunningham ML, Howard TD, Korf BR, Lipson MH, Grix AW, Feingold M, Goldberg R, Borochowitz Z, Aleck K, Mulliken J, Yin M, Jabs EW (1998) Genetic heterogeneity of Saethre-Chotzen syndrome, due to TWIST and FGFR mutations. Am J Hum Genet 62:1370–1380
Rice DP, Aberg T, Chan Y, Tang Z, Kettunen PJ, Pakarinen L, Maxson RE, Thesleff I (2000) Integration of FGF and TWIST in calvarial bone and suture development. Development 127:1845–1855
Rose CS, Patel P, Reardon W, Malcolm S, Winter RM (1997) The TWIST gene, although not disrupted in Saethre-Chotzen patients with apparently balanced translocations of 7p21, is mutated in familial and sporadic cases. Hum Mol Genet 6:1369–1373
Ruiz-Ponte C, Loidi L, Vega A, Carracedo A, Barros F (2000) Rapid real-time fluorescent PCR gene dosage test for the diagnosis of DNA duplications and deletions. Clin Chem 46:1574–1582
Saethre M (1931) Ein Beitrag zum Turmschaedelproblem (Pathogenese, Erblichkeit und Symptomatologie). Dtsch Z Nervenheilk 119:533–555
Scherer SW, Cheung J, MacDonald JR, Osborne LR, Nakabayashi K, Herbrick JA, Carson AR, Parker-Katiraee L, Skaug J, Khaja R, Zhang J, et al (2003) Human chromosome 7: DNA sequence and biology. Science 300:767–772
Seto ML, Lee SJ, Sze RW, Cunningham ML (2001) Another TWIST on Baller-Gerold syndrome. Am J Med Genet 104:323–330
Verzi MP, Anderson JP, Dodou E, Kelly KK, Greene SB, North BJ, Cripps RM, Black BL (2002) N-Twist, an evolutionarily conserved bHLH protein expressed in the developing CNS, functions as a transcriptional inhibitor. Dev Biol 249:174–190
Wilke K, Duman B, Horst J (2000) Diagnosis of haploidy and triploidy based on measurement of gene copy number by real-time PCR. Hum Mutat 16:431–436
Zhou X, Marks PA, Rifkind RA, Richon VM (2001) Cloning and characterization of a histone deacetylase, HDAC9. Proc Natl Acad Sci USA 98:10572–10577
Acknowledgements
We thank the families and their physicians and counselors, including Lola Cook, Donald Day, Luna Okada, Michael Petersen, Peggy Rush, Lawrence Walsh, Lester Weiss, and Wilfredo Torres for their participation. We are grateful to J. Kunz for cosmid IIIA9 (Kunz et al. 1999) and A.O. Wilkie for DNA from SA (Johnson et al. 1999). This work was funded by NIH P60 DE13078, T32 GM07814, RO1 HD 24061, and M01 RR0052.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Cai, J., Goodman, B.K., Patel, A.S. et al. Increased risk for developmental delay in Saethre-Chotzen syndrome is associated with TWIST deletions: an improved strategy for TWIST mutation screening. Hum Genet 114, 68–76 (2003). https://doi.org/10.1007/s00439-003-1012-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00439-003-1012-7