
Abstract
This study was aimed at investigating the clinicopathological characteristics of tubal metastases originating from primary endometrial, cervical, and nongynecological malignancies. We performed a 4-year retrospective study in which fallopian tube tissues obtained from 60 patients with tubal metastases were examined. In addition, we compared the number of tubal metastasis cases detected during periods of representative or whole tubal sampling. Twenty-three and 37 tubal metastases were found in cases examined after representative and whole tubal sampling techniques, respectively. Four cases of microscopic tubal metastases were detected via whole sampling, whereas no microscopic lesions were identified via representative sampling. The metastatic lesions originated from 14 uterine (10, endometrium; 4, cervix) and 46 nongynecological tumors (21, colon; 15, stomach; 5, biliary; 3, appendix; 2, breast). Tumors were most commonly involved in the muscle and lamina propria (n = 17). We noted distinctive histopathological features according to the extent of mural involvement: fibromyxoid stromal reaction and lymphohistiocytic infiltration in tumors involving the muscle and subepithelial connective tissue, architectural alterations of plicae in those involving the subepithelial connective tissue, and intraluminal mucinous and inflammatory exudate adjacent to intraepithelial tumors. We observed distinctive histopathological features associated with tubal metastases according to the extent of mural involvement. In addition, we demonstrated that the sampling method used in the routine microscopic examination of the fallopian tube affects the detection of tubal metastases. Our data support the notion that it is more logical to thoroughly sample both the fimbrial ends and the nonfimbriated portions of fallopian tubes for all salpingectomy specimens in the setting of cancer surgery.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Metastasis to the pelvic cavity is a commonly observed phenomenon in advanced-stage gynecological and nongynecological malignancies [1]. The pelvic cavity can be the only site of metastasis, and the symptoms associated with a pelvic metastasis may be the first clinical presentation of primary tumors [2]. Common sites for pelvic metastases are the ovary, uterine serosa, anterior and posterior cul-de-sac, and the pelvic peritoneum [2]. Transperitoneal dissemination is considered to be the most likely mechanism for pelvic metastases. Metastases through the lymphovascular system are also possible, although this is less common [3].
Metastasis to the fallopian tube has been reported to be uncommon, except for the direct extension of ovarian malignancy [4]. It seems plausible that the proximity of the fallopian tube and the ovary may reduce the detection of true metastases to the fallopian tube. Some previous studies have suggested possible reasons for the relatively low incidence of tubal metastases in these cases [5, 6]. Most patients with adnexal metastases present with symptoms related to primary tumors or large ovarian metastatic tumors, whereas tubal metastases are usually asymptomatic and only detected during microscopic examination. Since representative samples of the fallopian tube have traditionally been submitted for microscopic examination, grossly unidentifiable tubal metastases are generally inadequately sampled [5, 6]. Gross tumors that can be seen macroscopically are, therefore, easily sampled and diagnosed, while small microscopic tumors may be overlooked.
In routine practice, we recently noted several cases of tubal metastases originating from primary endometrial, cervical, and nongynecological tumors. The metastatic tumors appeared to exhibit variable degrees of mural extension and show distinctive histopathological features according to the extent of mural involvement. In this study, we performed a retrospective study in which all fallopian tube tissues obtained from patients with tubal metastases were examined histopathologically, noting the extent of mural involvement and associated histopathological features. We also analyzed the clinical characteristics of primary endometrial, cervical, and nongynecological tumors metastasizing to the fallopian tube that were diagnosed at a single institution.
In addition, we recently changed our macroscopic examination and sampling techniques for all fallopian tube specimens obtained via salpingectomy. Although this change was initiated based on a hypothesis linking the detection of serous tubal intraepithelial carcinoma (STIC) within the fimbrial ends to ovarian carcinogenesis, we observed several microscopic metastases in both the fimbrial and the nonfimbriated portions. To evaluate this observation, we retrospectively analyzed whether the sampling method (i.e., whole or representative submission) used in routine microscopic examination of the fallopian tube affected the detection of tubal metastases.
Materials and methods
Patient selection
The pathology database at Severance Hospital was queried for all cases that were diagnosed as malignant tumors involving the fallopian tubes between 2013 and 2016. The midpoint of this 4-year period coincided with a departmental policy change in how the fallopian tubes were processed in routine practice. Before this change, whether the fallopian tubes were submitted in their entirety or as a representative sample relied on the discretion of the individual prosector. The policy change mandated the submission of whole fallopian tubes in all cases. In other words, the study period consisted of 2 years of traditional representative fallopian tube submissions for microscopic examination followed by 2 years of whole fallopian tube submissions.
Histopathological diagnoses were made based on the 2014 WHO classification [7,8,9]. The inclusion criteria for confirming the metastasis from primary endometrial or cervical tumors to the fallopian tube were (1) extensive uterine tumors with evidence of endometrial or cervical precancerous lesions, such as an endometrioid intraepithelial neoplasia, serous endometrial intraepithelial carcinoma, high-grade squamous intraepithelial lesion, or endocervical adenocarcinoma in situ, and a small number of tumor cells in the ovary; and (2) the same histopathology in primary and metastatic tumors. The exclusion criteria were (1) primary ovarian, peritoneal, or tubal neoplasms; and (2) concurrent extensive tumors in the ovary and uterus.
Histopathological examination
Before 2015 in our department, grossly unremarkable fallopian tubes were sectioned transversely and two ring-shaped sections were typically taken from each tube, using two or less cassette per tube (range, one to two; mean, 1.23). As this method implies, the fimbrial ends were not sampled consistently. After 2015, we submitted whole tubal tissue sample split among at least two cassettes (range, two to four; mean, 2.51).
The resected specimens were fixed in 10% neutral-buffered formalin and embedded in paraffin. From each formalin-fixed, paraffin-embedded block, 4-μm sections were cut and stained with hematoxylin and eosin (H&E). A variable number of H&E-stained slides from each case were available for review. Among these, the most representative slide containing an appropriate volume of tumor tissue was chosen for immunohistochemical staining.
Pathology review
We thoroughly reviewed the pathology reports and all available gross photographs. We also examined all available H&E-stained slides obtained from each case using light microscopy. During the microscopic examination, we analyzed the anatomical distribution of the metastatic tumors and associated histopathological features. In cases showing intraepithelial metastases, immunohistochemical staining was performed to exclude the possibility of STIC.
Immunohistochemistry
The 4-μm sections were deparaffinized and rehydrated using xylene and alcohol. Immunohistochemical staining was performed using the Ventana Benchmark XT Automated Staining System according to the manufacturer’s instructions [10,11,12,13,14,15,16,17,18]. Antigen retrieval was performed using Cell Conditioning Solution. The sections were incubated with primary antibodies against p16 (prediluted, E6H4, Ventana Medical Systems), p53 (1:300; DO-7, Novocastra), WT1 (1:200; 6F-H2, Cell Marque), cytokeratin (CK) 7 (1:100; OV-TL 12/30, Dako), CK20 (1:100; Ks20.8, Dako), and CDX2 (1:400; EPR2764Y, Cell Marque). After chromogenic visualization, the slides were counterstained with hematoxylin. Appropriate positive and negative controls were stained concurrently to validate the staining method. For p16, p53, and CK7, endometrial serous carcinoma was used as positive control. For WT1, normal tubal epithelium was used as positive control. For CK20 and CDX2, colonic adenocarcinoma was used as positive control. For negative controls, nonspecific activity was assessed by omitting the primary antibodies. The intensity and proportion of staining, as well as the subcellular location, were evaluated. Moderate-to-strong staining in the nuclei (p16, p53, WT1, and CDX2) or membrane (CK7 and CK20) 50% or more tumor cells were designated as positive.
Results
Malignant tumors involving the fallopian tube
Table 1 summarizes the locations of the primary tumors and histopathological diagnoses of 60 patients with tubal metastasis. In these patients, 14 (23.3%) had uterine tumors and 46 (76.6%) had nongynecological tumors. Ten of the 14 (71.4%) uterine tumors were of endometrial origin, and the remaining 4 (28.5%) were of cervical origin. The locations of the nongynecological tumors were the colon (21/46; 45.6%), stomach (15/46; 32.6%), biliary tract (5/46; 10.8%), appendix (3/46; 6.5%), and the breast (2/46; 4.3%).
Clinical features of primary endometrial, cervical, and nongynecological malignancies metastasizing to the fallopian tube
Table 2 summarizes the clinical features of the patients with primary endometrial or cervical tumors metastasizing to the fallopian tube. All (14/14; 100.0%) patients underwent a total or radical hysterectomy with bilateral salpingo-oophorectomy, bilateral pelvic and/or para-aortic lymphadenectomy, and a peritoneal biopsy for suspicious lesions. Nine (90.0%) of the 10 endometrial tumors invaded the uterine serosa and/or parametrium. Concurrent ovarian, peritoneal, and tubal metastases were consistently found in all (9/9; 100.0%) patients. One (10.0%) case, of endometrial carcinosarcoma, displayed invasion into more than half of the myometrium and tubo-ovarian metastases, but no peritoneal or nodal metastases were present. This patient showed malignant cells in the intraoperative peritoneal washing cytology. All (4/4; 100.0%) cases of cervical carcinoma showed parametrial extension. One case of squamous cell carcinoma exhibited concurrent tubo-ovarian, peritoneal, and nodal metastases. The fallopian tube was the only metastatic site in one of the three patients with cervical adenocarcinoma. Overall, tubal metastases accompanied ovarian, peritoneal, and nodal metastases in 11 (78.5%), 10 (71.4%), and 7 (50.0%) of the 14 patients with uterine tumors, respectively.
Table 3 summarizes the clinical features of patients with nongynecological tumors metastasizing to the fallopian tube. Of the 46 patients with nongynecological tumors, 43 (93.4%) underwent bilateral salpingo-oophorectomy, and the remaining 3 (6.6%) underwent unilateral salpingo-oophorectomy. Thirty-one (67.3%) patients received surgery for primary tumors, and all (46/46; 100.0%) patients had peritoneal biopsies for suspicious lesions. All of the primary tumors infiltrated at least to the subserosa; 29.0% (9/31) exhibited subserosal invasion and 70.9% (22/31) serosal penetration. Ten of the 15 (66.7%) patients with gastric signet ring cells had peritoneal metastases. Of the 21 patients with colonic carcinoma, 19 (90.4%) had peritoneal metastases. All (5/5; 100.0%) patients with biliary adenocarcinoma had tubo-ovarian metastases, and 4 (80.0%) of those patients also had peritoneal metastases. All (3/3; 100.0%) patients with appendiceal carcinoma had both tubo-ovarian and diffuse peritoneal metastases (pseudomyxoma peritonei). All (2/2; 100.0%) patients with breast carcinoma had tubo-ovarian metastases, but none had peritoneal metastases. In summary, tubal metastases originating from nongynecological tumors were accompanied by ovarian and peritoneal metastases in 45 (97.8%) and 36 (80.0%) of the 46 patients, respectively.
Difference in the number of tubal metastases detected via representative versus whole tubal sampling
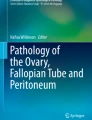
During the 4-year study period, we found 92 patients with ovarian metastases. Forty-seven (51.1%) of these patients were identified during the first 2 years when representative tubal sampling was used, and the remaining 45 (48.9%) patients were diagnosed via whole tubal sample during the latter 2-year period. After confirming that overall numbers of ovarian metastases detected during these two periods were similar, we compared the number of patients in each group with tubal metastases (Fig. 1). Of the 60 cases of tubal metastases, 23 (38.3%) and 37 (61.6%) were found during the earlier and later periods, respectively. We further classified the cases into grossly identifiable and unidentifiable lesions. Grossly identifiable lesions included masses encasing the fallopian tube completely, nodules involving the fimbriae and/or the serosal surfaces, fimbrial swelling, and serosal mucin deposition associated with pseudomyxoma peritonei. Of the 19 cases with grossly identifiable lesions, all (19/19; 100.0%) cases had ovarian lesions. The bilateral ovarian and tubal metastases were found in 19 (100.0%) and 12 (63.2%) cases, respectively. Of the 41 cases with grossly unidentifiable tubal metastasis, the ovarian lesions were identified in 31 (75.6%) cases. The bilateral ovarian and tubal were detected in 20 (48.7%) and 13 (31.7%), respectively. During the earlier period, grossly unidentifiable tubal metastases were observed in 14 cases. In contrast, during the later period, 27 grossly unidentifiable lesions were detected. In addition, there were four cases of microscopic tubal-only metastases found in cases after whole tubal sampling. Three (75.0%) of the four cases were intraepithelial metastases originating from the uterine cervix, which were endocervical adenocarcinoma, usual type; mucinous carcinoma, intestinal type; and mucinous carcinoma, gastric type. The remaining one case was endolymphatic tumor emboli from colonic adenocarcinoma. No microscopic tubal-only lesions were detected in cases examining representative samples.

Difference in the number of ovarian and/or metastases detected during periods of whole and representative tubal sampling. The numbers of ovarian metastases and grossly identifiable tubal metastases were similar. In contrast, whole tubal sampling enabled grossly unidentifiable tubal metastases to be detected. Five cases of microscopic tubal-only metastases were identified with whole tubal sampling, whereas none were found during the period of representative sampling
Anatomical distribution of tubal metastases
Eight (57.1%) of the 14 primary uterine tumors involved the fimbria, whereas 30 (65.2%) of the 46 nongynecological tumors involved the nonfimbriated portion. We classified the extent of mural involvement as serosa, subserosa, muscle, lamina propria, epithelium, and lymphovascular space (Table 4). Tumors involving more than one location were observed in 26 (43.3%) of the 60 cases: muscle and lamina propria in 17, subserosa and muscle in 6, and lamina propria and lymphovascular space in 3 case. The majority of metastatic tumors involving the serosa (13/14; 92.9%) originated from nongynecological tumors. In contrast, the majority of the intraepithelial lesions (4/5; 80.0%) originated from uterine tumors.
Histopathological features associated with tubal metastases
Table 5 summarizes histopathological features observed within and around the tubal metastatic lesions. Representative photomicrographs are shown in Fig. 2. Fibromyxoid stromal reaction or fibrosis were observed in 23 (38.3%) cases, 22 (95.6%) of which involved the muscle. Lymphohistiocytic infiltrate was found in 29 (48.3%) cases. All tumors showing peritumoral inflammatory infiltration consistently involved the muscle or subepithelial connective tissue. Architectural alteration of tubal plicae was observed in 26 (43.3%) cases. Most of the cases showed coexisting plicae thickening and flattening (loss of the complicated maze-like pattern of folds). Twenty-one (80.7%) cases showed architectural changes in the plicae involving the subepithelial connective tissue. The tubal folds of both the fimbrial and nonfimbriated portions were expanded by subepithelial tumor cell clusters, while the adjacent, uninvolved plicae were flattened. Plicae thickening and flattening were also associated with subepithelial hyalinization, lymphovascular space invasion in the subepithelial connective tissue, and intraepithelial metastases.

Histopathological features associated with tubal metastases. a, b Fibromyxoid stromal reaction. c Peritumoral fibrosis. d Lymphohistiocytic infiltration. e Plicae thickening associated with metastatic colonic adenocarcinoma. f Intraluminal inflammatory exudate admixed with floating tumor cell clusters
There were five cases of intraepithelial tubal metastases originating from the uterine cervix (3/5; 60.0%), uterine corpus (1/5; 20.0%), and colon (1/5; 20.0%). Representative photomicrographs are shown in Fig. 3. All cases were found in whole tube specimens. The carcinomatous component of the uterine carcinosarcoma involved the fimbrial epithelium. No sarcomatous components were identified. The metastatic tumors from the uterine cervix and colon showed multifocal involvement of the fimbrial and nonfimbrial epithelium. Morphologically, metastatic endocervical adenocarcinoma showed a mucin-poor columnar epithelium that exhibits pseudostratified architecture with enlarged, elongated, and hyperchromatic nuclei. In contrast, metastatic intestinal-type cervical mucinous carcinoma showed focal presence of goblet cells between atypical cells. Metastatic cervical gastric-type mucinous carcinoma showed abundant, pale, or eosinophilic cytoplasm; and enlarged, irregular, and hyperchromatic nuclei. Metastasis from colonic adenocarcinoma showed enlarged, hyperchromatic nuclei, varying degrees of nuclear spindling, stratification, and loss of polarity.

Immunophenotyping of intraepithelial tubal metastases. (a) Metastatic colonic adenocarcinoma showing (b) strong membranous CK20 immunoreactivity, (c) strong nuclear CDX2 immunoreactivity, and (d) absent WT1 expression. (e) Metastatic cervical intestinal-type mucinous carcinoma showing (f) p16 block positivity and (g) WT1 negativity. (h) Metastatic usual-type endocervical adenocarcinoma showing (i) p16 block positivity and (j) WT1 negativity. (k) Metastatic cervical gastric-type mucinous carcinoma showing (l) uniform, strong p53 expression; and (m) absent WT1 expression. (n) Metastatic serous carcinoma originating from a uterine carcinosarcoma and showing (o) complete loss of p53 expression; (p) uniform, strong p16 expression; and (q) absent WT1 expression
Immunohistochemical staining revealed that metastatic colorectal adenocarcinoma was positive for CK20 and CDX2, but negative for WT1, which highlighted the adjacent uninvolved tubal epithelium. Metastatic usual-type endocervical adenocarcinoma and intestinal-type mucinous carcinoma originating from the uterine cervix showed block positivity for p16, but were negative for WT1. Metastatic serous carcinoma derived from the endometrial carcinosarcoma displayed a complete loss of p53 expression, diffuse, strong p16 expression, and negative WT1 expression, thus diagnostic of uterine serous carcinoma.
Discussion
Determining tumor origin in patients with concurrent ovarian and uterine tumors is often difficult. Many pathologists use the morphological criteria suggested by Scully et al. [19]. According to these criteria, evidence supporting a primary uterine tumor includes (1) histopathological similarity between uterine and ovarian tumors, (2) large uterine and small ovarian tumors, (3) presence of endometrial precancerous lesions, (4) involvement of the deep myometrium, and (5) involvement of bilateral ovaries [19]. Immunohistochemical staining for WT1 has been applied to distinguish tubo-ovarian high-grade serous carcinoma from uterine serous carcinoma [20]. Negativity or focal, weak positivity for WT1 suggests a uterine origin. The presence of serous endometrial intraepithelial carcinoma within a background of endometrial atrophy or polyps also supports the diagnosis of a primary uterine tumor. Identifying the origin of tumors involving both the uterine cervix and the ovary is less debatable. Relatively simple morphological criteria using tumor size and laterality, immunohistochemical staining for p16, and the detection of human papillomavirus, can be used to distinguish metastatic lesions of the uterine cervix from primary ovarian neoplasms [21].
We observed more microscopic metastatic lesions in the fallopian tubes with the whole tube sampling technique than with traditional representative sampling. It has been suggested that metastasis to the fallopian tube may be an exceedingly rare event, but our results raise the possibility that the historically observed rarity of this event may be an artifact of the tissue sampling strategy employed. In this study, 14 (34.1%) of the 41 grossly unidentifiable lesions were detected during a 2-year period of representative sampling, but the remaining 27 (65.8%) cases were diagnosed during the 2 years since the whole tube sampling strategy was initiated in our department. Moreover, four cases with microscopic tubal-only metastases were identified in whole tube specimens, whereas no microscopic lesions were detected in cases using the traditional sampling method. Complete microscopic examination of the fallopian tubes in the setting of widespread metastases is not clinically necessary. Still, the point remains that the completeness of specimen sampling directly affects the results of studies defining the prevalence of disease in an organ of interest.
In several large case series, the proportion of gynecological tumors metastasizing to the ovary ranged from 20 to 50% of the ovarian metastatic tumors. In this study, primary uterine tumors comprised 23.3% (14/60) of the tubal metastases. Given the observation that concurrent ovarian and tubal metastases were identified in most of the cases, it is reasonable to assume that tubal metastases may be identified in a similar proportion of cases as ovarian metastases. It has been reported that nongynecological tumors metastasizing to the ovary most commonly originate from the colon, breast, and appendix [22,23,24]. In two previous studies regarding nongynecological tumors metastasizing to the fallopian tube, the most common sites of origin were also the colon, breast, and appendix [5, 6]. In this study, the most common primary nongynecological tumors were from the colon and stomach. In contrast with the data from Western populations, however, breast and appendiceal tumors occupied a relatively low proportion. A higher prevalence of gastric cancer in the Asian population could explain this difference.
We noticed that most of the nongynecological tumors with tubal metastases displayed deeply invasive primary tumors and multiple metastases to the ovary and peritoneum. An analysis of the anatomical distribution of the metastatic lesions demonstrated fimbrial or serosal involvement in 71.7% (32/46) of the nongynecological tumors. This finding suggests that transperitoneal metastasis is the main route for tubal metastases of nongynecological tumors. Considering that lymphovascular space invasion was present in 23.9% (11/46) of the cases, lymphovascular dissemination may be also an important route for tubal metastases. Our observations of intraepithelial metastases support the possibility of transtubal spread of nongynecological tumors. In addition, we observed malignant cells in the cervicovaginal smear of a patient with colonic adenocarcinoma without uterine metastases. Consistent with this finding, some previous studies have shown the detection of malignant cells of nongynecological origin in cervicovaginal cytology specimens [25, 26].
In nine (90.0%) patients with endometrial tumors exhibiting parametrial invasion and peritoneal metastasis, transperitoneal metastasis seemed to be a reasonable explanation for the route of tubal metastasis. Interestingly, in the remaining one (10.0%) patient whose endometrial tumors lack evidence of parametrial invasion or peritoneal metastasis, malignant cells were detected in the intraperitoneal lavage cytology. Peritoneal metastasis in early-stage endometrial carcinomas is an unusual phenomenon [27]. Some previous studies have shown the presence of floating tumor cells within the tubal lumen to be associated with peritoneal metastasis in patients with superficially invasive endometrial carcinoma [28, 29]. This suggests transtubal spread of malignant cells as a route of peritoneal metastasis in early-stage endometrial carcinoma.
Adnexal metastasis of cervical carcinoma is very uncommon. In fact, previous literature has focused mainly on ovarian metastasis [30,31,32,33]. Reyes et al. [34] recently described a series of 20 cervical carcinomas involving the adnexa. We observed that five patients with cervical carcinoma had adnexal metastases (ovarian metastasis only in one, concurrent ovarian and tubal metastases in one, and tubal metastasis in three patients). In both our and the Reyes et al. series, tubal metastases were more frequent than ovarian metastases, and involvement of the adnexa was mainly unilateral. In addition, 75.0% (3/4) of our cases and 50.0% (7/14) of the Reyes et al. cases [34] had intraepithelial metastases, respectively. There have been some reports of tubal metastasis in early-stage cervical carcinoma, and the authors suggested superficial spread of cervical carcinoma to explain such findings [34,35,36,37]. Frequent cervical carcinoma involving the tubal epithelium supports the idea of luminal spreading of tumor cells as one of the routes for tubal metastasis.
The most important differential diagnosis of tubal intraepithelial metastasis is STIC [5, 6]. STIC is histopathologically characterized by cellular crowding, stratification, loss of polarity, and enlarged nuclei with hyperchromasia, all of which can be seen in cases of tubal intraepithelial metastasis. When the mucinous differentiation is present, the diagnosis favors intraepithelial metastasis [6]. However, its absence causes diagnostic difficulty on the morphological bases. In these cases, careful consideration of clinical history and the use of immunohistochemistry would be helpful.
We observed distinctive morphological features according to the extent of mural involvement: (1) fibromyxoid stromal reaction, fibrosis, and lymphohistiocytic infiltrate in tumors involving the muscle and subepithelial connective tissue; (2) architectural alterations of plicae in tumors involving the subepithelial connective tissue or tubal epithelium; and (3) intraluminal mucinous and/or inflammatory exudate associated with intraepithelial tumors. Based on our observations, we suggest that identification of the associated histopathological features could be useful clues for identifying metastatic tumors of the fallopian tube. In routine practice, it is not difficult for pathologists to find a grossly identifiable metastatic lesion in the fallopian tube under low-power magnification. Instead, when they encounter a lesion that is too small to detect at low-power fields, an awareness of the abovementioned histopathological features may lead to more careful examination when a strong suspicion of metastasis is present.
In summary, we described clinicopathological characteristics of tubal metastases originating from primary endometrial, cervical, and nongynecological tumors diagnosed at a single institution. We observed distinctive histopathological features associated with tubal metastases according to the extent of mural involvement. In addition, we consider the sampling of entire fallopian tubes to give much more information about the extent of metastatic lesions. We also believe that it is more logical to thoroughly sample both fimbrial ends and nonfimbriated portions of the fallopian tube for all salpingectomy specimens in the setting of cancer surgery.
References
Vroomen L, Scheffer HJ, Melenhorst M, van Grieken N, van den Tol MP, Meijerink MR (2017) Irreversible electroporation to treat malignant tumor recurrences within the pelvic cavity: a case series. Cardiovasc Intervent Radiol. doi:10.1007/s00270-017-1657-6
Mazur MT, Hsueh S, Gersell DJ (1984) Metastases to the female genital tract. Analysis of 325 cases. Cancer 53:1978–1984
Charnley RM, Banerjee AK, Whitaker SC, Spiller RC, Doran J (1995) Peritoneal seeding of pancreatic cancer following transperitoneal biliary procedures. Br J Surg 82:393
Finn WF, Javert CT (1949) Primary and metastatic cancer of the fallopian tube. Cancer 2:803–814
Stewart CJ, Leung YC, Whitehouse A (2012) Fallopian tube metastases of non-gynaecological origin: a series of 20 cases emphasizing patterns of involvement including intra-epithelial spread. Histopathology 60:E106–E114. doi:10.1111/j.1365-2559.2012.04194.x
Rabban JT, Vohra P, Zaloudek CJ (2015) Nongynecologic metastases to fallopian tube mucosa: a potential mimic of tubal high-grade serous carcinoma and benign tubal mucinous metaplasia or nonmucinous hyperplasia. Am J Surg Pathol 39:35–51. doi:10.1097/PAS.0000000000000293
Kurman RJ, Carcangiu ML, Herrington CS, Young RH (2014) World Health Organization classification of tumours of female reproductive organs. International Agency for Research on Cancer. Lyon, France
Bosman FT, Carneiro F, Hruban RH, THeise ND (2010) World Health Organization classification of tumours of the digestive system. International Agency for Research on Cancer, Lyon
Lakhani SR, Ellis IO, Schnitt SJ, Tan PH, van de Vijver MJ (2012) World Health Organization Classification of Tumours International Agency for Research on Cancer, Lyon
Yoon N, Yoon G, Park CK, Kim HS (2016) Stromal p16 expression is significantly increased in malignant ovarian neoplasms. Oncotarget 7:64665–64673. doi:10.18632/oncotarget.11660
Yoon G, Oh CS, Kim HS (2016) Hypergravity upregulates renal inducible nitric oxide synthase expression and nitric oxide production. Oncotarget 7:30147–30154. doi:10.18632/oncotarget.9253
Yoon G, Oh CS, Kim HS (2016) Distinctive expression patterns of hypoxia-inducible factor-1alpha and endothelial nitric oxide synthase following hypergravity exposure. Oncotarget 7:33675–33688. doi:10.18632/oncotarget.9372
Kim HS, Yoon G, Do SI, Kim SJ, Kim YW (2016) Down-regulation of osteoprotegerin expression as a novel biomarker for colorectal carcinoma. Oncotarget 7:15187–15199. doi:10.18632/oncotarget.7885
Yoon G, Won Koh C, Yoon N, Kim JY, Kim HS (2016) Stromal p16 expression is significantly increased in endometrial carcinoma. Oncotarget. doi:10.18632/oncotarget.13594
Park CK, Yoon G, Cho YA, Kim HS (2016) Clinicopathological and immunohistochemical characterization of papillary proliferation of the endometrium: a single institutional experience. Oncotarget 7:39197–39206. doi:10.18632/oncotarget.10049
Jung YY, Nahm JH, Kim HS (2016) Cytomorphological characteristics of glassy cell carcinoma of the uterine cervix: histopathological correlation and human papillomavirus genotyping. Oncotarget 7:74152–74161. doi:10.18632/oncotarget.12361
Kim EK, Yoon G, Kim HS (2016) Chemotherapy-induced endometrial pathology: mimicry of malignancy and viral endometritis. Am J Transl Res 8:2459–2467
Bae GE, Yoon G, Song YJ, Kim HS (2016) High-grade squamous intraepithelial lesion arising adjacent to vulvar lymphangioma circumscriptum: a tertiary institutional experience. Oncotarget 7:48120–48129. doi:10.18632/oncotarget.10158
Soliman PT, Slomovitz BM, Broaddus RR, Sun CC, Oh JC, Eifel PJ, Gershenson DM, Lu KH (2004) Synchronous primary cancers of the endometrium and ovary: a single institution review of 84 cases. Gynecol Oncol 94:456–462. doi:10.1016/j.ygyno.2004.05.006
Zhang Y, Garcia-Buitrago MT, Koru-Sengul T, Schuman S, Ganjei-Azar P (2013) An immunohistochemical panel to distinguish ovarian from uterine serous papillary carcinomas. Int J Gynecol Pathol 32:476–481. doi:10.1097/PGP.0b013e31826ddc4e
Elishaev E, Gilks CB, Miller D, Srodon M, Kurman RJ, Ronnett BM (2005) Synchronous and metachronous endocervical and ovarian neoplasms: evidence supporting interpretation of the ovarian neoplasms as metastatic endocervical adenocarcinomas simulating primary ovarian surface epithelial neoplasms. Am J Surg Pathol 29:281–294
de Waal YR, Thomas CM, Oei AL, Sweep FC, Massuger LF (2009) Secondary ovarian malignancies: frequency, origin, and characteristics. Int J Gynecol Cancer 19:1160–1165. doi:10.1111/IGC.0b013e3181b33cce
Moore RG, Chung M, Granai CO, Gajewski W, Steinhoff MM (2004) Incidence of metastasis to the ovaries from nongenital tract primary tumors. Gynecol Oncol 93:87–91. doi:10.1016/j.ygyno.2003.12.039
Ulker V, Numanoglu C, Alpay V, Akbayir O, Polat I, Gedikbasi A, Akca A (2013) Characteristics and prognosis of ovarian metastatic tumors: review of a single-institution experience. Eur J Gynaecol Oncol 34:75–78
Selvaggi LE, Di Vagno G, Loverro G, Masotina A, Cramarossa D, Napoli A, Resta L (1993) Abnormal cervical PAP smear leading to the diagnosis of gastrointestinal cancer without cervico-vaginal metastases. Eur J Gynaecol Oncol 14:398–401
Pambuccian SE, Bachowski GJ, Twiggs LB (2000) Signet ring cell lobular carcinoma of the breast presenting in a cervicovaginal smear. A case report. Acta Cytol 44:824–830
Gemer O, Bergman M, Segal S (2004) Ovarian metastasis in women with clinical stage I endometrial carcinoma. Acta Obstet Gynecol Scand 83:208–210
Stewart CJ, Doherty DA, Havlat M, Koay MH, Leung YC, Naran A, O'Brien D, Ruba S, Salfinger S, Tan J (2013) Transtubal spread of endometrial carcinoma: correlation of intra-luminal tumour cells with tumour grade, peritoneal fluid cytology, and extra-uterine metastasis. Pathology 45:382–387. doi:10.1097/PAT.0b013e328360b6e7
Snyder MJ, Bentley R, Robboy SJ (2006) Transtubal spread of serous adenocarcinoma of the endometrium: an underrecognized mechanism of metastasis. Int J Gynecol Pathol 25:155–160. doi:10.1097/01.pgp.0000179614.47838.82
Ronnett BM, Yemelyanova AV, Vang R, Gilks CB, Miller D, Gravitt PE, Kurman RJ (2008) Endocervical adenocarcinomas with ovarian metastases: analysis of 29 cases with emphasis on minimally invasive cervical tumors and the ability of the metastases to simulate primary ovarian neoplasms. Am J Surg Pathol 32:1835–1853. doi:10.1097/PAS.0b013e3181758831
Sutton GP, Bundy BN, Delgado G, Sevin BU, Creasman WT, Major FJ, Zaino R (1992) Ovarian metastases in stage IB carcinoma of the cervix: a Gynecologic Oncology Group study. Am J Obstet Gynecol 166:50–53
Ngamcherttakul V, Ruengkhachorn I (2012) Ovarian metastasis and other ovarian neoplasms in women with cervical cancer stage IA-IIA. Asian Pac J Cancer Prev 13:4525–4529
Shimada M, Kigawa J, Nishimura R, Yamaguchi S, Kuzuya K, Nakanishi T, Suzuki M, Kita T, Iwasaka T, Terakawa N (2006) Ovarian metastasis in carcinoma of the uterine cervix. Gynecol Oncol 101:234–237. doi:10.1016/j.ygyno.2005.10.004
Reyes C, Murali R, Park KJ (2015) Secondary involvement of the adnexa and uterine corpus by carcinomas of the uterine cervix: a detailed morphologic description. Int J Gynecol Pathol 34:551–563. doi:10.1097/PGP.0000000000000206
Deel CD, Allen RA, Holman LL, Zuna RE (2016) Adenocarcinoma of the cervix involving the fallopian tube mucosa: report of a case. Diagn Pathol 11:77. doi:10.1186/s13000-016-0529-8
Gungor T, Altinkaya SO, Ozat M, Akbay S, Mollamahmutoglu L (2011) Unusual form of superficial spreading squamous cell carcinoma of cervix involving the endometrium, bilateral tubes and ovaries: a case report with literature review. Arch Gynecol Obstet 283:323–327. doi:10.1007/s00404-010-1672-1
Pins MR, Young RH, Crum CP, Leach IH, Scully RE (1997) Cervical squamous cell carcinoma in situ with intraepithelial extension to the upper genital tract and invasion of tubes and ovaries: report of a case with human papilloma virus analysis. Int J Gynecol Pathol 16:272–278
Acknowledgments
This research was supported by the Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education (2016R1D1A1B03935584) and by a faculty research grant of Yonsei University College of Medicine for 2016 (6-2017-0036).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
This study was reviewed and approved by the Institutional Review Board at the Severance Hospital, Yonsei University Health System, Seoul, Republic of Korea (2016-2886-001).
Conflict of interest
The authors declare that they have no conflict of interest.
Rights and permissions
About this article

Cite this article
Na, K., Kim, HS. Clinicopathological characteristics of fallopian tube metastases from primary endometrial, cervical, and nongynecological malignancies: a single institutional experience. Virchows Arch 471, 363–373 (2017). https://doi.org/10.1007/s00428-017-2186-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00428-017-2186-z