
Abstract
Arterial hypertension in childhood is less frequent as compared to adulthood but is more likely to be secondary to an underlying disorder. After ruling out more obvious causes, some patients still present with strongly suspected secondary hypertension of yet unknown etiology. A number of these children have hypertension due to single gene mutations inherited in an autosomal dominant or recessive fashion. The finding of abnormal potassium levels (low or high) in the presence of suppressed renin secretion, and metabolic alkalosis or acidosis should prompt consideration of these familial diseases. However, mild hypertension and the absence of electrolyte abnormalities do not exclude hereditary conditions. In monogenic hypertensive disorders, three distinct mechanisms leading to the common final pathway of increased sodium reabsorption, volume expansion, and low plasma renin activity are documented. The first mechanism relates to gain-of-function mutations with a subsequent hyperactivity of renal sodium and chloride reabsorption leading to plasma volume expansion (e.g., Liddle's syndrome, Gordon's syndrome). The second mechanism involves deficiencies of enzymes that regulate adrenal steroid hormone synthesis and deactivation (e.g., subtypes of congenital adrenal hyperplasia, apparent mineralocorticoid excess (AME)). The third mechanism is characterized by excessive aldosterone synthesis that escapes normal regulatory mechanisms and leading to volume-dependent hypertension in the presence of suppressed renin release (glucocorticoid remediable aldosteronism). Hormonal studies coupled with genetic testing can help in the early diagnosis of these disorders.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Arterial hypertension in childhood is less frequent as compared to adulthood but is more likely to be secondary to an underlying disorder. Essential hypertension is rarely diagnosed in children less than 5 years of age and only more often beyond the age of 10 years. Obviously, it is of paramount importance to identify secondary origins of persistent hypertension (blood pressure >95th percentile for height and gender) in these children [14]. Treatment of hypertension without a specified workup such as often seen in the adult setting is not justified.
The assessment of a hypertensive child should begin with a careful personal and family medical history and a physical examination. If not diagnostic, investigations should focus on renal or cardiac causes. Appropriate investigations include: full blood cell count, electrolytes with emphasis on potassium, acid–base balance, uric acid and creatinine, urinalysis, and the measurement of the ratio of urinary protein to creatinine in an early morning urine sample [10]. The trans-tubular potassium gradient, an estimate of aldosterone bioactivity, is useful with respect to diseases with extracellular fluid volume expansion secondary to increased mineralocorticoid activity. Renin and aldosterone should be measured and normal values in children are available [11]. Renal imaging by ultrasound and Doppler of renal arteries is essential. Further imaging techniques such as NMR, angiography, or renal scan are performed if appropriate. Echocardiography has a place in the workup in every child with severe hypertension in order to assess left ventricular mass and to rule out aortic coarctation [10].
Having excluded the more obvious causes, there are still patients in whom secondary hypertension is strongly suspected while the standard search for an etiology is unsuccessful. A number of these children will have hypertension due to single gene mutation inherited in an autosomal dominant or recessive fashion. These familial disorders are common enough to be included in the differential diagnosis of any hypertensive child irrespective of the severity. The purpose of this review is to discuss the monogenic forms of low-renin hypertension, which may become manifest in childhood. Of particular importance, we will point out when and how should the pediatrician search for these diseases and discuss the appropriate antihypertensive strategies. Further causes of monogenic hypertension will only shortly be addressed (Table 1).
When to consider a monogenic form of hypertension
The inheritance pattern of a given family may already indicate the presence of a monogenic form of hypertension. A family history of severe hypertension, especially with early onset (adolescence or young adult age) is suggestive of one of the dominantly inherited conditions, whereas consanguinity may indicate recessive inheritance. Nevertheless, family history is often misleading as essential hypertension is highly prevalent in adults. Consideration of hereditary forms of hypertension should not be limited to children with severe hypertension or electrolyte abnormalities, since mild hypertension and the absence of electrolyte abnormalities does not exclude an inherited condition; in fact, many individuals with these forms of inherited hypertension have only mild to moderate hypertension without electrolyte disturbances. Abnormal potassium levels (low or high), suppressed renin, and metabolic alkalosis or acidosis should rise suspicion for the presence of these familial disorders. Plasma renin activity or renin concentration (random) and plasma aldosterone levels are useful at the beginning (prior to therapy) to identify the etiology of the hypertension. All hereditary forms of hypertension lead to a suppression of the renin–angiotensin system (low plasma renin level or reduced plasma renin activity) due to an autonomous plasma volume expansion. In addition to hyporeninemia, expansion of the extracellular fluid volume can be associated with hypouricemia (by reducing its proximal tubular reabsorption). In synopsis with the suppressed renin, the level of aldosterone (increased or suppressed) will further discriminate the different diseases (Table 2).
Physiology of Na transport in the distal nephron
The consequence of a defective gene in each case of these forms of hypertension is abnormally increased sodium (Na) transport in the distal nephron causing an expansion of the circulating plasma volume and a consecutive increase of the cardiac output with resulting hypertension. A compromised renal natriuresis favoring a positive Na and thus volume balance in the distal nephron is an essential element of forms of hypertension associated with a high cardiac output, as hypothesized by Guyton et al. [7]. Therefore, we will discuss distal nephron Na transport as related to the different diseases presented in this review.
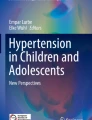
The distal convoluted tubule cell and the principal cells of the collecting duct cell are the two cell types most important for Na transport in the distal nephron. A simplified model of these cell types is presented in Fig. 1. The target of the regulation is the transepithelial Na transport into the cell through the luminal Na transporter: in the distal convoluted tubule cell, it is the thiazide-sensitive sodium chloride (NaCl) cotransporter (NCC); in the collecting duct, it is the amiloride-sensitive epithelial Na channel (ENaC). Additionally, basolateral sodium–potassium adenosine triphosphate (Na/K-ATPase) and the luminal renal outer medulla K channel (ROMK) are responsible for Na and K homeostasis. The mechanisms of regulation are still insufficiently understood, the best documented mechanism being the regulation by mineralocorticoids. Aldosterone binds to the cytosolic mineralocorticoid receptor (MR) and leads to increased activity of the apical Na transporter (ENaC). Deoxycorticosterone and deoxycortisol and their metabolites are alternative agonists of the MR with cortisol being the most important one. The 11β-hydroxysteroid dehydrogenase type 2 enzyme (11βHSD-2) which converts active cortisol to the inactive cortisone protects the MR from cortisol, an alternative agonist of the MR, thus establishing the aldosterone specificity of the MR [3].

Simplified diagram of a distal nephron sodium transporting cell in the distal convolute tubule and collecting duct. The amiloride-sensitive epithelial Na channel (ENaC) is found predominantly in principal cells of the collecting duct and the thiazide-sensitive sodium chloride cotransporter (NCC) in the distal convolute tubule. 11βHSD-2 11β-hydroxysteroid dehydrogenase type 2 enzyme, WNK1 and WNK4 kinases with no lysine serine/threonine protein kinase type 1 and 4, respectively, Na/K-ATPase contraluminal sodium-potassium adenosine triphosphate. Activation is indicated by green arrows and suppression by red lines ending with a circle (adapted from Vehaskari [20])
Na reabsorption is controlled by mineralocorticoid active steroid hormones in both the distal convoluted tubule and the collecting duct. Additional regulatory elements are involved including, but not limited to kinases (WNK1 and WNK4) [22]. WNK4 exerts a suppression of the NCC activity. WNK1 inhibits WNK4 and activates ENaC.
Given the magnitude of regulatory mechanisms, multiple candidate genes might be involved in abnormalities of the Na transport and consecutive hypertension. The known disorders leading to hypertension can be classified in (a) induced by a mineralocorticoid effect (with the disorder being primarily in the distal nephron or being primarily adrenal disorder) and (b) induced by excessive natrium uptake independent of mineralocorticoid action.
How to diagnose a monogenic form of hypertension
The evaluation of the renin–angiotensin–aldosterin system (RAAS) is of paramount importance for the initial evaluation of children with a suspected monogenic form of arterial hypertension. As already discussed, the assessment of the plasma renin activity (or renin concentration) together with plasma aldosterone concentration is a useful screening. All these monogenic forms of hypertension share a low-renin activity (“low-renin hypertension”), whereas suppressed plasma aldosterone is present in all forms of inherited hypertension except primary aldosteronism (which in most cases is not heritable and is not a matter of discussion in this review), glucorticoid remediable aldosteronism, and Gordon's syndrome (Table 2; Fig. 2, and next chapter). Electrolyte abnormalities like metabolic alkalosis with hypokalemia or metabolic acidosis with hyperkalemia are important markers for the first suspicion of these forms of monogenic hypertension but may be absent in many individuals with hereditary forms of hypertension. In some hypokalemic patients with low-renin hypertension, mechanical trauma during venipuncture results in the release of potassium from red cells and causes apparently normal or even high levels of potassium.

Flow chart for the discrimination of different heritable forms of arterial hypertension. Non-heritable forms of hypertension and primary aldosteronism (Conn's syndrome) are not discussed. K potassium, N normal
The next step for the evaluation of distal tubular functions, especially the function of the ENaC and mineralocorticoid activity, is the assessment of the trans-tubular potassium gradient (TTKG), which is high (>2) despite hypokalemia with increased ENaC activity. The TTKG is derived from (potassiumurine*osmolarityplasma)/(potassiumplasma*osmolarityurine).
Urinary steroid hormone profiling (in a 24-h urine specimen) is another important step for the evaluation of the different forms of hereditary hypertension. The analysis of the steroid hormone metabolites and the respective apparent enzyme activities in the urine provides information on the adrenal production and metabolism of glucocorticoids, mineralocorticoids, and sexual hormones, thus assisting in locating the putative defect. Genetic testing for the mutations causing hereditary hypertension is increasingly becoming available. Most tests are based on direct DNA sequencing or on probing for known mutations. It must be noted that the test spectrum provided is variable and while most tests will only consider known mutants, some might also include the gene as a whole.
Pathophysiology of diseases, diagnosis, and treatment
In the following section, we aim to list the most common heritable diseases with a clinical phenotype to be observed as early as in childhood or during adolescence. Diagnostic procedures and treatment options of these different diseases are briefly explained. The flow chart on Fig. 2 aids to discriminate between the different diseases described. Other hereditary conditions causing arterial hypertension such as neurofibromatosis type I, tuberous sclerosis, Turner's syndrome, familial pheochromocytoma, polycystic kidney disease, autosomal-dominant hypertension with brachydactyly, and Williams–Beuren syndrome are beyond the scope of this review and are briefly described in Table 1.
Hypertension induced by a mineralocorticoid effect
Syndrome of apparent mineralocorticoid excess
This is a rare autosomal recessive disorder due to an inactivating mutation of the 11β-hydroxysteroid dehydrogenase (HSD) type 2 enzyme [21]. As a result, cortisol can bind to the MR (Fig. 1). Hypokalemia with metabolic alkalosis is observed. Renal concentrating defect (due to the hypokalemia) and hypercalciuria with nephrocalcinosis may be present [13]. The severe phenotype begins in early childhood with low birth weight and failure to thrive in the presence of severe arterial hypertension, leading very early to end organ damage [1]. Milder phenotypes have been described without electrolyte abnormalities and development of arterial hypertension only in adulthood [13, 15].
The diagnosis should be suspected in any form of low-renin, low aldosterone hypertension with signs of mineralocorticoid excess, like an increased trans-tubular potassium gradient (TTKG). Urinary steroid hormone profiling can confirm the diagnosis showing a low apparent enzyme activity as given by an increased ratio of (tetrahydrocortisol + allotetrahydrocortisol)/tetrahydrocortisone or free cortisol/free cortisone in a 24-h urine sample. Genetic testing is available. The genetic disease must be well distinguished from liquorice abusus which inhibits the 11β-HSD type 2 enzyme and may cause a similar picture with low-renin arterial hypertension with hypokalemia.
The therapy consists of MR antagonists and ENaC blockers like spironolacotone or eplerenone and amiloride, respectively, as well as symptomatic K supplementation and dietary Na restricition. Thiazide diuretics may ameliorate hypercalciuria.
Glucocorticoid remediable aldosteronism (familial hyperaldosteronism type I)
The gene for the aldosterone synthase (CYP11B2 expressed in the zona glomerulosa) is considered to be the result of an ancient duplication of the gene of the cortisol and corticosterone synthezising enzyme 11β-hydroxylase (CYP11B1 expressed in the zona fasciculata of the adrenal cortex) closely neighbored on chromosome 8. Glucocorticoid remediable aldosteronism (GRA) is the result of unequal crossing over between these two genes [8]. As a result, the hybrid gene has the CYP11B1-specific ACTH-responsive promoter and an aldosterone synthase coding region, resulting in ACTH-stimulated aldosterone production, mainly independent of renin. The high levels of mineralocorticoids activate the MR and upregulate Na reabsorption and K secretion.
The hereditary pattern is autosomal dominant and is absent in blacks. Most individuals have severe hypertension since infancy but milder phenotypes have been described [2]. GRA patients are at risk for cerebral aneurysms and intracranial bleeding, therefore, magnetic resonance screening beginning at puberty has been recommended [9, 20]. Mild hypokalemia and metabolic alkalosis can be observed. Plasma renin activity is always suppressed, yet plasma aldosterone concentration may be normal. An increased ratio of aldosterone to renin is highly suggestive of the differential diagnosis of primary aldosteronism. The genetic testing for the chimeric gene has eliminated the need for complicated evaluations like dexamethasone suppression test, adrenal imaging, and adrenal-vein sampling, yet we suggest to perform a urinary steroid hormone analysis to establish the biochemical features of the disease before testing genetics [20]. Therapy of first choice therapy is represented by glucocorticoids in order to suppress ACTH and the resulting ACTH-stimulated mineralocorticoid production [19]. MR antagonists can be added.
Congenital adrenal hyperplasia—subtypes associated with arterial hypertension
The most common type of congenital adrenal hyperplasia (CAH), i.e., the 21-hydroxylase deficiency, causes a Na-losing state and does not cause hypertension. Deoxycortisol, deoxycorticosterone, and typical as well as atypical metabolites express mineralocorticoid activity. In two subtypes of CAH, there is an accumulation of intermediate products with MR activity. Defects in 11β-hydroxylase (CAH type IV) and 17α-hydroxylase (CAH type V) lead to an overproduction of 21-hydroxylated steroids, which are responsible for the activation of the MR. In type IV CAH, the enzyme block results in an increased sex hormone with androgenic action, causing virilization in girls and precocious puberty in boys. In type V CAH, the inability to synthesize cortisol and the early block in sex hormone synthesis results in primary amenorrhea and delayed sexual development in girls, whereas boys have ambiguous genitalia [12]. In both forms, aldosterone synthesis is greatly reduced. Steroid profile analysis leads to the diagnosis. Treatment is based on steroid supplementation in type IV and both steroids and sex hormones in type V disease. Hypertension can be improved with MR antagonists.
Hypertension induced by excessive renal tubular sodium uptake independent of mineralocorticoid action
Liddle's syndrome
Liddle's syndrome is characterized by an increased ENaC-mediated Na reabsorption in the distal tubule, due to gain-of-function mutations of the encoding gene [17]. Like most activating mutations not affecting reproduction capabilities and gestational outcome, Liddle's syndrome has an autosomal dominant inheritance pattern. Early-onset hypertension with hypokalemia, metabolic alkalosis, and sometimes hypercalciuria are the clinical characteristics of the disease [4]. Plasma renin activity and plasma aldosterone levels are markedly suppressed. Liddle's syndrome may be the most common type of monogenic hypertension, and it has been described in many different populations (Caucasians, Asians, and Blacks). The treatment consists of a low-salt diet and substances that directly inhibit ENaC, like amiloride or triamterene. MR antagonists are without effect (which can be used as diagnostic tool to suspect the disease). Of interest, loss-of-function mutations have also been described, causing water and salt wasting and consequently hyperaldosteronism (pseudohypoaldosteronism type I).
Gordon's syndrome (familial hyperkalemic hypertension, pseudohypoaldosteronism type II)
The characteristics of Gordon's syndrome are hyperkalemia with normal renal function, mild hyperchloremic metabolic acidosis, low urinary excretion of sodium, hypercalciuria, and hypertension [5, 6].
The syndrome has been linked to abnormal function of the thiazide sensitive nephron segment, the distal convolute tubule. Mutations in the kinases WNK1 and WNK4 have been identified to be responsible for some forms of Gordon's syndrome [22]. As no activating mutations have been found in the NCC, the genetic background of other forms of Gordon's syndrome remains unclear. Gordon's syndrome is inherited as an autosomal dominant trait. The metabolic abnormalities may precede the development of arterial hypertension (Spitzer–Weinstein syndrome with hyperkalemia, metabolic acidosis, and growth failure is now believed to be early presentation of Gordon's syndrome [18]). Plasma renin activity is suppressed together with normal or high aldosterone levels. In fact, despite the volume overload, aldosterone is not always suppressed because hyperkalemia can induce its secretion.
The therapy consists of low-dose thiazide diuretics. Pathophysiologically, the clinical features of Gordon's syndrome are the opposite of Gitelman syndrome, characterized by abnormalities in the NCC [16].
Conclusion
Hypertension in children frequently develop as a result of RAAS activation secondary to renal disease but occasionally is because of salt and water overload due to abnormal electrolyte transport. In monogenic hypertensive disorders, three distinct mechanisms leading to the common final pathway of increased sodium reabsorption, volume expansion, and low plasma renin activity are documented:
-
1.
Mutations with consequent hyperactivity of sodium and chloride transporters leading to hypertension (e.g., Liddle's syndrome, Gordon's syndrome).
-
2.
Deficiencies of enzyme that regulate adrenal steroid metabolism and activity (e.g., CAH, AME).
-
3.
Excessive aldosterone synthesis that escapes normal regulatory mechanisms and gives volume-dependent hypertension and suppresses renin release (GRA).
In conclusion, the key points of this review can be summarized, as follows:
-
1.
All monogenic forms of hypertension lead to volume expansion.
-
2.
All monogenic forms of hypertension are associated with low-renin activity (low-renin hypertension).
-
3.
Arterial hypertension with electrolyte disturbances is highly suggestive for monogenic forms of hypertension.
-
4.
To evaluate distal tubular dysfunction (especially the function of the ENaC and mineralocorticoid activity), assess the TTKG, its formula is (potassiumurine*osmolarityplasma)/(potassiumplasma*osmolarityurine). TTKG is high (>2) despite hypokalemia with increased ENaC or mineralocorticoid activity.
-
5.
Urinary steroid hormone analysis and genetic testing are additional tools in the early diagnosis of these disorders.
References
Dave-Sharma S, Wilson RC, Harbison MD et al (1998) Examination of genotype and phenotype relationships in 14 patients with apparent mineralocorticoid excess. J Clin Endocrinol Metab 83:2244–2254
Dluhy RG, Lifton RP (1995) Glucocorticoid-remediable aldosteronism (GRA): diagnosis, variability of phenotype and regulation of potassium homeostasis. Steroids 60:48–51
Ferrari P, Lovati E, Frey FJ (2000) The role of the 11beta-hydroxysteroid dehydrogenase type 2 in human hypertension. J Hypertens 18:241–248
Findling JW, Raff H, Hansson JH et al (1997) Liddle's syndrome: prospective genetic screening and suppressed aldosterone secretion in an extended kindred. J Clin Endocrinol Metab 82:1071–1074
Gordon RD (1986) Syndrome of hypertension and hyperkalemia with normal glomerular filtration rate. Hypertension 8:93–102
Gordon RD, Geddes RA, Pawsey CG et al (1970) Hypertension and severe hyperkalaemia associated with suppression of renin and aldosterone and completely reversed by dietary sodium restriction. Australas Ann Med 19:287–294
Guyton AC, Coleman TG, Cowley AV Jr et al (1972) Arterial pressure regulation. Overriding dominance of the kidneys in long-term regulation and in hypertension. Am J Med 52:584–594
Lifton RP, Dluhy RG, Powers M et al (1992) A chimaeric 11 beta-hydroxylase/aldosterone synthase gene causes glucocorticoid-remediable aldosteronism and human hypertension. Nature 355:262–265
Litchfield WR, Anderson BF, Weiss RJ et al (1998) Intracranial aneurysm and hemorrhagic stroke in glucocorticoid-remediable aldosteronism. Hypertension 31:445–450
Lurbe E, Cifkova R, Cruickshank JK et al (2009) Management of high blood pressure in children and adolescents: recommendations of the European Society of Hypertension. J Hypertens 27:1719–1742
Martinez-Aguayo A, Aglony M, Campino C et al (2010) Aldosterone, plasma renin activity, and aldosterone/renin ratio in a normotensive healthy pediatric population. Hypertension 56:391–396
Milford DV (1999) Investigation of hypertension and the recognition of monogenic hypertension. Arch Dis Child 81:452–455
Morineau G, Sulmont V, Salomon R et al (2006) Apparent mineralocorticoid excess: report of six new cases and extensive personal experience. J Am Soc Nephrol 17:3176–3184
National high blood pressure education program working group on high blood pressure in children and adolescents (2004) The fourth report on the diagnosis, evaluation, and treatment of high blood pressure in children and adolescents. Pediatrics 114:555–576
Nunez BS, Rogerson FM, Mune T et al (1999) Mutants of 11beta-hydroxysteroid dehydrogenase (11-hsd2) with partial activity: improved correlations between genotype and biochemical phenotype in apparent mineralocorticoid excess. Hypertension 34:638–642
Rodriguez-Soriano J, Vallo A (1988) Renal tubular hyperkalaemia in childhood. Pediatr Nephrol (Berlin, Germany) 2:498–509
Shimkets RA, Warnock DG, Bositis CM et al (1994) Liddle's syndrome: heritable human hypertension caused by mutations in the beta subunit of the epithelial sodium channel. Cell 79:407–414
Spitzer A, Edelmann CM Jr, Goldberg LD et al (1973) Short stature, hyperkalemia and acidosis: a defect in renal transport of potassium. Kidney Int 3:251–257
Stowasser M, Bachmann AW, Huggard PR et al (2000) Treatment of familial hyperaldosteronism type I: only partial suppression of adrenocorticotropin required to correct hypertension. J Clin Endocrinol Metab 85:3313–3318
Vehaskari VM (2009) Heritable forms of hypertension. Pediatr Nephrol (Berlin, Germany) 24:1929–1937
Wilson RC, Krozowski ZS, Li K et al (1995) A mutation in the hsd11b2 gene in a family with apparent mineralocorticoid excess. J Clin Endocrinol Metab 80:2263–2266
Yang CL, Angell J, Mitchell R et al (2003) Wnk kinases regulate thiazide-sensitive Na-Cl cotransport. J Clin Investig 111:1039–1045
Conflict of interest
The author declares that he has no conflict of interest and no financial relationships that might have influenced the present work.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Simonetti, G.D., Mohaupt, M.G. & Bianchetti, M.G. Monogenic forms of hypertension. Eur J Pediatr 171, 1433–1439 (2012). https://doi.org/10.1007/s00431-011-1440-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00431-011-1440-7