
Abstract
The present study assesses the impact of beverage consumption pattern on diet quality and anthropometric proxy measures for abdominal adiposity in Spanish adolescents. Data were obtained from a representative national sample of 1,149 Spanish adolescents aged 10–18 years. Height, weight, and waist circumferences were measured. Dietary assessment was performed with a 24-h recall. Beverage patterns were identified by cluster analysis. Adherence to the Mediterranean diet was measured by the KIDMED index. Three beverage clusters were identified for boys—“whole milk” (62.5 %), “low-fat milk” (17.5 %) and “soft drinks” (20.1 %)—and for girls—“whole milk” (57.8 %), “low-fat milk” (20.8 %) and juice (21.4 %), accounting for 8.3, 9.6, 13.9, 8.6, 11.5 and 12.9 % of total energy intake, respectively. Each unit of increase in the KIDMED index was associated with a 14.0 % higher (p = 0.004) and 11.0 % lower (p = 0.048) probability of membership in the “low-fat milk” and “soft drinks” cluster in girls and boys, respectively, compared with the “whole milk” cluster. Boys in the “soft drinks” cluster had a higher risk of 1-unit increase in BMI z score (29.0 %, p = 0.040), 1-cm increase in waist circumference regressed on height and age (3.0 %, p = 0.027) and 0.1-unit increase in waist/height ratio (21.4 %, p = 0.031) compared with the “whole milk” cluster. Conclusion: A caloric beverage pattern dominated by intake of “soft drinks” is related to general and abdominal adiposity and diet quality in Spanish male adolescents.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Obesity is one of the most important risk factors for all disabilities and premature death in the adult population of Western countries [48]. Excessive abdominal fat accumulation has been associated with a high cardiometabolic risk profile in adults [9, 22] and, alarmingly, with an unhealthy cardiometabolic profile in children and adolescents [30, 40], setting the stage for the adult profile. Therefore, it is paramount to identify variables associated with abdominal adiposity in youth if we intend to stop the overall population obesity epidemic in Western countries.
Adequate dietary intake is of paramount concern for adolescents’ health and development. Furthermore, poor food choices in early life can affect dietary habits in adulthood [7]. Consumption of caloric beverages constitutes an important portion of total energy intake among children and adolescents; of particular concern is the replacement of micronutrient-dense beverages such as milk with low nutrient density choices, such as sugar-sweetened beverages (SSB) [10, 46]. It has been hypothesised that reduced consumption of these beverages is a key obesity prevention strategy in this population [6] and can have an impact on overall diet quality [45]. For example, increased carbonated soda consumption decreased the odds of achieving recommended intakes of vitamin A and magnesium in a population aged 12–17 years [1]. Frary and colleagues [14] reported lower intakes of calcium, fibre and fruit with increasing soft drinks consumption in adolescents, and a recent study associated high soft drinks consumption with high intakes of pizza, burgers, fried potatoes and savoury snacks in boys and girls aged 12–18 years [26]. However, further research is need to establish the impact of caloric beverage patterns on diet quality [8, 19, 23, 31] and their association with surrogate markers of abdominal adiposity in adolescents [29].
The aim of the present study was to identify caloric beverage consumption patterns and their association with overall diet quality and adiposity among Spanish adolescents.
Methods
Study population
The enKid study on nutritional status and food habits of Spanish children and young people, conducted between 1998 and 2000, was a cross-sectional survey of the Spanish population aged 2–24 years (n = 3,534, 1,629 boys and 1,905 girls), selected by multistage random sampling procedures based on an official population census. The theoretical sample size was set at 5,500 individuals, taking into account an anticipated 70 % participation rate, which would result in a sample of approximately 3,850 individuals. The present study included the subset of all participants aged 10–18 years (n = 1,149; mean age = 14.2 ± 2.2 years). The study protocol was approved by the ethics committee of the Spanish Society of Community Nutrition. Parental written informed consent was obtained for each participant younger than 18 years.
Dietary assessment
Dietary intake information based on a single 24-h recall was collected at each participant’s home, using household measures to estimate portion sizes [36]. Children aged 10–13 answered the interviews with support from the caretaker responsible for their nutrition; older children answered independently. Additional information on food descriptions and portion sizes was gathered as required on site. Day of collection was randomly assigned, including weekends and non-school days and covering all seasons of the year (May 1998–April 2000). Individual caloric beverages were aggregated in three groups according to their energy value and nutrient properties: (a) 100 % juices, including commercial and natural fruit and vegetable juices; (b) low-fat milk, including skim, and semi-fat (2 %) milk; (c) whole-fat milk (4 % fat); and (d) soft drinks, including carbonated and non-carbonated SSB. Intake was expressed as millilitre consumed per day. Less than 1 % of the study population reported vegetable juice consumption. Therefore, we combined vegetable and fruit juice consumption. The nutrient calculations used for the study combined a Spanish database [25] with information from French [12] food composition tables.
The KIDMED index was derived on the basis of a 16-item questionnaire administered separately from the 24-h recalls as part of the enKID survey [37]. KIDMED was created to estimate adherence to the Mediterranean diet in children and young adults, based on the principles that sustain Mediterranean dietary patterns and those that undermine it [37]. Items denoting lower adherence were assigned a value of −1 (4 items), and those related to higher adherence were scored +1 (12 items). Scores range from −4 to 12, with higher scores indicating greater adherence to the Mediterranean diet. The KIDMED index shows reasonable construct validity [35].
Anthropometric measurements
Anthropometric measurements were assessed for each individual following standard protocols. Body weight, height, and waist circumferences were measured on the day of the interview, with the subject in underwear without shoes, using an electronic scale (to the nearest 100 g), a portable Kawe stadiometer (to the nearest 1 mm), and a Hoechst metric tape (to the nearest 1 mm). Using a flexible non-stretch tape measure, waist circumference was measured by trained interviewers in the narrowest zone between the lower costal rib and iliac crest, in the supine decubitus and horizontal positions.
Energy underreporting
Basel metabolic rate (BMR) was estimated with Schofield’s equations based on sex, age, weight and height [33]. Implausible reporters of energy intake were identified by replacing Goldberg’s single cut-off [15] with age- and sex-specific cut-offs for children. The cut-off values are the 95 % confidence limits of the agreement between physical activity level (PAL) and the ratio of energy intake to BMR. The following formula was used:
Where
Intra-individual variations of energy intake (CV 2wEI ) and BMR (CV 2wBMR ) and inter-individual variation in physical activity level (CV 2wtP ) were calculated using sex- and age-specific reference values for adolescents [5, 27, 44]. The single Goldberg PAL of 1.55 was replaced by sex- and age-dependent PAL for adolescents. We estimated dietary intake by one 24-h recall and set the number of days (d) to 1.
Other measurements
Data on physical activity and maternal education (primary school or beyond) were reported by participants responding to an interviewer-administered questionnaire. The physical activity questionnaire included 14 questions on type, frequency and time spent doing physical activity at school and outside school. Primary education was defined as completing primary school (ages 6–14 years).
Puberty status was not measured in the EnKid study. It has been shown that height is differentially associated with surrogate measures of adiposity according to pubertal status [21]. Therefore, we presented data on waist circumference residuals regressed on age and height.
Statistical analysis
K-means clustering was performed to identify caloric beverage patterns, and individuals were classified into mutually independent groups or clusters. The beverage groups were standardised (z values) before clustering to ensure an equal influence on the cluster procedure. The number of clusters to be retained from analysis was predefined. Solutions ranging from two to six clusters were run, and the final three-cluster solution was selected because it most clearly identified distinct and meaningful caloric beverage patterns while maintaining a reasonable sample size of boys and girls. This solution was confirmed by the tree diagram resulting from Ward’s method of cluster analysis. Finally, discriminant function analysis was carried out to examine the stability and classification ability of the three-cluster solution in each sex.
One-way ANOVA compared continuous variables between cluster memberships. Tests of proportions used the chi-square method.
Multinomial logistic regression analysis was run to determine the association between cluster membership and waist circumference (WC), regressed for age and height (WCage,height), waist/height ratio (WHtR) and adherence to the Mediterranean diet. The multinomial logistic regression coefficients can be interpreted as changes in the membership probability of the analysed cluster versus the reference category.
Results
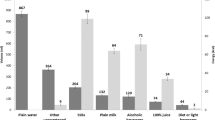
In this population, 9.8 % of total energy (210 kcal) was derived from non-alcoholic caloric beverages. Three caloric beverage clusters were identified for boys and girls according to their main beverage consumption characteristics: “whole-fat milk” (4 % fat), “low-fat milk” (skim and semi-fat milk) and “soft drinks” in boys and “whole-fat milk”, “low-fat milk” and “juice” in girls. In the whole-fat milk cluster, the mean intake of that beverage was 301 and 244 ml/day in boys and girls, respectively. In the low-fat milk cluster, similar intakes were reported by boys (357 ml/day) and girls (321 ml/day). Clusters of high consumption of soft drinks and juices were sex specific. Boys in the soft drinks cluster had a daily mean consumption of 530 ml of soft drinks, whereas girls in the juice cluster reported an intake of 248 ml of juices per day.
Discrimination function analysis revealed a small Wilks’ lambda (boys, 0.113, p < 0.001; girls, 0.067, p < 0.001), indicating only 11.3 and 6.7 % of the variance in the discriminant scores is not explained by differences between clusters for boys and girls, respectively. Cross-classification of individuals according to their original cluster classification and that obtained from the discriminant analysis showed that 99.5 % of original cluster cases were correctly classified in boys and 98.6 % in girls.
Excluding energy underreporters from cluster analysis had no effect on type of cluster formation. We found the same meaningful clusters with similar prevalence in both boys and girls. Furthermore, associations between clusters and anthropometric variables and diet quality were in the same direction and magnitude. Therefore, we present data of the whole sample size of Spanish adolescents, adjusting for energy underreporting when appropriate.
The “whole-fat milk” cluster was the most prevalent in both boys (62.5 %) and girls (57.8 %), followed by “soft drinks” (21.1 %) and “low-fat milk” (17.5 %) in boys and by the “juice” cluster (21.4 %) and “low-fat milk” (20.8 %) in girls. Members of the “soft drinks” cluster were older and had the lowest proportion of energy underreporters (Table 1).
The “soft drinks” and “juice” clusters provide the highest amount of energy from beverages in boys (14.0 %) and girls (12.9 %), respectively (Table 2). Members of the “soft drinks” cluster showed the highest total energy consumption. High intakes of carbohydrates and low intakes of proteins were found among the members of the “soft drinks” and “juice” clusters, respectively. The “soft drinks” cluster was further characterised by low intakes of dietary fibre, vitamin C, folic acid and magnesium (Table 2).
We fitted a multivariate multinomial logistic regression model, adjusted to determine the relationship between cluster membership and adherence to the Mediterranean diet (Table 3). An increase of 1 unit in the KIDMED index was associated with 14 % higher (p = 0.004) and 11 % lower (p = 0.048) odds of belonging to the “low-fat milk” and “soft drinks” cluster in girls and boys, respectively, compared with the “whole-fat milk” cluster.
Multinomial logistic regression analysis adjusted for age, energy underreporting, mother’s educational level, physical activity and energy intake revealed a weak positive association between “soft drinks” membership and BMI z scores, WCage,height and WHtR, compared with the “whole-milk” cluster (Table 4).
Discussion
The observed relationship between certain beverage drinking patterns and low diet quality in children and adolescents is of concern for two main reasons. First, healthy dietary behaviours in youth are paramount for physical and mental development, and second, unhealthy early dietary patterns can set the stage for high metabolic risk in adulthood [7, 43]. In the present study, cluster analysis identified three non-overlapping patterns of caloric beverage consumption in Spanish boys and girls. A whole- and low-fat milk cluster was identified in both groups; a “soft drinks” cluster was characteristic for boys and a “juice” cluster for girls. Adherence to the Mediterranean diet was associated with a 14 % higher odds ratio of membership in the “low-fat milk” cluster in girls, compared to the “whole-fat milk” cluster. Among boys, this dietary pattern was associated with an 11 % lower odds ratio of membership in the “soft drinks” cluster; furthermore, boys in the “soft drinks” cluster had an increased risk of higher BMI z scores, WCage,height and WHtR in comparison with the “whole milk” cluster. The effect size of these associations was modest.
A limitation of the present study is its cross-sectional design, which precludes drawing causal relationships. Furthermore, 24-h recalls—and particularly a single day’s recall—have inherent limitations in the individual assessment of dietary intake due to daily variations in food intake [2, 4] and thus did not necessarily reflect habitual intakes. Additionally, day-to-day variation results in random (non-differential) errors that may have weakened the association between caloric beverage consumption and adiposity. A further limitation is that there is no standardised definition of underreporting in children and adolescents. Including objective measurements for physical activity would have improved the estimation of energy underreporters. Furthermore, it was not feasible to determine the validity of energy underreporting estimation by comparison of the results with a biomarker such as doubly labelled water. Although the 68 % participation rate of the enKid study can be considered appropriate, we cannot rule out a possible selection bias in our study population due to the parental consent requirement for children younger than 18 years.
This study also has several important strengths, including a nationwide population-based sample with standardised anthropometric measurements available.
The energy derived from non-alcoholic caloric beverages (juices, soft drinks and low-fat and whole-fat milk) in our study was comparable with that of a previous report [10]. However, our analysis shows great variation between clusters in the proportion of energy consumption from beverages. In the “soft drinks” cluster, energy from beverages constitutes a considerable amount of the total energy intake, with soft drinks as the main contributor. In contrast, beverages provide only a small proportion of total energy in the “low-fat milk” cluster. These findings were independent of age and energy underreporting.
Soft drinks have a low nutrient density and thus are prone to dilute the micronutrient content of the diet. In this study, the “soft drinks” cluster had the most unfavourable nutrient intake profile compared to the “whole-fat milk” and “low-fat milk” clusters in boys. This finding is in line with reports showing that soft drinks consumption is associated with lower intakes of nutrients such as dietary fibre and calcium among children and youth [1, 14, 49].
There is scarce evidence about the impact of beverage consumption patterns on overall diet quality [8, 19, 23, 31]. Duffey and Popkin [11] reported that adult members of an unhealthy beverage cluster had a greater probability of also being members of an unhealthy eating cluster. Furthermore, soft drinks consumption was negatively associated with diet quality, as characterised by the healthy eating index (HEI), in American [19] and Spanish children [31]. A German study that chose the nutritional quality index (NQI) as an indicator for diet quality reported similar results [23]. In the present study, we estimated diet quality with the KIDMED index, which was developed to estimate adherence to the Mediterranean diet among Spanish youth [37]. High adherence to this index has been associated with healthy nutrient and food intake profile in various adolescent populations [13, 18, 24]. In our data, an increase of 1 unit in the KIDMED index was associated with a 14 % higher and 11 % lower odds of membership in the “low-fat milk” and “soft drinks” clusters in girls and boys, respectively, compared to the “whole-milk” cluster. Although further research is required, all of these different a priori constructs of diet quality—the HEI, the NQI, and the KIDMED index—show a negative association with unhealthy patterns of beverage consumption.
Low diet quality has been related to higher WC in youth [35]. The loss of healthy eating habits may partially account for the trends toward increasing WC in this segment of the Spanish population. This is of particular concern because abdominal fat accumulation has a strong independent impact on the cardiometabolic profile in children and adolescents [20, 40], as well as in adults [9, 12]. In our study, membership in the “soft drinks” cluster was associated with a greater risk of higher WCage,height and WHtR (two surrogate markers for abdominal adiposity), compared to being a member of the “whole-fat milk” cluster, independent of potential confounders. Energy intake is directly associated with energy density in adults and children [32]. It has been hypothesised that high energy density diets lead to passive overconsumption and thus increase the risk of weight gain [16]. Recently, we have shown that a high energy density diet is directly related with abdominal adiposity in Spanish youth [34]. In the present study, a high energy density diet was characteristic for the membership of the soft drinks cluster. However, controlling for energy density did not attenuate the risk of increased abdominal fat distribution of members of the soft drinks cluster compared with the whole-fat milk cluster. In other words, the association between increased abdominal adiposity and membership in the soft drinks cluster is independent of energy density.
It is of interest to note that the “soft drinks” cluster was sex specific. A possible explanation for this finding might be that boys are more vulnerable to soft drinks advertisements. In a recent study, intake of soft drinks was nearly twice as high among European boys, compared to girls [10].
Sugar-sweetened beverage consumption has been associated in some [39, 41, 47] but not all [17, 28] adiposity studies in children and youth. One explanation for the positive association of soft drinks consumption and adiposity is inadequate energy compensation after soft drinks consumption, leading to an increase in total energy intake [3]. Alternatively, fructose has been proposed as the mechanistic link between sugar-sweetened beverages and obesity [38]. However, evidence is inconsistent regarding the metabolic effects of fructose on weight gain [42]. Compared with reported results from the USA [48], the proportion of soft drinks consumers and the amount of soft drinks consumed in our study can be considered low. The observed trend of increasing SSB consumption generates concern because the effect size also can be expected to increase.
Remarkable differences in caloric beverage drinking patterns were identified in Spanish adolescent girls and boys, although a whole-fat milk cluster was the most prevalent in both groups. The soft drinks cluster was associated with somewhat lower diet quality and a slightly higher risk of increased abdominal fat compared with the “whole-fat milk” cluster in male adolescents. Girls in the low fat-milk cluster reported a somewhat higher diet quality compared with their peers of the whole-fat milk cluster. Long-term prospective studies are needed to get better insight about the impact of caloric beverage consumption on diet quality and adiposity in adolescents.
Abbreviations
- BMI:
-
Body mass index
- BMR:
-
Basal metabolic rate
- PAL:
-
Physical activity level
- SSB:
-
Sugar-sweetened beverages
- WC:
-
Waist circumference
- WHtR:
-
Waist/height ratio
References
Ballew C, Kuester S, Gillespie C (2000) Beverage choices affect adequacy of children’s nutrient intakes. Arch Pediatr Adolesc Med 154:1148–1152
Beaton GH, Burema J, Ritenbaugh C (1997) Errors in the interpretation of dietary assessments. Am J Clin Nutr 65:1100S–1107S
Bertenshaw EJ, Lluch A, Yeomans MR (2008) Satiating effects of protein but not carbohydrate consumed in a between-meal beverage context. Physiol Behav 93:427–436
Bingham SA (1991) Limitations of the various methods for collecting dietary intake data. Ann Nutr Metab 35:117–127
Black AE (2000) Critical evaluation of energy intake using the Goldberg cut-off for energy intake:basal metabolic rate. A practical guide to its calculation, use and limitations. Int J Obes Relat Metab Disord 24:1119–1130
Clabaugh K, Neuberger GB (2011) Research evidence for reducing sugar sweetened beverages in children. Issues Compr Pediatr Nurs 34(3):119–130
Craigie AM, Lake AA, Kelly SA, Adamson AJ, Mathers JC (2011) Tracking of obesity-related behaviours from childhood to adulthood: a systematic review. Maturitas 70:266–284
Danyliw AD, Vatanparast H, Nikpartow N, Whiting SJ (2011) Beverage intake patterns of Canadian children and adolescents. Public Health Nutr 14:1961–1969
Després JP, Lemieux I, Bergeron J, Pibarot P, Mathieu P, Larose E, Rodés-Cabau J, Bertrand OF, Poirier P (2008) Abdominal obesity and the metabolic syndrome: contribution to global cardiometabolic risk. Arterioscler Thromb Vasc Biol 28:1039–1049
Duffey KJ, Huybrechts I, Mouratidou T, Libuda L, Kersting M, De Vriendt T, Gottrand F, Widhalm K, Dallongeville J, Hallström L, González-Gross M, De Henauw S, Moreno LA, Popkin BM, HELENA Study group (2012) Beverage consumption among European adolescents in the HELENA study. Eur J Clin Nutr 66:244–252
Duffey KJ, Popkin BM (2006) Adults with healthier dietary patterns have healthier beverage patterns. J Nutr 136:2901–2907
Favier JC, Ireland-Ripert J, Toque C, Feinberg M (1995) Repertoire général des aliments. Table de composition. Parıs, Lavoisier Tec + Doc
Farajian P, Risvas G, Karasouli K, Pounis GD, Kastorini CM, Panagiotakos DB, Zampelas A (2011) Very high childhood obesity prevalence and low adherence rates to the Mediterranean diet in Greek children: the GRECO study. Atherosclerosis 217:525–530
Frary CD, Johnson RK, Wang MQ (2004) Children and adolescents’ choices of foods and beverages high in added sugars are associated with intakes of key nutrients and food groups. J Adolesc Health 34:56–63
Goldberg GR, Black AE, Jebb SA, Cole TJ, Murgatroyd PR, Coward WA, Prentice AM (1991) Critical evaluation of energy intake data using fundamental principles of energy physiology: 1. Derivation of cut-off limits to identify under-recording. Eur J Clin Nutr 45:569–581
Johnson L, Wilks DC, Lindroos AK, Jebb SA (2009) Reflections from a systematic review of dietary energy density and weight gain is the inclusion of drinks valid? Obes Rev 10:681–692
Johnson L, Mander AP, Jones LR, Emmett PM, Jebb SA (2007) Is sugar-sweetened beverage consumption associated with increased fatness in children? Nutrition 23:557–563
Kontogianni MD, Vidra N, Farmaki AE, Koinaki S, Belogianni K, Sofrona S, Magkanari F, Yannakoulia M (2008) Adherence rates to the Mediterranean diet are low in a representative sample of Greek children and adolescents. J Nutr 138:1951–1956
LaRowe TL, Moeller SM, Adams AK (2007) Beverage patterns, diet quality, and body mass index of US preschool and school-aged children. J Am Diet Assoc 107:1124–1133
Lawlor DA, Benfield L, Logue J, Tilling K, Howe LD, Fraser A, Cherry L, Watt P, Ness AR, Davey Smith G, Sattar N (2010) Association between general and central adiposity in childhood, and change in these, with cardiovascular risk factors in adolescence: prospective cohort study. BMJ 341:c6224
Lewitt MS, Baker JS, Mooney GP, Hall K, Thomas NE (2012) Pubertal stage and measures of adiposity in British schoolchildren. Ann Hum Biol 39:440–477
Li WC, Chen IC, Chang YC, Loke SS, Wang SH, Hsiao KY (2013) Waist-to-height ratio, waist circumference, and body mass index as indices of cardiometabolic risk among 36,642 Taiwanese adults. Eur J Nutr 52:57–65
Libuda L, Alexy U, Buyken AE, Sichert-Hellert W, Stehle P, Kersting M (2009) Consumption of sugar-sweetened beverages and its association with nutrient ntakes and diet quality in German children and adolescents. Br J Nutr 101:1549–1557
Mariscal-Arcas M, Rivas A, Velasco J, Ortega M, Caballero AM, Olea-Serrano F (2009) Evaluation of the Mediterranean Diet Quality Index (KIDMED) in children and adolescents in Southern Spain. Public Health Nutr 12:1408–1412
Mataix J, Mañas M, Llopis J, Martínez de Vitoria E (1998) Tabla de composició n de alimentos españoles, 3rd edn. Granada, Universidad de Granada
Mathias KC, Slining MM, Popkin BM (2013) Foods and beverages associated with higher intake of sugar-sweetened beverages. Am J Prev Med 44:351–357
Nelson M, Black AE, Morris JA, Cole TJ (1989) Between- and within-subject variation in nutrient intake from infancy to old age: estimating the number of days required to rank dietary intakes with desired precision. Am J Clin Nutr 50:155–167
Newby PK, Peterson KE, Berkey CS, Leppert J, Willett WC, Colditz GA (2004) Beverage consumption is not associated with changes in weight and body mass index among low-incomepreschool children in North Dakota. J Am Diet Assoc 104:1086–1094
Olsen NJ, Andersen LB, Wedderkopp N, Kristensen PL, Heitmann BL (2012) Intake of liquid and solid sucrose in relation to changes in body fatness over 6 years among 8- to 10-year-old children: the European Youth Heart Study. Obes Facts 5:506–512
Olsen NJ, Heitmann BL (2009) Intake of calorically sweetened beverages and obesity. Obes Rev 10:68–75
Rodríguez-Artalejo F, García EL, Gorgojo L, Garcés C, Royo MA, Martín Moreno JM, Benavente M, Macías A, De Oya M, Investigators of the Four Provinces Study (2003) Consumption of bakery products, sweetened soft drinks and yogurt among children aged 6–7 years: association with nutrient intake and overall diet quality. Br J Nutr 89:419–429
Rolls BJ (2009) The relationship between dietary energy density and energy intake. Physiol Behav 97:609–615
Schofield WN (1985) Predicting basal metabolic rate, new standards and review of previous work. Hum Nutr Clin Nutr 39(suppl 1):S5–S41
Schröder H, Mendez MA, Gomez SF, Covas MI, Ribas L, Aranceta J, Serra-Majem L (2013) Energy density, diet quality, and central body fat in a nationwide survey of young Spaniards. Nutrition 29:1350–1355
Schröder H, Méndez MA, Ribas-Barbas L, Covas MI, Serra-Majem L (2010) Mediterranean diet and waist circumference in a representative national sample of young Spaniards. Int J Pediatr Obes 5:516–519
Serra-Majem L, Ribas L, García A, Pérez-Rodrigo C, Aranceta J (2003) Nutrient adequacy and Mediterranean diet in Spanish school children and adolescents. Eur J Clin Nutr 57(Suppl1):S35–S39
Serra-Majem L, Ribas L, Ngo J, Ortega RM, García A, Pérez-Rodrigo C, Aranceta J (2004) Food, youth and the Mediterranean diet in Spain. Development of KIDMED, Mediterranean diet quality index in children and adolescents. Public Health Nutr 7:931–935
Stanhope KL, Schwarz JM, Keim NL, Griffen SC, Bremer AA, Graham JL, Hatcher B, Cox CL, Dyachenko A, Zhang W, McGahan JP, Seibert A, Krauss RM, Chiu S, Schaefer EJ, Ai M, Otokozawa S, Nakajima K, Nakano T, Beysen C, Hellerstein MK, BerglundL HPJ (2009) Consuming fructose-sweetened, not glucose-sweetened, beverages increases visceral adiposity and lipids and decreases insulin sensitivity in overweight/obese humans. J Clin Invest 119:1322–1334
Striegel-Moore RH, Thompson D, Affenito SG, Franko DL, Obarzanek E, Barton BA, Schreiber GB, Daniels SR, Schmidt M, Crawford PB (2006) Correlates of beverage intake in adolescent girls: the National Heart, Lung, and Blood Institute Growth and Health Study. J Pediatr 148:183–187
Suliga E (2009) Visceral adipose tissue in children and adolescents: a review. Nutr Res Rev 22:137–147
Tam CS, Garnett SP, Cowell CT, Campbell K, Cabrera G, Baur LA (2006) Soft drink consumption and excess weight gain in Australian school students: results from the Nepean study. Int J Obes (Lond) 30:1091–1093
Tappy L, Lê KA, Tran C, Paquot N (2010) Fructose and metabolic diseases: new findings, new questions. Nutrition 26:1044–1049
Tirosh A, Shai I, Afek A, Dubnov-Raz G, Ayalon N, Gordon B, Derazne E, Tzur D, Shamis A, Vinker S, Rudich A (2011) Adolescent BMI trajectory and risk of diabetes versus coronary disease. N Engl J Med 364:1315–1325
Torun B, Davies PS, Livingstone MB, Paolisso M, Sackett R, Spurr GB (1996) Energy requirements and dietary energy recommendations for children and adolescents 1 to 18 years old. Eur J Clin Nutr 50(suppl 1):S37–S80
Vartanian LR, Schwartz MB, Brownell KD (2007) Effects of soft drink consumption on nutrition and health: a systematic review and meta-analysis. Am J Public Health 97:667–675
Wang YC, Bleich SN, Gortmaker SL (2008) Increasing caloric contribution from sugar-sweetened beverages and 100 % fruit juices among US children and adolescents, 1988–2004. Pediatrics 121:e1604–e1614
Welsh JA, Cogswell ME, Rogers S, Rockett H, Mei Z, Grummer-Strawn LM (2005) Overweight among low-income preschool children associated with the consumption of sweet drinks: Missouri, 1999–2002. Pediatrics 115:e223–e229
WHO (2009) Mortality and burden of disease attributable to selected major risks. World Health Organization, Geneva
Yamada M, Murakami K, Sasaki S, Takahashi Y, Okubo H (2008) Soft drink intake is associated with diet quality even among young Japanese women with low soft drink intake. J Am Diet Assoc 108:1997–2004
Acknowledgements
We appreciate the English revision by Elaine M. Lilly, Ph.D. (Writers First Aid). This study was supported by grants from Instituto de Salud Carlos III-FEDER, (PI11/01900), the Spanish Ministry of Health [RED: “Alimentación saludable en la prevención primaria de enfermedades crónicas: la Red Predimed”, one of the Redes Temáticas de Investigación Cooperativa Sanitaria (RETICs)] Fundación Dieta Mediterránea, Spain; and Kellogg’s España SA and Kellogg’s Company, Battle Creek, USA via the Fundación Universitaria de Las Palmas de Gran Canaria and the Fundación para la Investigación Nutricional and by a joint contract “Miguel Servet” (CES09/030) with the Instituto de Salud Carlos III and the Health Department of the Catalan Government (Generalitat de Catalunya). The CIBERESP and the CIBEROBN and the RETIC Predimed are initiatives of the Instituto de Salud Carlos III, Madrid, Spain.
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Additional information
Communicated by David Nadal
Rights and permissions
About this article
Cite this article
Schröder, H., Mendez, M.A., Ribas, L. et al. Caloric beverage drinking patterns are differentially associated with diet quality and adiposity among Spanish girls and boys. Eur J Pediatr 173, 1169–1177 (2014). https://doi.org/10.1007/s00431-014-2302-x
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00431-014-2302-x