
Abstract
Decreased height and weight in treated children with classical galactosemia have been reported. However, growth has not been extensively studied. Patients might be at risk for an abnormal growth because of either disease-related intrinsic factors or diet-related factors. The objective was to gain insight in growth in treated children and adolescents with classical galactosemia. The studied population was a previously reported group of 40 classical galactosemia children. Prenatal growth was evaluated using length, weight and head circumference (HC) data from welfare centers or parents. Postnatal growth was evaluated using three height and weight measurements at baseline, 1 and 2 years to calculate growth velocities. Height Z-score was also corrected for target height Z-score (height Z-score divided by target height Z-score). Linear regression analysis was performed between growth velocities, IGF-I, IGFBP-3, dietary intake and galactose-1-phosphate-uridyltransferase activity. We found normal length (median 50.5 cm), weight (median 3,255 grams) and HC (median 33.9 cm) at birth. Mean height growth velocity was 0.87±1.2 for boys and −0.89±2.1 for girls, and mean weight growth velocity was 0.91±1.6 for boys and −0.74±1.3 for girls. Mean height corrected for target height was −1.5±0.9 in girls and −0.6±0.7 in boys. Height growth velocity was correlated with IGF-I (Pearson correlation= 0.499), IGFBP-3 (Pearson correlation 0.4) and height Z-scores corrected for target height Z-scores (Pearson correlation=0.550). Five children grew beyond the age of 18 years. In conclusion, prenatal growth was normal but postnatal growth was affected. Predicted final height is less than target height in most patients; however, target height might be reached for the children who grow beyond the age of 18. Decreased IGF-I and IGFBP-3 and or suboptimal hormonal replacement in girls might play a role.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Classical galactosemia (Mc Kusick 230400) is caused by the deficiency of galactose-1-phosphate-uridyltransferase (GALT, EC 2.7.7.10), the enzyme that converts galactose-1-phosphate to uridine-diphosphate-galactose. Affected children usually present after ingestion of galactose with a neonatal toxic syndrome. Treatment consists of life-long dietary restriction of galactose. Soy products are used as substitute for cow-milk products.
Decreased height in childhood and early adolescence has been reported in treated galactosemia patients [6, 7]. In our study cohort of 40 classical galactosemia children and adolescents, we previously found two children with height <−2 SD scores. In 17 patients, the difference between actual height Z-score and mid-parental target height Z-score was >1.3 SD score (1.3 SD score is regarded as the normal target range) [4]. However, growth has not been extensively studied. The objective of this study was to evaluate growth in children and adolescents with classical galactosemia under dietary treatment.
Patients and methods
Study population
Growth was evaluated in a previously reported group of 40 Dutch children and adolescents (13 boys and 27 girls, median age 7.8 years, range 3.0 to 17.3 years) with classical galactosemia [3, 4]. All patients were of Dutch origin. Diagnosis in all children had been established in the neonatal period by GALT enzymatic studies in erythrocytes and/or by mutation analysis of the GALT gene. Thirty-one patients were prepubertal (Tanner 1). Two patients had Tanner stage 2, one patient had Tanner stage 4, and six patients had Tanner stage 5. Height, weight, weight-for-height, IGF-I and insulin-like growth factor binding protein-3 (IGFBP-3) Z-scores and height Z-score, when compared to mid-parental target height Z-score, had been found decreased. Furthermore, lean tissue mass and fat mass had been found decreased [3, 4]. Median erythrocyte GALT activity was 0.37 μmol/hr.gHb (range 0–0.6; reference range, mean 32.8±5.4 μmol/hr.gHb). All patients followed a galactose-restricted diet, used soy as substitute for dairy products, and had an adequate physical activity pattern. Urinary galactose and galactitol concentrations and galactose-1-phosphate levels in erythrocytes of all patients (markers for diet compliance) were within the range of treated patients. Dietary intake was assessed by means of a food frequency questionnaire adapted for galactosemia and a 3-day food diary. It was assessed every year. None of the patients had a known concomitant disease that could affect growth. At the end of the study period, seven girls were treated with estrogens to induce puberty. There were no patients with untreated delayed puberty.
Prenatal growth
Data on height, weight and HC at birth were collected from infant welfare centers and or parents. Results were corrected for gestational age and expressed in centimeters for height and HC, in grams for weight, and in Z-scores. Z-scores were derived by subtracting the mean value of an age- and gender-matched Dutch reference population from an individual score, and then dividing the difference by the SD of the reference population [1].
Postnatal growth
Height (expressed in cm) and weight (expressed in kg) of all patients were assessed when undressed at baseline and after 1 and 2 years by a single observer. Height and weight growth velocities over the 24-month period were calculated (difference in height divided by time span) and expressed in cm/yr and kg/yr respectively and in Z-scores [1]. Height Z-score was also corrected for target height Z-score (height Z-score – target height Z-score).
Statistical analysis
Normally distributed metric data were expressed as means and SD scores, or as median values with ranges. When metric variables were normally distributed, one-sample t-test was used to test differences with the reference population. Linear regression analysis was carried out between growth velocity data, IGF-I and IGFBP-3 Z-scores, dietary intake (soy, protein and calories) and GALT activity. In order to account for the longitudinal character of the study, ‘patient’ was used as a random factor for the analysis of the growth. A P-value <0.05 was considered statistically significant. All analyses were done with SPSS-pc, version 11.5.
Results
Study population
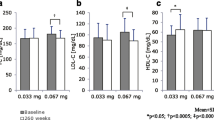
Descriptive characteristics, IGF-I and IGFBP-3 Z-scores and dietary intake data are shown in Table 1.
Prenatal growth
Prenatal growth data corrected for gestational age were within reference ranges (Table 2).
Postnatal growth
Mean height growth velocity in the 2-year study period expressed in Z-scores was 0.87±1.2 (range −0.4 to 3.6) for boys and −0.89±2.1 (range −2.5 to 3.7, p=0.047) for girls. Mean weight growth velocity in the 2-year study period expressed in Z-scores was 0.91±1.6 (range −0.8 to 4.2) for boys and −0.74±1.3 (range −3.1 to 2.3, p=0.008) for girls. Height and weight growth velocities were decreased in girls in contrast to boys (Figs. 1 and 2). Mean height expressed in Z-scores corrected for target height Z-scores (height Z-scores − target height Z-scores) was decreased in both genders, girls (−1.5±0.9, p<0.001) being more affected than boys (−0.6±0.7, p=0.015). Four boys and one girl grew beyond the age of 18 years. Height growth velocity was correlated with IGF-I Z-score (Pearson correlation=0.499, p=0.002), IGFBP-3 Z-score (Pearson correlation=0.4, p=0.014) and also with height Z-scores corrected for target height Z-scores (Pearson correlation=0.550, p<0.001). There was no correlation between height and weight growth velocities and dietary intake (soy, protein and calories) or GALT activity.

Height growth velocities in boys and girls with classical galactosemia

Weight growth velocities in boys and girls with classical galactosemia
Discussion
Growth was studied in a group of 40 galactosemia patients. We found a normal prenatal growth in boys and girls, and decreased height and weight growth velocities in girls. Mean height corrected for target height was decreased in both genders, girls being more affected than boys. Five children grew beyond the age of 18 years. Height growth velocity was correlated with IGF-I Z-score, IGFBP-3 Z-score and with height Z-score corrected for target height Z-score. Predicted final height was less than target height in most patients, but target height might be reached if children grow beyond the age of 18 years.
Decreased height in childhood and early adolescence has been reported in treated galactosemia patients. Waggoner et al. studied height-for-age and weight-for-height data of treated galactosemia patients aged from 2 weeks to 37 years [7]. They found decreased height-for-age and weight-for-height. Final height was within normal limits as growth continued through the late teens; however, height was not related to target height. Schweitzer et al. studied weight, height and head circumferences (HC) of 78 patients with galactosemia aged from 9 months to 33 years [6]. They found decreased weight and height. Ten out of 78 patients were microcephalic at time of assessment, although it is not documented whether HC was corrected for length. They concluded that growth was normal for most patients, but did not include predicted target height in their evaluation.
Data on prenatal growth in classical galactosemia are contradictory. Hsia et al. found reduced birth weight in affected neonates when compared with their unaffected sibs [2]. Waggoner et al. could not confirm this observation [7]. We find normal weight, length and HC at birth, making prenatal growth disturbances unlikely, but did not compare birth data with unaffected sibs.
Longitudinal height growth velocity was abnormal in girls with ovarian dysfunction receiving estrogen replacement therapy, and might partly reflect suboptimal supplementation. The fact that some children grow beyond puberty may be due to delayed puberty.
Possible risk factors for an abnormal growth are either intrinsic or diet-related factors. Normal growth is under hormonal influence, IGF-I being very important [5]. In this limited group of patients, we found decreased mean IGF-I and IGFBP-3 concentrations [4], which may play a role in the decreased growth. Height and height velocity in this group of patients might also be influenced by their soy diet. In this group of classical galactosemia patients, however, no relationship was found between growth velocity data and soy dietary intake.
In conclusion, growth studied in this limited group of classical galactosemia patients reveals normal prenatal growth and decreased height velocity in girls. Mean height corrected for target height was decreased in both genders. Predicted final height is less than target height in most patients; however, target height might be reached for the children who grow beyond the age of 18. Decreased IGF-I and IGFBP-3 might play a role.
Abbreviations
- GALT:
-
galactose-1-phosphate-uridyltransferase
- HC:
-
head circumference
- IGF-I:
-
insulin-like growth factor-I
- IGFBP-3:
-
insulin-like growth factor binding protein-3
References
Gerver WJM, de Bruin R (2001) Paediatric Morphometrics, a reference manual (second extended edition). Universitaire Pers Maastricht, Maastricht, The Netherlands
Hsia DY, Walker FA (1961) Variability in the clinical manifestations of galactosemia. J Pediatr 59:872–883
Panis B, Forget PP, van Kroonenburgh MJ, Vermeer C, Menheere PP, Nieman FH, Rubio-Gozalbo ME (2004) Bone metabolism in galactosemia. Bone 35:982–987
Panis B, Forget PP, Nieman FH, van Kroonenburgh MJ, Rubio-Gozalbo ME (2005) Body composition in children with galactosaemia. J Inherit Metab Dis 28:931–937
Pozo J, Martos-Moreno GA, Barrios V, Argente J (2005) The IGF system in childhood: physiology and clinical implications. J Endocrinol Invest 28:38–42
Schweitzer S, Shin Y, Jakobs C, Brodehl J (1993) Long-term outcome in 134 patients with galactosaemia. Eur J Pediatr 152:36–43
Waggoner DD, Buist NR, Donnell GN (1990) Long-term prognosis in galactosaemia: results of a survey of 350 cases. J Inherit Metab Dis 13:802–818
Acknowledgements
We especially acknowledge all patients with galactosemia and their parents for their participation. We thank Angèle Gerver for her assistance with data analysis. This study was financially supported by a grant from the “Profileringsfonds” of the University Hospital Maastricht and by the Dutch Society for Galactosemia.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Panis, B., Gerver, WJ.M. & Rubio-Gozalbo, M.E. Growth in treated classical galactosemia patients. Eur J Pediatr 166, 443–446 (2007). https://doi.org/10.1007/s00431-006-0255-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00431-006-0255-4