
Abstract
Objective
Frequent workflow interruptions jeopardise clinicians’ efficiency and quality of clinical care. We sought to determine the effect of a documentation-assistant intervention. Our hypothesis was that the expected decrease of workflow interruptions enhances paediatricians’ performance and simultaneously improves patients’ perceived quality of care.
Methods
This was a controlled intervention study with data collected before and after the intervention at a University Children’s Hospital. For the intervention, a documentation assistant was assigned to an inpatient ward. The main outcome measures were workflow interruptions, paediatricians’ performance, as well as patients’ perceived quality of care. Workflow interruptions were assessed via standardised expert observations. Paediatricians’ evaluated their performance in terms of productivity, quality, and efficiency. Additionally, standardised patients’ reports on perceived quality of care were collected.
Results
For paediatricians in the intervention ward, workflow interruptions decreased significantly from 5.2 to 3.1 disruption events per working hour (decrease in the control unit was from 3.8 to 3.1). Furthermore, paediatricians reported at follow-up significantly enhanced productivity, quality, and efficiency. Similarly, patients’ ratings of care quality improved significantly over time. In multivariate analyses, we found substantial changes attributable to the intervention: for all three outcomes, we found a significant interaction effect of the intervention over study time.
Conclusions
The intervention streamlined paediatricians’ workflow, improved day-to-day functioning of the ward, and enhanced organisational efficiency and delivery of paediatric care. Future studies should investigate potential influences between the reduction of workflow interruptions, paediatricians’ perceived performance, and patient-related outcomes in quality and efficiency of paediatric care.
Similar content being viewed by others



Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Quality of paediatric care is inextricably linked to the nature of the paediatricians’ working environment in the hospital. Clinical environments with elevated levels of workflow interruptions are suspected to jeopardise clinical performance and, potentially, negatively affect the quality of patient care [27]. Specifically, workflow interruptions are conducive to detrimental safety and quality practices in healthcare delivery [7, 10, 20]. Workflow interruptions are a particularly prevalent and detrimental stressor of medical professionals’ working environment [4, 6, 18]. Workflow interruptions in clinical care are linked to higher mental workload, aggravated work stress, and suboptimal clinical performance [5, 11, 13, 23, 28]. Furthermore, frequent workflow interruptions act as potential root cause for suboptimal staff communication, unfocused diagnostic procedures, deficient handovers, and/or medication errors during drug administration [1, 7, 18, 27]. Also in paediatric care, studies on workflow interruptions have shown that clinicians frequently face fragmented workflow and that the quality of patient care is closely related to the nature of paediatricians’ immediate work organisation [8, 16].
To address the complex socio-technical nature of workflow interruptions one adequate approach is to re-organise clinicians work organisation in the hospital environment [5, 16, 20]. However, the evidence base for interventions aiming to improve paediatricians’ workflow is limited. Specifically, limited knowledge on potential effects and outcomes arises in two directions: in terms of improved and smooth workflow (indicated by a low level of workflow interruptions), as well as in regard to paediatricians’ performance, and most importantly, in regard to patients’ perceptions of care quality.
Effective interventions to reduce physicians’ workflow interruptions should be specific to clinical context as well as sensitive to potential beneficial and harmful consequences [5, 12]. Sensitivity to the specific needs of health care delivery is particularly important since workflow interruptions can serve also in a positive way (e.g. stopping someone from making an error or alerts on patient’s critical condition) and are occasionally essential means to transfer important information among healthcare professionals [12, 20]. Additionally, the translation and external validity of study findings is enhanced if the investigation is conducted in real hospital environments.
Although several measures to reduce interruptions in healthcare settings were undertaken, questions concerning their effectiveness remain [5, 20, 25]. Most common approaches are isolation-type concepts similar to the sterile cockpit environment in aviation (i.e., ‘no interruption zones’ for preparing medication or use of ‘do-not-disturb vests’). Recently, a study in hospital physicians used a participatory approach to re-design physicians’ internal organisation and nurse-physician coordination [22]. Overall, in regard to the short- and long term values and effectiveness of those measures, a void of controlled studies remains [25]. Thus, robust controlled designs with reliable pre- and post-evaluations enhance the validity of the intervention effects; particularly to investigate the character and impact of clinicians’ workflow interruptions [14, 19].
In Germany, the assignment of documentation assistants to ward physicians is a widely requested proposition to streamline workflow and enhance patient care. Assistants are assigned to ward physicians and perform documentation and administrative functions. Documentation assistants are expected to relieve paediatricians from documentation and administrative workload, support non-clinical duties, as well as to enhance the internal organisation of the inpatient ward by coordinating and responding to certain patient-related requests from internal and external professions [16]. Concurrently, the assignment of a documentation assistant is expected to reduce paediatricians’ workflow interruptions by streamlining paediatricians’ workflow and patient care activities. As an example, by coordinating patient-related requests from nursing staff, documentation assistants’ activities target one of the main causes of hospital doctors’ workflow interruptions [24].
Our primary objective was to determine the effect of a documentation assistant intervention for reducing hospital paediatricians’ workflow interruptions and its impact on paediatricians’ performance, indicated by self-reported productivity, quality, and efficiency of work. Our secondary objective was to determine whether the intervention improved the patients’ perceived quality of care. We hypothesised that the intervention on limiting workflow interruptions would enhance physicians’ performance and lead to an improved quality of care perceived by the patients and patients’ relatives.
Subjects and method
Study design and setting
The study was a prospective unit-based intervention-control design with a baseline and follow-up assessment. It was conducted at Dr. von Hauner University Children’s Hospital, which is affiliated with the Munich University Hospital, Germany. The children’s hospital is a well-renowned university paediatric clinic with 150 patient beds and 10 medical specialty units.
The study was conducted within two paediatric inpatient wards that are similar in terms of specialty (internal medicine), case load and mix, diagnoses, staffing, size, and internal organisation. The intervention took place in the 16-bed intervention ward, which is regularly staffed with three paediatricians during the day, four nurses, and one to two healthcare assistants. All ward physicians are supervised by rotating senior physicians, who are usually present at the unit for ward rounds (in the morning) and occasionally for chart reviews (in the afternoon). The control ward encompasses 10 to a maximum of 12 beds and is staffed with two paediatricians during the day, two nurses, and one to two assistants. The routine work organisation was similar to the intervention ward. In both inpatient wards, children are treated for all areas of internal paediatric diseases with main focus on gastrointestinal, renal, infectious, and metabolic diseases. Usually two thirds of the patients are accompanied by parents or guardians during the hospital stay.
The study was approved by the Ethics Committee of the Medical Faculty of Munich University (no. 124-07). All eligible paediatricians and patients were provided written informed consent before inclusion into the study.
Intervention
The intervention was based on an assignment of a documentation assistant to the ward paediatricians of the intervention unit. Their primary function is to perform documentation and administrative tasks in patient care on ward. Their primary role is to support ward physicians in documentation, i.e. completion of patient charts, filing of medical reports, checking for missing patient documents, preparation of requirements, handling of mailings, and packaging of packages and lab specimens. Additionally, documentation assistants perform coordination functions, especially with the nursing staff, e.g. handing out patient documents or monitoring discharge documents. Within the ward team the assistant collaborates thus with ward physicians and nursing staff. In addition, interaction with hospital staff from other departments occurs, i.e. radiography, MRI. In some instances, mainly to facilitate timely performance of procedures on inpatient ward patients, collaboration with other subspecialties was carried out. In our specific case, the documentation assistant was installed to address problems in the hospital, such as complaints due physicians’ work overload, especially due to overtaxing administrative burden for paediatricians, overload through documentation, and large amount of non-clinical duties. This resulted frequently in delayed procedures and insufficient patient care. The documentation assistant was hired through newspaper advertisement. Key job requirement was education as medical record assistant. No specific training was conducted on site prior to start of the intervention.
The intervention took place right after completion of the baseline assessment. Time lag between baseline and follow-up assessment was on average four months. Neither group received feedback on study results before the end of the follow-up assessment. The paediatricians were aware of the study’s aims but were blinded from the specific hypotheses and outcome criteria. The patients and their relatives were blinded to the group assignment.
Recruitment process and study sample
All N = 8 paediatricians of the intervention and control ward were informed about the study. Inclusion criteria were working full-time on the respective wards. Exclusion criteria were working on ward less than four months, working without patient contact, or working half time. No paediatricians met exclusion criteria. The majority of paediatricians and nurses remained on their respective wards during the study period, however, three junior physicians changed because of their rotation schedules and specialty training.
Eligible patients and parents had to be inpatients in one of the two wards within the respective study period. Overall, 161 eligible patients, parents, or guardians were provided with oral and written information about the objectives of the study. Exclusion criteria included ambulatory care as well as duration of stay less than 2 days. No patients met exclusion criteria. With regard to patient characteristics, the general medical ward census for the baseline period was similar to that for the follow-up assessment.
Measures and data collection
Paediatricians’ workflow interruptions
Paediatricians’ workflow interruptions are defined as an intrusion of an unplanned event, that requires clinician’s attention, causing a discontinuation of tasks, a noticeable break, or task switch behaviour, e.g. a beeper call interrupts clinician while talking to a patient, urges him to call back, and to postpone the patient communication for two minutes [15, 24]. Expert observation using standardised methods has shown to be valid and reliable for healthcare services with particular application to the investigation of workflow interruptions [16, 20, 24, 26, 29]. Full-day shift observations serve as a meaningful way to investigate extended periods of paediatricians’ workflow and, therefore, enhance the validity of the observational results [16, 24].
In this study, we applied a well-established tool to observe hospital physicians’ workflow interruptions based on expert observation [24]. It enables reliable assessment of interruption events that occur in hospital clinicians’ work [22–24]. As in detail described elsewhere, the participant observer codes various sources of workflow interruptions that cause observable task switch behaviour or noticeable breaks from the primary task [22–24]. An experienced and well-trained expert with a medical background conducted the full-day observations and was familiarised with the study site prior to the study start. The observer shadowed the paediatricians throughout the entire day shift and consistently coded workflow interruptions [24]. To minimise observational effects, the observers kept an appropriate distance and were instructed not to interrupt doctors or co-working staff (e.g. not to start a conversation). All observation dates were selected randomly.
To ensure tool’s reliability for observation of workflow interruptions several measures were undertaken before commencement of the main study. First, pilot observations were conducted on study site prior to the baseline assessment, i.e. to become familiar with the hospital environment and to discuss potential problems in detecting interruption events. Secondly, we tested tool’s reliability in terms of inter-observer agreement in four observations: four hospital doctors were simultaneously observed by an experienced observer (author Matthias Weigl) and newly trained observer (author Nina Barth (NB)) simultaneously (range, 37.18–64.5 min; sum, 204.01 min). Sixty-six workflow interruptions were observed and the resulting Kappa coefficient was 0.63. This indicates substantial inter-rater agreement and supports the tool’s previous reliability tests [23, 24]. All observations during the main study were conducted by NB.
Paediatricians reported productivity, quality, and efficiency
Paediatricians reported on three essential facets of their clinical performance during the observations based on three items of an established scale to measure performance [9]. During the observations the paediatricians reported twice on their performance: during halftime and at the end of the observed shift. The three items refer to perceived productivity (‘How productive were you at your work?’; Scale range: 0 = very unproductive, 10 = very productive), quality (‘How do you rate the quality of your work?’; 0 = very low quality, 10 = very high quality), and perceived efficiency of work (‘How efficient were you at your work’; 0 = very inefficient, 10 = very efficient). All three items used a visual response scale. Additionally, an aggregated score for the three items, indicating the overall self-perceived performance, was computed. The scale’s reliability in terms of internal consistency was good: Cronbach’s Alpha = 0.77.
Patients perceived quality of care
Patient Care Quality—patients reported perceived quality of care using an established, standardised questionnaire (Munich Patient Inventory [3]). Two major facets of paediatric care quality were covered: (1) Goodness of paediatricians’ patient-oriented work-organisation as an indicator of the patient centeredness of paediatricians’ work schedules and routines (three items: ‘I know the physician who is responsible for me’, ‘During ward rounds, physicians only turn to the next patient after completing my visit’, ‘The physicians devote enough time to me’). (2) Quality of paediatricians’ information to inpatients (three items: ‘Physicians inform me in a comprehensible way about the progress of my therapy and treatment’, ‘Physicians discuss with me in detail my further therapy and treatment’, and ‘Physicians explain me how I ought to cope with my disease back home’). All items and scales had a visual response scale ranging from 1 = ‘not at all’ to 5 = ‘yes, very much’. The scales showed consistently sufficient psychometric quality: (1) CA, Cronbach’s Alpha = .62; (2) CA = .72. (3) As third quality indicator the patients reported an overall rating of their hospital treatment in terms of a German school grade. The question was ‘How do you rate your hospital stay until now in total of a school grade?’ The range was from 6 (‘insufficiently’), 5 (‘deficient’), to 2 (‘good’), and 1 (‘very good’).
The questionnaire was handed out to patients towards the end of their hospital stay by an independent study assistant. If inpatients were incapable reading or filling out the survey their parents or guardians were asked to participate. Completed questionnaires were directly returned within a sealed envelope to the study team. No further patient data were collected.
Statistical analyses
For all time points, observational as well as paediatricians’ and patients’ data were recorded on clipboards or questionnaires, transferred via double data entry into a database, and checked for errors and implausible values. First, we computed interruption rates per hour for the observational data and mean scores for paediatricians and patients self-report data. Descriptive statistics included means and 95 % confidence intervals (CI) for each group and time point. Interruption rates were treated as Poisson random variables. Secondly, as the main objective of the study is the change in interruption rates for the intervention group compared with the control group over time, we computed a Poisson regression model with logarithmic link functions (generalised linear model). This included binary covariates for intervention/control ward and baseline/follow-up as well as their two-way interaction. Main model outcome of interest was the (exponent of the) estimated coefficient of the interaction term, since this indicates the percentage change attributable to the intervention. Thirdly, a linear regression approach was applied to paediatricians and patients reports (with similar covariates). Again, the main outcome criterion was a significant interaction effect between time and group. All analyses were performed using SPSS 20.0 and for all tests, p < .05 was considered statistically significant.
Results
Overall 28 full-shift observations were conducted; at baseline 17 (intervention ward (IW), 11; control ward (CW), 6) and at follow-up 11 (IW, 5; CW, 6). Allocation of observations to groups across the time points showed no significant difference (Chi2 = 1.01, df = 1, p = .31). The overall duration of expert observation was 287 h, 28 min, and 35 s. The average shift duration was 9 h, 25 min, and 32 s (standard deviation (SD) = 00:36:59) and did not differ between time points or groups under study.
-
1.
Rate of observed workflow interruptions
To account for the time length of the observations we computed the average rate of workflow interruptions per observed work hour. Overall, the observed paediatricians were interrupted on average 4.17 times per working hour (SD = 3.35). Figure 1 reports the average number of interruption events for the intervention and control group and across time points:
Fig. 1 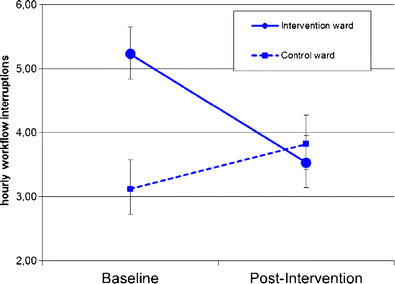
Paediatricians’ workflow interruptions across intervention and control ward for baseline and follow-up
At baseline we recorded in the intervention ward M = 5.23 hourly interruptions (Standard error, SE = 0.21, N = 123 h of observation, 95 % CI= 4.84–5.65). In the control ward M = 3.11 interruptions per working hour occurred (SE = 0.22, N = 66, CI = 2.72–3.57). During follow-up we observed M = 3.53 hourly workflow interruptions in the intervention unit (SE = 0.25, N = 55, CI = 3.06–4.06), whereas in the control ward M = 3.82 interruptions events were recorded (SE = 0.24, N = 66, CI = 3.37–4.32).
Poisson regression analyses for change revealed a significant main effect for time (baseline β = .394, SE = .136, p = .004) but no main effect for intervention/control ward allocation (intervention ward β = .079, SE = .162, p = .24). Primary objective was to detect change in interruption rates for the intervention group compared with the control group. The two-way interaction of baseline/follow-up and intervention/control ward revealed a significant effect (baseline/intervention ward β = − .596, SE = .213, p = .005). This corresponds to a percentage of change in interruptions rates attributable to the intervention of 55.1 % (CI = 36.3–83.6 %).
-
2.
Paediatricians’ reported productivity, quality, and efficiency at work over time
All paediatricians completed a self-rating on their performance two times during the day shift, resulting in N = 56 performance evaluations.
For all three reports of paediatricians’ performance at work we observed a significant interaction between time and intervention/control ward allocation, i.e. an effect over time that can be attributed to the intervention (cf. Table 1). For self-perceived productivity we observed in the intervention ward an increase of +45.27 % over time (CW, −25.05 %). Similarly, substantial changes that were attributable to the intervention were also observed for reported quality (IW, +54.1 %; CW, −28.69 %) and efficiency of paediatricians work (IW, +69.6 %; CW, −9.31 %).
Table 1 Paediatricians’ self-rated productivity, quality, and efficiency at work-over time -
3.
Patients’ perceived quality of care over time
Additionally, patients and patients’ relatives were requested to report on their perceived quality of care. At baseline assessment ten selected patients refused to participate (IW, 3; CW, 7), during follow-up 19 patients did not join the survey (IW, 10; CW, 9). Most cited reasons were limited German language skills of the patients or their relatives, no presence of relatives during assessment, or non-scheduled, sudden discharge of patients. We found no significant difference for the drop-out over units and time: Chi2 (df = 1) = 1.36, p = .24. Overall, 132 inpatients, or inpatients’ relatives or guardians filled out the survey. Across time points and wards we found no significant difference in survey participation: Chi2 (df = 1) = .049, p = .48. Patients’ perceived quality of care was rated as follows:
We observed a significant interaction effect between time and intervention/control ward allocation on patient rated goodness of paediatricians’ work-organisation. In the intervention ward a 10.43 % increase attributable to the intervention was observed (CW, −8.97 %). Moreover, we also observed a significant interaction effect between time and intervention/control ward allocation, (cf. Table 2) that there was a relative improvement of the quality of patient information in the intervention group compared with the control group over time (cf., Table 2; IW, +11.12 %; CW, −3.39 %). For perceived quality of care only a slight trend for the effectiveness of the intervention was observed (p = 0.08; cf., Table 2; IW, +16.59 %; CW, −7.29 %).
Table 2 Patients’ perceived quality of care across units and time

Discussion
In this controlled study, the intervention was associated with reduced workflow interruptions, increased paediatricians’ performance in terms of self-rated performance, quality, and efficiency in their daily clinical work practices. Additionally, we found effects attributable to the intervention in regards to increased patients’ perceptions of quality of care. Patient-related effects associated with the intervention revealed increased paediatricians’ patient-oriented work-organisation, the quality of paediatricians’ patient information, and an overall quality rating for the hospital stay.
Increasingly, detrimental work conditions in paediatricians’ clinical work are identified as root cause of unfavourable patient outcomes. Our study demonstrates that interruptions occur frequently in hospital paediatricians’ work: the overall degree of observed workflow interruptions is in line with previous studies in hospital clinicians [24, 26]. On the one hand, this reflects the high need of intra- and inter-professional communication in hospital work and the inherent risk for disruptive clinical work practices [14, 20]. On the other hand, this may also be attributed to ‘interruptive communication mechanisms’ and behaviours between healthcare professionals [6].
We sought to investigate the effect of an intervention to reduce workflow interruptions and its impact on certain quality indicators of paediatric care—from the perspective of care providers, i.e. the affected paediatricians, as well as the care recipients, i.e. patients and their relatives. The paediatricians’ workflow interruptions were observed via independent, expert observation and showed a significant reduction through the assignment of documentation assistants who performed documentation and administrative functions. The respective outcomes changed according to the allocation of the intervention. First, paediatricians in the intervention unit reported a significant improvement in their daily performance—in terms of self-perceived productivity, quality, and efficiency. Secondly, patients’ appraisals of care quality showed similar patterns of improvements. This is particularly of interest, as patients were blinded to the allocation of the intervention. The intervention caused improved goodness of paediatricians’ patient-oriented work-organisation and quality of paediatricians’ patient information in the intervention units. A slight effect in favour of the intervention was additionally observed for patients’ overall quality rating.
This study cannot fully reveal the specific mechanisms of the intervention that caused the observed change. However, as it was the duty of the documentation assistant to enhance the internal organisation of the intervention ward by coordinating and responding to patient-related requests from internal and external professions the reduction of interruptions by the intervention is plausible. Moreover, as the documentation assistant took over documentation and administrative functions, we assume, that clinicians’ benefited from reduced mental workload as well as less fragmented workflow and, thus, more effectively managed clinical duties [8, 23]. Eventually, with that also the patients benefited, as paediatricians provide better care in work environments without consistent interruptions [20]. More specifically, as the paediatricians were relieved from additional documentation and coordination duties in their daily practice they might be able to provide improved and comprehensive information to the patients about further therapy and treatment.
Interventions to reduce interruptions should be sensitive to the complexity of healthcare, the special requirements of intra- and inter-professional communication, as well as to the nature and purpose of disruptive incidents in clinical care [20]. Thus, our intervention contributes to the evidence base, as our approach for the first time, as far as we know, specifically addressed workflow interruptions and their impact on care-related outcomes. Overall, this intervention demonstrates a feasible solution to address and diminish inappropriate workflow interruptions between healthcare professionals. Thus, our study contributes to multifactor approaches that are needed to mitigate adverse impact of frequent workflow interruptions in healthcare work environments [19]. Considering the challenges of conducting and evaluating organisational interventions in real hospital settings, the results of our prospective-controlled design support the external validity of our findings for work design practices in paediatric care.
We acknowledge that the intervention is associated with substantial costs and resources. The specific costs associated with implementing the new role were roughly 30.000€ (per year), particularly due to the wage for the documentation assistant. The future challenge will be to generate continuous funding to compete for and retain personnel in this role. Further potential downsides of the intervention may refer to the enhanced needs for coordination between the assistant and the ward personnel, increased needs for information transfer (nurse- and physician-assistant interface), and retention after labour intensive training and orientation. Consistent to a somewhat similar approach in paediatric care, local staff also reported frictions due to initial confusion over professional roles [17].
Limitations of the study
Although our study addressed many previous limitations of this area of research, a quasi-experimental study such as this has certain inherent limitations: First, we only counted the number of timely inappropriate interruptive events but did not specify for the content or severity of observed interruptive events. Specifically, we did not control for the nature of the interruptive events, e.g. alert about a critical patient condition [20]. Therefore, we cannot exclude that observed workflow interruptions also occurred for appropriate reason, i.e. ensuring a quick and effective functioning of care activities on the wards. However, this is very unlikely due to the nature of the intervention. The results apply to paediatricians providing ward coverage and thus the prevalence of disruptive events may differ in ED- or operating room environments [2, 21]. Secondly, we applied a four month time lag for the follow-up. We cannot conclude about the temporal sustainability of the identified effects above the observational period. Groups were not identical over time, i.e. different physicians and patients at baseline and after the intervention. Thirdly, we cannot exclude the possibility of confounding observer bias, as it is possible that the observed staff in the intervention and control unit behaved according to the overall study objectives. Observational data was tested for inter-rater reliability prior to the baseline assessment. Clinicians and nurses were informed about the study objectives and were obviously aware about the allocation of the intervention. Although we sought not to communicate our hypothesis prior to study commencement, we cannot exclude that staff may have inferred about our hypothesis and thus shaped their responses accordingly. Taking potential bias due to paediatricians’ self-reports into account, we however also observed a positive intervention effect in patients’ reports. This supports our findings because patients were completely blinded to the assignment of the intervention and as such were not able to respond according to the study objectives. However, we acknowledge that the magnitude of change in patient ratings was comparatively smaller than paediatricians’ reports what may indicate potential bias. Fourth, we acknowledge that the overall effectiveness of the intervention was also attributable to differences between the units at baseline as well as changes in the control ward over time, i.e. inferior performance reports over time.
Finally, the reported study was a single-centre trial and may only apply to the specific intervention that was studied. University-based medical care, with teaching and research obligations, may encompass different organisational and care routines than in community hospital environments. Although the study setting is an academic, paediatric-specific facility, the distribution of observed workflow interruptions was similar to that in previous studies in physicians providing ward coverage [23, 24]. This supports the validity of our data and suggests that our data may be generalisable to other hospital settings.
In regard to transfer to other settings, we assume that the intervention and its above reported advantages can be replicated in other hospital settings. As many health care organisations face cost constraints and manpower regulations, our experience and the reported benefits may serve as an argument to allocate resources to front line care in order to simultaneously improve physicians’ work life and patient care.
Implications of the study
This study’s results carry several implications: Clinically, the findings demonstrate that the re-organisation of paediatricians’ clinical practice to mitigate workflow interruptions may be a promising strategy to enhance performance and quality of paediatric care. The results support that reducing unnecessary workflow interruptions may be conducive to paediatricians’ work-life as well as to patients’ perceived quality of care. Furthermore, this approach might contribute to activities to foster clinical safety and high quality care practices.
Our results also provide ground for future research. Specific investigations into the character and frequency of paediatricians’ workflow interruptions and routines are necessary [14]. In this study, we used a comparatively simple definition to observe interruption events and did not take into account entirely the complexity of the role of interruptions [5, 12, 20]. As mentioned above, interruptions in healthcare can also be associated with potentially positive outcomes, i.e. improved safety, accuracy, or patient’s conditions [5, 12]. Future interventions that target interruptions in clinical care should also examine to what extent harmful interruptions can be decreased as well as simultaneously maintaining interruption events with positive outcomes. Studies should also investigate potential side-effects or unintended effects of interventions to reduce workflow interruptions. Potentially, fewer interruptions may streamline patient care as well as enhance effective and timely communication between various professional groups, i.e. potential solutions in paediatricians’ favour may pose disadvantages for other professions involved in patient care. Incorporating qualitative measures to elicit the views of affected professions, particularly the nurses, may widen the scope as well as identify relevant process-related factors of the intervention and its consequences.
In regard to policy implications, our study serves as an example that providing additional resources (i.e. documentation assistant) to the front line of care is associated with benefits from the perspective of patients and providers. As many health care systems nowadays are cash-strapped and driven by strategies to remove and limit front line resources, our intervention serves as a feasible example that can also be easily transferred to other health care institutions.
Conclusions
To our knowledge, no studies exist in the paediatric care literature on workflow interruptions and its consequences for care practices. We assume that this is the first intervention study performed in paediatric care that determines the effect of an intervention to re-organise and smooth paediatricians’ workflow. Moreover, we are unaware of any multi-method study used to examine the effect of a change in paediatricians’ workflow in terms of paediatricians’ self-reported performance as well as patients’ reports on care quality.
In combining observational and self-report data we have shown that assigning a documentation assistant to hospital paediatricians significantly reduced workflow interruptions and improved paediatricians’ performance and patients’ perceived quality of care. Thus, our findings strengthen the claim that in order to reduce workflow interruptions, paediatricians’ work environments need to be well designed socio-technical systems, balancing inter- and intra-professional interactions and coordination in healthcare delivery.
References
Biron AD, Loiselle CG, Lavoie-Tremblay M (2009) Work interruptions and their contribution to medication administration errors: an evidence review. Worldviews Evid Based Nurs 6(2):70–86
Brixey JJ, Tang Z, Robinson DJ, Johnson CW, Johnson TR, Turley JP, Patel VL, Zhang J (2008) Interruptions in a level one trauma center: a case study. Int J Med Inform 77(4):235–241
Bussing A, Glaser R (2003) Employee and client orientation in health care services. Zeitschrift fuer Arbeits- und Organisationspsychologie. J Work Organ Psychol 47(4):222–228
Chisholm CD, Dornfeld AM, Nelson DR, Cordell WH (2001) Work interrupted: a comparison of workplace interruptions in emergency departments and primary care offices. Ann Emerg Med 38(2):146–151
Coiera E (2012) The science of interruption. BMJ Qual Saf 21(5):357–360
Coiera E, Tombs V (1998) Communication behaviours in a hospital setting: an observational study. Bmj 316(7132):673–676
Flynn EA, Barker KN, Gibson JT, Pearson RE, Berger BA, Smith LA (1999) Impact of interruptions and distractions on dispensing errors in an ambulatory care pharmacy. Am J Health Syst Pharm 56(13):1319–1325
Gabow PA, Karkhanis A, Knight A, Dixon P, Eisert S, Albert RK (2006) Observations of residents’ work activities for 24 consecutive hours: implications for workflow redesign. Acad Med 81(8):766–775
Grawitch MJ, Granda SE, Barber LK (2008) Do prospective workday appraisals influence end-of-workday affect and self-monitored performance? J Occup Health Psychol 13(4):331–344
Grundgeiger T, Sanderson P (2009) Interruptions in healthcare: theoretical views. Int J Med Inform 78(5):293–307
Hakimzada AF, Green RA, Sayan OR, Zhang J, Patel VL (2008) The nature and occurrence of registration errors in the emergency department. Int J Med Inform 77(3):169–175
Hopkinson SG, Jennings BM (2013) Interruptions during nurses’ work: a state-of-the-science review. Res Nurs Health 36(1):38–53
Jett QR, George JM (2003) Work interrupted: a closer look at the role of interruptions in organizational life. Acad Manage Rev 28(3):494–507
Laxmisan A, Hakimzada F, Sayan OR, Green RA, Zhang J, Patel VL (2007) The multitasking clinician: decision-making and cognitive demand during and after team handoffs in emergency care. Int J Med Inform 76(11–12):801–811
Li SY, Magrabi F, Coiera E (2012) A systematic review of the psychological literature on interruption and its patient safety implications. J Am Med Inform Assoc 19(1):6–12
Mache S, Vitzthum K, Kusma B, Nienhaus A, Klapp BF, Groneberg DA (2010) Pediatricians’ working conditions in German hospitals: a real-time task analysis. Eur J Pediatr 169(5):551–555
Mathur M, Rampersad A, Howard K, Goldman GM (2005) Physician assistants as physician extenders in the pediatric intensive care unit setting-A 5-year experience. Pediatr Crit Care Med 6(1):14–19
O’Shea E (1999) Factors contributing to medication errors: a literature review. J Clin Nurs 8(5):496–504
Relihan E, O’Brien V, O’Hara S, Silke B (2010) The impact of a set of interventions to reduce interruptions and distractions to nurses during medication administration. Qual Saf Health Care 19(5)
Rivera-Rodriguez AJ, Karsh BT (2010) Interruptions and distractions in healthcare: review and reappraisal. Qual Saf Health Care 19(4):304–312
Sevdalis N, Sonal A, Undre S, Vincent CA (2009) Distractions and Interruptions in the Operating Room. In: Flin R, Mitchell L (eds) Safer surgery: distractions and interruptions in the operating room. Ashgate, Farnham, pp 405–419
Weigl M, Hornung S, Glaser J, Angerer P (2012) Reduction of hospital physicians’ workflow interruptions: a controlled unit-based intervention study. J Healthc Eng 3(4):605–620
Weigl M, Müller A, Vincent C, Angerer P, Sevdalis N (2012) The association of workflow interruptions and hospital doctors’ workload: a prospective observational study. BMJ Qual Saf 21(5):399–407
Weigl M, Müller A, Zupanc A, Glaser J, Angerer P (2011) Hospital doctors’ workflow interruptions and activities: an observation study. BMJ Qual Saf 20(6):491–497
Westbrook JI (2013) Interruptions to clinical work: how frequent is too frequent? J Grad Med Educ 5(2):337–339
Westbrook JI, Coiera E, Dunsmuir WT, Brown BM, Kelk N, Paoloni R, Tran C (2010) The impact of interruptions on clinical task completion. Qual Saf Health Care 19(4):284–289
Westbrook JI, Woods A, Rob MI, Dunsmuir WT, Day RO (2010) Association of interruptions with an increased risk and severity of medication administration errors. Arch Intern Med 170(8):683–690
Wiegmann DA, ElBardissi AW, Dearani JA, Daly RC, Sundt TMI (2007) Disruptions in surgical flow and their relationship to surgical errors: an exploratory investigation. Surgery 142(5):658–665
Yen K, Shane EL, Pawar SS, Schwendel ND, Zimmanck RJ, Gorelick MH (2009) Time motion study in a pediatric emergency department before and after computer physician order entry. Ann Emerg Med 53(4):462–468, e461
Acknowledgements
The authors gratefully acknowledge Susanne Jüstel, Kathrin Krohn, and Christoph Bidlingmaier for assistance in preparation and conducting the study. This research was part of the doctoral dissertation research of Nina Barth. Jürgen Glaser assisted in preparing measure development. We thank Jake Burns for assistance in manuscript preparation.
Ethics approval
This study was conducted with the approval of the Ethics Committee of the Medical Faculty of Munich University (no. 124/07).
Conflict of interest
The authors declare that they have no conflict of interest. The authors also have no financial relationship with the organisation that sponsored the research.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Weigl, M., Hoffmann, F., Müller, A. et al. Hospital paediatricians’ workflow interruptions, performance, and care quality: a unit-based controlled intervention. Eur J Pediatr 173, 637–645 (2014). https://doi.org/10.1007/s00431-013-2232-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00431-013-2232-z