
Abstract
We examined the relationship between cesarean section (C-section) and the risk of overweight and obesity in children in grade 6 (mean age, 11.92 years; standard deviation = 0.34). Data from phase I through phase III of the National Institute of Child Health and Human Development Study of Early Child Care and Youth Development were used. Children with complete data from 1991 through 2004 were included in this study (n = 917). Multiple logistic regression analyses were used to adjust for potential confounding and to evaluate the association of C-section and childhood overweight and obesity. Compared to children delivered vaginally, children delivered by C-section had approximately twice the likelihood of being overweight (odds ratio (OR) = 1.86, 95 % confidence interval (CI) = 1.27–2.73) or obese (OR = 1.87, 95 % CI = 1.19–2.95). However, when examined according to sex, males delivered by C-section had an increased risk for being overweight (OR = 1.78, 95 % CI = 1.01–3.12) and obese (OR = 2.58, 95 % CI = 1.36–4.88), while females had an increased risk only for being overweight (OR = 1.99, 95 % CI = 1.17–3.39). Conclusion: C-section was associated with an increased risk of overweight and obesity in children in grade 6, but the relationship differed according to gender. Further longitudinal studies are warranted to examine the long-term effect of delivery mode on the risk of childhood overweight.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The prevalence of childhood overweight tripled from 1980 to 2000 in the USA [30]. Although surveillance data suggest that these rates may be slowing or leveling off [9, 29], childhood obesity remains an important public health concern due to the immediate and long-term health effects. Childhood obesity is associated with an increased risk for high cholesterol and high blood pressure [11], prediabetes [6, 23], sleep apnea [39], and psychosocial problems [7]. Childhood obesity also increases the likelihood that the child will be obese as an adult [10, 37] with an increased risk for heart disease, type 2 diabetes, stroke [28], and numerous cancers [22].
Effective strategies are needed to confront the global obesity epidemic. One possible strategy is to identify modifiable risk factors that occur during the perinatal stage [12]. Over the past two decades, there has been a marked increase in the rates of cesarean sections (C-sections) worldwide [4]. In many middle- and upper-income countries, C-sections are increasing and may eventually surpass vaginal births as the primary delivery mode. For example, in the USA, Huh and colleagues reported that C-sections increased by 11.3 % between 1996 and 2007 [16] and accounted for approximately one in three births [15, 19], whereas in other countries, this rate has increased to half of all births [25]. Studies have associated the increase in cesarean deliveries to the mothers' preference because they fear of having an adverse experience with vaginal birth, such as vaginal tearing or an emergency C-section [16, 25]. These procedures are also often needed to reduce or eliminate the potential for medical complications during vaginal births. Yet, there is mounting evidence that the increasing C-section rates may have adverse effects on offspring that persist into adulthood [5, 8, 42]. To our knowledge, few studies have investigated the relationship between delivery mode and the risk of childhood overweight and obesity. Among those studies that do exist, findings have been inconsistent [1, 2, 16]. The purpose of this study is to examine the association of C-section and the risk of childhood overweight and obesity among students in grade 6.
Methods
Data source and participants
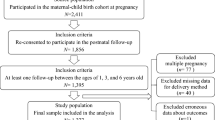
Data were obtained from phase I to phase III of the National Institute of Child Health and Human Development (NICHD) Study of Early Child Care and Youth Development (SECCYD), one of the most comprehensive studies of children, and the contexts of their development were conducted in the USA. During phase I (1991–1994), a cohort of 1,364 children and their families were recruited at 1 month of age and studied intensively through age 3. During phase II (1995–1999), 1,226 of the enrolled children and their families were followed through first grade. During phase III (2000–2004), 1,061 of the enrolled children and their families continued to have follow-up through sixth grade. More information can be found at http://www.nichd.nih.gov/research/supported/Pages/seccyd.aspx or elsewhere [26]. Only subjects followed from birth to grade 6 (with complete data on weight status, C-section, and covariates) from phase I through phase III for the years 1991 to 2004 were included in this study (n = 917). The average age of these included children in grade 6 was 11.92 years (standard deviation = 0.34). The study was approved by the Institutional Review Boards of all participating institutions.
Variables
Childhood overweight and obesity
Overweight and obesity measures were defined according to the Centers for Disease Control and Prevention (CDC) growth charts [21] for body mass index (BMI), with overweight (including obesity) defined as ≥85th percentile and obesity as ≥95th percentile. Both overweight and obesity were expressed as dichotomized variables. Standardized procedures were used to measure height and weight during the interviews by NICHD SECCYD staff. Height was measured with children without shoes who were standing, feet together, and their backs against a calibrated 7-ft measuring stick. Weight was measured using a physician's two-beam scale. Scales were calibrated monthly using certified calibration weights. Weight was measured with children in minimal clothing and recorded twice, each time to the nearest 0.25 lb (0.1 kg). This study followed the same children from birth through grade 6. We used data on BMI values from when the children were in grade 6 as outcome variables.
C-section
Home visit interviews were conducted with the mothers when the child was 1 month old. Delivery modes were determined by asking mothers the question, “What type of delivery did you have?” Response options included vaginal delivery, planned C-section, and emergency C-section. In our study, delivery mode was dichotomized as C-section and vaginal delivery due to small sample size.
Covariates
Maternal factors were collected during a maternal interview conducted when the child was 1 month old. These covariates included maternal age in years, education (bachelor's degree or above, less than a bachelor's degree), poverty (above poverty line, at or below poverty line), living status (living single, not living single), depression (depressed, not depressed), breastfeeding status (breastfeeding, not breastfeeding), and smoking during pregnancy (smoked, not smoked). The poverty threshold for a household was determined by the year the income was earned, the total number of members in the household, and the number of full-time children living in the home. The income-to-needs ratios were based on the total family income and calculated as an indicator of socioeconomic status. If the ratio of income to needs was less than 1, households were considered below poverty level, while households with 1 and above were considered at or above poverty level. Maternal depressive symptoms were measured using the Center for Epidemiologic Studies Depression Scale (CES-D). The CES-D provides an index of depressive symptoms and has a high internal reliability (Cronbach's alpha = 0.878). The scores can range from 0 to 60 with higher scores representing higher levels of depressive symptoms. In our study, mothers who scored 16 or higher on the CES-D scale were considered to have clinically significant depressive symptoms [35]. Breastfeeding status was determined by asking mother whether they were currently breastfeeding at the visit when the child was 1 month of age. Child factors determined included sex, ethnicity, birth weight, and behavioral characteristics such as physical activity in hours, index of healthy eating habits, and total daily television (TV) viewing time in hours. The child's sex, ethnicity, and birth weight were reported by the mother during interviews either at the first hospital visit at the time of the child's birth or at the first study home visit when the child was 1 month old. The sample sizes for individual ethnic minority groups were not large enough to allow separate subgroup analyses; thus, ethnicity was dichotomized into White and non-White. The total number of minutes of physical activity ranged from 0 to 515 min (equal to 8.58 h) and was computed on the most recent day of school from the Self-Administered Physical Activity Checklist (SAPAC) that was developed for use in the Child and Adolescent Trial for Cardiovascular Health (CATCH) multisite school-based health promotion study [34]. During the sixth grade, children were asked to complete a questionnaire designed to assess dietary choices. The items on eating habits were slightly modified from the Youth Risk Behavior Survey. Index of healthy eating habits was computed as sum of the responses to four items including: “# times drink fruit juice,” “# times eat raw vegetables,” “# times eat cooked vegetables,” and “# times eat fruit;” the index ranged from 0 to 12 with higher scores indicating more healthy eating habits (Cronbach's alpha = 0.56). Total daily TV time ranged from 0 to 510 min (equal to 8.5 h) and was computed as the sum of before and after school minutes of TV/video watching from SAPAC.
Statistical analysis
Chi-squared (χ2) or t tests were used to compare the characteristics of participants in the analytic sample (n = 917) with the characteristics of subjects in the excluded sample (n = 447). χ2 tests were also used to determine significance for categorical variables (expressed in frequencies with percentage values), and t tests were used to determine the significance for continuous variables (expressed as mean ± standard deviation). Univariate analyses were conducted to examine the relationship between maternal/child factors and childhood overweight/obesity. Factors whose p values were less than 0.20 were considered as potential confounders. Multiple logistic regression analyses were used to adjust for potential confounding and to evaluate the association of C-section and overweight and obesity for children in grade 6. We also examined the association separately for male and female children. Results included 95 % confidence intervals, and p values less than 0.05 were considered statistically significant. All analyses were performed using SAS, version 9.2 (SAS, Inc., Cary, NC).
Results
Table 1 shows the characteristics of participants in the analytic sample, and these are compared to those of subjects that were excluded due to incomplete. Excluded mothers were more likely to have less than a bachelor's degree (p = 0.001), live below the poverty line (p < 0.0001), live single (p = 0.012), and smoke during pregnancy (p = 0.002). There was no significant difference for C-section between the analytic sample and excluded subjects. With respect to child characteristics, there were no significant differences between the analytic and excluded samples, except for sex (50.9 vs. 43.0 % female, respectively, p = 0.006).
Univariate analyses of the associations of delivery mode and maternal and child factors for both childhood overweight and obesity are shown in Table 2. A total of 186 children (20.3 %) were delivered by C-section. Children delivered by C-section, compared to vaginal delivery, were significantly more likely to be overweight (41.4 vs. 32.2 %) and obese (24.7 vs. 17.0 %) (both p < 0.05). Children of mothers who were younger, had less than a bachelor's degree, lived single, were depressed, not breastfeeding, and smoked during pregnancy or children who were non-White and had higher birth weight were at an increased risk for being overweight (all p < 0.05) and obese (all p < 0.05, except for those who smoked during pregnancy). In addition, children who had more total TV watching time in hours daily were more likely to become overweight.
Multiple logistic regression analyses of the association between C-section and the risk of childhood overweight and obesity in grade 6 are presented in Table 3. Compared to children delivered vaginally, children delivered by C-section had approximately twice the likelihood of being overweight (odds ratio (OR) = 1.86, 95 % confidence interval (CI) 1.27–2.73) and obese (OR = 1.87, 95 % CI 1.19–2.95). However, after examining the association separately by child sex, males delivered by C-section had an increased risk for being overweight (OR = 1.78, 95 % CI = 1.01–3.12) and obese (OR = 2.58, 95 % CI = 1.36–4.88), while females delivered by C-section had an increased risk only for being overweight (OR = 1.99, 95 % CI = 1.17–3.39).
Discussion
In this population-based cohort study of 917 mother–child dyads, delivery mode was found to be associated with the risk of both childhood overweight and obesity. However, the relationship between C-section and the risk of childhood overweight status varied by child sex. The observed relationship between C-section and childhood overweight and obesity may be due to adverse outcomes associated with delivery by C-section compared to vaginal delivery. C-section is correlated with increased susceptibility to certain pediatric comorbidities. For example, children delivered by C-section are more likely to develop respiratory (allergies and asthma), autoimmune (type 1 diabetes and celiac disease) [5, 8, 42], and endocrine disorders [16]. The presence of contact at birth with maternal vaginal microbes may compromise the offspring's immune system, leading to greater susceptibility to disease [27]. Infants born by C-section also exhibit a different intestinal microbiota composition in their digestive tracts that may persist into adulthood when compared to vaginally born infants [14, 40]. These obesogenic microbes may influence weight and contribute to higher rates of obesity [18, 24, 38]. For example, C-section-born children have lower counts of Bifidobacteria and higher counts of Clostridium difficile (a potential obesogenic microbiota) than vaginally delivered children [17, 33, 40].
The relationship between delivery mode and obesity has not been explored in depth. Among the few studies that do exist, the findings are inconsistent. Similar to our findings, a few studies have reported an increased prevalence of obesity among young adults and adolescents delivered by C-section as compared to vaginal deliveries [3, 13, 16, 46]. In a recent prospective study, Huh and colleagues found that delivery by C-section doubled the odds of obesity at age 3 when compared to vaginally delivered children after controlling for maternal weight at the time of conception, gestational weight gain, and infant birth weight [16]. These findings are also similar to a longitudinal study of Brazilian children that reported higher odds of obesity among younger children delivered by C-section, although this increased risk did not persist into adolescence [3]. Other longitudinal studies [2, 3] found that delivery mode was not associated with overweight or obesity at any age among females but was found to predict overweight among male cohorts.
This study has several strengths. First, child's height and weight were measured with standardized procedures for calculating objective child's BMI. Second, the NICHD SECCYD had a relatively large sample size which increased the power of our study. Also, this national dataset included information on a broad range of social and health-related variables in a diverse population group which allowed adjustment for many potential confounders. The findings of our study contribute to the sparse evidence on the relationship between C-section and the risk of later childhood overweight and obesity.
As expected, our study had some limitations. It is important to note that our findings may have been influenced by childhood-associated birth cohort trends in obesity. In particular, our study found a considerably higher proportion of overweight and obese children. This finding may be due, in part, to the fact that for the older age groups, the BMI references in the CDC 2000 charts were derived from national surveys of US children as measured from 1963 to 1994 and not to measurements done in the year 2000 as was the case for the youngest age groups. Therefore, the findings may reflect secular trends in changes in BMI among older children when compared to younger cohorts. Despite this concern, the CDC 2000 growth charts provide one of the best reference data available for adiposity [20]. There is the possibility of selection bias due to incomplete data or loss to follow-up. One concern is that the participants in the analytic sample might have higher socioeconomic status and may be at a decreased risk of being overweight or obese [43]. However, no significant difference for delivery mode was found in the analytic and excluded samples. It is widely acknowledged that maternal birth weight and the subsequent alteration of the intrauterine environment are perinatal predictors of fetal growth, offspring BMI, and later obesity [31, 32, 36, 44, 45]. Higher maternal pregravid weight and excessive gestational weight gain have been linked to the delivery of large-for-gestational-age infants and an increased risk for childhood obesity [32, 41]. However, lack of information about these perinatal variables may result in residual confounding, which may explain part of the observed relationship. In addition, breastfeeding status could not be determined as exclusive breastfeeding or mixed breastfeeding due to lack of such information. Finally, the index used for the child's healthy eating habits had only a modest internal reliability indicating some misclassification of this variable.
Conclusions
Children delivered by C-section compared to those delivered vaginally were at an increased risk of being overweight or obese in grade 6. Males delivered by C-section were at an increased risk for being overweight and obese, while females delivered by C-section were at an increased risk for being overweight. Longitudinal studies are needed to examine the long-term effect of delivery mode on the risk of childhood overweight and obesity.
Abbreviations
- CATCH:
-
Child and Adolescent Trial for Cardiovascular Health
- CDC:
-
Centers for Disease Control and Prevention
- CI:
-
Confidence interval
- C section:
-
Cesarean section
- NICHD:
-
National Institute of Child Health and Human Development
- OR:
-
Odds ratio
- SAPAC:
-
Self-Administered Physical Activity Checklist
- SECCYD:
-
Study of Early Child Care and Youth Development
References
Agras WS, Hammer LD, McNicholas F, Kraemer HC (2004) Risk factors for childhood overweight: a prospective study from birth to 9.5 years. J Pediatr 145:20–25
Ajslev TA, Andersen CS, Gamborg M, Sørensen TI, Jess T (2011) Childhood overweight after establishment of the gut microbiota: the role of delivery mode, pre-pregnancy weight and early administration of antibiotics. Int J Obes 35:522–529
Barros FC, Matijasevich A, Hallal PC et al (2012) Cesarean section and risk of obesity in childhood, adolescence, and early adulthood: evidence from 3 Brazilian birth cohorts. Am J Clin Nutr 95:465–470
Betrán AP, Merialdi M, Lauer JA et al (2007) Rates of caesarean section: analysis of global, regional and national estimates. Paediatr Perinat Epidemiol 21:98–113
Cardwell CR, Stene LC, Joner G et al (2008) Caesarean section is associated with an increased risk of childhood-onset type 1 diabetes mellitus: a meta-analysis of observational studies. Diabetologia 51:726–735
Centers for Disease Control and Prevention (2011) National diabetes fact sheet: national estimates and general information on diabetes and prediabetes in the United States. U.S. Department of Health and Human Services, Atlanta
Daniels SR, Arnett DK, Eckel RH et al (2005) Overweight in children and adolescents: pathophysiology, consequences, prevention, and treatment. Circulation 111:1999–2002
Decker E, Engelmann G, Findeisen A et al (2010) Cesarean delivery is associated with celiac disease but not inflammatory bowel disease in children. Pediatrics 125:e1433–e1440
Flegal KM, Carroll MD, Ogden CL, Curtin LR (2010) Prevalence and trends in obesity among US adults, 1999–2008. JAMA 303:235–241
Freedman DS, Khan LK, Serdula MK et al (2005) The relation of childhood BMI to adult adiposity: the Bogalusa Heart Study. Pediatrics 115:22–27
Freedman DS, Zuguo M, Srinivasan SR, Berenson GS, Dietz WH (2007) Cardiovascular risk factors and excess adiposity among overweight children and adolescents: the Bogalusa Heart Study. J Pediatr 150:12–17
Gillman MW, Rifas-Shiman SL, Kleinman K, Oken E, Rich-Edwards JW, Taveras EM (2008) Developmental origins of childhood overweight: potential public health impact. Obesity (Silver Spring) 16:1651–1656
Goldani HA, Bettiol H, Barbieri MA et al (2011) Cesarean delivery is associated with an increased risk of obesity in adulthood in a Brazilian birth cohort study. Am J Clin Nutr 93:1344–1347
Grönlund MM, Lehtonen OP, Eerola E, Kero P (1999) Fecal microflora in healthy infants born by different methods of delivery: permanent changes in intestinal flora after cesarean delivery. J Pediatr Gastroenterol Nutr 28:19–25
Hamilton BE, Martin JA, Ventura SJ (2010) Births: preliminary data for 2009. National vital statistics report. National Center for Health, Hyattsville
Huh SY, Rifas-Shiman SL, Zera CA et al (2012) Delivery by caesarean section and risk of obesity in preschool age children: a prospective cohort study. Arch Dis Child 97:610–616
Huurre A, Kalliomaki M, Rautava S, Rinne M, Salminen S, Isolauri E (2008) Mode of delivery effects on gut microbiota and humoral immunity. Neonatol 93:236–240
Kalliomäki M, Collado MC, Salminen S, Isolauri E (2008) Early differences in fecal microbiota composition in children may predict overweight. Am J Clin Nutr 87:534–538
Kamath BD, Todd JK, Glazner JE, Lezotte D, Lynch AM (2009) Neonatal outcomes after elective cesarean delivery. Obstet Gynecol 113:1231–1238
Krebs NF, Himes JH, Jacobson D, Nicklas TA, Guilday P, Styne D (2007) Assessment of child and adolescent overweight and obesity. Pediatrics 120(Suppl 4):S193–228
Kuczmarski RJ, Ogden CL, Guo SS et al (2002) 2000 CDC growth charts for the United States: methods and development. Natl Cent Health Stat Vital Health Stat 11(246):1–190
Kushi LH, Byers T, Doyle C et al (2006) American Cancer Society guidelines on nutrition and physical activity for cancer prevention: reducing the risk of cancer with healthy food choices and physical activity. CA Cancer J Clin 56:254–281
Li C, Ford ES, Zhao G, Mokdad AH (2009) Prevalence of pre-diabetes and its association with clustering of cardiometabolic risk factors and hyperinsulinemia among US adolescents: NHANES 2005–2006. Diabetes Care 32:342–347
Luoto R, Kalliomäki M, Laitinen K et al (2011) Initial dietary and microbiological environments deviate in normal-weight compared to overweight children at 10 years of age. J Pediatr Gastroenterol Nutr 52:90–95
Modi N, Steer P (2009) Elective caesarean sections—risks to infants. Lancet 374:665–667
National Institute of Child Health and Human Development Early Child Care Research Network (2001) Child care and common communicable illnesses: results from the National Institute of Child Health and Human Development Study of Early Child Care. Arch Pediatr Adolesc Med 155(4):481–488
Neu J, Rushing J (2011) Cesarean versus vaginal delivery: long-term infant outcomes and the hygiene hypothesis. Clin Perinatol 38:321–331
Office of the Surgeon General (2010) The surgeon general's vision for a healthy and fit nation. U.S. Department of Health and Human Services, Rockville
Ogden CL, Carroll MD, Curtin LR, Lamb MM, Flegal KM (2010) Prevalence of high body mass index in US children and adolescents, 2007–2008. JAMA 303:242–249
Ogden CL, Kuczmarski RJ, Flegal KM et al (2002) Centers for Disease Control and Prevention 2000 growth charts for the United States: improvements to the 1977 National Center for Health Statistics version. Pediatrics 109:45–60
Oken E, Gillman MW (2003) Fetal origins of obesity. Obes Res 11:496–506
Oken E, Taveras EM, Kleinman KP, Rich-Edwards JW, Gillman MW (2007) Gestational weight gain and child adiposity at age 3 years. Am J Obstet Gynecol 196(4):e1–8, 322
Penders J, Thijs C, Vink C et al (2006) Factors influencing the composition of the intestinal microbiota in early infancy. Pediatrics 118:511–521
Perry CL, Stone EJ, Parcel GS et al (1990) School-based cardiovascular health promotion: child and adolescent trial for cardiovascular health. J Sch Health 60:406–413
Radloff LS (1977) The CES-D scale: a self-report depression scale for research in the general population. Appl Psychol Meas 1:385–401
Reilly JJ, Armstrong J, Dorosty AR et al (2005) Early life risk factors for obesity in childhood: cohort study. BMJ 330:1357
Reilly JJ, Methven E, McDowell Z et al (2003) Health consequences of obesity. Arch Dis Child 88:748–752
Reinhardt C, Reigstad CS, Bäckhed F (2009) Intestinal microbiota during infancy and its implications for obesity. J Pediatr Gastroenterol Nutr 48:249–256
Rhodes SK, Shimoda KC, Waid LR et al (1995) Neurocognitive deficits in morbidly obese children with obstructive sleep apnea. J Pediatr 127:741–744
Salminen S, Gibson GR, McCartney AL, Isolauri E (2004) Influence of mode of delivery on gut microbiota composition in seven year old children. Gut 53:1388–1389
Tanentsapf I, Heitmann BL, Adeqboye AR (2011) Systematic review of clinical trials on dietary interventions to prevent excessive weight gain during pregnancy among normal weight, overweight, and obese women. BMC Pregnancy Childbirth 26:81
Thavagnanam S, Fleming J, Bromley A, Shields MD, Cardwell CR (2008) A meta-analysis of the association between caesarean section and childhood asthma. Clin Exp Allergy 38:629–633
Wang Y (2001) Cross-national comparison of childhood obesity: the epidemic and the relationship between obesity and socioeconomic status. Int J Epidemiol 30:1129–1136
Whitaker RC, Dietz WH (1998) Role of the prenatal environment in the development of obesity. J Pediatr 132:768–776
Whitaker RC, Wright JA, Pepe MS, Seidel KD, Dietz WH (1997) Predicting obesity in young adulthood from childhood and parental obesity. N Engl J Med 337:869–873
Zhou L, He G, Zhang J, Xie R, Walker M, Wen SW (2011) Risk factors of obesity in preschool children in an urban area in China. Eur J Pediatr 170:1401–1406
Acknowledgments
This study was conducted by the NICHD Early Child Care Research Network supported by NICHD through a cooperative agreement that calls for scientific collaboration between the grantees and the NICHD staff. The East Tennessee State University have restricted data use agreements to analyze the SECCYD data.
Conflict of interest
The authors have no disclosures of competing interests.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Wang, L., Alamian, A., Southerland, J. et al. Cesarean section and the risk of overweight in grade 6 children. Eur J Pediatr 172, 1341–1347 (2013). https://doi.org/10.1007/s00431-013-2043-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00431-013-2043-2