
Abstract
Introduction
In this paper, we evaluated the feasibility of a telemedical (TM) support program and its effect on glycemic control in adolescents with type 1 diabetes mellitus (T1DM). Thirty-six adolescents (m=20, median age at the start of the study: 15.3 years (range: 10.7–19.3 years), median age at diagnosis: 9.3 years (2.1–13.8 years), median duration of disease: 6.4 years (1.0–12.8 years), HbA1c>8%, all on intensified insulin therapy) were randomized in a crossover trial over 6 months (3 months with TM, 3 months with conventional support and paper diary (PD)). During the TM phase, the patients sent their data (date, time, blood glucose, carbohydrate intake, insulin dosage) via mobile phone, at least daily, to our server and diabetologists sent back their advice via short message service (SMS) once a week.
Results
Glycemic control improved during the TM phase, while it deteriorated during the PD phase: TM-PD group HbA1c (%, median (range)): 9.05 (8–11.3) (at 0 months), 8.9 (6.9–11.3) (at 3 months), and 9.2 (7.4–12.6) (at 6 months), and PD-TM group: 8.9 (8.3–11.6), 9.9 (8.1–11), and 8.85 (7.3–11.7) (p<0.05). Patients rated the TM support program to be a good idea. Technical problems with General Packet Radio Service (GPRS) data transmission led to data loss and decreased patient satisfaction.
Conclusion
Our telemedical support program, VIE-DIAB, proved to be feasible in adolescents and helped to improve glycemic control.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The Diabetes Control and Complications Trial (DCCT) clearly demonstrated the importance of lowering HbA1c values by intensive diabetes management in order to reduce the progression of long-term diabetes complications. The DCCT trial also showed that adolescents with type 1 diabetes mellitus (T1DM) less often reached the metabolic targets [7, 8].
More frequent contact with the clinic can improve glycemic control. During the DCCT, the intervention group had their HbA1c evaluated every month, compared to every 3 months in the conventional group, and the intervention group also had frequent contact with their health care providers [6–8]. Such an increased personal contact is usually not considered feasible from the point of view of both the patients and the diabetologists.
The American Diabetes Association recommends clinic visits every 3 months for patients with T1DM [1]. The average median frequency of outpatient visits at our pediatric and adolescent diabetes clinic is 4.3 times per year.
One possibility to intensify the communication between chronically ill patients and the clinic without increasing the time which patients spent at the hospital and the clinical workload of caregivers is by telemedicine (TM), the use of remote communication between patients and a health care center. TM has been shown to improve glycemic control in adult patients with T1DM [2, 3, 11].
We therefore developed a telemedical system and program, VIE-DIAB, in order to try to improve glycemic control in our target group of adolescent patients with T1DM.
The aim of our study was to evaluate whether VIE-DIAB is feasible in adolescents with T1DM and if it would improve their glycemic control.
Methods
Study design
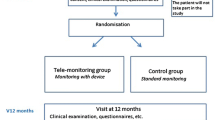
The study was designed as a randomized crossover trial for 6 months. One group started using the VIE-DIAB system (telemedicine, TM) and weekly advice for 3 months, and then switched to the routine scheme with a daily written protocol (paper diary, PD) and a clinical visit after 3 months (TM-PD group), while the other group started with their PD and switched thereafter to TM (PD-TM group). During the PD-TM phase, there was no additional contact scheduled to or from the clinic.
Patients
The power analysis prior to the beginning of the study calculated a patient number of 36 in order to find statistical significance by improving the HbA1c values by 0.5%. Therefore, a total of 36 adolescents with T1DM were randomized into the two groups. Inclusion criteria were an HbA1c≥8% (normal range: 4–6%), a duration of disease>1 year, an age between 10–19 years, and the willingness and consent to participate in our study and to attend follow up visits every 3 months.
All patients (m=20, f=16) were on intensified insulin therapy (2 times long-acting insulin and short-acting insulin analogs (lispro or aspart) for meal boluses), with three of them on a continuous subcutaneous insulin infusion therapy (CSII) with either lispro or aspart insulin. For the patients’ characteristics, see Table 1.
Patients were instructed to measure at least four blood glucose values per day. At the start of the TM phase, the patients were provided with a regular mobile phone (Nokia 3510) and a pre-paid phone card (courtesy of Telecom Austria). They were advised to send their data (date, time, blood glucose, carbohydrate intake, and insulin dosage, divided into short- and long-acting insulin) every time they measured a blood glucose value or at least once daily. They were also asked, for safety reasons, to continue their diary notes during the TM phase. In addition, all patients were informed about the technical features of our program, of the short message service (SMS) communication, and all patients received a manual containing these instructions.
Assessment of glycemic control, complications, and patient satisfaction
HbA1c levels were measured every 3 months during the patients’ routine visits, first at the time of randomization (0 months), then at the time of crossover (3 months), and then at the end of the study (6 months). The HbA1c levels were measured by the DCA 2000+ analyzer (Bayer Corp., Elkhart, IN).
Severe hypoglycemia was defined as loss of consciousness and/or seizure, and was validated by reviewing the patients’ diary and reports by patients or their parents.
Diabetic ketoacidosis was defined was serum pH<7.2, the presence of ketonuria, hyperglycemia, and clinical symptoms (e.g., polyuria, polydipsia, vomiting).
At the end of the TM phase, the patients were asked to complete a questionnaire to assess patient satisfaction about the VIE-DIAB program.
Technical details of the telemedical support program (VIE-DIAB)
VIE-DIAB collects and processes the following data on glycemic control, as received from mobile phone services (SMS, GPRS, WAP) or from a password-protected Internet connection to our server (data forms): date and time, serum glucose value (range 30–1000 mg/dL), short-acting and long-acting insulin dosage (international units, range 0–99), carbohydrate intake (units equal to 12 g glucose or 50 kcal), and additional notes (free text, sports, postprandial value, symptoms of hypoglycemia).
In order to facilitate the data overview for caregivers, the daily serum glucose concentrations are displayed on-screen using specifically designed glyphs (see Figs. 1 and 2).

VIE-DIAB graphic representation of diabetes data (four different views). Bottom: graphical display of glycemic range, carbohydrate units (1 unit equals 12 g carbohydrates) and dosage of various insulins. One glyph shows the serum glucose values according to one of five ranges (hypoglycemia, normal range, slight, moderate, and severe hyperglycemia) and five time periods (morning, late morning, noon, afternoon, evening, late evening)

VIE-DIAB overview data display. Serum glucose values are displayed as glyphs representing the serum glucose values of one day, seven multiples (one week) in a row, four rows (one month) per sheet. If more than one serum glucose value is available within one time period, the highest or a hypoglycemic value is displayed. The relative distribution of the serum glucose values according to the various categories of glycemia is displayed on the right margin
Once weekly, according to the number and level of values within or without the target range, the patients with telemedicine support (TM phase) received either an automatically generated SMS (e.g., glycemic control OK, nothing to be changed), or a personalized message with more specific advice (e.g., increase basal insulin in the morning by 2 IE). The analysis and the specific advice were conducted by the two diabetologists (BR and ES).
Statistical analysis
We used a linear mixed model in order to estimate the association between the dependent variable Hba1c and the independent variables intervention (TM vs. PD) and Hba1c at baseline. The double-logarithm was used for HbA1c in order to achieve normally distributed residuals. A squared term for HbA1c at baseline was included. Additional variables (age, sex, BMI, insulin dosage, severe hypoglycemia, diabetic ketoacidosis) were tested by the same mixed model. Since they turned out to be insignificant, they were excluded in the final model in order to maintain power for the remaining variables.
The model was estimated with the procedure “proc mixed” in SAS version 8.2 [13].
Results
Metabolic control
All 36 patients completed the 6-month trial. Our primary end point was glycemic control, as indicated by HbA1c levels. Glycemic control improved during the TM phase, while it deteriorated during the PD phase: TM-PD group HbA1c (%, median (range)): 9.05 (8–11.3) (at 0 months), 8.9 (6.9–11.3) (at 3 months), and 9.2 (7.4–12.6) (at 6 months), and PD-TM group: 8.9 (8.3–11.6), 9.9 (8.1–11), and 8.85 (7.3–11.7) (p<0.05). The changes in HbA1c are displayed in Fig. 3.

The change of HbA1c during each of the 3-month periods (medians). The range in the TM-PD group is −1.7 to 1.9 (at 3 months) and −1.6 to 2.8 (at 6 months), and −0.6 to 1.8 and −2.2 to 1.8 in the PD-TM group
Nine patients (25%), despite weekly attempts of motivation via SMS, sent only <50% of the required four daily blood glucose values. Comparing the metabolic control of this subset of patients to that of patients who sent >50% of the required four daily blood glucose values, we could not see a statistically significant difference.
Analysis of adverse events, such as severe hypoglycemia or diabetic ketoacidosis, was similar in both groups: no severe hypoglycemia, but two events of diabetic ketoacidosis where observed (in two different patients), one during the TM phase, one during the PD phase.
BMI (kg/m2) and insulin dosage (IE/kg/d) were not different between the two groups, and there was no influence of age, sex, or social background on metabolic control.
Technical problems
During the TM phase, we had to face some technical difficulties which were not related to our telemedical system, but to GPRS (General Packet Radio Service) access. GPRS was not available in some geographical areas and network capacity overload/connection problems were reported several times by 26/36 patients, resulting in error messages. These problems occurred especially at weekends, when the network was busy or the patients were on holidays.
Patient satisfaction
The results of the Telemedicine Patient Satisfaction Survey are shown in Table 2. The questionnaire, which was developed by our team for this study, was answered during the clinic visit after the TM phase.
Discussion
Our pilot study demonstrated that our telemedical (TM) support program VIE-DIAB is feasible. We observed a trend to improved glycemic control during the TM phase (p<0.05), while HbA1c deteriorated during the PD phase (Fig. 3). At the end of the study, the HbA1c values in both groups reached almost the same endpoint (median (range): TM-PD group: 9.2 (7.4–12.6), PD-TM group: 8.85 (7.3–11.7%), similar to the one at the beginning of the study.
The technical problems with General Packet Radio Service (GPRS) communication were, possibly, a negative factor for patient motivation.
Analysis of the questionnaires about patient satisfaction led to the following conclusions: most patients thought that the VIE-DIAB system was useful for their diabetes management. Entering and sending the values took most of them about 1 minute or less, but the majority still rated this as too time consuming. This reflects the reluctance of adolescents to document and record their blood glucose values for various reasons. Clinicians have noticed problems with paper-based diaries (e.g., back-filling, not writing at all, etc.), which are well-known problems, especially during adolescence [14].
The additional communication with the diabetologists during the TM phase was perceived to be positive, the technical problems with the GPRS system probably influenced overall satisfaction and willingness to continue the program.
Overall satisfaction with VIE-DIAB was good. The patients mainly criticized the additional workload and GPRS access problems. Mainly due to these problems, the patients rated that the system is time consuming and only about half of them would have wanted to continue with the VIE-DIAB-system.
Diabetologists consider adolescents as a difficult to treat age group. The Diabetes Control and Complications Trial (DCCT) showed that, despite the same effort in all age groups, adolescents had the worst glycemic control [7, 8]. The Hvidore study group reported that glycemic control deteriorated over a 3-year period in a large group of adolescents, even though the number and amount of daily insulin injections increased [9].
In adult patients with type 1 diabetes mellitus (T1DM), various telemedical support programs have improved glycemic control [2, 3, 11]. In a group of 10 adults with excellent metabolic control, the use of TM had no impact on HbA1c during a 6-month trial [12]. In adolescents, the use of telemedical support programs is still rare, although this age group uses all kinds of telecommunication services in their daily life. One group from Colorado published a study with adolescents who electronically transmitted self-monitored blood glucose values and other diabetes related data. Additionally, they received phone calls from their health care providers to discuss the treatment. Compared to the control group, the study group could not improve glycemic control, but reduced costs and decreased need for clinical visits were the positive findings [4]. In a publication by Howells et al. [10], the authors could not see an improvement of metabolic control after a 1-year observation period, but they did observe a significant improvement in self-efficacy. In addition, an Italian group published data about the improvement of glycemic control in adolescents with T1DM in their T-IDDM project, but the number of patients participating was very small (n=6) [5].
We did not analyze the cost-effectiveness of our study, but the telecommunication costs per month were rather low (about €4). The diabetologists reviewed the data during their routine working hours. It took them about 30 min per week to review the data and to reply by SMS to the patients, whereas a routine clinic visit takes about 20–30 min per patient.
In conclusion, the telemedical support program VIE-DIAB proved to be feasible in adolescents, despite the technical problems, and glycemic control improved during the TM phase. We estimate that, after a reduction of the GPRS-related technical problems, the patient satisfaction would also improve.
Several telemedical projects are currently being developed. In the future, a blood glucose meter integrated into a mobile phone with automatic data transmission should facilitate data transfer and, thus, improve patient compliance. To improve glycemic control, a feedback option to our opinion is necessary. However, the key point in the diabetes care of adolescents remains the difficult task of motivating the patients with T1DM in this age group.
Abbreviations
- T1DM:
-
Type 1 diabetes mellitus
- TM:
-
Telemedicine/telemedical
- PD:
-
Paper diary
- BMI:
-
Body mass index
- DCCT:
-
The Diabetes Control and Complications Trial
- SMS:
-
Short message service
- GPRS:
-
General Packet Radio Service
References
American Diabetes Association (1999) Clinical practice recommendations. Diabetes Care 22(Suppl 1):S35
Bellazzi R, Montani S, Riva A, Stefanelli M (2001) Web-based telemedicine systems for home-care: technical issues and experiences. Comput Methods Prog Biomed 64(3):175–187
Biermann E, Dietrich W, Rihl J, Standl E (2002) Are there time and cost savings by using telemanagement for patients on intensified insulin therapy? A randomised, controlled trial. Comput Methods Programs Biomed 69(2):137–146
Chase HP, Pearson JA, Wightman C, Roberts MD, Oderberg AD, Garg SK (2003) Modem transmission of glucose values reduces the costs and need for clinic visits. Diabetes Care 26(5):1475–1479
d’Annunzio G, Belazzi R, Larizza C, Montani S, Pennati C, Castelnovi C, Stefanelli M, Rondini G, Lorini R (2003) Telemedicine in the management of young patients with type 1 diabetes mellitus: a follow-up study. Acta Biomed Ateneo Parmese 74(Suppl 1):49–55
The DCCT Research Group (1987) Diabetes control and complications trial (DCCT): results of feasibility study. Diabetes Care 10(1):1–19
The DCCT Research Group (1993) The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. N Engl J Med :329(14):977–986
The DCCT Research Group (1994) Effect of intensive diabetes treatment on the development and progression of long-term complications in adolescents with insulin-dependent diabetes mellitus. J Pediatr 125(2):177–188
Holl RW, Swift PG, Mortensen HB, Lynggaard H, Hougaard P, Aanstoot HJ, Chiarelli F, Daneman D, Danne T, Dorchy H, Garandeau P, Greene S, Hoey HM, Kaprio EA, Kocova M, Martul P, Matsuura N, Robertson KJ, Schoenle EJ, Sovik O, Tsou RM, Vanelli M, Aman J (2003) Insulin injection regimens and metabolic control in an international survey of adolescents with type 1 diabetes over 3 years: results from the Hvidore study group. Eur J Pediatr 162(1):22–29
Howells L, Wilson AC, Skinner TC, Newton R, Morris AD, Greene SA (2002) A randomized control trial of the effect of negotiated telephone support on glycaemic control in young people with Type 1 diabetes. Diabet Med 19(8):643–648
Montori VM, Smith SA (2001) Information systems in diabetes: in search of the holy grail in the era of evidence-based diabetes care. Exp Clin Endocrinol Diabetes 109(Suppl 2):S358–S372
Perlemuter L, Yomtov B (2002) Feasibility and usefulness of dedicated software and e-mail for self-monitoring blood glucose in treating diabetes. Diabet Med 19(8):701–702
SAS Institute (1999) SAS/STAT user’s guide, version 8. SAS Institute Inc., Cary, North Carolina
Stone AA, Shiffman S, Schwartz JE, Broderick JE, Hufford MR (2002) Patient non-compliance with paper diaries. BMJ 324(7347):1193–1194
Acknowledgment
This project was, in part, sponsored by Telecom Austria.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Rami, B., Popow, C., Horn, W. et al. Telemedical support to improve glycemic control in adolescents with type 1 diabetes mellitus. Eur J Pediatr 165, 701–705 (2006). https://doi.org/10.1007/s00431-006-0156-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00431-006-0156-6