
Abstract
Tungiasis, caused by the sand flea Tunga penetrans, is a health problem in many impoverished communities in Latin America, the Caribbean, and sub-Saharan Africa. Sand flea disease is associated with a broad spectrum of clinical and histological pathology. The factors determining the disease burden in endemic communities are not well understood, and severity of clinical pathology has never been assessed quantitatively. Thus, two severity scores were developed: one for acute disease and one for chronic sequels. These scores were evaluated in a cohort of 70 severely infested patients living in a shantytown in Fortaleza, a capital city in Northeast Brazil. Patients were examined during a period of 25 days and followed-up after a twice daily application of a plant-based repellent to prevent reinfestation. The severity score for acute disease symptoms significantly correlated with the infestation rate and the number of embedded fleas. It turned zero when reinfestation was prevented. The score for chronic disease also significantly correlated with the infestation rate. Tungiasis is associated with considerable acute and chronic morbidity. The degree of acute morbidity is directly related to the number of embedded sand fleas. When transmission is interrupted, the chronic morbidity reflects the infestation rates individuals have experienced in the past.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The penetration of the female sand flea Tunga penetrans into the upper layers of the skin with the subsequent development of a “neosome” is called tungiasis. The ectoparasitosis is confined to the tropics and subtropics and mainly affects impoverished populations living in urban squatter settlements, in villages in the rural hinterland, and in traditional fishing communities along the littoral (Ade-Serrano and Ejezie 1981; Carvalho et al. 2003; Chadee 1998; Feldmeier et al. 2003; Muehlen et al. 2003; Wilcke et al. 2002).
In these resource-poor settings, tungiasis causes a broad spectrum of clinical pathology, such as intense inflammation of toes and heels, formation of ulcers and fissures, abscesses and suppuration, as well as deformation and loss of nails (Bezerra 1994; Falkenstein 1877; Feldmeier et al. 2003; Gordon 1941; Valença et al. 1972). Tetanus, gangrene, and even autoamputation of digits are known sequels of tungiasis (Heukelbach et al. 2001; Joyeux and Sicé 1937; Litvoc et al. 1991; Schweizer 1952; Soria and Capri 1953). Death caused by septicemia and tetanus has been described recently in heavily infested individuals from Haiti (Joseph et al. 2006).
In the endemic area, constant reinfestation is the rule, and individuals may experience up to ten newly embedded sand fleas per day (Feldmeier et al. 2006a). Preliminary findings suggest that the accumulation of parasites at certain predilection sites is a risk factor for the development of severe disease (Feldmeier et al. 2003). The correlation between the infestation rate and the number of embedded fleas has been shown previously (Feldmeier et al. 2006a). To assess the association between the degree of infestation and morbidity, we developed severity scores for acute and chronic clinical pathology in patients with tungiasis. The score for acute disease significantly correlated with the number of embedded sand fleas and the infestation rate became zero when reinfestation was prevented by a repellent. The score for chronic pathology correlated also with the number of embedded fleas.
Materials and methods
Setting
The study was realized in five neighborhoods of the favela Vicente Pinzón, namely Luxou, Morro do Sandra’s, Favela das Placas, Morro da Vitória, and Novo Rumo, an agglomeration of urban squatter settlements in Fortaleza, Northeast Brazil.
Fortaleza is the capital of Ceará State and has about three million inhabitants. The social and economic characteristics of the favela have been described previously (Heukelbach et al. 2003). In brief, the community is characterized by poor housing, crowding, precarious hygienic conditions, and a high rate of illiteracy and unemployment. Few houses have a concrete floor. Stray dogs and cats as well as rats are seen everywhere. Crime, alcoholism, adolescent prostitution, and domestic violence are major social problems, and most inhabitants are desperately poor. The prevalence of parasitic skin diseases such as pediculosis, scabies, tungiasis, and cutaneous larva migrans is high (Heukelbach et al. 2004, 2005a,b).
Study cohort
As part of an intervention study on the efficacy of a plant-based repellent, 79 individuals were identified in the five neighborhoods who had at least ten embedded sand fleas or sand flea lesions manipulated with a perforating instrument at the recruitment examination. Individuals were eligible for the study, provided they planned to reside in their present domicile for the next 14 weeks. Individuals with deeply ulcerated lesions requiring antibiotic treatment were not eligible. As heavy infestations are predominantly seen in children 5 to 15 years (Muehlen et al. 2003), this age group was disproportionably highly represented in the cohort. Cohort members were visited twice a week for a period of 14 weeks (July 15 to October 21, 2003).
Baseline examinations were carried out during a period of 25 days followed by 10 weeks of intervention. Final assessment was done immediately after cessation of intervention. In total, each patient was visited 25 times.
Clinical examination
Tungiasis lesions were classified according to the Fortaleza Classification, a recently elaborated staging system (Eisele et al. 2003). The following findings were considered diagnostic for tungiasis:
-
Flea in statu penetrandi (stage I)
-
A dark and itching spot in the epidermis with a diameter of 1 to 2 mm, with or without local pain and itching (early lesion, stage II)
-
Lesions presenting as a white halo with a diameter of 3 to 10 mm with a central black dot (mature egg-producing flea, stage III)
-
A brownish–black circular crust with or without surrounding necrosis of the epidermis (dead parasite, stage IV)
Lesions altered through manipulation by the patient (such as partially or totally eliminated fleas leaving a characteristic crater-like sore in the skin) and suppurative lesions caused by the use of nonsterile perforating instruments such as needles and thorns, were documented as well.
The exact topographic localization of each lesion, its stage, and appearance were documented on a visual record sheet. Since more than 90% of sand flea lesions are found at the feet, ectopic localizations were not recorded (Heukelbach et al. 2002). The surface of each foot was divided into nine topographical areas, in which sand fleas mainly penetrate (Chadee 1998; Heukelbach et al. 2002; Muehlen et al. 2003): toe one to five, sole, lateral, and medial foot rim and heel, giving a total of 18 topographical areas for both feet.
The following symptoms and signs were noted: erythema, edema, pain, and warmness as signs of acute inflammation; pustule, abscess, and superficial suppuration as signs of superinfection; fissure and ulcer as skin defects related to tungiasis lesions or to manipulation of lesions reaching to the upper dermis; lesion in clusters, a dense accumulation of embedded sand fleas and therefore a sign of severe disease; nail deformation being alterations of the surface of the nails as can be seen in Figs. 1 and 2; nail loss caused by destruction of the nail bed; toe deformation due to chronic edema and/or constrictions caused by cicatrices; itching and sleep disturbance due to itching, pain upon pressure, pain while walking, or persistent pain as reported by the patient and difficulty walking as an altered gait observed by the examiner. These clinical alterations are characteristic findings in the different stages of the disease (Eisele et al. 2003; Feldmeier et al. 2003).

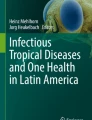
Right foot of a patient shows: edema and erythema at the first and fifth toe, clusters of embedded sand fleas at the first and fifth toe (SSAT of 1.5 points). There is deformation of the fifth toe, nail deformation at the first, second, and third toe, loss of nail at the fifth toe, hypertrophic nail rim at the first, second, and third toe (SSCT of 5.0 points)

Right foot of another patient: edema and erythema at first and third toe, honeycomb-like lesions at first toe (SSAT of 1.5 points). Score of chronic disease: nail deformation and toe deformation of the first toe due to chronic edema (SSCT of 1.5 points)
Infestation rate
The individual infestation rate was determined by dividing the number of newly embedded sand fleas diagnosed at an examination through the number of days passed since the last examination (Feldmeier et al. 2006a).
Severity score
Since the natural history of tungiasis is well known and can be divided into acute disease and chronic sequels (Eisele et al. 2003), two severity scores were elaborated: one for acute disease and one for chronic disease manifestations.
Symptoms and signs used to determine the severity score for acute tungiasis (SSAT) were divided into two categories as summarized in Table 1. The first category comprised variables that can be associated with individual sand flea lesions or with a group of lesions in a defined topographic area. According to the number of topographic areas affected, 0.5 to 3 points were assigned to these variables. The second type of variables included symptoms and signs which cannot be localized precisely or which affect the well-being of the patient in a more general manner. Itching was included in this category because, similar to other parasitic skin diseases such as scabies and pediculosis, the pruritus is not confined to the single lesions (Heukelbach and Feldmeier 2006; Ständer et al. 2006). According to the relative importance of the variables, 0.5 to 3 points were assigned to these characteristics. Thus, the SSAT has a maximum of 24 points, and due to its weighted composition of variables, reflects the degree of acute clinical pathology in a balanced manner. Examples of symptoms and signs of acute disease are shown in the Figs. 1, 2 and 5.
Signs and symptoms that contributed to the severity score for chronic tungiasis (SSCT) are outlined in Table 2. The following were considered as chronic signs of tungiasis: nail deformation being alterations of the nail surface as seen in Figs. 1 and 2 or the complete loss of the toe nail due to destruction of the nail bed by tungiasis lesions, hypertrophy of the nail rim typical for tungiasis, and deformation of toes due to chronic edema and/or constrictions caused by cicatrices as shown in Figs. 2 and 3. The chronic sequels, which are confined to the toes, such as deformation or loss of toenails, can take values of either 0.5 or 1 point for each toe. The SSCT can vary between 0 and 33 points.

Right foot of a patient: toe deformation due to cicatrice (SSCT of 1 point)
Intervention
After 25 days of base-line observation, an intervention was carried out to prevent reinfestation using a repellent based on coconut oil (Zanzarin®). The repellent was applied twice a day on the feet of the patients by a community health worker. Regular application of the repellent during a period of 4 weeks reduced the infestation rate by 90% (Feldmeier et al. 2006b).
Statistics
As the variables assessed were not normally distributed and variances varied considerably, the median and the interquartile ranges were used to indicate the average and dispersion of data. The Spearman rank correlation coefficient was calculated to assess the significance of the association between the severity scores and intensity of infestation and infestation rate, respectively. To compare data before and after intervention, the median of each variable was determined for each patient during the base line and the postintervention period. Significance of differences was assessed by the Wilcoxon matched pairs signed rank test.
Ethics
The study was approved by the Ethical Committee of the Federal University of Ceará State, Fortaleza, Brazil. Before the study, meetings with community health workers, community leaders, and members of the neighborhood associations were held, during which the objectives of the study were explained. Written consent was obtained from each study participant or, in the case of a minor, by his/her guardian. Participants could withdraw from the study at any time without any disadvantage.
Results
A total of 79 individuals from 34 families were enrolled in the study. Nine patients were excluded because they were not encountered at home for at least two consecutive examinations during follow-up. The demographic and parasitological characteristics of the remaining 70 patients are summarized in Table 3. Clinical pathology and the severity scores are detailed in Table 4.
There was an increasing tendency of the SSAT with age (Fig. 4). Whereas in younger children, relatively mild acute inflammation was accompanied by rather strong pain and difficulty walking, in children older than 5 years acute inflammation-related signs were much more impressive, but pain and difficulty walking seemed less severe. The correlation of age and the SSAT was not significant (p = 0.73).

Severity score for acute tungiasis (SSAT), stratified according to age. The SSAT is also divided up into symptoms (itching and pain) including difficulty walking (as it is mainly due to the pain) and signs (edema, erythema, ulcers, fissures, and lesion clusters)
When reinfestation was prevented by the daily application of the repellent during a period of 4 weeks, the infestation rate decreased by 93%. This was paralleled by a drastic reduction of the SSAT, but not of the SSCT (Table 5). The photographs of patient A.E., taken between August 11, 2003 (last base-line examination) and September 4, 2003 (after 24 days of repellent application; Figs. 5, 6, 7 and 8) show vividly that signs of chronic pathology remained present, whereas signs of acute inflammation almost completely disappeared.

Right foot of a patient: severe tunigasis in a 4-year-old boy at baseline. Edema and erythema toes one, two, three, and five, honeycomb-like lesion at the fifth toe, suppuration at the fifth, and fissure at the second toe (SSAT as far as it can be seen in the picture: 3.5 points). Hyperkeratosis, hypertrophic nail rim in toes one to three, toe deformation in toes one, three and five, and nail deformation in all toes (SSCT: 8 points)

The same child as in Fig. 5 after 7 days of application of a repellent. Edema and erythema on the first and fifth toe, honeycomb-like lesions at the fith toe (SSAT: 1.5 points). Hyperkeratosis, hypertrophic nail rim at toes one to three, nail deformation of all five toes, and toe deformation of toes one, three, and five (SSCT: 8 points)

The same patient as in Fig. 5 after 10 days of repellent application. Edema and erythema in the fifth toe (SSAT 0.5 points). Hyperkeratosis, hypertrophic nail rim in toes one to three, nail deformation in all five toes, and toe deformation of toes one, three, and five (SSCT: 8 points)

The same patient as in Fig. 5 after 24 days of repellent application (SSAT: 0 points). Hypertrophic nail rim in toes one to three, nail deformation in all five toes, and toe deformation of toes one, three, and five (SSCT: 7 points)
Both severity scores significantly correlated with the infestation rate at baseline (ρ = 0.44; p < 0.001 and ρ = 0.50; p < 0.001, respectively; Figs. 9 and 10). After 4 weeks of prevention of reinfestation, the SSCT still significantly correlated to the infestation rate at baseline (ρ = 0.35; p = 0.008). Clearly, no such correlation was observed for the SSAT (ρ = 0.06; p = 0.67).

Correlation between the severity score for acute tungiasis (SSAT) and the infestation rate (newly embedded sand fleas per individual per day) at baseline (ρ = 0.44; p < 0.001)

Correlation between the severity score for chronic tungiasis (SSCT) and the infestation rate at baseline (ρ = 0.50; p < 0.001)
Discussion
Tungiasis is associated with a broad spectrum of acute and chronic clinical morbidity. Especially the elder literature abounds with reports on debilitating conditions such as ulcers, abscesses, phlegmone, gangrene, lymphangitis, osteomyelitis, fasciitis, deep mycosis, ascending neuritis, and tetanus (Casala et al. 1954; Soria and Capri 1953; Tonge 1989). Also, more recent publications underline the extensive morbidity caused by embedded sand fleas, mostly being the consequence of superinfection with pathogenic microorganisms. From a tungiasis outbreak in Haiti, three cases of death were reported to be caused by tetanus and severe superinfection (Cardoso 1990; Feldmeier et al. 2002; Joseph et al. 2006; Linardi 1995, 1998).
A particular finding in our study are “honeycomb-like lesions”, clusters of up to 27 embedded sand fleas (unpublished observation) on a small space often located at the heel and accompanied by necrosis of the surrounding tissue (Cardoso 1990; Karsten 1865; Linardi 1998). It has been suggested that these clusters are related to the reproductive biology of T. penetrans enabling a single male to fertilize several embedded females within a short period of time (Geigy and Suter 1960). The pathophysiological mechanisms of other alterations are not understood, such as deformation and loss of toenails, hyper- and parakeratosis, as well as hypertrophy of the nail rim (Casala et al. 1954; Soria and Capri 1953). Autoamputation of digits has been observed in single cases and is thought to result from necrosis of bone and ligament tissue (Gordon 1941; Linardi 1998). Difficulty walking is the consequence of persistent pain and is known since the first descriptions of the disease (Cotes 1899; Gordon 1941; Jolly 1926; Linardi 1998).
Surprisingly, it has never been attempted to assess the clinical pathology of acute and chronic tungiasis in a systematic manner. We propose to use different scales for the assessment of acute disease and chronic sequels: the severity score for acute tungiasis (SSAT) and the severity score for chronic tungiasis (SSCT). The differentiation between acute and chronic pathology is justified, as clinical observations suggest that chronic signs persist for several months and even years also when transmission is interrupted.
Both scores are easy to apply in practice, since they are based on visual findings, history taking, and the observation of an altered gait. By weighting signs and symptoms, the scores mirrored the many clinical facets, which can be present in a single patient. Both, SSAT and SSCT, correlate significantly with the infestation rate and the number of embedded fleas. This means that morbidity is directly related to the parasite burden, thus confirming an assumption made previously (Feldmeier et al. 2003).
When the SSAT was divided in local signs (inflammation, ulcer, fissure, suppuration, abscess, and lesion cluster) and symptoms (pain, itching) and difficulty walking, it became obvious that young children, aged 1 to 5, tended to relate more pain to a similar or even a lower degree of clinical pathology than older individuals of 5 to 16 years (Fig. 4).
The disproportional infestation in children compared to other age groups has been described previously (Ade-Serrano and Ejezie 1981; Arene 1984; Carvalho et al. 2003; Wilcke et al. 2002). Behavior-related risk factors, such as a higher exposure, have served as an explanation for the higher prevalence in children as well as less keratinization of the skin during childhood (Wilcke et al. 2002). The stronger response in younger children (with pain, itching, and altered gait pattern) to sand flea infestation does not come surprisingly, as the relation between pain perception and age has been described by other authors (Robieux et al. 1992). Whether the increasing keratinization of the skin also plays a role is still to be determined.
The practical relevance of the severity score becomes evident, when reinfestation was prevented by a repellent as described elsewhere (Feldmeier et al. 2006b). Local inflammation and signs related to bacterial superinfection disappeared almost completely after 4 weeks of prophylaxis (Figs. 5, 6, 7 and 8), and pain ceased to exist. In the cohort, this was paralleled by the reduction of the SSAT to zero. As expected, deformation of nails and toes, the latter due to cicatrices and/or chronic edema, remained unchanged during the observation period and hyperkeratosis became even more obvious (Figs. 5, 6, 7 and 8). By consequence, the SSCT remained virtually unchanged as compared to the preintervention period. After intervention, the SSCT still correlated significantly with the infestation rate before intervention; consequently, this score could help to infer on transmission dynamics, which existed in a community in the past. However, for how long the SSCT can reflect infestation rates of the past, still has to be determined.
As coconut oil may have an insecticide property on embedded sand fleas, the reduction of the severity scores could partially have been caused by direct killing of embedded parasites if it is assumed that dead parasites cause less inflammation than viable ones. However, as location and stage of each lesion was documented at each examination, it became apparent that Zanzarin® reduced the infestation rate, i.e., that the observed effect was related to the repellent activity of the compound.
The use of scoring systems is widespread in all medical disciplines, especially when factors of different qualities (for example age, sex, body weight, and laboratory parameters) contribute to the classification into low-risk and high-risk patients. A score is helpful in diseases that vary in their occurrence from almost asymptomatic to severe manifestation, in order to standardize a procedure, which is adjusted to the individual patient. In parasitic diseases, a good example for a score is the multiorgan dysfunction score (MODS) used in patients with malaria to identify different levels of severity and herewith to predict the course of disease (Helbok et al. 2005). The elaborated scores SSAT and SSCT, similar to the MODS, are based mainly on clinical findings and thus easy to apply in resource-poor settings.
A clear limitation of the study was that the patients were only eligible when they had a minimum of ten embedded fleas at the recruitment examination. This led to a disproportional presence of patients with severe disease manifestations. Therefore it is assumable that the correlation coefficients for the infestation rate and the number of embedded fleas will be slightly different, if patients with a low parasite burden are included in the ingression analysis.
In summary, we have shown that clinical morbidity is associated with intensity of infestation. We propose the use of two severity scores to describe the extent of acute and chronic morbidity caused by tungiasis.
References
Ade-Serrano MA, Ejezie GC (1981) Prevalence of tungiasis in Oto-Ijanikin village, Badagry, Lagos State, Nigeria. Ann Trop Med Parasitol 75:471–472
Arene FO (1984) The prevalence of sand flea (Tunga penetrans) among primary and post-primary school pupils in Choba area of the Niger Delta. Public Health 98:282–283
Bezerra SM (1994) Tungiasis—an unusual case of severe infestation. Int J Dermatol 33:725
Cardoso AEC (1990) Tunguíase. An Bras Dermatol 65:29S–33S
Carvalho RW, Almeida AB, Barbosa-Silva SC, Amorim M, Ribeiro PC, Serra-Freire NM (2003) The patterns of tungiasis in Araruama township, state of Rio de Janeiro, Brazil. Mem Inst Oswaldo Cruz 98:31–36
Casala AM, Copello AR, Pensa VN (1954) Sarcopsiliasis (pique o nigua). Arch Argent Dermatol 4:245–254
Chadee DD (1998) Tungiasis among five communities in South-western Trinidad, West Indies. Ann Trop Med Parasitol 92:107–113
Cotes EC (1899) The jigger or chigoe pest. Ind Med Gaz 4:160–163
Eisele M, Heukelbach J, van Marck E, Mehlhorn H, Meckes O, Franck S, Feldmeier H (2003) Investigations on the biology, epidemiology, pathology and control of Tunga penetrans in Brazil: I. Natural history of tungiasis in man. Parasitol Res 90:87–99
Falkenstein (1877) Über das Verhalten der Haut in den Tropen, ihe Pflege und Krankheiten. Virchows Arch Pathol Anat 71:421–440
Feldmeier H, Heukelbach J, Eisele M, Sousa AQ, Barbosa LM, Carvalho CB (2002) Bacterial superinfection in human tungiasis. Trop Med Int Health 7:559–564
Feldmeier H, Eisele M, Sabóia Moura RC, Heukelbach J (2003) Severe tungiasis in underprivileged communities: case series from Brazil. Emerg Infect Dis 9:949–955
Feldmeier H, Kehr JD, Poggensee G, Heukelbach J (2006a) High exposure to Tunga penetrans (Linnaeus, 1758) correlates with intensity of infestation. Mem Inst Oswaldo Cruz 101:65–69
Feldmeier H, Kehr JD, Heukelbach J (2006b) A plant-based repellent protects against Tunga penetrans infestation and sand flea disease Acta Trop (in press)
Geigy R, Suter P (1960) Zur Copulation der Flöhe. Rev Suisse Zool 67:206–210
Gordon RM (1941) The jigger flea. Lancet 2:47–49
Helbok R, Dent W, Nacher M, Lackner P, Treeprasertsuk S, Krudsood S, Wilairatana S, Silachamroo U, Looareesuwan S, Schmutzhard E (2005) The use of the multi-organ-dysfunction score to discriminate different levels of severity in severe and complicated Plasmodium falciparum malaria. Am J Trop Med Hyg 72:150–154
Heukelbach J, Feldmeier H (2006) Scabies. Lancet 367:1767–1774
Heukelbach J, de Oliveira FA, Hesse G, Feldmeier H (2001) Tungiasis: a neglected health problem of poor communities. Trop Med Int Health 6:267–272
Heukelbach J, Wilcke T, Eisele M, Feldmeier H (2002) Ectopic localization of tungiasis. Am J Trop Med Hyg 67:214–216
Heukelbach J, van Haeff E, Rump B, Wilcke T, Moura RC, Feldmeier H (2003) Parasitic skin diseases: health care-seeking in a slum in north-east Brazil. Trop Med Int Health 8(4):368–373
Heukelbach J, Wilcke T, Feldmeier H (2004) Cutaneous larva migrans (creeping eruption) in an urban slum in Brazil. Int J Dermatol 43:511–515
Heukelbach J, Wilcke T, Harms G, Feldmeier H (2005a) Seasonal variation of tungiasis in an endemic community. Am J Trop Med Hyg 72(2):145–149
Heukelbach J, Wilcke T, Winter B, Feldmeier H (2005b) The epidemiology and morbidity of scabies and pediculosis in resource-poor communities in northeast Brazil. Br J Dermatol 153(1):150–156
Jolly GG (1926) An entomological episode of the East African Campaign. Ind Med Gaz 61:164–165
Joseph JK, Bazile J, Mutter J, Shin S, Ruddle A, Ivers L, Lyon E, Farmer P (2006) Tungiasis in rural Haiti: a community-based response. Trans R Soc Trop Med Hyg 100:970–974
Joyeux C, Sicé A (1937) Précis de médecine coloniale. Masson, Paris, p 441
Karsten H (1865) Beitrag zur Kenntniss des Rhynchoprion penetrans. Virchows Arch Pathol Anat 32:269–292
Linardi PM (1995) Siphonaptera. In: David Pereira Neves (Org) Parasitologia humana, 9th edn. Livraria Atheneus, Sao Paolo, pp 431–445
Linardi PM (1998) Tungíase: uma pulga diferente que provoca um problema persistente.Vet Prag 2:19–21
Litvoc J, Leite RM, Katz G (1991) Aspectos epidemiológicos do tétano no estado de São Paulo (Brasil). Rev Inst Med Trop São Paulo 33:477–484
Muehlen M, Heukelbach J, Wilcke T, Winter B, Mehlhorn H, Feldmeier H (2003) Investigations on the biology, epidemiology, pathology and control of Tunga penetrans in Brazil II. Prevalence, parasite load and topographic distribution of lesions in the population of a traditional fishing village. Parasitol Res 90:449–455
Robieux I, Eliopoulos C, Hwang P, Greenberg M, Blanchette V, Olivieri N, Klein N, Koren G (1992) Pain perception and effectiveness of the eutectic mixture of local anaesthetics in children undergoing venipuncture. Pediatr Res 32:520–523
Schweizer A (1952) A lórée de la foret vierge. Recits et réflexions d’un medicin en Afrique Equatoriale Francaise. Albin Michel, Paris
Soria MF, Capri JJ (1953) Tetanos y “piques”. La Prensa Med Arg 40:4–11
Ständer S, Streit M, Darsow U, Niemeier V, Vogelsang M, Ständer H, Gieler U, Gollnick H, Metze D, Weisshaar E (2006) Diagnostisches und therapeutisches Vorgehen bei chronischem Pruritus. J Dt Derm Ges 4:350
Tonge BL (1989) Tetanus from chigger flea sores. J Trop Pediatr 35:94
Valença ZO, Cardoso AEC, Cardoso AS (1972) Tunguiase generalizada: relato de dois casos tratados com thiabendazol. Dermatol Ib-Lat-Am 3:375–378
Wilcke T, Heukelbach J, Cesar Saboia MR, Regina SK-P, Feldmeier H (2002) High prevalence of tungiasis in a poor neighbourhood in Fortaleza, Northeast Brazil. Acta Trop 83:255–258
Acknowledgements
We are grateful to the Associação dos Moradores do Sandra`s for supporting the study and to Antonia Valéria Assunção, Vânia Santos de Andrade Souza and Maria de Fátima Cavalcante for skilful assistance. This study was supported by the DAAD-CAPES PROBRAL program no. 152/02. Judith Dorothea Kehr received a grant from the Studienstiftung des Deutschen Volkes, Bonn, Germany. Engelhard Arzneimittel, Niederdorfelden, Germany, provided the repellent Zanzarin® free of charge. The data are part of a medical thesis by Judith Dorothea Kehr.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kehr, J.D., Heukelbach, J., Mehlhorn, H. et al. Morbidity assessment in sand flea disease (tungiasis). Parasitol Res 100, 413–421 (2007). https://doi.org/10.1007/s00436-006-0348-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00436-006-0348-z