
Abstract
Purpose
Estrogen receptor β (ERβ) is the second identified receptor mediating the effects of estrogen on target tissues. The role of ERβ in cancer pathobiology is largely unknown, because specific antibodies have not been available until recently. Initial studies have shown that ERβ expression declines in breast, ovarian, prostatic, and colon carcinomas. Tamoxifen, a synthetic anti-estrogen compound that is a mixed agonist/antagonist of estrogen receptor α (ERα) and a pure antagonist of ERβ, has moderate beneficial effects in human astrocytic neoplasms. However, most published studies agree that glial tumors do not express ERα. The purpose of this study was to explore the expression of ERβ in astrocytic neoplasms.
Methods
ERβ expression was monitored immunohistochemically in 56 cases of astrocytomas of all grades (grade I–IV) and in adjacent non-neoplastic brain tissue.
Results
Moderate or strong nuclear immunopositivity was obtained in non-neoplastic astrocytes and in low-grade astrocytomas, whereas the majority of high-grade tumors were immunonegative or displayed weak immunoreactivity. The progressive decline in ERβ expression paralleled the increase in tumor grade.
Conclusions
In as much as ERβ is possibly the only ER expressed in astrocytes, its decreased expression may play an important role in astrocytic tumor initiation and in the potential response of glial neoplasms to tamoxifen.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Estrogen is a steroid hormone that exerts important biological actions in many tissues such as the male and female reproductive tract, the gastrointestinal tract, the mammary gland, and the skeletal, nervous, and immune system. Most of the effects of estrogen are mediated through one of two specific estrogen receptors (ERs), ERα and ERβ.
ERα was initially characterized and cloned in 1986, and for a decade it was believed to be the only receptor responsible for mediating the effects of estrogen on target tissues (Green et al. 1986; Greene et al. 1986). Research focused on ERα, which was then called ER, showed that it belongs to the steroid-thyroid-retinoid acid receptor superfamily, an evolutionary conserved nuclear receptor superfamily of ligand-inducible transcription factors. Estrogen binding to ERα results in translocation of the ligand-receptor complex to the nucleus, where it binds to specific DNA recognition sequences (estrogen response elements) within the promoter region of cognate genes and initiation of downstream response (Mangelsdorf et al. 1995).
This was the knowledge until 1996, when a second ER, ERβ, was sequenced initially from rodents and soon afterwards from human testis (Kuiper et al. 1996; Mosselman et al. 1996). This new discovery prompted reevaluation of the role of ERs during development and in tumorigenesis. ERβ binds estrogen with similar affinity to ERα and activates the expression of reporter genes bearing estrogen response elements in an estrogen-dependent manner. ERα and ERβ are highly homologous, although they are products of different genes. ERα is located on chromosome 6q25.1 and ERβ on chromosome 14q 22–24. Upon ligand binding ERs dimerize (ERα/ERα, ERβ/ERβ and ERα/ERβ). There is high homology on the DNA-binding and the ligand-binding domains (96% and 60% homology, respectively), whereas the A/B domain, hinge region, and F region are not well conserved. These differences are thought to be the basis for tissue-specific agonist/antagonist action of SERMS (selected estrogen receptor modulators) (Hall et al. 2001). The mechanism of action of the two ERs is not identical either. Besides the “classical” mode of action described above it has been shown that ERs can regulate target genes via “non-classical” routes, through promoter elements that bind heterologous transcription factors. Along these lines it has been shown that ERα enhances the activity of nuclear transcription factor AP-1 (activator protein-1), when complexed with 17β-estradiol, whereas ERβ does not. ERβ and ERα potentiate this pathway when complexed with antiestrogens, such as tamoxifen. Moreover, it has been shown that ERβ in the presence of estrogens suppresses transcriptional activation and hence modulates the proliferating effects of ERα (Pettersson et al. 2000, 2001). It is speculated that ERα and ERβ may have different roles in gene regulation and their relative levels within tissues may influence cellular responses to estrogens. The demonstration that ERβcx, one of the splice variant forms of ERβ, heterodimerizes and has dominant negative effects on ERα function, strengthens this hypothesis (Moore et al. 1998).
The role of ERα in several cancers, with the notable example of breast cancer, is fairly well characterized; however, the function of ERβ in cancer pathobiology is unclear. A major drawback has been the lack of available antibodies to detect ERβ expression in formalin-fixed paraffin-embedded material. Thus, most studies so far have focused on expression of ERβ mRNA. Recently, the availability of specific antibodies has enabled the first analyses on the expression of ERβ protein which have demonstrated that ERβ protein expression declines in breast, ovarian, prostatic, and colon carcinomas (Pujol et al. 1998; Chang and Prins 1999; Speirs 2002; Kostantinopoulos et al. 2003).
Gliomas are the most common primary tumors of the central nervous system. Among them, the most abundant are the intracranial neoplasms of astrocytic origin. According to the WHO grading system, astrocytic neoplasms can be classified into four grades, based upon four criteria, namely nuclear atypia, mitoses, microvascular proliferation, and necrosis (Louis et al. 2001). They range from the pilocytic astrocytoma (grade I), to low-grade or diffuse astrocytoma (grade II), anaplastic astrocytoma (grade III), and pleiomorphic glioblastoma (grade IV). Grade I neoplasms have very good prognosis, whereas pleiomorphic glioblastomas have a mean survival of less than 1 year, despite therapeutic efforts (Hofer and Hermmann 2001). The vast majority of these tumors are ERα-negative (Vaquero et al. 1983; Khalid et al. 1995; Carroll et al. 1995; Assimakopoulou et al. 1998). However, high concentrations of tamoxifen, a synthetic anti-estrogen compound, have been shown to reduce neoplastic glial cell proliferation and induce apoptosis (Iwasaki et al. 1995; Da Rocha et al. 1999). Several possible mechanisms have been proposed in an attempt to explain tamoxifen action on glioma cells, but the possible action through ERβ has not been addressed, since nothing is yet known about the expression of ERβ on astrocytic tumors (Couldwell et al. 1994; Zhang et al. 2000).
The present study aimed at investigating the expression of ERβ protein in astrocytic neoplasms of all grades, and correlating it with the degree of neoplastic cell differentiation.
Materials and Methods
Samples
We studied 56 astrocytic neoplasms including: three grade I (median age 14 years; two male, one female); nine grade II (median age 53.3 years; six male, three female); 11 astrocytomas grade III (median age 56.6 years; six male, five female); and 33 astrocytomas grade IV (median age 66.5 years; 14 male, 19 female).
Samples were surgically resected at the Department of Neurosurgery of the Ioannina University Hospital (Ioannina, Greece) from 2001 to2003. They were fixed in 10% (v/v) buffered formalin and embedded in paraffin. Serial, 5-μm sections were obtained for staining with hematoxylin and eosin and immunohistochemistry.
Immunohistochemistry and evaluation of ERβ expression
ERβ expression was detected by immunohistochemistry using the EnVision System (DAKO, Carpinteria, Calif., USA) and the monospecific polyclonal antibody to Estrogen Receptor β protein (Ab No. 385P, Biogenex, San Ramon, Calif., USA). The antibody is directed against a 17-meric sequence close to the COOH-terminus of the ERβ protein. Briefly, 5-μm-thick, histological sections were dewaxed in xylene, rehydrated through graded alcohols, immersed in 0.01 M citric buffer (pH 6.0), and microwaved twice for 5 min each. Subsequently, the sections were incubated with 0.3% H2O2 for 30 min to block endogenous peroxidase activity. The sections were then incubated for 1 h at RT with the primary antibody (dilution 1:500). Non-specific binding was blocked by incubating the sections for 30 min with Blocking Solution (DAKO). Detection was carried out using the EnVision System kit (DAKO) with diaminobenzidine as chromogen. Counterstaining was performed with hematoxylin Harris. Sections from normal prostate were used as controls. Negative controls were processed by omitting the primary antibody and substituting it with non-immune serum.
Immunostained sections were assessed by a semiquantitative method based on a four-level scale, as previously described (Kostantinopoulos et al. 2003). Briefly, immunoreactivity was graded as negative (−) if <10% of cells showed nuclear staining; weak (+) if there was weak nuclear staining intensity or 10–50% of cells showed nuclear staining; moderate (++) if there was moderate nuclear staining intensity and >50% of cells displayed nuclear staining; or strong (+++) if there was strong nuclear intensity and >50% of cells exhibited nuclear staining. The evaluation of immunohistochemistry was done independently by two pathologists. In rare cases where there was disagreement, both pathologists re-examined the slides together and agreed on the final percentage/intensity.
Statistical analysis
Descriptive statistics (percentages for grade and ERβ expression, mean and standard deviation for age) were used for available patient characteristics. The WHO grade groups were compared with chi-squared test for trend for ERβ expression and with ANOVA for age. The tumors were also split into “low grade” (WHO grade I or II) and “high grade” (WHO grade III and IV), and the two groups were compared with chi-squared test for trend for ERβ expression and t-test for age. Logistic and ordinal regression were also used to evaluate whether age could predict a patient having “high grade” tumor. Analyses were performed in SPSS 10.0 and StatXact-3. P-values are two-tailed.
Results
Astrocytic neoplasms
Immunohistochemical findings are summarized in Table 1 and depicted in Fig. 1a–d. ERβ expression levels were not statistically significantly different between male and female subjects and they are reported together.

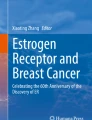
Evaluation of estrogen receptor beta (ERβ) expression in astrocytic neoplasms and non-neoplastic brain (immunostaining with DAB, original magnification ×40). a Strong nuclear immunoreactivity (+++) in grade I tumor (pilocytic astrocytoma); b Strong nuclear immunoreactivity (+++) in grade II tumor (diffuse or low-grade astrocytoma); c Moderate nuclear immunoreactivity (++) in grade III tumor (anaplastic astrocytoma); d Grade IV tumor (pleiomorphic glioblastoma) exhibiting no immunostaining (−). Note the immunopositive mitosis of a tumor cell; e Hyperplastic endothelial cells in a pleiomorphic glioblastoma displaying weak staining (+). Note the immunopositive mitosis of a tumor cell; f Non-neoplastic brain tissue exhibiting strong nuclear staining of glial cells (+++) and weak immunostaining of occasional neurons
Of the three grade I tumors, two (66.7%) showed strong and one (33.3%) showed moderate nuclear immunopositivity (Fig. 1a). Of the nine grade II tumors, eight (88.9%) showed strong and one (11.1%) showed moderate nuclear immunopositivity (Fig. 1b). Regarding grade III tumors (anaplastic glioma), only 1/11 (9%) displayed strong nuclear immunopositivity, four (36.5%) showed moderate, five (45.5%) weak, and one (9%) was negative (Fig. 1c). Of the grade IV neoplasms (pleiomorphic glioblastomas), the majority were immunonegative (45.5%) or exhibited weak immunoreactivity (30.3%), while only 18.2% showed moderate and 6% showed strong immunostaining (Fig. 1d). Interestingly, the observed mitoses of tumor cells were immunopositive (Fig. 1d–e). In anaplastic gliomas and pleiomorphic glioblastomas weak-moderate staining of the hyperplastic endothelial cells was observed (Fig. 1e).
There was a statistically significant association between WHO grade and ERβ immunoexpression (P<0.005). Statistically significant association was also observed between “low grade”/”high grade” tumors and ERβ expression (P<0.005).
Non-neoplastic brain tissue
ERβ immunostaining was observed in non-neoplastic brain tissue, in all cases where fragments were included in the biopsies and was exclusively nuclear. Strong nuclear staining was noted in glial cells as well as in occasional neurons (Fig. 1f). ERβ expression levels were not statistically significantly different between male and female subjects in any cell type.
Discussion
It is generally accepted that ERα is not significantly expressed in brain astrocytic tumors and normal brain tissue (Vaquero et al. 1983; Khalid et al. 1995; Carroll et al. 1995; Assimakopoulou et al. 1998; Chaidarun et al. 1998; Savaskan et al. 2001; Kruijver et al. 2002). The present retrospective immunohistochemical study demonstrated that ERβ is expressed in normal brain in both genders. In the initial report on identification and characterization of ERβ by Mosselman et al., Northern blot analysis revealed that ERβ was expressed in human thymus, spleen, ovary, and testis (Mosselman et al. 1996). No signal was detected in brain tissue, colon or prostate. Moreover, there was also a lack of signal in peripheral blood lymphocyte preparations, from which the initial PCR fragment was cloned. The authors speculate that the sensitivity of Northern blot analysis is insufficient to detect ERβ expression in some tissues.
There are only a few studies in the literature concerning the expression of ERβ in human brain tissues. It has been reported that ERβ is present in some neurons in the hippocampus and in astrocytes as well as in human pituitary tumors (and in some ERα is expressed as well) (Chaidarun et al. 1998; Savaskan et al. 2001; Kruijver et al. 2002).
We have shown that ERβ is expressed in glial neoplasms as well as in non-neoplastic astrocytes and, occasionally, in neurons. ERβ expression is significantly lower in high-grade astrocytic tumors compared to normal glial cells and there is a progressive decline in ERβ expression that parallels the increase in tumor grade. In tumor types such as breast, prostate, and ovarian, loss or reduction of ERβ expression is associated with the malignant phenotype, suggesting a potential tumor suppressing function for ERβ (Pujol et al. 1998; Chang et al. 1999; Speirs et al. 2002; Kostantinopoulos et al. 2003). Interestingly, in all other neoplasms ERα was expressed as well, leading to the hypothesis that alterations in the ratio of ERα:ERβ may govern tumor development. In breast, for example, it is postulated that ERβ protects from the mitogenic activity of estrogens by modulating the proliferative effects of ERα. Different mechanisms must be involved in astrocytic neoplasms since they generally do not express ERα. Identification of genes that are differentially regulated by ERβ is essential in elucidating its role in the development of glial neoplasms. The expression of ERβ in vascular cells that are also hyperplastic in high-grade glial tumors, indicates its possible involvement in paracrine signaling mechanisms associated with tumor growth.
Several studies have shown that astrocytic neoplasms harbor various genetic pathways implicated in their progression, but little is known about the events that are important for tumor initiation (Xu et al. 2001; Shiraishi et al. 2003). Grade I tumors, represented by pilocytic astrocytomas, are predominantly pediatric neoplasms with very good prognosis. So far, specific genetic alterations have been identified in pilocytic astrocytomas (Cheng et al. 2000; Weiss 2000; Roberts et al. 2001). Recent studies suggest epigenetic modifications (i.e., methylation) as an important early event in this subtype (Uhlmann et al. 2003). We have documented high ERβ expression in these neoplasms, comparable to non-neoplastic astrocytes. Grade IV neoplasms (pleiomorphic glioblastomas), are the most malignant gliomas and develop either de novo (primary glioblastoma) or from the progression of a more differentiated astrocytoma (secondary glioblastoma). In high-grade gliomas there is frequent amplification of the EGFR gene. Other known targets of genetic events in glioma tumorigenesis include the p53/MDM 2/p14 ARF pathway, the p16 INK4A pathway, and regions 19q, 10p, 10q (involving PTEN) with propensity to loss of heterozygosity (Shiraishi et al. 2003). Remarkably, it has been recently reported that deletions of chromosome 14q is a recurrent genetic event in the development of astrocytomas (Hu et al. 2002). This is the same region where the ERβ gene is located and thus one can surmise that it is involved in pathobiology of astrocytic neoplasms.
Tamoxifen is widely used to treat breast cancer and is also employed as an adjuvant treatment with modest efficacy in glial neoplasms (Chamberlain and Kormanik 1999; Puchner et al. 2001). The general mechanisms of anti-estrogen action have been studied extensively. Tamoxifen, a synthetic anti-estrogenic compound has been shown to antagonize the effects of estrogen for binding to ERα. In experimental models estrogen-dependent transcriptional activation by ERβ is inhibited by tamoxifen (Pettersson et al. 2000; Speirs 2002). Taking into account that gliomas are ERα -negative and since the expression of ERβ has not been addressed so far, the moderate beneficial effect of tamoxifen in glial neoplasms has been puzzling. It is believed that tamoxifen action in gliomas is independent of steroid-related pathways. In this vein, it has been shown that tamoxifen impairs protein kinase C activity, binds to calmodulin, and possesses antioxidant properties (Da Rocha et al. 1999). Zhang et al., using glioma and MCF7 breast cancer cell lines, have shown that the antitumor action of tamoxifen might be linked to modulation of tumor-associated calcium signaling (Zhang et al. 2000). Based on our findings we propose that tamoxifen, being a pure antagonist of ERβ, also acts, at least in part, through blocking the ERβ-related actions on neoplastic cells. If this is the case, then exploiting the experience with breast cancer, where it is firmly established that ER-positive tumors are more likely to respond to endocrine therapy, the identification of those gliomas that express ERβ would help identify the patients that could benefit from tamoxifen therapy.
In conclusion, we have shown that ERβ is highly expressed in non-neoplastic astrocytes and low-grade astrocytic neoplasms. Its expression declines in high-grade neoplasms, paralleling their loss of differentiation. Because ERβ is possibly the only ER expressed in astrocytes, its deregulation may be of crucial importance to astrocytic tumor progression and to potential response of glial tumors to tamoxifen.
References
Assimakopoulou M, Sotiropoulou-Bonikou G, Maraziotis T, Varakis J (1998) Does sex steroid receptor status have any prognostic or predictive significance in brain astrocytic tumors? Clin Neuropathol 17:27–34
Carroll RS, Zhang J, Dashnr K, Sar M, Black PM (1995) Steroid hormone receptors in astrocytic neoplasms. Neurosurgery 37:496–503
Chaidarun SS, Swearingen B, Alexander JM (1998) Differential expression of estrogen receptor beta (ER beta) in human pituitary tumors: functional interactions with ER alpha and a tumor-specific splice variant. J Clin Endocrinol Metab 83:3308–3315
Chamberlain MC, Kormanik PA (1999) Salvage chemotherapy with tamoxifen for recurrent anaplastic astrocytomas. Arch Neurol 56:703–708
Chang WY, Prins GS (1999) Estrogen receptor-β: implications for the prostate gland. Prostate 40:115–124
Cheng Y, Pang JC, Ng HK, Ding M, Zhang SF, Zheng J, Liu DG, Poon WS (2000) Pilocytic astrocytomas do not show most of the genetic changes commonly seen in diffuse astrocytomas. Histopathol 37:437–444
Couldwell WT, Hinton DR, He S, Chen TC, Sebat I, Weiss MH, Law RE (1994) Protein kinase C inhibitors induce apoptosis in human malignant glioma cell lines. FEBS Lett 345:43–46
Da Rocha AB, Mans DR, Bernard EA, Ruschel C, Logallo AF, Wetmore LA, Leyva A, Schwartsmann G (1999) Tamoxifen inhibits particulate-associated protein kinase C activity, and sensitises cultured human glioblastoma cells not to etoposide but to gamma-radiation and BCNU. Eur J Cancer 35:833–839
Green S, Walter P, Kumar V, Krust A, Bornert JM, Argos P, Chambon P (1986) Human estrogen receptor cDNA: sequence, expression and homology to v-erb-A. Nature 320:134–139
Greene GL, Gilna P, Waterfield M, Baker A, Hort Y, Shine J (1986) Sequence and expression of human estrogen complementary DNA. Science 231:1150–1154
Hall JM, Couse JF, Corah KS (2001) The multifaceted mechanisms of estradiol and estrogen receptor signaling. J Biol Chem 276:36869–36872
Hofer S, Herrmann R (2001) Chemotherapy for malignant brain tumors of astrocytic and oligodendroglial lineage. J Cancer Res Clin Oncol 127:91–95
Hu J, Pang JC, Tong CY, Lau B, Yin XL, Poon WS, Jiang CC, Zhou LF, Ng HK (2002) High resolution genome-wide allelotype analysis identifies loss of chromosome 14q as a recurrent genetic alteration in astrocytic tumors. Br J Cancer 87:218–224
Iwasaki K, Toms SA, Barnett GH, Estes ML, Gupta MK, Barna BP (1995) Inhibitory effects of tamoxifen and tumor necrosis factor alpha on human glioblastoma cells. Cancer Immunol Immunother 40:228–234
Khalid H, Yaunaga A, Kishikawa M, Shibata S (1995) Immunohistochemical expression of the estrogen receptor-related antigen (ER-D5) in human intracranial tumors. Cancer 75:2571–2580
Kostantinopoulos PA, Kominea A, Vandoros G, Sykiotis GP, Andrikopoulos P, Varakis J, Sotiropoulou-Bonikou G, Papavassiliou AG (2003) Oestrogen receptor beta (ERβ) is abundantly expressed in normal colonic mucosa, but declines in colon adenocarcinoma paralleling the tumors dedifferentiation. Eur J Cancer 39:1251–12458
Kruijver FP, Balesar R, Espila AM, Unmehopa UA, Swaab DF (2002) Estrogen receptor-alpha distribution in human hypothalamus in relation to sex and endocrine status. J Comp Neurol 454:115–139
Kuiper GG, Enmark E, Pelto-Huikko M, Nilsson S, Gustafsson JA (1996) Cloning of a novel receptor expressed in rat prostate and ovary. Proc Natl Acad Aci 93:5925–5990
Louis DN, Holland EC, Cairncross JG (2001) Glioma classification: a molecular reappraisal. Am J Pathol 159:779–786
Mangelsdorf DJ, Thummel C, Beato M, Herrlich P, Schutz G, Umesono K, Blumberg B, Kastner P, Mark M, Chambon P (1995) The nuclear receptor supefamily: the second decade. Cell 83:835–839
Moore JT, McKee DD, Sletz-Kesler K, Moore LB, Jones SA, Horne SA, Su JL, Kliener SA, Lehmann JM, Willson TM (1998) Cloning and characterization of human estrogen receptor β isoforms. Biochem Biophys Res Commun 247:75–78
Mosselman S, Polman J, Dijkema R (1996) ER-β: identification and characterization of a novel human estrogen receptor. FEBS Lett 392:49–53
Pettersson K, Gustafsson JA (2000) Estrogen receptor beta acts as a dominant regulator of estrogen signalling. Oncogene 19:4970–4978
Pettersson K, Gustafsson JA (2001) Role of estrogen receptor beta in estrogen action. Annu Rev Physiol 63:165–192
Puchner MJA, Giese A, Zapf S, Grebe M, Westphal M (2001) Tamoxifen sensitivity-testing of glioblastomas: comparison of in vitro and in vivo results. Acta Neurochir (Wien) 143:563–573
Pujol P, Rey JM, Nirde P, Roger P, Gastaldi M, Laffargue F, Rochefort H, Mandelonde T (1998) Differential expression of estrogen receptor-α and –β messanger RNAs as a potential marker of ovarian carcinogenesis. Cancer Res 58:5367–5373
Roberts P, Chumas PD, Picton S, Bridges L, Livingstone JH, Sheridan E (2001) A review of the cytogenetics of 58 pediatric brain tumors. Cancer Genet Cytogenet 131:1-12
Savaskan E, Olivieri G, Meirer F, Ravid R, Muller-Spahn F (2001) Hippocampal estrogen beta-receptor immunoreactivity is increased in Alzheimer’s disease. Brain Res 908:113–119
Shiraishi T, Tabuchi K (2003) Genetic alterations of human brain tumors as molecular prognostic factors. Neuropathology 23:95–108
Speirs V (2002) Oestrogen receptor β in breast cancer: good, bad or still too early to tell? J Pathol 197:143–147
Uhlmann K, Rohde K, Zeller C, Szymes J, Vogel S, Marczinek K, Thiel G, Nurnberg P, Laird PW (2003) Distinct methylation profiles of glioma subtypes. Int J Cancer 106:52–59
Vaquero J, Marcos ML, Martinez R, Bravo G (1983) Estrogen and progesterone-receptor proteins in intracranial tumors. Surg Neurol 19:11–13
Weiss WA (2000) Genetics of brain tumors. Curr Opin Pediatr 12:543–548
Xu S, Zhu X, Zhang S, Yin S, Zhou L, Chen C, Gu J (2001) Over-expression of 1,4-galactosyltransferase I, II, and V in human astrocytoma. J Cancer Res Clin Oncol 127:502–506
Zhang W, Couldwell WT, Song H, Takano T, Kin J, Nedergaard M (2000) Tamoxifen-induced enhancement of calcium signaling in glioma and MCF-7 breast cancer cells. Cancer Res 60:5395–5400
Acknowledgements
We thank Dr Evangelia Ntzani for aid in the statistical analysis and A. Christodoulou for excellent technical assistance.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Batistatou, A., Stefanou, D., Goussia, A. et al. Estrogen receptor beta (ERβ) is expressed in brain astrocytic tumors and declines with dedifferentiation of the neoplasm. J Cancer Res Clin Oncol 130, 405–410 (2004). https://doi.org/10.1007/s00432-004-0548-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00432-004-0548-9