
Abstract
The school day offers several different time periods that provide varying opportunities for sedentary time (SED) and engagement in physical activity (PA), yet little is known about the PA and sedentary behaviour patterns of boys and girls during these times. The volume, intensity and temporal distributions of SED and PA undertaken by 135 schoolchildren aged 10–14 years, during different segments of the school day: (a) school transport, (b) morning recess, (c) lunch break, (d) class time and (e) after school, were explored using triaxial accelerometry. PA was categorised into SED, light PA (LPA), moderate PA (MPA) and vigorous PA (VPA). Girls engaged in significantly more SED and LPA than boys during recess and lunch break (p < 0.05), while boys engaged in significantly higher levels of VPA during recess (p < 0.001) and MPA and VPA during lunch break (p < 0.001). PA engagement was similar between sexes during other segments of the day. Conclusion: PA patterns appear more beneficial for health in boys during less structured school-based time periods and interventions may therefore target opportunities for girls to be physically active during these times to overcome this observed sex deficit.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The prevalence of childhood obesity has reached epidemic proportions in the UK [39], as well as in other European countries [46] and the US [30]. Despite significant investment in research and changes in policy making, there have been no signs of decline in childhood obesity levels in recent years [30, 39]. In children, overweight and obesity may predispose to dyslipidaemia, hypertension, impaired glucose metabolism and low cardiorespiratory fitness (CRF) [2, 7], and each of these risk factors may confer poor cardiometabolic health and associated co-morbidities in later life [27, 45].
The causes of overweight and obesity are varied and complex, but at population level, are consistent with sustained positive energy balance that may be a result of sedentary behaviour and low levels of physical activity (PA) [40]. Guidelines for health thus recommend that young people engage in at least 60 min per day of moderate-to-vigorous PA (MVPA) and that time spent being sedentary (SED) should be minimised [13]. However, there is debate as to whether children are sufficiently active to benefit their health and prevalence values for sufficiently active youth range between 1 and 100 % when assessed using accelerometry [11, 15, 32] and recent data suggest that only 32 % of boys and 24 % of girls in England aged 2–15 years typically meet the government’s recommended guidelines [12]. Although variations in reported PA levels may be due in part to discrepancies in methods of accelerometry data analysis [15], these findings advocate the need for a greater insight into young people’s PA patterns to more effectively tailor PA promotion strategies in this population.
The school day offers several opportunistic time periods (e.g. school transport, morning recess, lunch break, class time and after school) for youth to be physically active through informal play, sport and active commuting. There is considerable evidence that demonstrates sex differences in PA levels, with boys typically engaging in more habitual PA than girls [12, 32]. However, little is known about the PA patterns of boys and girls during segments of the school day, and, more specifically, their engagement in different subcomponents of the PA intensity continuum, i.e. SED, light PA (LPA), moderate PA (MPA) and vigorous PA (VPA). Given that the magnitude of the association between PA and some health outcomes are intensity driven [13], it is of paramount importance to gain an insight into which segments of the day may benefit from strategies to reduce sedentary behaviour and increased engagement in MPA and VPA.
Accelerometers may permit greater accuracy and precision than self-report measures and pedometers [1, 16] and allow analysis and interpretation of PA patterns and intensity across various segments of the day. Accelerometry-based studies to date investigating PA patterns typically report on total PA [34], combined MVPA [19] or only selected PA subcomponents, e.g. only SED and VPA [41]. In addition, these studies have also focused on average weekday and weekend day PA [34], hourly patterns [41] or in- and out-of-school time periods [19] as opposed to specific segments of the day. These investigations have suggested that both in- and out-of-school hours are important times for youths to engage in PA. However, the patterns of children’s engagement in different PA intensities during specific segments of the school day remains unclear, nor is it understood which segments of the day boys and girls differ in their PA intensity engagement. Furthermore, PA levels may be influenced by cardiorespiratory fitness (CRF) [21] and adiposity [5] and many past studies have failed to adjust for these important covariates when investigating the pattern and volume of boys’ and girls’ PA levels during the school day [29, 44]. Quantifying and adjusting for the potential effects of these variables would strengthen our understanding of any observed sex differences in PA levels.
The primary aim of this study was therefore to utilise accelerometry to explore the volume and patterns of 10–14-year-old boys’ and girls’ engagement in SED, LPA, MPA and VPA during different segments of the school day: (a) school transport, (b) morning recess, (c) lunch break, (d) class time and (e) after school. The secondary aim of this study was to explore boys’ and girls’ compliance with recommendations for MVPA during recess and lunch breaks.
Methodology
Sample
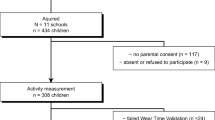
The 135 participants (78 girls) included were part of the HAPPY (Health and Physical activity Promotion in Youth) study. This school-based study explored the effects of three interventions on PA levels and health outcomes in 10–14-year-old schoolchildren. Participants were recruited on a voluntary basis from 11 schools across Bedfordshire, UK and their baseline data used for analyses in the present study. Participants were excluded if they had any contraindications to taking part in physical exercise. The study was approved by the University of Bedfordshire ethics review board. Written informed consent was obtained from participants’ parents and verbal assent from the participants before any testing procedures.
Measurements
Age was recorded as a decimal value for each participant using date of birth. Ethnicity was recorded as white or non-white. A score for socioeconomic status (SES) was attributed to each participant using home postcode and the 2007 Indices of Multiple Deprivation (IMD) [18, 26]. Postcodes were converted into IMD scores using the GeoConvert application [26]. These scores were categorised into tertiles with the lowest tertile indicating the most deprived.
Stature was recorded to the nearest 0.5 cm using the portable Leicester Height Measure (Seca, Birmingham). Body mass was recorded to the nearest 0.1 kg and body fat % (BF%) recorded to the nearest 0.1 % using the Tanita BC-418® Segmental Body Composition Analyzer (Tanita Corp., Tokyo). To determine CRF, participants completed an age- and sex-specific all-out progressive cycle ergometer test to exhaustion using a previously validated protocol [31]. Briefly, workloads increased every 3 min until the participant was no longer able to continue. A maximal effort was deemed as a final heart rate ≥ 185 beats per min (bpm) and subjective observation from the researcher that the child could not continue. Power output (watts) was calculated as being equal to W 1 + (W 2 · t/180), where W 1 is work rate at fully completed stage, W 2 is the work rate increment at final incomplete stage, and t is time in seconds at final incomplete stage. VO2max was calculated using previously described formula [31] and expressed relative to body mass (millilitres per kilogramme per minute).
RT3® triaxial accelerometers (Stayhealthy, Inc., Monrovia, CA) were used to measure seven consecutive days of habitual PA using minute-by-minute sampling. Total minutes and proportion of total time (to account for variations in the length of daily wear time between participants) spent in each segment of the school day was determined for SED (<288 counts per min [cpm]), LPA (288–969 cpm), MPA (970–2,332 cpm), and VPA (≥2,333 cpm). PA intensity cutoff points were based on previously published literature in which the RT3® triaxial accelerometer was validated against oxygen consumption (r = 0.87) in children [37]. Participants were only included for data analysis if they had worn the accelerometer for a minimum of three school days [25] and acquired a minimum daily wear time of 9 h [25]. Sustained 10-min periods of zero counts were removed during the recoding process.
The segments of the school day analysed were (a) school transport (the 30-min time period prior to school starting time), (b) morning recess, which ranged from 15 to 20 min in duration, (c) lunch break, which ranged from 45 to 65 min in duration, (d) class time (typically 5 to 6 h across the school day) and (e) after school, which included the time from the end of the last school lesson until 1830 hours.
The secondary aim of this study was to explore boys’ and girls’ compliance with recommendations for MVPA during recess and lunch breaks. The recommendations applied were engagement in MVPA for at least 40 % of recess and lunch breaks [35]. It is suggested that children should be active for 50 % of physical education lesson time [6]. However, when applying this guideline to recess time in previous research, few children met this recommendation [42] and it may thus be an unrealistic target. In light of this, an alternative suggestion of 40 % based on minimum activity recommendations that may be more achievable has been proposed [35] and was thus applied in this study.
Statistical analysis
All analyses were carried out using SPSS version 18.0 (SPSS Inc., Chicago, IL.). Sex differences in descriptive variables were determined by one-way analysis of variance (ANOVA). Analysis of covariance (ANCOVA) was used to explore sex differences in accumulated minutes and the proportion of time spent in each PA subcomponent during each segment of the school day. Covariates entered into each of the ANCOVA models for school transport and after school segments were BF%, CRF, ethnicity and SES. Morning recess and lunch break models additionally included morning recess duration and lunch break duration as covariates, respectively, while class time models included both morning recess and lunch break duration as additional covariates. Prior to ANCOVA analysis, tests for homogeneity of regression slopes were conducted and several significant interaction effects between sex (independent variable) and covariates were found. Sub-group analyses were then conducted to explore where sex differences in the dependent variable (PA intensity) varied according to levels of the covariate. Where interaction effects were observed for BF% and CRF, these variables were split into tertiles (lowest tertile representing least fat and least fit, respectively) for sub-group analyses, while for lunch break duration, a median split was performed with the lowest group representing the shortest duration. The proportion of boys and girls who met the recommendations for PA engagement during recess and lunch break was determined, i.e. those who spent 40 % of recess and lunch break time in MVPA [35]. χ 2 tests were used to evaluate associations between sex and achievement of the PA recommendations for recess and lunch break. The level of significance was set at p < 0.05.
Results
Table 1 shows the descriptive characteristics of the participants. One-way ANOVA revealed that BF% was significantly higher in girls versus boys, while CRF was significantly higher in boys. The proportion of white and non-white children was similar for both boys and girls.
Table 2 shows the percentage of total daily (i.e. school transport to after school hours time period) PA intensity minutes accrued in each segment of the school day. The majority of SED time was accrued during class time (63.9 %), while after school hours also contributed substantially (25.8 %). The majority of LPA was also accrued during class time (46.3 %) and after school hours (30.3 %). In addition to class time (37.1 and 31.2 % for MPA and VPA, respectively) and after school (27.9 and 30.3 % for MPA and VPA, respectively), lunch break also substantially contributed towards total daily minutes of MPA and VPA (18.1 and 22.3 %, respectively). School transport and morning recess time periods contributed towards SED, LPA, MPA and VPA to a lesser extent compared with the other longer duration segments.
Comparisons were made between sexes for total minutes spent in each PA subcomponent during segments of the school day (see Table 3). Girls engaged in significantly more LPA than boys during the school transport time period, but there were no significant differences in any other PA subcomponent. During morning recess and lunch break, girls spent significantly more minutes in SED and LPA compared to boys, while boys engaged in significantly more minutes of VPA during morning recess and significantly more MPA and VPA during lunch break. Girls also spent significantly more minutes in SED during class time than boys, but no other significant differences were observed for any other PA subcomponents. Minutes spent in SED, LPA, MPA and VPA did not differ significantly between girls and boys after school.
In terms of the proportion of total time spent in each PA subcomponent during segments of the school day (Table 2), girls spent a significantly greater proportion of time in LPA during school transport than boys. Girls also spent a significantly greater proportion of time in SED and LPA during morning recess compared to boys, while boys spent significantly more in VPA. The proportion of time in SED and LPA was also significantly higher in girls than in boys during lunch break, whereas boys spent significantly more in MPA and VPA during this segment of the day. There were no significant differences between boys and girls for the proportion of time spent in any PA subcomponent during class time and after school hours.
Main effect sizes for sex (according to Cohen’s effect sizes for ANCOVA [9]) were small (eta-squared = 0.01–0.05) for minutes and proportions of time spent in SED, LPA, MPA, VPA and MVPA during the school transport segment. Effect sizes ranged from small to large (eta-squared = ≥0.14) for minutes and proportions of time spent in SED, LPA, MPA, VPA and MVPA during morning recess and ranged from medium (eta-squared = 0.06–0.13) to large for lunch break, apart from LPA%, which was small. For class time and after school, effect sizes for sex were small for all PA subcomponents.
However, as noted in Table 3, a number of significant interaction effects were evident, suggesting that differences on the dependent variable among groups may vary as a function of a covariate and this particular data where the homogeneity of regression slopes assumption (i.e. equal sex effects across different levels of covariates) is violated should be interpreted with caution. In light of this, where significant interaction effects were observed, further sub-group analyses were conducted to explore sex differences in PA according to different levels of covariates. It was revealed that mean adjusted differences for VPA min (minutes in VPA) and VPA% (proportion of time in VPA) during school transport between boys and girls in the highest BF% tertile were significant; mean (SE) = 5.8 (1.2) and 1.7 (0.6) VPA min and 19.3 (4.2) and 5.7 (2.0) VPA% for boys and girls, respectively (p < 0.05); whereas no significant sex differences were observed in the lowest and middle tertiles. There was also a significant sex difference for VPA% during school transport in white participants (12.6 (1.8) and 5.9 (1.3) for boys and girls, respectively, p < 0.05), but not in non-white participants. A significant interaction effect between sex and CRF for after school VPA min was also evident, with girls in the highest CRF tertile accumulating significantly more VPA minutes than boys (13.6 (1.9) and 4.9 (1.9) minutes, respectively, p < 0.05), with no significant sex differences being observed in the middle and lowest tertiles.
Significant interactions between sex and SES were also observed. Girls in the lowest SES tertile (most deprived) spent a significantly higher proportion of time in SED during school transport compared to boys (41.5 % (3.7 %) and 24.8 % (4.4 %) for girls and boys, respectively, p < 0.05), with no significant sex differences in the middle and highest tertiles. Furthermore, boys in the lowest SES tertile spent a significantly higher proportion of time in MPA during school transport compared to girls (35.9 % (3.8 %) and 21.3 % (3.2 %) for boys and girls, respectively, p < 0.05). There was also a significant interaction between sex and lunch break duration for the proportion of time children engaged in VPA during this time period, with boys in the highest lunch break duration group spending significantly higher proportions of time in VPA than girls (19.5 % (2.0 %) and 6.0 % (1.4 %) for boys and girls, respectively, p < 0.05), whereas no significant sex difference was observed in the lowest group.
The secondary aim of this study was to explore boys’ and girls’ compliance with recommendations for MVPA during recess and lunch breaks. As shown in Fig. 1, significantly more boys met the guideline for recess and lunch break PA engagement, i.e. taking part in MVPA for at least 40 % of the time. There were 59.6 % of boys who met the suggested PA guideline for recess compared with 28.2 % of girls. During lunch break, 64.9 % of boys achieved the recommended level of MVPA engagement compared to only 10.3 % of girls.

Discussion
The primary aim of this study was to investigate the volume and patterns of boys’ and girls’ engagement in PA intensities and sedentary behaviours during different segments of the school day. The results of this study extend the current literature by providing a detailed analysis of sex differences in SED, LPA, MPA and VPA during specific segments of the day. Current PA guidelines recommend young people to engage in at least 60 min per day of MVPA [13]. The results of this study suggest that segments both during and out-of-school hours are important sources for MPA and VPA engagement in boys and girls. In particular, morning recess, lunch break and school transport appear to be key segments of the school day where both sexes engage in MPA and VPA and spend less time in SED. However, important sex differences in PA engagement during recess and lunch break were observed with boys engaging in greater levels of MPA and VPA than girls.
The majority of daily SED and LPA minutes were accrued during class time and after school, while a higher proportion of time was also spent in SED during these segments of the day compared with school transport, morning recess and lunch break. However, a higher proportion of time was spent in LPA during school transport and the lowest during class time compared with the other time periods for both boys and girls. Class time contributed the highest amount of daily MPA minutes, followed by after school and lunch break, respectively. However, class time and after school contributed similar total minutes of daily VPA, while a relatively high proportion of VPA minutes were also accrued during lunch break.
Given the relatively shorter durations of school transport (30 min) and morning recess (15 to 20 min), these segments of the day expectedly contributed to daily minutes of SED, LPA, MPA and VPA to a lesser extent compared with the other longer duration time periods. However, the proportion of time spent in MPA was substantially higher during school transport, morning recess and lunch break in comparison to class time and after school for both boys and girls. For VPA, boys spent substantially higher proportions of time in this PA intensity during morning recess and lunch break compared to other segments of the day, while girls spent higher proportions of time in VPA during school transport, morning recess, lunch break and after school compared with class time. As most minutes of SED are accrued during class time and after school with both sexes also spending the highest proportion of time in SED during these segments of the day, strategies to reduce sedentary time during these time periods, such as reducing TV viewing time [10], may be appropriate to reduce health risk. Additionally, despite its relatively short duration (compared to class time and after school), lunch break makes a substantial and promising contribution to total daily minutes of MVPA and schools should thus be encouraged to maintain or extend the duration of this time period.
In the present study, 10–14-year-old boys spent significantly more minutes and a greater proportion of time in VPA compared to girls during morning recess and accumulated significantly fewer minutes and a lower proportion of time in SED and LPA. Although in a slightly younger age group (5–10 year olds), previous research supports the finding of greater VPA engagement in boys compared to girls during morning recess [36]. However, the cohort of boys in the current research engaged in substantially higher levels of VPA compared to those in Ridger et al’s [36] study (19.1 vs. 4.5–7.0 %, respectively), whereas girls’ engagement in VPA was similar between studies; 5.5 % in the current study vs. 2.9–6.5 % in Ridger et al’s [36]. The disparity observed in boys may be due to differences in accelerometry device and there remains controversy regarding which set of cut-points for PA intensity thresholds is most representative of ‘moderate’ and ‘vigorous’ levels of physical exertion in youths [33]. It is possible that the amount of time spent in each PA intensity may vary with different cut-points.
A pedometer-based study in third- to fifth-grade students reported that boys were physically active for 78 % of recess time, which was significantly higher than girls (63 %) [4]. Nettleford et al. [29] found that 8–11-year-old boys and girls spent 27.9 and 19.6 % (p < 0.001) of recess in MVPA, respectively, while boys and girls in the current study engaged in MPA for 27.8 and 25.1 % (p > 0.05) and in VPA for 19.1 and 5.5 % (p < 0.001) of recess, respectively. The main reason for differences in PA levels between accelerometer and pedometer-based studies is due to the fact that pedometry data represents total volume of PA accumulated, whereas accelerometers permit representation of engagement in specific PA intensities. Since the magnitude of the association between PA and some health outcomes are intensity driven [13] and given that current PA guidelines pertain specifically to time spent in MVPA [13], the latter method appears to be preferable when analysing PA patterns and targeting interventions in youth.
Regarding sex differences in PA during lunch break, boys engaged in significantly higher amounts of MPA and VPA compared to girls and significantly less SED and LPA. Since health benefits of PA primarily accrue at or above moderate intensity PA [13], the higher levels of MPA and VPA exhibited by boys during this segment of the school day are more likely to result in enhanced CRF [3, 21] and cardiometabolic health [14]. Similar to these findings, Tudor-Locke et al. [44] reported that in sixth-grade students, boys accumulated more steps than girls during lunch break, while Nettleford et al. [29] reported that boys spent more time in accelerometry-determined MVPA (34.7 vs. 27.9) and less time in SED (45.5 vs. 51.6 %) compared to girls. However, the current study is the first to report on children’s engagement in SED, LPA, MPA and VPA during lunch break, which is important given that current PA guidelines encourage participation in both MVPA and VPA, as well as minimising sedentary time [13].
During class time, girls accumulated significantly more minutes of SED compared to boys, although no significant differences were noted for any of the PA variables. In 8–11 year olds, it was reported that girls accumulated more minutes (209.7 vs. 200.3 min) of SED than boys during regular class time (i.e. excluding physical education (PE)), although unlike the present study, girls also spent a significantly higher proportion of time in SED than boys (74.2 vs. 71.2 %, respectively) [29]. The school setting appears to promote prolonged periods of sitting and it is hence unsurprising to observe high levels of SED during class time [22]. Nettleford et al. [29] reported that girls accumulated fewer minutes and spent a smaller proportion of time in MVPA than boys during regular class time (33.8 vs. 39.9 min and 12.0 vs. 14.1 % in girls and boys, respectively), although there was no difference in LPA. During PE, however, no significant differences were observed between girls’ and boys’ engagement in SED, LPA and MVPA [29]. Unfortunately, PA patterns could not be determined separately for regular and PE class time in the current study as it was unknown when PE classes took place. A previous investigation, however, reported no sex differences in accumulated number of steps during PE in sixth-grade children [44], although other studies using pedometry and accelerometry have observed higher PA levels in boys [24, 28]. It has been suggested that boys’ PA may be greater during PE due to sex differences in lesson content, such as boys taking part in team invasion games whereas girls’ lessons may focus more on PE curricula movement-based activities that expel less energy [17].
PA patterns for school transport and after school were similar between sexes; the only significant difference observed being girls’ higher accumulated minutes and proportion of time in LPA during school transport. Boys did engage in higher levels of MPA and less SED, but these differences were non-significant (p > 0.05). One previous pedometry study also reported similar PA engagement during the school transport time period for sixth-grade boys and girls, although boys accumulated more steps than girls after school [44]. In third- to fifth-grade children, higher levels of PA were observed in boys outside of school hours compared to girls using pedometry [4]. However, because this study failed to discriminate between school transport and after school hours, it is unknown whether sex differences existed for these specific segments of the school day. Nonetheless, using self-report, 12–18-year-old boys were 1.32 (95 % CI 1.15–1.50) and 1.38 (95 % CI 1.20–1.59) times more likely to be ‘more active’ during school commuting and after school, respectively, compared to girls [23]. However, it is difficult to compare these studies to the current investigation due to differences in the assessment of PA and the fact that pedometry and self-report measures limit the interpretation of PA intensity and patterns [1].
The current study also identifies a number of groups which have different PA engagement between boys and girls. There were a number of significant interaction effects observed between sex and covariates for PA engagement; the majority being evident for PA during the school transport time period. Boys in the highest BF% tertile engaged in significantly more VPA than girls during school transport. White boys also engaged in a higher proportion of VPA during school transport than white girls. Previous research in youths has shown that PA is lowest for female and ethnic minorities [20] and children with high levels of body fat [5]. Furthermore, boys in the lowest SES tertile spent a significantly lower proportion of time in SED and significantly higher proportion of time in MPA during school transport compared to girls. No previous studies have reported sex by SES differences in PA intensity engagement and future research should continue to address this issue.
For the after school segment, a significant interaction effect was observed between sex and CRF for VPA min, with girls in the highest CRF tertile accumulating significantly more VPA minutes than boys. The last significant interaction effect observed was between sex and lunch break duration for VPA%. Previous research demonstrates that boys are more active than girls during lunch break [29]. However, the present study revealed that boys in the highest lunch break group spent a significantly higher proportion of time in VPA than girls. Interventions to promote equal PA opportunities for boys and girls during school transport might thus target girls with high levels of BF%, those of white ethnic origin, and those who are most deprived. Interventions might also target increasing PA in girls at schools that have longer lunch break durations. Regarding CRF, VPA engagement was significantly lower (p < 0.05) in the middle (5.7 (1.3) min) and least fit girls (4.9 (1.5) min) compared to the highest fit girls (13.7 (1.9) min), whereas no significant differences between tertiles were observed for boys and it may thus be appropriate for interventions to target PA promotion in girls with lower levels of CRF.
The secondary aim of this study was to explore girls’ and boys’ achievement of suggested guidelines for PA engagement during recess and lunch break [35]. There were 59.6 % of boys who engaged in MVPA for 40 % of recess time compared with 28.2 % of girls, while during lunch break, 64.9 % of boys achieved the recommended time in MVPA compared to just 10.3 % of girls. Nettleford et al [29] also found that more 8–11-year-old boys achieved the recommended level of PA during recess and lunch break, although the proportion of boys sufficiently active was less than that of the current study (34.1 vs. 59.6 % for recess and 37.4 vs. 64.9 % for lunch break, respectively). However, although less girls achieved the recommended level of PA during recess in Nettleford et al’s study [29] compared to the present findings (15.7 vs. 28.2 %, respectively), less girls in the current study were sufficiently active during lunch break (16.7 vs. 10.3 %, respectively). In slightly younger children (mean age 8 ± 1.4 years), 14.9 % of boys and 4.3 % of girls engaged in at least moderate intensity PA for 40 % of recess time [35], which is lower than that of the current study.
This disparity observed between studies regarding the proportion of boys and girls who are sufficiently active during recess and lunch break may be in part due to differences in accelerometry device and the cut-points employed to define PA intensity [33]. Furthermore, it is possible that differences in school policy and length of recess and lunch break may influence children’s PA engagement during these segments of the day. In the current study, recess was 15–20 min and lunch 45–65 min in duration and it is unknown how school policy or seasonal variations influenced PA during these times, e.g. whether and for how long children had to sit and eat before playing outside. However, although disparities in the proportion of children sufficiently active during recess and lunch breaks may be observed between studies, the finding that more boys are sufficiently active than girls is consistent [29, 35]. It may therefore be particularly important to focus intervention strategies towards increasing girls’ participation in MVPA during these segments of the school day.
Limitations of this study include the absence of a physical maturity measure. Previous research suggests that sex differences in PA levels may be eliminated after controlling for maturation [43] and it is unknown whether this hypothesis is applicable to the current cohort. However, unlike previous research [4, 29, 35, 44], this study accounted for BF% and CRF when comparing boys’ and girls’ segmented PA levels. Given that there are sex differences in body fat [3, 38] and CRF [38] and that both variables may influence PA engagement [5, 21], we can be confident that these factors were not accountable for the sex differences observed. Next, although accelerometry is now considered the gold-standard measure of PA levels, this method still has limitations. In addition to variation in intensity cut-points discussed above, most accelerometers cannot be worn in water and devices also fail to accurately reflect energy expenditure associated with cycling, upper body movements and walking uphill. Furthermore, the definition of school transport has potential limitations in that much PA prior to school may be non-commuting PA. It is possible that some inactive commuters (i.e. who travel by car) may have arrived at school relatively early and accumulated PA before school started, which would thus misrepresent the amount of PA they accumulate during their commute. The study is also limited due to the inability to explore the independent contributions of PE and normal class time to total daily PA or indeed sex differences in PA intensities during these specific time periods. Lastly, the sample size was relatively small and included only schools in Bedfordshire, UK. Although socioeconomic status of the recruitment areas was similar to other regions of the UK according to local area statistics [8], the ability to generalise the findings may be limited due to lower overweight and obesity levels in comparison to national averages [39] as well as variations in ethnic representation between schools.
In conclusion, this study has added important information on the patterns of boys’ and girls’ engagement in different PA intensities during segments of the school day, with boys utilising more opportunities to engage in health-promoting MVPA and minimising their time spent sedentary. This study showed that girls are substantially less active than boys during recess and lunch breaks, although a relatively large proportion of both sexes are not achieving PA recommendations during these time periods. Strategies to increase engagement in MVPA and promote equal opportunities for PA in girls and boys during these segments are warranted.
References
Adamo KB, Prince SA, Tricco AC, Connor-Gorber S, Tremblay M (2009) A comparison of indirect versus direct measures for assessing physical activity in the pediatric population: a systematic review. Int J Pediatr Obes 4(1):2–27
Andersen LB, Sardinha LB, Froberg K, Riddoch CJ, Page AS, Anderssen SA (2008) Fitness, fatness and clustering of cardiovascular risk factors in children from Denmark, Estonia and Portugal: the European Youth Heart Study. Int J Pediatr Obes 3(Suppl 1):58–66
Bailey DP, Boddy LM, Savory LA, Denton SJ, Kerr CJ (2012) Associations between cardiorespiratory fitness, physical activity and clustered cardiometabolic risk in children and adolescents: the HAPPY study. Eur J Pediatr 171(9):1317–1323
Beighle A, Morgan CF, Le Masurier G, Pangrazi RP (2006) Children’s physical activity during recess and outside of school. J Sch Health 76(10):516–520
Butte NF, Puyau MR, Adolph AL, Vohra FA, Zakeri I (2007) Physical activity in nonoverweight and overweight Hispanic children and adolescents. Med Sci Sports Exerc 39(8):1257–1266
Centers for Disease Control and Prevention (1997) Guidelines for school and community programs to promote lifelong physical activity among young people. Morb Mort Wkly Rep 46(RR-6):1–36
Chen LJ, Fox KR, Haase A, Wang JM (2006) Obesity, fitness and health in Taiwanese children and adolescents. Eur J Clin Nutr 60(12):1367–1375
Child and Maternal Health Observatory (2009) Available at: http://atlas.chimat.org.uk/IAS/dataviews/view?viewId=11. Accessed 7 Jan 2012
Cohen J (1988) Statistical power analysis for the behavioral sciences, 2nd edn. Erlbaum, Hillsdale
Danner FW (2008) A national longitudinal study of the association between hours of TV viewing and the trajectory of BMI growth among US children. J Pediatr Psychol 33(10):1100–1107
Deforche B, De Bourdeaudhuij I, D’Hondt E, Cardon G (2009) Objectively measured physical activity, physical activity related personality and body mass index in 6- to 10-yr-old children: a cross-sectional study. Int J Behav Nutr Phys Act 6:25
Department of Health. Health Survey for England (2008) Physical activity and fitness. http://www.ic.nhs.uk/webfiles/publications/HSE/HSE08/Volume_1_Physical_activity_and_fitness_revised.pdf. Accessed 18 April 2011
Department of Health (2011) Start Active, Stay Active: a report on physical activity for health from the four home countries’ Chief Medical Officers. http://www.dh.gov.uk/prod_consum_dh/groups/dh_digitalassets/documents/digitalasset/dh_128210.pdf. Accessed 7 July 2011
Ekelund U, Anderssen SA, Froberg K, Sardinha LB, Andersen LB, Brage S (2007) Independent associations of physical activity and cardiorespiratory fitness with metabolic risk factors in children: the European Youth Heart Study. Diabetologia 50(9):1832–1840
Ekelund U, Tomkinson G, Armstrong N (2011) What proportion of youth are physically active? Measurement issues, levels and recent time trends. Br J Sports Med 45(11):859–865
Eston RG, Rowlands AV, Ingledew DK (1998) Validity of heart rate, pedometry, and accelerometry for predicting the energy cost of children’s activities. J Appl Physiol 84(1):362–371
Fairclough S, Stratton G (2005) Physical education makes you fit and healthy. Physical education’s contribution to young people’s physical activity levels. Health Educ Res 20(1):14–23
Fairclough SJ, Boddy LM, Hackett AF, Stratton G (2009) Associations between children’s socioeconomic status, weight status, and sex, with screen-based sedentary behaviours and sport participation. Int J Pediatr Obes 4(4):299–305
Gidlow CJ, Cochrane T, Davey R, Smith H (2008) In-school and out-of-school physical activity in primary and secondary school children. J Sports Sci 26(13):1411–1419
Gordon-Larsen P, McMurray RG, Popkin BM (1999) Adolescent physical activity and inactivity vary by ethnicity: The National Longitudinal Study of Adolescent Health. J Pediatr 135(3):301–306
Gutin B, Yin Z, Humphries MC, Barbeau P (2005) Relations of moderate and vigorous physical activity to fitness and fatness in adolescents. Am J Clin Nutr 81(4):746–750
Harrington DM, Dowd KP, Bourke AK, Donnelly AE (2011) Cross-sectional analysis of levels and patterns of objectively measured sedentary time in adolescent females. Int J Behav Nutr Phys Act 8:120
Hohepa M, Scragg R, Schofield G, Kolt GS, Schaaf D (2009) Self-reported physical activity levels during a segmented school day in a large multiethnic sample of high school students. J Sci Med Sport 12(2):284–292
LeMura LM, Andreacci J, Carlonas R, Klebez JM, Chelland S (2000) Evaluation of physical activity measured via accelerometry in rural fourth-grade children. Percept Mot Skills 90(1):329–337
Mattocks C, Ness A, Leary S, Tilling K, Blair SN, Shield J et al (2008) Use of accelerometers in a large field-based study of children: protocols, design issues, and effects on precision. J Phys Act Health 5(Suppl 1):S98–S111
MIMAS (2008) Welcome to GeoConvert. Available at: http://geoconvert.mimas.ac.uk/. Accessed 30 April 2011
Morrison JA, Friedman LA, Wang P, Glueck CJ (2008) Metabolic syndrome in childhood predicts adult metabolic syndrome and type 2 diabetes mellitus 25 to 30 years later. J Pediatr 152(2):201–206
Nader PR (2003) Frequency and intensity of activity of third-grade children in physical education. Arch Pediatr Adolesc Med 157(2):185–190
Nettlefold L, McKay HA, Warburton DE, McGuire KA, Bredin SS, Naylor PJ (2011) The challenge of low physical activity during the school day: at recess, lunch and in physical education. Br J Sports Med 45(10):813–819
Ogden CL, Carroll MD, Curtin LR, Lamb MM, Flegal KM (2010) Prevalence of high body mass index in US children and adolescents, 2007–2008. Jama 303(3):242–249
Riddoch C, Edwards D, Page A, Froberg K, Anderssen SA, Wedderkopp N et al (2005) The European Youth Heart Study—cardiovascular disease risk factors in children: rationale, aims, study design, and validation of methods. J Phys Act Health 2(1):115–129
Riddoch CJ, Bo Andersen L, Wedderkopp N, Harro M, Klasson-Heggebo L, Sardinha LB et al (2004) Physical activity levels and patterns of 9- and 15-yr-old European children. Med Sci Sports Exerc 36(1):86–92
Ridgers ND, Fairclough SJ (2011) Assessing free-living physical activity using accelerometry: Practical issues for researchers and practitioners. Eur J Sport Sci 11(3):205–213
Ridgers ND, Graves LE, Foweather L, Stratton G (2010) Examining influences on boy’s and girls’ physical activity patterns: the A-CLASS project. Pediatr Exerc Sci 22(4):638–650
Ridgers ND, Stratton G, Fairclough SJ (2005) Assessing physical activity during recess using accelerometry. Prev Med 41(1):102–107
Ridgers ND, Stratton G, Fairclough SJ, Twisk JW (2007) Children’s physical activity levels during school recess: a quasi-experimental intervention study. Int J Behav Nutr Phys Act 4:19
Rowlands AV, Thomas PW, Eston RG, Topping R (2004) Validation of the RT3 triaxial accelerometer for the assessment of physical activity. Med Sci Sports Exerc 36(3):518–524
Ruiz JR, Ortega FB, Rizzo NS, Villa I, Hurtig-Wennlof A, Oja L et al (2007) High cardiovascular fitness is associated with low metabolic risk score in children: the European Youth Heart Study. Pediatr Res 61(3):350–355
Stamatakis E, Wardle J, Cole TJ (2010) Childhood obesity and overweight prevalence trends in England: evidence for growing socioeconomic disparities. Int J Obes (Lond) 34(1):41–47
Steele RM, van Sluijs EM, Cassidy A, Griffin SJ, Ekelund U (2009) Targeting sedentary time or moderate- and vigorous-intensity activity: independent relations with adiposity in a population-based sample of 10-y-old British children. Am J Clin Nutr 90(5):1185–1192
Steele RM, van Sluijs EM, Sharp SJ, Landsbaugh JR, Ekelund U, Griffin SJ (2010) An investigation of patterns of children’s sedentary and vigorous physical activity throughout the week. Int J Behav Nutr Phys Act 7:88
Stratton G (2000) Promoting children’s physical activity in primary school: an intervention study using playground markings. Ergonomics 43(10):1538–1546
Thompson AM, Baxter-Jones AD, Mirwald RL, Bailey DA (2003) Comparison of physical activity in male and female children: does maturation matter? Med Sci Sports Exerc 35(10):1684–1690
Tudor-Locke C, Lee SM, Morgan CF, Beighle A, Pangrazi RP (2006) Children’s pedometer-determined physical activity during the segmented school day. Med Sci Sports Exerc 38(10):1732–1738
Twisk JW, Kemper HC, van Mechelen W (2002) The relationship between physical fitness and physical activity during adolescence and cardiovascular disease risk factors at adult age. The Amsterdam Growth and Health Longitudinal Study. Int J Sports Med 23(Suppl 1):S8–S14
Wang Y, Lobstein T (2006) Worldwide trends in childhood overweight and obesity. Int J Pediatr Obes 1(1):11–25
Acknowledgments
The authors would like to thank the participants who gave their time to the study. We would also like to thank all of the schools who helped facilitate the research. This study was funded by the Bedford Charity.
Conflict of interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Bailey, D.P., Fairclough, S.J., Savory, L.A. et al. Accelerometry-assessed sedentary behaviour and physical activity levels during the segmented school day in 10–14-year-old children: the HAPPY study. Eur J Pediatr 171, 1805–1813 (2012). https://doi.org/10.1007/s00431-012-1827-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00431-012-1827-0