
Abstract
The aim of this study was to investigate levels of clustered cardiometabolic risk and the odds of being ‘at risk’ according to cardiorespiratory fitness status in children. Data from 88 10–11.9-year-old children (mean age 11.05 ± 0.51 years), who participated in either the REACH Year 6 or the Benefits of Fitness Circuits for Primary School Populations studies were combined. Waist circumference, systolic blood pressure, diastolic blood pressure, glucose, triglycerides, high-density lipoprotein cholesterol, adiponectin and C-reactive protein were assessed and used to estimate clustered cardiometabolic risk. Participants were classified as ‘fit’ or ‘unfit’ using recently published definitions (46.6 and 41.9 mL/kg/min for boys and girls, respectively), and continuous clustered risk scores between fitness groups were assessed. Participants were subsequently assigned to a ‘normal’ or ‘high’ clustered cardiometabolic risk group based on risk scores, and logistic regression analysis assessed the odds of belonging to the increased cardiometabolic risk group according to fitness. The unfit group exhibited significantly higher clustered cardiometabolic risk scores (p < 0.001) than the fit group. A clear association between fitness group and being at increased cardiometabolic risk (B = 2.509, p = 0.001) was also identified, and participants classed as being unfit were found to have odds of being classified as ‘at risk’ of 12.30 (95 % CI = 2.64–57.33).
Conclusion Assessing cardiorespiratory fitness is a valid method of identifying children most at risk of cardiometabolic pathologies. The ROC thresholds could be used to identify populations of children most at risk and may therefore be used to effectively target a cardiometabolic risk-reducing public health intervention.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Adverse cardiometabolic risk factors are associated with an increased risk of cardiovascular disease-related morbidity and mortality in adults [12, 24, 29]. Cardiovascular disease is a pathological process that begins in childhood [26], and children with established adverse risk profiles already show markers of subclinical cardiovascular disease [21]. Cardiometabolic risk factors that originate in childhood and increase the risk of early morbidity and mortality such as obesity, hypertension, insulin resistance and dyslipidaemia track from childhood into adulthood [18, 23]. In the current era when cardiovascular disease-associated morbidity and mortality represents a significant disease burden worldwide [20], the early detection of children with increased cardiometabolic risk factors would therefore be extremely beneficial. Such early detection would allow the introduction of targeted interventions aimed at reducing cardiometabolic risk in children and subsequent morbidity.
Cardiorespiratory fitness (CRF) is a key determinant of health, and emerging evidence describes a direct relationship between poor CRF and increased cardiometabolic risk in children [4, 5, 13]. Worryingly, levels of CRF have declined in children in recent years, suggesting that more children may be at cardiometabolic risk than in previous decades [9]. CRF assessments could offer a valid and pragmatic method of accurately estimating cardiometabolic risk in the paediatric population. Furthermore, CRF has potential as a method of stratifying children into groups that may require further investigation and intervention [1].
A recent study by Boddy et al. [10] developed receiver operating characteristic (ROC)-generated thresholds for CRF related to obesity in 10–11.9-year-old children. The thresholds provided cutpoints for field-assessed CRF using a 20-m multi-stage shuttle run test (20mSRT) and also detailed equivalent VO2peak thresholds. When the cutpoints were applied in an independent population of adolescents, participants classified as unfit demonstrated significantly increased clustered cardiometabolic risk scores in comparison to those classified as fit [10]. The paper highlighted the potential utility of using CRF values or scores to identify children and adolescents as at increased cardiometabolic risk. To date, these thresholds have not been applied to primary school-aged children or used to calculate the odds of children being classified as ‘at risk’ of cardiometabolic disease. This type of analysis is particularly important as it has the potential to provide a method for non-invasively identifying children at risk of cardiometabolic disease. This would be particularly beneficial in clinical settings where detecting children at risk of cardiometabolic disease as early as possible is vital to facilitate effective, timely and targeted risk-reducing intervention. Furthermore, CRF assessments can be conducted on a large scale, therefore offering an opportunity to screen for ‘at risk’ children at the population level.
The aim of this study was therefore to investigate levels of clustered cardiometabolic risk and the odds of being ‘at risk’ according to fitness status in 10–11.9-year-old schoolchildren classified using published ROC-generated CRF thresholds.
Materials and methods
Data were generated by the REACH Year 6 study based in Liverpool, UK, and the Benefits of Fitness Circuits for Primary School Populations study based in western Scotland, UK.
REACH Y6 study
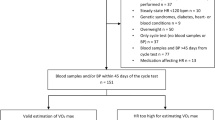
After gaining informed parental consent, participant assent and medical screening, 62 10–11.9-year-old participants agreed to take part in the study in summer 2010. Prior to recruitment, institutional ethical approvals for all procedures were received; in addition, Local Research Ethics Committee approvals were received for blood sampling protocols and analysis that involved the local Children’s Foundation NHS Trust. The participants attended the laboratories on one occasion to complete assessments of anthropometrics, blood pressure and cardiorespiratory fitness and one school-based blood sampling morning.
Laboratory measures
Stature (Seca Ltd., Birmingham, UK) to the nearest 0.1 cm and body mass to the nearest 0.1 kg (Seca Ltd. Birmingham, UK) were assessed using standard techniques [22]. Waist circumference was measured by passing a non-elastic anthropometric tape around the mid-point between the bottom of the ribs and the iliac crest. Blood pressure (BP) was assessed once after a 15-min rest period with the participant in a supine position (GE DINAMAP ProCare 100–400 Series, UK). Cardiorespiratory fitness (peak oxygen uptake (VO2peak)) was assessed using an individually calibrated, continuous incremental treadmill (H P Cosmos, Traunstein, Germany) test to volitional exhaustion using breath-by-breath gas analysis (Jaeger Oxycon Pro, Viasys Health Care, Warwick, UK). All participants wore a heart rate monitor (Polar, Kempele, Finland) throughout. To account for differences in biological age and limb length, VO2peak test speeds were individually calibrated by anchoring treadmill speeds to set Froude (Fr) numbers. This approach has been described previously (please refer to [17] for further information). Peak VO2 was defined as the highest 15-s average oxygen uptake achieved during the test when participants reached volitional exhaustion, and the subjective endpoints were met (respiratory exchange ratio > 1.05 and/or HR > 199 beats/min).
Blood sampling morning
The participants attended one blood sampling morning at their school site. After verbal confirmation of overnight fast, samples were drawn from the vena antecubitus by one experienced phlebotomist. Samples were taken between 8:30 and 10:30 am and were transported to the pathology laboratories at the local Children’s Foundation NHS Trust for analysis.
Fitness circuits for primary school populations study
After gaining informed parental consent and participant assent, 55 10–11.9-year-old participants were involved in this study, which was conducted in 2011. Prior to recruitment, ethical approval was received from the University of the West of Scotland Ethics Committee. Testing sessions occurred in school sites on two separate occasions: all fitness, anthropometric and blood pressure measurements were taken on day 1, and blood sampling was conducted 2 days later.
Stature was measured to the nearest 0.1 cm (Seca Stadiometer, Seca Ltd., Birmingham, UK). Body mass was measured to the nearest 0.1 kg using calibrated electronic weighing scales (Seca 880, Digital Scales, Seca Ltd., Birmingham, UK). Waist circumference was measured at the mid-point between the lower ribs and the iliac crest. Blood pressure was measured once with an automated monitor (Omron M10-IT Blood Pressure Monitor HEM-7080IT-E, Omron Healthcare UK Ltd., Milton Keynes, UK) after each participant had sat quietly for a period of 10 min [11]. Cardiorespiratory fitness (CRF) was estimated using the 20-m multi-stage shuttle runs test (20mSRT) [19]. VO2peak was calculated using 20mSRT score using previously validated, widely used equations [19].
Blood sampling
Blood samples were collected between 9:00 and 11:00 am by two experienced paediatric phlebotomists after an overnight fast in all participants. Blood samples were obtained from an antecubital vein, and analyses were subsequently completed within 5 months from collection.
Clustered cardiometabolic risk
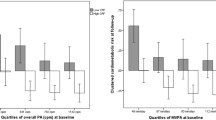
The following variables from both studies were used in the present study to estimate clustered cardiometabolic risk: waist circumference, systolic blood pressure (SBP), diastolic blood pressure (DBP), glucose, triglycerides, high-density lipoprotein cholesterol (HDL), adiponectin and C-reactive protein (CRP). Data were examined for normality by sex, and the following variables were normalised by log transformation: waist circumference, SBP (boys only), DBP (boys only), glucose (boys only), triglycerides, adiponectin and CRP. Adiponectin and HDL were inverted using a constant of −1, and standardised z-scores were calculated separately by sex for the risk score components. These z-scores were then summed to create a continuous risk score. This method of estimating cardiometabolic risk has been used for numerous times within paediatric exercise science research, including the European Youth Heart Study [3, 6]. Selection of risk variables was based on the International Diabetes Federation’s definition for metabolic syndrome [2], with both CRP and adiponectin included as potent markers of cardiovascular disease risk [15, 28].
Statistical analysis
Participants were classified as ‘fit’ or ‘unfit’ using recently published definitions (46.6 and 41.9 mL/kg/min for boys and girls, respectively) [10]. Analysis of covariance (ANCOVA) was completed to assess differences in continuous clustered risk score between the fitness groups, controlling for age and sex. Following ANCOVA analysis, participants were assigned to a ‘normal’ or ‘high’ clustered cardiometabolic risk group, with increased risk defined as ≥1 SD in risk score above the pooled (boys and girls) mean. This method has been used previously in similarly aged children [4, 6, 16]. Logistic regression analysis was used to assess the odds of belonging to the increased risk group according to fitness status (low fit vs fit). All analyses were completed using SPSS V20.0 (SPSS Statistics, IBM Corp.), and an alpha value of p ≤ 0.05 was used to denote statistical significance.
Results
Eighty-eight participants (42 girls, 46 boys) had complete data for all clustered risk components and VO2peak. Table 1 displays the descriptive characteristics for anthropometrics, VO2peak and risk score components by sex. Girls were less fit and had higher body mass, body mass index and triglyceride values than boys.
In total, 18 participants were classed as ‘unfit’; ANCOVA analysis revealed that the unfit group exhibited significantly higher clustered cardiometabolic risk scores in comparison to the fit group after controlling for sex and decimal age (estimated marginal mean risk score fit group = −0.63, SE = 0.37; unfit group mean = 2.74, SE = 0.75; F = 15.83, p < 0.001). Participants with a clustered risk score of ≥3.25 (unadjusted mean plus 1 SD) were classed as ‘at risk’. Fourteen participants were classified as ‘at risk’. Logistic regression found an association between fitness group and being ‘at risk’ (B = 2.509, p = 0.001) after controlling for age and sex. For participants classed as ‘unfit’, the odds of being classified as ‘at risk’ were 12.30 (95 % CI = 2.64–57.33) in comparison to those classed as fit.
Discussion
The aim of this study was to investigate levels of clustered cardiometabolic risk and the odds of being ‘at risk’ according to fitness status in 10–11.9-year-old schoolchildren classified using recently published ROC-generated CRF thresholds. Importantly, the results of this study showed that the unfit group (VO2peak <46.6 and <41.9 mL/kg/min for boys and girls, respectively) exhibited significantly higher clustered cardiometabolic risk scores in comparison to the fit group (p < 0.001), and for participants classed as ‘unfit’, the odds of being classified as ‘at risk’ were 12.30 (95 % CI = 2.64–57.33). As cardiorespiratory fitness represents the capacity of the respiratory and cardiovascular systems [25], these findings are somewhat intuitive. The association between CRF and clustered cardiometabolic risk likely reflects the broad physiological effects of regular physical activity and adequate CRF including cardiovascular (structural and functional), metabolic (including energy balance) and hormonal parameters [8]. Though some debate exists surrounding fitness levels in children due to the influence of maturation and genetics, it is possible to improve levels of CRF in children if the physical activity stimulus is of sufficient intensity, frequency and duration [7].
Increasing cardiometabolic risk in the paediatric population is a global concern [20], and evidence demonstrates that risk factors for cardiometabolic disease track from childhood to adulthood [18]. In order to effectively manage and reduce this public health problem, the introduction of targeted health interventions for the ‘at risk’ groups is of crucial importance. This is particularly so when the treatment of children exhibiting cardiometabolic risk has been found to be more effective than the treatment of adults [14]. The findings of the present study are of significant clinical importance as they provide further evidence of the strong association between CRF and cardiometabolic disease risk in children. Furthermore, this study lends support to the use of the published CRF thresholds [10] as a method of identifying children at risk of cardiometabolic disease before clinical manifestations are apparent. These data provide a significant contribution towards the development of a valid risk stratification tool to identify children that may benefit from a health intervention aimed at reducing their cardiometabolic risk profile.
Clustered cardiometabolic risk scores for children have been successfully calculated in previous studies [3, 6, 16]. Composite risk scores may be more representative of the constellation of disturbances associated with cardiometabolic disease [6], are less sensitive to daily changes in individual risk markers and may provide a better estimate of risk than individual markers [6, 16]. Despite these advantages, the data required to calculate clustered risk scores are labour intensive, invasive and costly to obtain, therefore limiting the appropriateness of these scores for assessing risk in children on a large scale. Our findings suggest that CRF provides an accurate representation of cardiometabolic risk that could feasibly be measured on a large scale, for example, using a 20-m multi-stage shuttle run test [9, 27].
This study is limited by a number of factors. Primarily, the data were merged from two studies, and although procedures were very similar across the studies they were not standardised. However, the range of markers included in the study is difficult to assess on a large scale; therefore, data were combined for compatible variables to maximise statistical power and ensure that these valuable data were utilised to their maximum potential. Secondly, CRF was measured using the 20mSRT in the Fitness Circuits for Primary School Populations, and VO2peak was estimated using equations [19] rather than directly assessed via treadmill VO2peak protocol. Despite this, the equations used to calculate VO2peak from 20mSRT scores have been widely used and are validated for use in this age group of children [19]. Furthermore, direct assessments of VO2peak require specialised equipment and are time-consuming; therefore, 20mSRT assessments may be more feasible for use on a large scale. Finally, the composite clustered risk score assumes equal risk rating for each component, and 1 SD above the mean was used to signify ‘at risk’. Whether this value actually represents risk clinically is open to debate, but in the absence of published cutpoints for clustered cardiometabolic risk, this was deemed the most appropriate method and has been previously used in studies assessing clustered cardiometabolic risk in children [4, 6].
The major strength of this study is the range of measures included within the clustered risk score, which include emerging risk markers such as adiponectin and CRP, as well as more established functional (BP) and metabolic variables. Furthermore, this is the first study to apply the recently published ROC cutpoints for CRF in similarly aged children [10] and lend support to their use as a tool to identify children at risk of cardiometabolic disease. Further studies should aim to develop similar cutpoints across the age range.
Conclusions
The findings of this study suggest that CRF could potentially be used as a valid method of identifying children most at risk of cardiometabolic pathologies. The ROC thresholds could be used to identify the populations of children who stand to benefit the most from a targeted cardiometabolic risk-reducing public health intervention.
References
Adegboye AR, Anderssen SA, Froberg K, Sardinha LB, Heitmann BL, Steene-Johannessen J, Kolle E, Andersen LB (2011) Recommended aerobic fitness level for metabolic health in children and adolescents: a study of diagnostic accuracy. Br J Sport Med 45:722–728
Alberti KG, Zimmet P, Shaw J (2005) The metabolic syndrome—a new worldwide definition. Lancet 366:1059–1062
Andersen L, Sardinha L, Froberg K, Riddoch C, Page A, Andersen S (2008) Fitness, fatness and clustering of cardiovascular risk factors in children from Denmark, Estonia and Portugal: the European Youth Heart Study. Int J Pediatr Obes 3:58–66
Andersen LB, Hasselstrom H, Gronfeldt V, Hansen SE, Karsten F (2004) The relationship between physical fitness and clustered risk, and tracking of clustered risk from adolescence to young adulthood: eight years follow-up in the Danish Youth and Sport Study. Int J Behav Nutr Phys Act 1:6
Anderssen SA, Cooper AR, Riddoch C, Sardinha LB, Harro M, Brage S, Andersen LB (2007) Low cardiorespiratory fitness is a strong predictor for clustering of cardiovascular disease risk factors in children independent of country, age and sex. Eur J Cardiovasc Prev Rehabil: Off J Eur Soc Cardiol, Work Group Epidemiol Prev Cardiac Rehabil Exerc Physiol 14:526–531
Bailey DP, Boddy LM, Savory LA, Denton SJ, Kerr CJ (2012) Associations between cardiorespiratory fitness, physical activity and clustered cardiometabolic risk in children and adolescents: the HAPPY study. Eur J Pediatr 171:1317–1323
Baquet G, van Praagh E, Berthoin S (2003) Endurance training and aerobic fitness in young people. Sport Med 33:1127–1143
Blair SN, Kohl HW, Gordon NF, Paffenbarger RSJ (1992) How much physical activity is good for health? Annu Rev Public Health 13:99–126
Boddy LM, Fairclough SJ, Atkinson G, Stratton G (2012) Changes in cardiorespiratory fitness in 9- to 10.9-year-old children: SportsLinx 1998–2010. Med Sci Sport Exerc 44:481–486
Boddy LM, Thomas NE, Fairclough SJ, Tolfrey K, Brophy S, Rees A, Knox G, Baker JS, Stratton G (2012) ROC generated thresholds for field-assessed aerobic fitness related to body size and cardiometabolic risk in schoolchildren. PLoS One 7:e45755
Buchan DS, Ollis S, Young JD, Thomas NE, Cooper SM, Tong TK, Nie J, Malina RM, Baker JS (2011) The effects of time and intensity of exercise on novel and established markers of CVD in adolescent youth. Am J Hum Biol 23:517–526
Doshi KB, Kashyap SR, Brennan DM, Hoar BM, Cho L, Hoogwerf BJ (2009) All-cause mortality risk predictors in a preventive cardiology clinic cohort-examining diabetes and individual metabolic syndrome criteria: a PRECIS database study. Diabetes Obes Metabol 11:102–108
Eisenmann JC (2007) Aerobic fitness, fatness and the metabolic syndrome in children and adolescents. Acta Paediatr 96:1723–1729
Epstein L, Valoski A, Kalarchian M, McCurley J (1995) Do children lose and maintain weight easier than adults: a comparison of child and parent weight changes from six months to ten years. Obes Res 3:411–417
Giannessi D, Maltinti M, Del Ry S (2007) Adiponectin circulating levels: a new emerging biomarker of cardiovascular risk. Pharmacol Res: Off J Ital Pharmacol Soc 56:459–467
Gobbi R, Davies IG, Fairclough SJ, Mackintosh KA, Warburton GL, Stratton G, George KP, Hackett AF, Boddy LM (2012) Clustered cardiometabolic risk, cardiorespiratory fitness and physical activity in 10–11 year-old children. The CHANGE! project baseline. Arch Exerc Health Dis 3:207–213
Hopkins N, Stratton G, Maia J, Tinken TM, Graves LE, Cable NT, Green DJ (2010) Heritability of arterial function, fitness, and physical activity in youth: a study of monozygotic and dizygotic twins. J Pediatr 157:943–948
Katzmarzyk PT, Perusse L, Malina RM, Bergeron J, Despres JP, Bouchard C (2001) Stability of indicators of the metabolic syndrome from childhood and adolescence to young adulthood: the Quebec Family Study. J Clin Epidemiol 54:190–195
Leger LA, Mercier D, Gadoury C, Lambert J (1988) The multistage 20 metre shuttle run test for aerobic fitness. J Sports Sci 6:93–101
Lloyd-Jones D, Adams R, Carnethon M, De Simone G, Ferguson TB, Flegal K, Ford E et al (2009) Heart disease and stroke statistics—2009 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation 119:480–486
Lobelo F, Pate RR, Dowda M, Liese AD, Daniels SR (2010) Cardiorespiratory fitness and clustered cardiovascular disease risk in US adolescents. J Adolesc Heal 47:352–359
Lohman T, Roche AF, Martorell R (1988) Anthropometric standardization reference manual. Human Kinetics, Champaign
Morrison JA, Friedman LA, Wang P, Glueck CJ (2008) Metabolic syndrome in childhood predicts adult metabolic syndrome and type 2 diabetes mellitus 25 to 30 years later. J Pediatr 152:201–206
Reppert A, Steiner BF, Chapman-Novakofski K (2008) Prevalence of metabolic syndrome and associated risk factors in Illinois. Am J Health Promot: AJHP 23:130–138
Ruiz J, Ortega F, Rizzo N, Villa I, Hurtig-Wennlof A, Oja L, Sjöström M (2007) High cardiovascular fitness is associated with low metabolic risk score in children: the European Youth Heart Study. Pediatr Res 61:350–355
Stary HC (1989) Evolution and progression of atherosclerotic lesions in coronary arteries of children and young adults. Arteriosclerosis 9:I19–I32
Stratton G, Canoy D, Boddy LM, Taylor SR, Hackett AF, Buchan IE (2007) Cardiorespiratory fitness and body mass index of 9–11-year-old English children: a serial cross-sectional study from 1998 to 2004. Int J Obes 31:1172–1178
Thomas NE, Baker JS, Graham MR, Cooper SM, Davies B (2008) C-reactive protein in schoolchildren and its relation to adiposity, physical activity, aerobic fitness and habitual diet. Br J Sport Med 42:357–360
Wang J, Ruotsalainen S, Moilanen L, Lepisto P, Laakso M, Kuusisto J (2007) The metabolic syndrome predicts cardiovascular mortality: a 13-year follow-up study in elderly non-diabetic Finns. Eur Hear J 28:857–864
Acknowledgments
We would like to thank all the schools, parents, participants and research teams involved in the REACH Y6 and the Fitness Circuits for Primary School Populations studies. We would also like to thank Nicola Lyons (phlebotomist), Dr. Marcus Auth, Paul Newland and Dr. Jeff Jones from Alder Hey Children’s NHS Foundation Trust. The REACH Y6 study was funded by Liverpool John Moores University. The Benefits of Fitness Circuits for Primary School Populations was funded by the University of the West of Scotland.
Conflict of interest
The research team confirm that there are no conflicts of interest for the current study.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Houston, E.L., Baker, J.S., Buchan, D.S. et al. Cardiorespiratory fitness predicts clustered cardiometabolic risk in 10–11.9-year-olds. Eur J Pediatr 172, 913–918 (2013). https://doi.org/10.1007/s00431-013-1973-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00431-013-1973-z