
Abstract
In European countries, toxoplasma antenatal screening is recommended to prevent toxoplasmosis. The seroprevalence of these infections in immigrants can be different than in native population. From February 2006 to June 2010, a cross-sectional study was carried out in all pregnant women attended at a reference unit in Elche, Spain. An enzyme immunoassay was used for detection of IgG antibodies against Toxoplasma gondii. For each immigrant woman, one Spanish pregnant woman of the same age cared for in the same day was recruited (Spanish control group). A total of 1,627 migrant pregnant women participated in this study. The adherence to screening among migrants was 91.9% (95% CI, 90.5–93.1%), similar than that found in Spaniards (92.2%; 95% CI, 90.8–93-4%). Among migrant women, 619 were positive for IgG anti-T. gondii antibodies (41.4%; 95% CI, 38.9–43.9%), compared with 12.0% (95% CI, 10.5–13.8%) among Spaniards (odds ratio (OR), 5.2 (95% CI, 4.3–6.3). Seroprevalence in pregnant women from Latin America, northern Africa, Eastern Europe, Africa Sub-Saharan and Western Europe was higher than in the Spanish control group (OR, 5.4, 5.8, 6.5, 5.4, and 2.4, respectively; p < 0.001). No Asian pregnant woman was immune. Seroprevalence increased with increasing age in migrant pregnant women: 15–25 years, 38.2%; 26–35 years, 40.7%; and 36–45 years, 52.8%. The seroprevalence of T. gondii infection in migrant pregnant women living in Spain was higher than in the native population. However, no cases were found in Asian immigrants, highlighting the importance of primary prevention of this infection in pregnant women coming from that geographic region.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Toxoplasmosis is a worldwide endemic disease caused by an obligate intracellular parasite, Toxoplasma gondii. Toxoplasmosis during pregnancy can cause congenital infection and manifest as mental retardation and blindness in the infant. The severity of fetal diseases varies inversely with the gestational age at which maternal infection occurs (Tenter et al. 2000).
Seroprevalence estimated for human population varies greatly among different countries, among different geographical areas within one country and among different ethnic groups living in the same area (Tenter et al. 2000). Seroprevalence of T. gondii infection in women at childbearing age ranges between 4–100% (Ertug et al. 2005; Montoya and Liesenfeld 2004). The highest rates have been found in countries from Central and South America, Africa and Asia (>60%) (Lin et al. 2008; Montoya and Liesenfeld 2004; Rosso et al. 2008). Over the past few decades, seroprevalence of T. gondii infection has been decreasing both in developed countries and to a lesser extent in developing countries (Montoya and Liesenfeld 2004).
The large wave of immigration in Spain has occurred within the last 10 years. Between 1998 and 2009, the number of foreigners registered in Spain has grown more than six times, from 637,058 to 6,466,278, which in 2009 accounted for 13.8% of the total Spanish population. Of the immigrant population, 1.35 million were born in the European Union (including 762,000 in Romania), 2.45 million are from Latin America and 1.04 million are from Africa (including 245,000 from Sub-Saharan) and Asia 323,000 (Instituto Nacional de Estadística 2010). The mobile population to Spain has changed the prevalence of different infectious diseases, including viral hepatitis, Chagas disease and syphilis (Manzardo et al. 2008; Monge-Maillo et al. 2009).
In Spain, serological screening is recommended to prevent congenital toxoplasmosis as part of the antenatal protocol. There are a few studies of seroprevalence of T. gondii infection in immigrant pregnant women in Spain (Bartolomé Alvarez et al. 2008) and other Western countries (Tomasoni et al. 2010). The objective of this study was to investigate (1) the prevalence of T. gondii infection and (2) adherence to the screening national programme in immigrant pregnant women in Eastern Spain according to countries of origin.
Patients and methods
From January 2006 to May 2010, a cross-sectional study was conducted in all pregnant women attended at Hospital General Universitario de Elche, Alicante, a general medical centre located in the Mediterranean Coast of Spain. During the study period, the hospital provided medical care to 290,481 inhabitants, from three municipalities: Crevillente (28,609 inhabitants), Elche (230,112 inhabitants) and Santa Pola (31,760 inhabitants), distributed in 11 primary care centres. A total of 44,341 of them were foreign people: 12,955 from Latin America and The Caribbean (29.9%), 11,271 were from Western Europe (25.4%), 9,330 were from Eastern Europe (2.0%), 7,508 were from Northern Africa (16.9%), 1,666 from Africa Sub-Saharan (3.7%) and 1,611 from Asia (3.6%). All immigrant women attending the antenatal clinic during the weeks previous to delivery were invited to participate and recruited in a consecutive manner (migrant group). For each immigrant enrolled, one Spanish pregnant woman with the same age attending in the same day was recruited (Spanish control group). Informed consent was obtained from all subjects. Blood samples for anti-T. gondii antibody testing were also taken in the first term of gestation for antenatal routine examination in primary care centres. The age and country of origin were collected in a case sheet specially designed for this study. The migrant population were divided in six groups according the geographical area of birth (Central and South America and The Caribbean, Northern Africa and Middle East, Sub-Saharan Africa, Eastern Europe, Western Europe and Asia).
The detection of IgG antibodies against T. gondii was performed by an enzyme immunoassay (Enzygnost toxoplasmosis/IgG, Siemens, Marburg, Germany), according to the manufacturer’s instructions.
A descriptive analysis was performed by setting the rates. The adherence to screening programme among migrant and Spanish women were calculated by the number of pregnant women in which an anti-T. gondii antibody test was performed in the primary care centre divided by total of pregnant women included in the study. We obtained estimates of the prevalence with confidence intervals (CI) of 95% by the method of Fleiss. We calculated the odds ratio (OR) with 95% of CI of each group of migrants with respect to the Spanish group (reference category).
Results
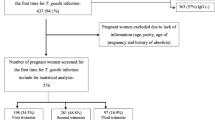
A total of 1,627 migrant pregnant women participated in this study. The distribution according to geographical area of birth was as follows: Latin America and The Caribbean (564; 34.6%), Northern Africa and Middle East (550; 33.8%), Eastern Europe (288; 15.7%), Sub-Saharan Africa (99; 6.1%), Asia (77; 4.7%) and Western Europe (49; 3.0%). The main country of origin was Morocco (492; 33.8%), followed by Romania (209; 12.8%) and Colombia (163; 10%) as shown in Table 1. Epidemiological data of participants by geographical distribution and country of birth are shown in Table 2. The mean age was 28.4 years (range, 15–45 years). Women from Eastern Europe were significantly younger than those coming from other geographical areas (29.9 years; p < 0.001). The mean time elapsed from arrival to Spain to consultation at the antenatal clinic was 48 months (range, 1 week to 170 months); this period was longer for pregnant women from Latin America and Western Europe (60 months in both regions) and lower for those from Northern Africa and Asia (36 months in both regions).
The adherence to the screening programme among migrants was 91.9% (95% CI, 90.5–93.1%), similar to Spaniards (92.2%; 95% CI, 90.8–93.4%). The adherence was lower in women from Western Europe (83.7%; 95% CI, 70.9–91.4%; p = 0.05) (Table 3).
IgG anti-T. gondii antibodies were positive in 619 of 1,495 (41.4%; 95% CI, 38.9–43.9%) migrant women and 179 of 1,488 (12.0%; 95% CI, 10.5–13.8%) Spaniards (OR, 5.2; 95% CI, 4.3–6.3). The seroprevalence for pregnant women from Latin America, Northern Africa, Eastern Europe, Africa Sub-Saharan and Western Europe are shown in Table 3. In pregnant women from all these areas, the prevalence was higher than that found in Spaniards (OR, 5.4%, 5.8%, 6.5%, 5.4%, and 2.4%, respectively; p < 0.001). No Asian pregnant woman was immune (OR, 0.0; 95% CI, 0.0–38.5%). Seroprevalence increased with increasing age in both migrants and Spaniards: 15–25 years: 38.2% and 7.4%, respectively; 26–35 years: 40.7% and 12.2%, respectively; and 36–45 year 52.8% and 23.7%, respectively. The increase in seroprevalence with age was seen in migrant women from all geographic areas (Fig. 1).

Seroprevalence of IgG anti-Toxoplasma cruzi antibodies in immigrant and native pregnant women stratified by age group 16 to 25, 26 to 35 and more than 35 years
Discussion
In the current study, the seroprevalence of Toxoplama-specific IgG was 12.0% in native pregnant women. In native women at childbearing age in Spain, a seroprevalence between 16% to 29% has been found during the last decade (Bartolomé Alvarez et al. 2008; Gutiérrez-Zufiaurre et al. 2004; Muñoz Batet et al. 2004). Our study confirms that T. gondii prevalence has continued to decline, approaching the seroprevalence of Northern European countries as The Netherlands (Hofhuis et al. 2010), Norway (Chen et al. 2005), Sweden (Evengård et al. 2001) or UK (Nash et al. 2005).
The seroprevalence of Toxoplama specific IgG was 41.1% in migrant pregnant women, significantly higher than in the native pregnant women. Other studies performed in Spain and in other European countries have also recorded a higher rate of infection among migrant pregnant women than those found in native populations (Bartolomé Alvarez et al. 2008; Tomasoni et al. 2010)
The seroprevalence in women from Latin America, Northern Africa and Sub-Saharan Africa was around 43%, a figure slightly lower than that found in women from Eastern Europe countries (47%). The seroprevalence in women coming from Western Europe countries was 24.4%, lower than in developing countries and slightly higher than in Spaniards. Noteworthy, in women coming from Asia, mainly from China, not a single case of T. gondii infection was detected.
The seroprevalence of T. gondii among migrant women in Spain reflects the prevalence of T. gondii specific IgG antibodies in their countries of birth, because the immigration in Spain is a recent fact. In this study, the majority of the women had been in Spain by less than 5 years, and the infection probably had been acquired in their country of origin. In survey studies carried out in Latin America, the seroprevalence varied from 30% in Chile (Contreras et al. 1995) to 46% in Colombia (Rosso et al. 2008) and 65% in Brazil (Fernandes et al. 2009). Human toxoplasmosis is endemic in Morocco where the seroprevalence is above 50% (El Mansouri et al. 2007) and the age plays a role in the epidemiology of the infection (Laboudi et al. 2009). A recent study performed in Qatar has found different prevalence rates of T. gondii according to origin of the patients: from 25% in patients from the Arabian Peninsula to 45% in people from African countries (Abu-Madi et al. 2008). Epidemiologic data published in the medical literature from Romania (Eastern Europe) are scantly. The seroprevalence of T. gondii antibodies among pregnant women is about 44% (Crucerescu 1998). Seroepidemiological studies from different Western Sub-Saharan African countries show prevalence rates ranging from 27 to 45% (Akinbami et al. 2010; Faye et al. 1998; Kamani et al. 2009).
The reported prevalence of T. gondii infection in the Chinese population is around 7–12%, but the sample size of most serological surveys have been limited (Liu et al. 2009; Xiao et al. 2010). Nevertheless, the prevalence has been generally lower than that found in other developed countries (Montoya and Liesenfeld 2004). This low prevalence of T. gondii among Chinese people is in line with the fact that we did not find a single case of the infection among the 73 women tested in our survey. Therefore, in our area is very important to inform Chinese pregnant women about the risk factors for acquiring toxoplasmosis in order to prevent the infection (mainly avoidance of consuming raw meat).
Interestingly, the age related trend in prevalence of IgG antibodies has been seen in each of the six groups representing countries of origin of the patients, as well as in the native pregnant women. The overall trend in each regional group was similar, indicating that there is ongoing and repeated exposure to T. gondii in all groups in the countries of origin, including Spain. The increasing seroprevalence with age highlights the continuing need to educate women of childbearing age about the risk factors for acquiring toxoplasmosis.
The adherence to the screening programme of T. gondii infection to prevent congenital toxoplasmosis among migrant pregnant women was similar than in Spaniards. This is probably related to the fact that in Spain the National Health Service is accessible free of charge for all population with independence of the irregular o regular legal situation of the people living in the country. In Italy, the adherence to screening programme was lower in immigrant than in native pregnant women (Tomasoni et al. 2010).
Although our data cannot be considered to reflect prevalence rates throughout the entire population, they provide a quantitative data on toxoplasmosis in the human community in Spain according of country of origin. The study has some limitations. The sample size was restricted by the characteristics of Spanish immigrant populations. As a result, Asian women were less represented and the estimates are therefore less accurate. We did not collect risk factors associated with acquisition of T. gondii infection as contact with cats, eating undercooked meat, working with soil or drinking beverages prepared with unboiled water.
In summary, the study confirms that the prevalence of T. gondii infection continues to decline in native Spanish population, thus contrasting with the high prevalence found in migrants from most geographic regions, except those coming from Asia. Targeted programmes aimed to primary prevention of toxoplasmosis in Asian pregnant women are warranted.
References
Abu-Madi MA, Al-Molawi N, Behnke JM (2008) Seroprevalence and epidemiological correlates of Toxoplasma gondii infections among patients referred for hospital-based serological testing in Doha, Qatar. Parasit Vectors 1:39
Akinbami AA, Adewunmi AA, Rabiu KA, Wright KO, Dosunmu AO, Dada MO, Adeyemo TA (2010) Seroprevalence of Toxoplasma gondii antibodies amongst pregnant women at the Lagos State University Teaching Hospital, Nigeria. Niger Postgrad Med J 17:164–167
Bartolomé Alvarez J, Martínez Serrano M, Moreno Parrado L, Lorente Ortuño S, Crespo Sánchez MD (2008) Prevalence and incidence in Albacete, Spain, of Toxoplasma gondii infection in women of childbearing age: differences between immigrant and non-immigrant (2001–2007). Rev Esp Salud Pública 82:333–342
Chen KT, Eskild A, Bresnahan M, Stray-Pedersen B, Sher A, Jenum PA (2005) Previous maternal infection with Toxoplasma gondii and the risk of fetal death. Am J Obstet Gynecol 193:443–449
Contreras MC, Escaff V, Salinas P, Saavedra T, Suárez M (1995) Parasitic and viral marker detection in pregnant adolescents and their newborn infants at risk. Rev Chil Obstet Ginecol 60:85–89
Crucerescu E (1998) Epidemiological data on toxoplasmosis. The aspects of congenital toxoplasmosis. Bacteriol Virusol Parazitol Epidemiol 43:147–155
El Mansouri B, Rhajaoui M, Sebti F, Amarir F, Laboudi M, Bchitou R, Hamad M, Lyagoubi M (2007) Seroprevalence of toxoplasmosis in pregnant women in Rabat, Morocco. Bull Soc Pathol Exot 100:289–290
Ertug S, Okyay P, Turkmen M, Yuksel H (2005) Seroprevalence and risk factors for toxoplasma infection among pregnant women in Aydin province, Turkey. BMC Public Health 5:66
Evengård B, Petersson K, Engman ML, Wiklund S, Ivarsson SA, Teär-Fahnehjelm K, Forsgren M, Gilbert R, Malm G (2001) Low incidence of toxoplasma infection during pregnancy and in newborns in Sweden. Epidemiol Infect 127:121–127
Faye O, Leye A, Dieng Y, Richard-Lenoble D, Diallo S (1998) Toxoplasmosis in Dakar. Seroepidemiologic sampling of 353 women of reproductive age. Bull Soc Pathol Exot 91:249–250
Fernandes GC, Azevedo RS, Amaku M, Yu AL, Massad E (2009) Seroepidemiology of Toxoplasma infection in a metropolitan region of Brazil. Epidemiol Infect 137:1809–1815
Gutiérrez-Zufiaurre N, Sánchez-Hernández J, Muñoz S, Marín R, Delgado N, Sáenz MC, Muñoz-Bellido JL, García-Rodríguez JA (2004) Seroprevalence of antibodies against Treponema pallidum, Toxoplasma gondii, rubella virus, hepatitis B and C virus, and HIV in pregnant women. Enferm Infecc Microbiol Clín 22:512–516
Hofhuis A, van Pelt W, van Duynhoven YT, Nijhuis CD, Mollema L, Van Der Klis FR, Havelaar AH, Kortbeek LM (2010) Decreased prevalence and age-specific risk factors for Toxoplasma gondii IgG antibodies in The Netherlands between 1995/1996 and 2006/2007. Epidemiol Infect 24:1–9
Instituto Nacional de Estadística. Avance del Padrón Municipal a 1 de enero 2010 (2010). Available at: http://www.ine.es/prensa/np595.pdf. Accessed 1 May 2010
Kamani J, Mani AU, Egwu GO, Kumshe HA (2009) Seroprevalence of human infection with Toxoplasma gondii and the associated risk factors, in Maiduguri, Borno state, Nigeria. Ann Trop Med Parasitol 103:317–321
Laboudi M, El Mansouri B, Sebti F, Amarir F, Coppieters Y, Rhajaoui M (2009) Risk factors of a positive serological test for toxoplasmosis in a pregnant women in Morocco. Parasite 16:71–72
Lin YL, Liao YS, Liao LR, Chen FN, Kuo HM, He S (2008) Seroprevalence and sources of Toxoplasma infection among indigenous and immigrant pregnant women in Taiwan. Parasitol Res 103:67–74
Liu Q, Wei F, Gao S, Jiang L, Lian H, Yuan B, Yuan Z, Xia Z, Liu B, Xu X, Zhu XQ (2009) Toxoplasma gondii infection in pregnant women in China. Trans R Soc Trop Med Hyg 103:162–166
Manzardo C, Treviño B, i Prat Gómez J, Cabezos J, Monguí E, Clavería I, Del Val Luis J, Zabaleta E, Zarzuela F, Navarro R (2008) Communicable diseases in the immigrant population attended to in a tropical medicine unit: epidemiological aspects and public health issues. Travel Med Infect Dis 6:4–11
Monge-Maillo B, Jiménez BC, Pérez-Molina JA, Norman F, Navarro M, Pérez-Ayala A, Herrero JM, Zamarrón P, López-Vélez R (2009) Imported infectious diseases in mobile populations, Spain. Emerg Infect Dis 15:1745–1752
Montoya JG, Liesenfeld O (2004) Toxoplasmosis. Lancet 363:1965–1976
Muñoz Batet C, Guardià Llobet C, Juncosa Morros T, Viñas Domenech L, Sierra Soler M, Sanfeliu Sala I, Bosch Mestres J, Dopico Ponte E, Lite Lite J, Matas Andreu L, Juste Sánchez C, Barranco Romeu M (2004) Toxoplasmosis and pregnancy. Multicenter study of 16,362 pregnant women in Barcelona. Med Clin (Barc) 123:12–16
Nash JQ, Chissel S, Jones J, Warburton F, Verlander NQ (2005) Risk factors for toxoplasmosis in pregnant women in Kent, United Kingdom. Epidemiol Infect 133:475–483
Rosso F, Les JT, Agudelo A, Villalobos C, Chaves JA, Tunubala GA, Messa A, Remington JS, Montoya JG (2008) Prevalence of infection with Toxoplasma gondii among pregnant women in Cali, Colombia, South America. Am J Trop Med Hyg 78:504–508
Tenter AM, Heckeroth AR, Weiss LM (2000) Toxoplasma gondii: from animals to humans. Int J Parasitol 30:1217–1258
Tomasoni LR, Sosta E, Beltrame A, Rorato G, Bigoni S, Frusca T, Zanardini C, Driul L, Magrini F, Viale P, Castelli F (2010) Antenatal screening for mother to child infections in immigrants and residents: the case of toxoplasmosis in Northern Italy. J Immigr Minor Health 12:834–840
Xiao Y, Yin J, Jiang N, Xiang M, Hao L, Lu H, Sang H, Liu X, Xu H, Ankarklev J, Lindh J, Chen Q (2010) Seroepidemiology of human Toxoplasma gondii infection in China. BMC Infect Dis 10:4
Acknowledgements
We thank the midwives of the Health Department of Hospital General Universitario de Elche for their assistance in collecting the data and samples of patients, especially to Ms. Paqui Rodrigo.
Conflicts of interest
There are no conflicts of interest, financial or of any other nature that may affect professional judgment in relation to this article.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Ramos, J.M., Milla, A., Rodríguez, J.C. et al. Seroprevalence of Toxoplasma gondii infection among immigrant and native pregnant women in Eastern Spain. Parasitol Res 109, 1447–1452 (2011). https://doi.org/10.1007/s00436-011-2393-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00436-011-2393-5