
Abstract
Hypersensitivity to Anisakis simplex is a worldwide medical problem. The parasite larvae die after freezing or cooking, but the tolerance of sensitized subjects to eating frozen fish remains a matter of controversy with contradictory findings. The aim of this study was to test if intolerance to properly cooked/frozen fish was due to the recognition of a particular allergen. Sixty-four patients with Anisakis simplex sensitization were studied by an IgE multiblot using simultaneously five different antigenic extracts. The antigens tested were a crude extract, excretory/secretory allergens, a heated extract, and two gradient ethanol precipitates of the crude extract. Intolerance was reported by 20% of the patients and was not related to the detection of any special allergen, nor to total or specific IgE levels. Intolerant patients only reported a higher frequency of digestive symptoms than the patients who tolerated fish ingestion. The most sensitive immunoblot antigen source was the 50–66% ethanol fraction of a crude extract (10× concentrated) that was found to be positive in 100% of the samples. Interestingly, 95% sensitivity in the IgE-immunoblot assay could be achieved using only two allergens, Ani s 1 and Ani s 4. Allergens from the dead larvae remain a problem for 20% of the sensitized subjects. The use of a fractionated and concentrated crude extract improved the sensitivity of the immunoblot assay.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Reports from many countries describe patients with acute or chronic disease due to the fish parasite Anisakis simplex (Buendia 1997; Akbar and Ghosh 2005). Allergic symptoms ranging from mild urticaria to anaphylactic shock are due to the presence of immunoglobulin E (IgE) antibodies that constitute an important component of immune response to the parasite (del Pozo et al. 1999; Daschner et al. 2000). The in vivo (skin-prick tests) and/or in vitro level of specific IgE are usually measured for diagnosis of sensitization to the parasite, and it is accepted that these determinations are highly sensitive methods (Lorenzo et al. 2000).
Specific IgE to allergens from the parasite can be also detected by immunoblotting. This method, although being more specific, lacks the sensitivity of CAP or skin tests (Lorenzo et al. 2000; Garcia et al. 1997; del Pozo et al. 1996). In this sense, the use of excretory/secretory allergens for clinical diagnosis increases the sensitivity and specificity of diagnosis (Baeza et al. 2004; Moneo and Caballero 2002). Allergens from the parasite are at present poorly characterized; many IgE-binding proteins remain unknown, and the clinical usefulness of different antigen sources (crude, heated, secretory, etc.) must be evaluated in the diverse diagnostic approaches (Baeza et al. 2004; Moneo and Caballero 2002; Rodero et al. 2004, 2005).
The risk of ingestion of properly cooked and frozen fish is still a matter of controversy. Some authors describe that sensitized patients tolerate ingestion of high amounts of lyophilized larvae or even excretory/secretory allergens (Baeza et al. 2004; Sastre et al. 2000), but others report clinical symptoms in patients after eating frozen or canned fish (Santaolalla 2006; Audicana et al. 2002; Moreno-Ancillo et al. 1997: Moneo et al. 2005). This discrepancy could result from the fact that some, but not all sensitized patients could detect heat-resistant allergens of the parasite, presenting symptoms only after eating fish that contains sufficient amount of these allergens.
The present work describes clinical and laboratory information obtained from patients with proven parasite sensitization, testing simultaneously five different antigenic sources.
Material and methods
Patients
Sixty-four patients referred for suspected Anisakis sensitization were studied after filling out a clinical questionnaire. Three doubtful cases (e.g., patients referring chronic urticaria, pruritus, etc., as not clearly related to fish ingestion) were put on a fish-exclusion diet and interviewed again 3 months later. Those patients that were still symptomatic after the diet were excluded from the study. All the included subjects had clinical symptoms in the first 24 h after raw or cooked fish consumption, and a CAP value to Anisakis > 0.7 kU/l and negative to fish. The patients were classified according to a clinical score in three categories (life-threatening symptoms score 3, moderate symptoms score 2, mild symptoms score 1). Thirty normal subjects with a negative CAP value, not complaining of symptoms after eating fish, were included in the study as a specificity control.
Antigen sources
-
1.
Crude antigen extract was obtained after crushing in a mortar manually collected larvae as described (Garcia et al. 1997; del Pozo et al. 1996).
-
2.
Excretory/secretory allergens (E/S) were obtained incubating larvae at a low pH (Moneo and Caballero 2002). The supernatant of this incubation was concentrated 10× for use in immunoblotting (Moneo et al. 2000).
-
3.
To obtain heat-resistant antigens, the crude extract was heated for 30 min in a boiling water bath and centrifuged for 15 min at 4,000 g (Moneo et al. 2005).
-
4.
To obtain enriched fractions, 5 ml of crude extract was mixed with the same volume of absolute ethanol. After 30 min, it was centrifuged at 4,000 g for 15 min, and the supernatant was now mixed with 5 ml ethanol to obtain a final ethanol concentration of 66%. After a new 30-min incubation, the mixture was centrifuged as above, and the pellet was resuspended in 0.5 ml of phosphate-buffered saline (PBS; Moneo et al. 2000). This fraction was considered as a 50–66% differential ethanol fraction.
-
5.
The ethanol content of the last supernatant obtained was now increased to 90%, incubated for an additional 30 min and centrifuged. The pellet was resuspended in 0.5 ml of PBS and considered as a 66–90% ethanol fraction.
IgE determinations and immunoblotting
Total and specific IgE was determined by CAP (Pharmacia, Uppsala, Sweden) according to manufacturer’s instructions.
Sodium dodecyl sulfate polyacrylamide gel electrophoresis (SDS-PAGE) was performed on 16% polyacrylamide minigels. The five different antigens (10 ul) were mixed with non-reducing sample buffer and electrophoresced at 150 V. Two sets of antigens were run in each gel (ten lanes). Antigens were transferred to nitrocellulose by diffusion, and two membranes were obtained from each gel. The membranes were cut in half after transfer, and in this way, each gel allowed the study of four patients’ sera. After transfer, simultaneous specific IgE detection to the five antigenic sources by immunoblotting was carried out as previously described without modifications (Moneo et al. 2000).
Specific IgE to Ani s 1 or to Ani s 4 was considered positive in the human samples when bands of molar weights of the allergens were detected, and these bands were more intensely stained in lane 4 corresponding to the 50–66% fraction (Moneo et al. 2000, 2005).
Results
Laboratory determinations
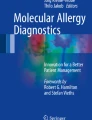
Figure 1 shows the protein profile of the different parasite extracts. Ethanol (50% v/v) induced a large precipitate, remaining in solution relevant allergens that could be now used 10× concentrated and separated in two different fractions, 50–66% and 66–90%. The major allergens Ani s 1 and 4 were previously purified after the same 50–66% ethanol precipitation from crude parasite extracts (Moneo et al. 2000, 2005), and this fraction induced stronger bands in the blot assays and, at the same time, contained other allergens. The other concentrated fraction (66–90%) also showed stronger detection of allergens. Representative patterns of the simultaneous detection of allergens in the five different parasite extracts are shown in Fig. 2, where the influence of the allergen concentration induced by the differential precipitation is clearly shown.

SDS-PAGE (16% acrylamide) of the different antigenic sources. Lanes 1 to 5 Crude extract, excretory/secretory antigens, heated crude extract, 50–66% ethanol fractionation, and 66–90% ethanol fractionation

Representative IgE multiblot patterns of sensitized patients. From left to right: patient detecting multiple IgE-binding proteins, patient monosensitized to Ani s 1, patient mainly sensitized to Ani s 4. Lanes 1 to 5 Crude extract, excretory/secretory antigens, heated crude extract, 50–66% ethanol fractionation, and 66–90% ethanol fractionation
The usefulness of the different parasite extracts and the frequency of Ani s 1 and 4 detection are represented in Fig. 3. As can be seen, the 50–66% ethanolic fraction had the highest diagnostic capacity, as it was positive in all the samples, followed by the crude extract (95%). The high diagnostic value of Ani s 1 (89% sensitivity) could be further increased by the combined detection of Ani s 1 and 4 detection and had the same sensitivity as the crude extract. This was caused by the presence of negative samples to Ani s 1 detecting Ani s 4 as shown in Fig. 4, which again demonstrates the usefulness of the ethanolic fractions when compared to the other alternatives. No positive results were obtained in the control group.

Percentages of positive results obtained in the 64 patients using the different antigenic sources. Positivity to Ani s 1 and 4 was considered when bands of compatible molar weight appeared in the first three lanes, and stronger bands in the fourth lane were observed (50–66% ethanol precipitation)

A representative case of increased sensitivity in the multiblot system using concentrated antigenic fractions in lanes 4 and 5. Serum sample from a sensitized patient, showing only faint bands in the crude extract (lane 1), excretory/secretory allergens (lane 2) or heated extract (lane 3), and clear positive results in the concentrated crude antigen fractions (lane 4 50–66% ethanol fractionation, lane 5 66–90% ethanol fractionation)
Clinical findings
Clinical symptoms after eating properly cooked and/or frozen fish were reported by 13 (20%) of the 64 patients enrolled in the study. We, therefore, tried to determine if this group of intolerant patients had any peculiarity compared with the tolerant subjects. The following variables had no differences between the two populations: type of fish, past history of fish-mediated urticaria, anaphylaxis or contact urticaria, frequency of detection of thermostable, 50–66 or 66–90 allergens, and Anis 1 or 4 (Table 1). Detection of other allergens besides Ani s 1 or 4 was not found to be different between both populations. Total and specific IgE level differences were not significant between both groups. The detection of E/S allergens was found to be more prevalent in tolerant subjects (n = 41, 80%) when compared to intolerant subjects (n = 6, 46%; p = 0.029, two-tailed Fisher’s exact test). The most significant difference was the frequency of digestive symptoms (abdominal cramps, diarrhea, or vomits) reported by intolerant patients (n = 10, 77%) vs the cooked/frozen fish tolerant patients (n = 20, 39%; p = 0.027, two-tailed Fisher’s exact test). The severity of the clinical symptoms obtained from the clinical score was not different in the two populations.
Discussion
This study was performed to elucidate if patients with a clear history of sensitization to Anisakis tolerated the ingestion of properly cooked and frozen fish and to find out if the intolerance was mediated by detection of a particular allergen or any other characteristic. To do this, patients were studied by a multiblot system that analyzed simultaneously five different antigenic sources.
It is widely accepted that sensitized subjects tolerate the ingestion of dead larvae and that the symptoms experienced by the patients are due to an active invasion of living larvae. Sastre et al. have given up to 100 dead larvae to parasite-allergic patients without adverse reactions. In their opinion, this fact demonstrated that only live larvae constitute a hazard for these patients, and therefore, they suggest that eating frozen fish is the only necessary preventive measure for these subjects. Baeza et al. administered to their patients up to 479 ug of ES antigen without any adverse reaction, a fact that further supports this hypothesis. They suspect that gastric pepsin hydrolysis destroys these allergens.
But some authors described the opposite phenomenon. The existence of heat-resistant allergens, among them Ani s 1 and 4, has been described (Moneo et al. 2000, 2005; Shikamura et al. 2004). These allergens would, therefore, resist the cooking procedures. Only their hydrolysis by digestive enzymes would destroy their allergenicity. However, the most important information about the clinical relevance of these allergens can be obtained by monitoring the sensitized patients. Santaolalla recently described that 10.6% of the patients presented symptoms after ingestion of frozen fish, and in our experience, this value was 20%. We tried to find out without success if these intolerant patients had any special characteristics, such as the recognition of a particular allergen, differences in the total or specific IgE , severity of symptoms, etc. We only detected that these patients had more often digestive symptoms and detected less frequently excretory allergens when compared to the tolerant population. All these facts led us to believe that intolerance to frozen fish could be due to the ingestion of fish containing very high amounts of allergen. In fact, the amount of allergen present in food has never been measured.
The diagnosis of anisakidosis can only be performed by endoscopy or surgery. As in other infectious diseases, the presence of specific antibodies reflects the immune response generated after contact with the parasite. However, the use of a supernatant obtained from ground larvae has shown to be an unreliable antigenic source. Cross-reactivities with other parasites and even with apparently unrelated antigens have been described (Iglesias et al. 1996; Pascual et al. 1997; Johansson et al. 2001; Lozano et al. 2004; Bernardini et al. 2004). In other parasitoses, the use of purified native or even recombinant antigens has increased the sensitivity and specificity of the diagnostic assays. Bradley et al. 1993 reported that a mixture of not more than three recombinant proteins from Onchocerca reached 96% sensitivity. We tried, therefore, to characterize important allergens from Anisakis simplex. Anis s 1 and 4 are both clinically relevant allergens stored in the excretory gland of the L3 larvae. Both were prepurified from the crude parasite extract by a 50–66% differential ethanolic precipitation. This simple procedure allowed us to enrich and concentrate the antigen source that contained other allergens besides Ani s 1 and 4. According to our results, this fraction is the antigen of choice for use in immunoblotting assays and probably in other diagnostic methods.
On the other hand, the frequency of recognition of Ani s 1 and 4 did not differ significantly from our previous studies, but the use of this multiblot system demonstrated that the combined use of these two allergens had the same sensitivity (95%) as the conventional crude extract. Therefore, the use of these isolated proteins or, alternatively, the use of their recombinant counterparts could offer an important diagnostic alternative to the use of crude extracts. We are, therefore, at present trying to produce recombinant proteins to substitute the use of Ani s 1 and 4 by recombinant allergens that should overcome the intrinsic difficulty in the isolation and standardization of native parasite proteins.
References
Akbar A, Ghosh S (2005) Anisakiasis—a neglected diagnosis in the West. Dig Liver Dis 37:7–9
Audicana MT, Ansotegui IJ, Fernández de Corres L, Kennedy MW (2002) Anisakis simplex: dangerous—dead and alive? Trends Parasitol 18:20–25
Baeza ML, Rodriguez A, Matheu V, Rubio M, Tornero P, de Barrio M, Herrero T, Santaolalla M, Zubeldia JM (2004) Characterization of allergens secreted by Anisakis simplex parasite: clinical relevance in comparison with somatic allergens. Clin Exp Allergy 34:296–302
Bernardini R, Mistrello G, Novembre E, Roncarolo D, Zanotta S, Lombardi E, Cianferoni A, Pucci N, De Martino M, Vierucci A (2005) Cross-reactivity between IgE-binding proteins from Anisakis simplex and Dermatophagoides pteronyssinus. Int J Immunopathol Pharmacol. 18:671–675
Bradley JE, Trenholme KR, Gillespie AJ, Guderian R, Titanji V, Hong Y, McReynolds L (1993) A sensitive serodiagnostic test for onchocerciasis using a cocktail of recombinant antigens. Am J Trop Med Hyg 48:198–204
Buendia E (1997) Anisakis, aniakidosis, and allergy to Anisakis. Allergy 52:481–482
Daschner A, Alonso-Gomez A, Cabañas R, Suarez-de-Parga JM, Lopez-Serrano MC (2000) Gastroallergic anisakiasis: Borderline between food allergy and parasitic disease—clinical and allergologic evaluation of 20 patients with confirmed acute parasitism by Anisakis simplex. J Allergy Clin Immunol 105:178–181
del Pozo V, Arrieta I, Tunon T, Cortegano I, Gomez B, Cardaba B, Gallardo S, Rojo M, Renedo G, Palomino P, Tabar AI, Lahoz C (1999) Immunopathogenesis of human gastrointestinal infection by Anisakis simplex. J Allergy Clin Immunol 104:637–643
del Pozo MD, Moneo I, Fernandez de Corres L, Audicana MT, Muñoz D, Fernández E, Navarro JA, García M (1996) Laboratory determinations in Anisakis simplex allergy. J Allergy Clin Immunol 97:977–984
Garcia M, Moneo I, Audicana MT, del Pozo MD, Muñoz D, Fernandez E, Diez J, Etxenagusia MA, Ansotegui IJ (1997) The use of IgE immunoblotting as a diagnostic tool in Anisakis simplex allergy. J Allergy Clin Immunol 99:497–501
Iglesias R, Leiro J, Ubeira FM, Santamarina MT, Navarrete I, Sanmartin ML (1996) Antigenic cross-reactivity in mice between third-stage larvae of Anisakis simplex and other nematodes. Parasitol Res 82:378–381
Johansson E, Aponno M, Lundberg M, van Hage-Hamsten M (2001) Allergenic cross-reactivity between the nematode Anisakis simplex and the dustmites Acarus siro, Lepidoglyphus destructor, Tyrophagus putrescentiae, and Dermatophagoides pteronyssinus. Allergy 56:660–666
Lorenzo S, Iglesias R, Leiro J, Ubeira FM, Ansotegui I, Garcia M, Fernandez de Corres L (2000) Usefulness of currently available methods for the diagnosis of Anisakis simplex allergy. Allergy 55:627–633
Lozano MJ, Martin HL, Diaz SV, Mañas AI, Valero LA, Campos BM (2004) Cross-reactivity between antigens of Anisakis simplex s.l. and other ascarid nematodes. Parasite 11:219–223
Moneo I, Caballero ML, Gómez F, Ortega E, Alonso MJ (2000) Isolation and characterization of a major allergen from the fish parasite Anisakis simplex. J Allergy Clin Immunol 106:177–182
Moneo I, Caballero ML (2002) Las larvas de Anisakis simplex incubadas en medio acido diluido liberan alergenos que pueden tener utilidad en diagnóstico clínico. Alergol Inmunol Clin 17:201–207
Moneo I, Caballero Ml, Gonzalez-Muñoz M, Rodriguez-Mahillo AI, Rodriguez-Perez R, Silva A (2005) Isolation of a heat-resistant allergen from the fish parasite Anisakis simplex. Parasitol Res 96:285–289
Moreno-Ancillo A, Caballero T, Cabañas R, Contreras J, Martin-Barroso JA, Barranco P, Lopez-Serrano MC (1997) Allergic manifestations to Anisakis simplex parasitizing seafood. Ann Allergy Asthma Immunol 79:246–250
Pascual CY, Crespo JF, San Martin S, Ornia N, Ortega N, Caballero T, Munoz-Pereira M, Martin-Esteban M (1997) Cross-reactivity between IgE-binding proteins from Anisakis, German cockroach,and chironomids. Allergy 52:514–520
Rodero M, Cuellar C, Chivato T, Jimenez A, Mateos JM, Laguna R (2004) Evaluation by the skin prick test of Anisakis simplex antigen purified by affinity chromatography in patients clinically diagnosed with Anisakis sensitization. J Helminthol 78:159–165
Rodero M, Chivato T, Muro A, Cuellar C (2005) Enzyme-linked immunosorbent assay and Western blot antibody determination in sera from patients diagnosed with different helminthic infections with Anisakis simplex antigen purified by affinity chromatography. Mem Inst Oswaldo Cruz 100:293–301
Santaolalla M (2006) Estudio epidemiológico de las manifestaciones clínicas, los hallazgos de laboratorio y la eficacia del tratamiento en al alergia a Anisakis simplex. Doctoral thesis, Universidad del Pais Vasco
Sastre J, Lluch-Bernal M, Quirce S (2000) A double-blind placebo controlled oral challenge study with lyophilized larvae and antigen of the fish parasite Anisakis simplex. Allergy 55:560–564
Shikamura K, Miura H, Ikeda K, Ishizaki S, Nagashima Y, Shirai T, Kasuya S, Shiomi K (2004) Purification and molecular cloning of a major allergen from Anisakis simplex. Mol Biochem Parasitol 135:69–75
Acknowledgment
This study was supported by a grant of the Fondo de Investigacion Sanitaria, Ministry of Health. David Peck assisted in editing the English of this manuscript.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Moneo, I., Caballero, ML., Rodriguez-Perez, R. et al. Sensitization to the fish parasite Anisakis simplex: clinical and laboratory aspects. Parasitol Res 101, 1051–1055 (2007). https://doi.org/10.1007/s00436-007-0587-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00436-007-0587-7