
Abstract
Ibuprofen (IBU) has previously been shown to be as effective as indomethacin (INDO) in closing the patent ductus arteriosus (PDA) of preterm infants, without severely affecting renal hemodynamics or basal cerebral blood flow. We conducted a meta-analysis of randomized trials to compare the efficacy and safety of IBU and INDO for treatment of PDA. Data from the nine relevant trials ( n =566), showed no significant difference in the efficacy of IBU and INDO in PDA closure ( P =0.70). However, five trials ( n =443) provided serum creatinine concentration data that revealed a significantly lower increase favoring IBU ( P < 0.001), and urine output data that showed a significantly lower decrease favoring IBU ( P < 0.001). In two trials ( n =188) the proportion of infants who required postnatal oxygen therapy at 28 days (defined as chronic lung disease) was significantly higher with IBU (52/94; 55.3%) than with INDO (38/94; 40.4%, P < 0.05). No statistically significant differences were found in mortality, intraventricular hemorrhage, necrotizing enterocolitis, surgical ligation, sepsis, retinopathy of prematurity, periventricular leukomalacia, length of hospital stay, gastrointestinal bleeding, re-opening of PDA, back-up treatment, surfactant therapy, or days on a ventilator. Conclusion:ibuprofen and indomethacin have similar efficacy in patent ductus arteriosus closure, but preterm infants treated with ibuprofen experience lower serum creatinine values, higher urine output, and less undesirable decreased organ blood flow and vasoconstrictive adverse effects.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Ibuprofen (IBU), a non-steroidal drug commonly used as an antipyretic, analgesic and anti-inflammatory agent, has also been used for closure of symptomatic patent ductus arteriosus (PDA) [20, 22, 29, 30,32]. PDA has been associated with increased neonatal morbidity, such as chronic lung disease, intraventricular hemorrhage (IVH) and apnea [8,13]. The conventional pharmacologic treatment for PDA closure is indomethacin (INDO) [12]; however, this drug has been associated with adverse events such as necrotizing enterocolitis (NEC) [11,14]. The recent availability of an intravenous preparation of IBU lysine has allowed the performance of clinical trials comparing IBU with saline (placebo) [9], a control group [24], or with INDO [15, 20, 22, 23, 24, 25, 28, 29,30]. These published data suggest that IBU is superior to placebo and at least equi-active with INDO in PDA closure. A meta-analysis of the efficacy and adverse effects was performed to determine whether there is a therapeutic advantage of IBU compared to INDO for use in the preterm newborn infant.
Methods
Inclusion criteria
Studies selected for inclusion tested the same primary hypothesis (PDA closure rate), using similar patient characteristics (gestational age ≤37 weeks; weight ≤2500 g), with an echocardiographically confirmed PDA. Random allocation to treatment groups and concealment of allocation had to be met to satisfy inclusion: inadequate allocation concealment, despite the use of randomization, allows a risk of selection bias. Methods of assignment such as date of birth and case record numbers are open to manipulation and were not accepted. IBU and INDO groups must have differed only by the drug type assignment. All comparisons between treatment groups had to be free of confound by additional agents or co-interventions.
Identification of trials
The search strategy employed computerized bibliographic searches of MEDLINE (1996–2003), the Cochrane Controlled Trials Register (2003), EMBASE (1980–2003) and abstracts published in Pediatric Research (1991–2003). Both published and unpublished trials were included in an effort to control for publication bias. Citations of appropriate studies were verified by reviewing the bibliographies and reference lists of identified trials. Identified titles of abstracts with potential relevance were downloaded and full manuscripts were then obtained for all abstracts deemed relevant, based upon the inclusion criteria. Nine trials met inclusion criteria: eight published studies and one published abstract.
Data collected and primary outcome
Data on 25 clinically relevant outcome measures: PDA closure; serum creatinine; urine output; mortality; IVH; NEC; surgical ligation; sepsis; retinopathy of prematurity; periventricular leukomalacia; length of hospital stay; gastrointestinal bleeding; re-opening of PDA; back-up treatment; surfactant therapy; days on a ventilator; bronchopulmonary disease; fractional excretion of sodium; inspired oxygen concentration; food intolerance; mean airway pressure; oliguria development; oxygen therapy after 28 days; number of ventilated neonates; and maternal corticosteroid use, were initially identified for extraction. Two reviewers (RLT and JVA) independently extracted data from the same articles using a data extraction sheet and subsequently compared results for agreement. The data obtained were checked for consistency between reviewers, integrity of randomization and concealment of allocation. Questions regarding the interpretability of certain data values were resolved by the same two reviewers. The final database entries were verified by the statistician. Few studies satisfied criteria for inclusion on every data variable. Where necessary, authors of selected studies were contacted to verify extracted data values derived from graphs. Documentation is available upon request.
Statistical analyses
Comprehensive Meta-Analysis [4], a stand-alone program, was used to synthesize data obtained from the nine trials. Briefly, the analysis software produces a Forrest plot as a schematic description of the meta-analysis results. The program is augmented using accepted computational algorithms. Where appropriate, results were reported using a pooled relative risk (RR). For continuous outcomes, the weighted mean difference (WMD) was calculated using the largest mean difference reported, irrespective of time point collected. The 95% confidence intervals (CI) were reported around the weighted effect size based on a fixed-effects model.
As only a small number of studies met the inclusion criteria, a fixed effects model was used as opposed to the random-effects model. The fixed effects model that was used treats each neonate as the unit of analysis nested within studies, yielding a more powerful test of an overall hypothesis [7]. Under the fixed effects model, the assumption is made that all studies come from a common population. Therefore, the only source of study-to-study variation is random error, which tends to zero as sample size increases. This approach is mirrored in the computational formula, with the only source of error identified as within-study error.
Variability (heterogeneity) among the obtained effects sizes was formally operationalized using a chi-squared test of significance. The formula for heterogeneity assesses the dispersion of individual outcomes, vis-à-vis the combined effect, and denotes this value using a Q statistic [7]. The formula computes the squared distance of each study from the combined effect and weights each value, giving a greater weight to more precise studies.
Results
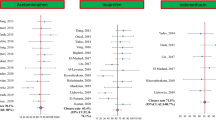
The author, year, methodology, sample size, and dose for each of the nine studies selected for inclusion in the meta-analysis are listed in Table 1 [15, 20, 22, 23, 24, 25, 28, 29,30]. Although all nine studies were randomized clinical trials, only five of the nine clearly indicated that they were double blinded. For the primary measure of PDA closure ( n =566), there was no significant difference between IBU and INDO (Fig. 1; RR 1.02; CI 0.94, 1.10; P =0.70; Q = 2.60, P =0.96).

PDA closure
Five trials [15, 24, 28, 29,30] reported serum creatinine levels. Table 2 provides the mean and standard deviation values for serum creatinine output given the largest mean difference reported, irrespective of time point. The largest mean difference occurred on day 8 in three trials [15, 24,29], day 2 in one trial [28], and day 3 in another [30]. Meta-analysis of these trials (Fig. 2; n =443) revealed a significantly lower increase favoring IBU treatment (WMD 0.44; SE 0.10; CI 0.25, 0.63; P <0.001; Q = 1.03; P =0.90).

Serum creatinine levels
The same five trials [15, 24, 28, 29,30] also reported urine output. Table 3 provides the mean and standard deviation values for urine output obtained from each trial. The largest mean difference in urine output recorded in two trials [24,29] was found on day 3. The largest mean difference in one trial occurred on day 5 [30]. In two trials [15,28], significantly different urine values occurred 24 h after commencement of treatment. Meta-analysis (Fig. 3; n =443) showed a significantly lower decrease favoring IBU treatment (WMD 0.74; SE 0.10; CI 0.55, 0.94; P <0.001; Q = 12.0; P ≤0.02). The presence of a significant Q value indicated evidence of heterogeneity. An examination of the Forrest plot was conducted to assess the clinical meaning of this dispersion. Two studies [24,29] with the smallest sample sizes ( n =40; n =17, respectively) had approximately two to four times larger effect sizes (1.32 and 2.85, respectively) than the statistically significant effect sizes (0.73, 0.58) reported by the two studies with the largest sample sizes [15,30] ( n =148; n =175 respectively).

Urine output
Three trials [20, 28,29] ( n =267) indicated IVH occurred similarly using either drug, but slightly higher for INDO (20/74; 27.0%) than IBU (15/74; 20.3%) in a fourth [30] (RR 0.73; CI 0.45, 1.20; P =0.22; Q = 0.26; P =0.97).
In two trials [29,30] ( n =188) the proportion of infants who required oxygen therapy postnatally at 28 days (defined as chronic lung disease) was significantly higher with IBU (52/94; 55.3%) use than with INDO (38/94; 40.4%) (RR 1.37; CI 1.01, 1.86; P ≤0.04; Q = 0.04; P =0.84).
Other measures for which there were no statistically significant differences between IBU and INDO, were analyzed from six of the nine studies [20, 24, 25, 28, 29,30]: NEC ( n =426) (RR 0.62; CI 0.27, 1.41; P =0.26; Q = 0.39; P =0.95); surgical ligation ( n =500) (RR 0.96; CI 0.58, 1.56; P =0.85; Q = 2.61; P =0.76); sepsis ( n =396) (RR 1.27; CI 0.60, 2.68; P =0.53; Q = 1.22; P =0.75); retinopathy of prematurity ( n =103) (RR 0.74; CI 0.40, 1.35; P =0.33; Q = 0.26; P =0.61); periventricular leukomalacia ( n =386) (RR 0.93; CI 0.47, 1.83; P =0.84; Q = 2.61; P =0.27); bleeding defined as either occult blood in the stool, gastric bleeding, or localized bowel perforation (n=426) (RR 0.86; CI 0.28, 2.70; P =0.80; Q = 1.57; P =0.67); back-up treatment ( n =221) (RR 1.46; CI 0.76, 2.81; P =0.26; Q = 0.67; P =0.72); surfactant therapy ( n =363) (RR 0.96; CI 0.87, 1.07; P =0.48; Q = 5.97; P =0.05), or days on a ventilator ( n =278) (RR 0.17; CI −0.07, 0.41; P =0.16; Q = 1.14; P =0.57), re-opening of the PDA ( n =325) (RR 1.34; CI 0.52, 3.45; P =0.55; Q = 0.76; P =0.98). Four trials [15, 20, 28,30] ( n =426) revealed no significant differences in mortality rate (RR 0.99; CI 0.53, 1.84; P =0.97, Q = 3.19; P =0.36).
Discussion
This meta-analysis confirms that IBU and INDO have similar efficacy in PDA closure. Moreover, based upon the comparative findings for serum creatinine and urine, IBU has significantly less toxic vasoconstrictive adverse effects than INDO relative to renal tolerance. A previously published meta-analysis [21] has been registered with the Cochrane Library comparing IBU and INDO for closure of PDA. However, this current analysis expands the number of clinical trials entered into the analysis and updates clinically relevant findings. Although the need for oxygen therapy at 28 days postnatally was found to be significantly more likely to occur with IBU use than INDO, it must be pointed out that only two of the nine studies included in this meta-analysis collected data for this outcome, conducted by the same investigator [29,30]. Nevertheless, if this outcome is defined by some clinicians as chronic lung disease, a word of caution should be mentioned for the still not fully elucidated possible toxic effects of IBU on this specific outcome.
Two investigations comparing IBU and INDO reported cerebral blood flow (CBF) and cerebral blood volume (CBV) data [20,23], but variation in collection time points and differences in technical and quantitative approaches precluded their contributing to the meta-analysis. It was reported [20] that INDO caused a significant reduction of CBV, a reduction in oxidized cytochrome oxidase concentration and CBF velocity, but a significant increase in CBV with IBU after 60 min. Although caution should be exercised in distinguishing changes in CBV relative to an arbitrary baseline from absolute CBV measurements, the conclusion was that treatment with IBU has less adverse effects on cerebral perfusion and oxygen availability compared to INDO. Similarly, the second study [23] reported significant reductions in CBF and CBV as well as changes in cerebral oxygen delivery after the first dose of INDO but not after the first dose of IBU. Significant differences in CBF, CBV, and cerebral oxygen delivery also occurred after a 24 h dose of INDO, but not after the 24 h dose of IBU. Both investigations found similar efficacy in PDA closure, but concluded that IBU, unlike INDO, had no adverse effects on cerebral hemodynamics.
Treatment with INDO, and not IBU, significantly reduced mesenteric and renal blood flow velocity [24]. Mesenteric and renal blood flow velocity changes in peak systolic velocity, mean velocity, and end-diastolic velocity were significantly different between the two treatments at 30 min. Both drugs caused a significant increase in relative vascular resistance at 30 min which returned to pre-treatment levels at 60 min with IBU but did not return to pre-treatment levels even 120 min after treatment with INDO.
Lastly, a significantly higher incidence of oliguria ( P ≤0.03) has been reported [30] in infants treated with INDO (14/74; 19%), as compared to IBU (5/74; 7%), observed during the 3 days after commencement of treatment.
Concerns have been raised regarding bilirubin-drug-albumin interactions. In vitro studies suggest that high IBU doses particularly at high bilirubin:albumin molar ratios may potentially displace bilirubin from the albumin binding sites, therefore increasing the risk for kernicterus [1, 2,3]. However, measurements of free bilirubin using the horseradish peroxidase assay [31] at therapeutic doses of IBU showed no increase in the free bilirubin in preterm newborns given ibuprofen. These observations [2, 3,31] support the lack of bilirubin toxicity noted in the clinical trials reviewed in this meta-analysis. Concern has also been noted by the occurrence of pulmonary hypertension in three infants after administration of prophylactic IBU [21]. Reasons given have focused on early administration of IBU (<6 h) preventing a normal drop in pulmonary vascular resistance and/or acidification of the IBU solution (buffered with tromethamine) itself resulting in precipitation and microembolism in the lungs. However, this adverse effect was not observed in any of the nine studies which fulfilled the inclusion criteria in this review. There are two available formulations of intravenous IBU namely IBU-tris-hydroxyamino-methane and IBU l -lysine. The problem of neonatal pulmonary hypertension was observed with IBU-tris-hydroxyamino-methane , not with IBU l -lysine. Given these findings, appropriate caution should be considered when IBU-tris-hydroxyamino-methane is used. Therefore, based upon the currently available data, we cannot support the conclusion of the previous review which included eight studies ( n =509) [21]. We conclude that treatment with IBU is significantly less likely to cause renal dysfunction in preterm infants in comparison to INDO, with similar efficacy in PDA closure. Therefore, it is questionable at best that INDO still remains the drug of choice for treatment of PDA.
This meta-analysis did not address long-term outcome of IBU and INDO treatment, since there are no published data for IBU. However, It is noteworthy that despite a substantial reduction in IVH and a significant increase in PDA closure by INDO [10, 17,26] there is minimal or no evidence of improved neurosensory or pulmonary outcomes at 18 to 21 months follow-up and even up to school age [18, 19, 27,33]. INDO significantly decreases CBF and mitochondrial oxidative function in animals and human newborns [5,16] and inferentially perturbs neuronal function. In contrast, IBU exerts no effect on cerebral and mesenteric blood flow [5, 6, 20, 23,24] and probably has little effect on cerebral perfusion. Whether IBU will prove to have a positive impact on later neurological outcome remains to be seen.
Strengths and limitations regarding meta-analysis
Critics of meta-analysis argue that some inherent bias in the sampling of trials exists as a result of the inclusion/exclusion criteria and the methodology selected to review the literature. Further, not every computer-assisted search will be exhaustive, nor is every piece of data collected on the topic obtainable, as some data are just not published.
However, concerns about publication bias in favor of statistically significant results can be addressed, albeit weakly, using statistical procedures for detecting funnel plot asymmetry. Still, some biases are not so readily apparent. A frustration in conducting a meta-analysis is when there is simply not enough data information, in the correct scaling format, to compute an effect size. No carefully collected data from well-designed randomized trials should ever be wasted. Unfortunately, data are wasted all the time: non-significant results that remain unreported in anticipation of rejection by journals; small sample studies that alone do not achieve statistical significance. Nevertheless, the cumulative techniques of meta-analysis allow such data to have meaning; investigators can provide answers to clinical questions that might not be available from a collection of conflicting research findings. The successful application of meta-analytical techniques in both the medical and pharmaceutical fields rests on uniform data reporting in individual clinical trials. Ideally, standards governing the content, format, and reporting of statistical aspects should be developed and adopted to guide authors. In this aspect, meta-analysis could best allow clinical investigators to arrive at conclusions that are more accurate and more credible than could ever be presented by any one primary study or in a non-quantitative, narrative review.
Abbreviations
- CBF :
-
cerebral blood flow
- CBV :
-
cerebral blood volume
- CI :
-
confidence interval
- IBU :
-
ibuprofen
- INDO :
-
indomethacin
- IVH :
-
intraventricular hemorrhage
- NEC :
-
necrotizing enterocolitis
- PDA :
-
patent ductus arteriosus
- RR :
-
relative risk
- WMD :
-
weighted mean difference
References
Ahlfors CE (2004) Effect of ibuprofen on bilirubin-albumin binding. J Pediatr 144: 386–388
Ambat MTC, Ostrea EM Jr, Aranda JV (2002) Influence of ibuprofen l -lysinate (IBU) on bilirubin binding to albumin. Pediatr Res APS-SPR 51: 344A
Ambat MTC, Ostrea EM Jr, Aranda JV (2003) Influence of ibuprofen l -lysinate (IBU) on bilirubin albumin binding as determined by the saturation index and horseradish peroxidase tests. Pediatr Res APS-SPR 53: 365A
Biostat Inc (1999) Comprehensive Meta-Analysis: a computer program for research synthesis
Chemtob S, Laudignon N, Beharry K, Rex J, Varma D, Wolfe L, Aranda JV (1990) Effects of prostaglandins and indomethacin on cerebral blood flow and cerebral oxygen consumption of conscious newborn piglets. Dev Pharmacol Ther 14: 1–14
Chemtob S, Beharry K, Barna T, Varma DR, Aranda JV (1991) Differences in the effects in the newborn piglet of various nonsteroidal antiinflammatory drugs on cerebral blood flow but not on cerebrovascular prostaglandins. Pediatr Res 30: 106–111
Cohen J (1994) The earth is round (P-less-than.05). American Psychologist 49: 997–1003
Cotton RB, Stahlman MT, Bender HW, Graham TP, Catterton WZ, Kovar I (1978) Randomized trial of early closure of symptomatic patent ductus arteriosus in small preterm infants. J Pediatr 93: 647–651
De Carolis MP, Romagnoli C, Polimeni V, Piersigilli F, Zecca E, Papacci P, Delogu AB, Tortorolo G (2000) Prophylactic ibuprofen therapy of patent ductus arteriosus in preterm infants. Eur J Pediatr 159: 364–368
Fowlie PW (2000) Intravenous indomethacin for preventing mortality and morbidity in very low birth weight infants. Cochrane Database Syst Rev CD000174
Fujii AM, Brown E, Mirochnick M, O’Brien S, Kaufman G (2002) Neonatal necrotizing enterocolitis with intestinal perforation in extremely premature infants receiving early indomethacin treatment for patent ductus arteriosus. J Perinatol 22: 535–540
Gersony WM (1986) Patent ductus arteriosus in the neonate. Pediatr Clin North Am 33: 545–560
Gersony WM, Peckham GJ, Ellison RC, Miettinen OS, Nadas AS (1983) Effects of indomethacin in premature infants with patent ductus arteriosus: results of a national collaborative study. J Pediatr 102: 895–906
Grosfeld JL, Chaet M, Molinari F, Engle W, Engum SA, West KW, Rescorla FJ, Scherer LR III (1996) Increased risk of necrotizing enterocolitis in premature infants with patent ductus arteriosus treated with indomethacin. Ann Surg 224: 350–355
Lago P, Bettiol T, Salvadori S, Pitassi I, Vianello A, Chiandetti L, Saia OS (2002) Safety and efficacy of ibuprofen versus indomethacin in preterm infants treated for patent ductus arteriosus: a randomised controlled trial. Eur J Pediatr 161: 202–207
Laudignon N, Chemtob S, Bard H, Aranda JV (1988) Effect of indomethacin on cerebral blood flow velocity of premature newborns. Biol Neonate 54: 254–262
Ment LR, Oh W, Ehrenkranz RA, Philip AG, Vohr B, Allan W, Duncan CC, Scott DT, Taylor KJ, Katz KH (1994) Low-dose indomethacin and prevention of intraventricular hemorrhage: a multicenter randomized trial. Pediatrics 93: 543–550
Ment LR, Vohr B, Oh W, Scott DT, Allan WC, Westerveld M, Duncan CC, Ehrenkranz RA, Katz KH, Schneider KC, Makuch RW (1996) Neurodevelopmental outcome at 36 months’ corrected age of preterm infants in the Multicenter Indomethacin Intraventricular Hemorrhage Prevention Trial. Pediatrics 98: 714–718
Ment LR, Vohr B, Allan W, Westerveld M, Sparrow SS, Schneider KC, Katz KH, Duncan CC, Makuch RW (2000) Outcome of children in the indomethacin intraventricular hemorrhage prevention trial. Pediatrics 105: 485–491
Mosca F, Bray M, Lattanzio M, Fumagalli M, Tosetto C (1997) Comparative evaluation of the effects of indomethacin and ibuprofen on cerebral perfusion and oxygenation in preterm infants with patent ductus arteriosus. J Pediatr 131: 549–554
Ohlsson A, Walia R, Shah S (2003) Ibuprofen for the treatment of a patent ductus arteriosus in preterm and/or low birth weight infants. Cochrane Database Syst Rev CD003481
Patel J, Marks KA, Roberts I, Azzopardi D, Edwards AD (1995) Ibuprofen treatment of patent ductus arteriosus. Lancet 346: 255
Patel J, Roberts I, Azzopardi D, Hamilton P, Edwards AD (2000) Randomized double-blind controlled trial comparing the effects of ibuprofen with indomethacin on cerebral hemodynamics in preterm infants with patent ductus arteriosus. Pediatr Res 47: 36–42
Pezzati M, Vangi V, Biagiotti R, Bertini G, Cianciulli D, Rubaltelli FF (1999) Effects of indomethacin and ibuprofen on mesenteric and renal blood flow in preterm infants with patent ductus arteriosus. J Pediatr 135: 733–738
Plavka R, Svihovec P, Borek I, Biolek J, Kostirova M, Liska K, Kopecky P, Sebron V, Zlatohlavkova B, Ruffer J, Dokoupilova M (2001) Ibuprofen vs indomethacin in the treatment of patent ductus arteriosus in very premature neonates. Pediatr Res APS-SPR 49: 375A
Schmidt B, Davis P, Moddemann D, Ohlsson A, Roberts RS, Saigal S, Solimano A, Vincer M, Wright LL (2001) Long-term effects of indomethacin prophylaxis in extremely-low-birth-weight infants. N Engl J Med 344: 1966–1972
Schmidt B, Asztalos EV, Roberts RS, Robertson CM, Sauve RS, Whitfield MF (2003) Impact of bronchopulmonary dysplasia, brain injury, and severe retinopathy on the outcome of extremely low-birth-weight infants at 18 months: results from the trial of indomethacin prophylaxis in preterms. JAMA 289: 1124–1129
Su PH, Chen JY, Su CM, Huang TC, Lee HS (2003) Comparison of ibuprofen and indomethacin therapy for patent ductus arteriosus in preterm infants. Pediatr Int 45: 665–670
Van Overmeire B, Follens I, Hartmann S, Creten WL, Van Acker KJ (1997) Treatment of patent ductus arteriosus with ibuprofen. Arch Dis Child Fetal Neonatal Ed 76: F179–F184
Van Overmeire B, Smets K, Lecoutere D, Van de Broek H, Weyler J, De Groote K, Langhendries JP (2000) A comparison of ibuprofen and indomethacin for closure of patent ductus arteriosus. N Engl J Med 343: 674–681
Van Overmeire B, Vanhagendoren S, Schepens PJ, Ahlfors CE (2004) The influence of ibuprofen-lysine on unbound bilirubin plasma levels in preterm neonates. Pediatr Res APS-SPR 55: 474A
Varvarigou A, Bardin CL, Beharry K, Chemtob S, Papageorgiou A, Aranda JV (1996) Early ibuprofen administration to prevent patent ductus arteriosus in premature newborn infants. JAMA 275: 539–544
Vohr BR, Allan WC, Westerveld M, Schneider KC, Katz KH, Makuch RW, Ment LR (2003) School-age outcomes of very low birth weight infants in the indomethacin intraventricular hemorrhage prevention trial. Pediatrics 111: e340–e346
Author information
Authors and Affiliations
Corresponding author
Additional information
No internal or external funding source existed for this review. All authors listed had a role in study design, data collection, data analysis, data interpretation, and writing of the manuscript.
Rights and permissions
About this article
Cite this article
Thomas, R.L., Parker, G.C., Van Overmeire, B. et al. A meta-analysis of ibuprofen versus indomethacin for closure of patent ductus arteriosus. Eur J Pediatr 164, 135–140 (2005). https://doi.org/10.1007/s00431-004-1596-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00431-004-1596-5