
Abstract
CIC-DUX4 and BCOR-CCNB3 fusion-gene-associated small round cell sarcomas account for a proportion of pediatric small round cell sarcomas, but their pathological features have not been sufficiently clarified. We reviewed a large number of soft tissue tumors registered at our institution, retrieved the cases of unclassified tumors with a small round cell component, and subjected them to histopathological, immunohistochemical, and gene profile analysis. We reviewed 164 cases of unclassified tumors with a small round cell component and analyzed them by RT-PCR and FISH. Tumors positive for a specific fusion-gene were also subjected to histopathological and immunohistochemical examinations. We identified 16 cases of BCOR-CCNB3/CIC-associated (CIC-DUX4 or CIC gene rearrangement-positive) sarcomas. These included seven BCOR-CCNB3 sarcomas and nine CIC-associated sarcomas. Heterogeneous elements included a myxoid spindle cell component in three BCOR-CCNB3 sarcomas and an epithelioid cell component in two CIC-associated sarcomas (one CIC-DUX4-positive and one CIC-DUX4-negative sarcomas). Mitotic activity was low in both heterogeneous components. By immunohistochemistry, in seven BCOR-CCNB3 sarcomas expression of EMA was positive in two cases, of p63 in three, of CD56 in six, of TLE1 in seven, of NKX2.2 in two, of CCNB3 in seven, and of BCOR in six cases (one case could not be tested for BCOR). In nine cases of CIC-associated sarcoma, CD56 was expressed in five, alpha-smooth muscle actin in one, ERG in three, and CD99, WT1 and TLE1 each in eight cases. Both sarcoma types showed not only a small round cell component, but also a myxoid/epithelioid component with low mitotic activity.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Small round cell sarcoma (SRCS), which includes rhabdomyosarcoma and Ewing sarcoma (EWS), is one of the most important tumor groups in pediatric oncology. SRCS is characterized by small-sized round-shaped tumor cells with scant cytoplasm, known as “blue cells.” The latest WHO classification categorizes undifferentiated/unclassified SRCS (USRCS) into undifferentiated/unclassified sarcoma with round cell morphology [1]. For a diagnosis of USRCS, a wide variety of neoplastic lesions, such as carcinoma, malignant melanoma, hematopoietic malignancy, and epithelioid-type soft tissue tumors, need to be ruled out.
Recently, recognition of CIC-DUX4, CIC-FOXO4, and BCOR-CCNB3 fusion-gene-associated SRCSs has improved because of their aggressive biological behavior and novel gene aberrations [2–20]. However, it can be difficult to differentiate these sarcomas from other small round cell tumors, especially EWS family tumors, by means of morphology and immunohistochemistry. In addition, due to the rarity of these tumors’ documentation of characteristics useful for diagnosis still needs to be improved.
We reviewed a large number of cases of soft tissue tumor registered at our institution, identified the specific-fusion gene-positive SRCSs among them, and examined histopathological, immunohistochemical, and gene-aberration profiles of the specific-fusion gene-positive SRCSs.
Materials and methods
Materials
Histopathology reports on 20,000 cases of soft tissue tumor, registered from 1975 to 2016 in the files of the Department of Anatomic Pathology, Graduate School of Medical Sciences, Kyushu University, Fukuoka, Japan, were reviewed. The authors initiated this investigation by reviewing histologically all unclassified tumors with a small round cell component registered in our institution. Ewing sarcoma, rhabdomyosarcoma, and synovial sarcomas were excluded. In this way, we retrieved 164 cases of an unclassified tumor with a small round cell component, including USRCS and round cell tumor, not otherwise specified. Available tumors were prepared for further examination as described below.
We used three different techniques to identify CIC-DUX4 and BCOR-CCNB3 fusion-gene-associated small round cell sarcomas. As a first step, CCNB3 immunohistochemical staining (IHC) was performed, followed by fluorescent in situ hybridization (FISH) with a split CIC gene probe and finally by reverse transcription-polymerase chain reaction (RT-PCR) (Supplementary Fig. 1). The CCNB3-positive tumors were directly analyzed by RT-PCR and direct sequencing instead of CIC gene FISH.
Methods
Clinicopathological and histopathological review
We reviewed clinicopathological and histopathological data of BCOR-CCNB3/CIC-DUX4 fusion-gene-positive or CIC gene-rearrangement-positive cases retrieved by the above processes, with a focus on age, sex, site, tumor cell shape, nucleoli, mitotic figures, growth pattern and capsule, as well as heterogeneous components other than round tumor cells.
Immunohistochemistry
Immunohistochemical staining was performed on all sarcomas with BCOR-CCNB3, CIC-DUX4, or CIC gene rearrangement. Formalin-fixed, paraffin-embedded tissue was sectioned at 3 μm thickness. The primary antibodies, their dilution, and the applied antigen retrieval procedure are summarized in Supplementary Table 1. Immunoreactivity was detected with the EnVision Detection System (DAKO, Glostrup, Denmark).
Fluorescent in situ hybridization
To assess rearrangement of the CIC gene, split dual-color FISH was performed on all available cases using ready-made FISH probes (GSP Laboratories, Kawasaki, Japan) on 3 μm thick sections. Fifty nuclei were counted to estimate the proportion of tumor cells having a CIC gene rearrangement. A split signal was defined by a distance between the red and green signals of at least twice the estimated signal diameter. CIC gene-rearrangement-positive tumors are called “CIC-associated sarcomas” in this report.
Reverse transcription-polymerase chain reaction
Total RNA was extracted from frozen or paraffin samples using a TRIzol reagent (Invitrogen, Carlsbad, CA, USA) and was reverse-transcribed using Superscript III reverse transcriptase (Invitrogen) to prepare the first-strand complementary DNA. CIC-DUX4 and BCOR-CCNB3 fusion assays were performed using newly designed primers (Supplementary Table 2) that specifically amplify the fusion gene transcripts. Each PCR product (5 μL) was loaded onto 2% agarose gel with ethidium bromide and visualized under UV illumination. The PCR products were also evaluated by direct sequence analysis using the BigDye Terminator method (version 1.1; Applied Biosystems, Foster City, CA, USA) to confirm the breakpoints of the fusion transcripts. All non-specific PCR bands were confirmed by direct sequence analysis.
Results
Clinicopathological and histopathological review
The clinicopathological data of all tumors are listed in Table 1 and Supplementary Table 3. BCOR-CCNB3 sarcomas occurred in five females and two males with an age range of 12 to 32 years (mean 16.5 years); two were located in an extremity, four in the trunk, and one in the cauda equina. CIC-associated sarcomas occurred in five females and four males with an age range of 5 to 81 years (mean 37.1 years); four were located in an extremity, two in the trunk, one in the omentum, one in the iliac bone, and one in the tongue.
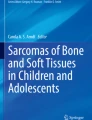
Histopathological findings and representative figures are summarized in Table 2 and Fig. 1. All seven BCOR-CCNB3 sarcomas had similar histological features: short, spindle-shaped to round cells, scant cytoplasm, and irregular but not bizarre nuclei (Fig. 1a, b). Similarly, all nine CIC-associated sarcomas had similar histological features such as oval to round cells, scant cytoplasm, irregular but not bizarre nuclei, and conspicuous nucleoli (Fig. 1c, d). Three evaluable sarcomas of each type showed a multinodular and focally infiltrative growth pattern. As heterogeneous elements, a myxoid spindle cell component was observed in three BCOR-CCNB3 sarcomas (Fig. 1e, f), and an epithelioid cell component was observed in two CIC-associated sarcomas (1 CIC-DUX4-positive sarcoma and 1 CIC-DUX4-negative sarcoma) (Fig. 1g, h). Myxoid areas showed proliferation of short spindle-shaped cells with bland or mildly atypical nuclei arranged in loose fascicular or haphazard pattern and embedded in a myxoid matrix. Epithelioid areas were composed of epithelioid tumor cells with mildly atypical nuclei arranged in a sheet-like pattern. Mitotic activity was low in the heterogeneous components: 5–76/10 HPF (mean 31.4) in the small round cell component vs 1–6/10 HPF (mean 3) in the myxoid spindle cell component in BCOR-CCNB3 sarcomas. In CIC-associated sarcomas this was 4–58/10 HPF (mean 23.7) in the small round cell component vs 3–6/10 HPF (mean 4.5) in the epithelioid cell component.

Histopathological features of the small round cell tumors. a,b Small round cell component of BCOR-CCNB3 sarcoma, c,d small round cell component of CIC-DUX4 sarcoma, e,f myxoid component of BCOR-CCNB3 sarcoma, and g,h epithelioid cell component of CIC-DUX4 sarcoma
One BCOR-CCNB3 sarcoma case initially presented as a tumor as a myxoid predominantly tumor and later recurred with an increased small cell component. Systemic metastases of the small round cell component and tumor death were confirmed in one case (case 2) by autopsy. One CIC-associated sarcoma (case 9) was resected under a clinical diagnosis of a benign cutaneous tumor, but subsequently diagnosed as undifferentiated small round cell sarcoma and additionally treated by chemotherapy. This tumor initially appeared to consist entirely of small round cell sarcoma, although the resected tumor after chemotherapy presented with a focal epithelioid cell component.
Immunohistochemistry
Representative images of immunohistochemical staining are presented in Fig. 2 and the results can be summarized as follows. All seven BCOR-CCNB3 sarcomas were positive for CCNB3 (diffuse and nuclear in both myxoid and round cell areas) (Fig. 2a, b) and for TLE1 (diffuse and nuclear) (Fig. 2c), while six cases were positive for CD56 (Fig. 2d), two for EMA (weakly positive), three for p63, two for NKX2.2 (nuclear staining), and six for BCOR (nuclear staining) (Fig. 2e). All were negative for AE1/AE3, S-100 protein, alpha-smooth muscle actin, desmin, myogenin, NY-ESO-1, ERG, WT1, and CD99. Of nine CIC-associated sarcomas eight were positive for CD99 (Fig. 2f), five for CD56, eight for WT1 (Fig. 2g), eight for TLE1 (weakly), one for alpha-smooth muscle actin (focally) and three for ERG. All were negative for CCNB3, AE1/AE3, EMA, p63, S-100 protein, desmin, myogenin, NY-ESO-1, NKX2.2 and BCOR. INI-1 was expressed all 11 tumors.

Immunohistochemical features of the small round cell tumors. a,b BCOR-CCNB3 sarcoma with CCNB3 IHC (a round cell area, b myxoid area), c BCOR-CCNB3 sarcoma with TLE1 IHC, d BCOR-CCNB3 sarcoma with CD56 IHC, e BCOR-CCNB3 sarcoma with BCOR IHC, f CIC-DUX4 sarcoma with CD99 IHC, g CIC-DUX4 sarcoma with WT1 IHC
Fluorescent in situ hybridization
Red and green fluorescent signals were obtained. Eight cases of CIC gene-rearrangement-positive tumors were identified (Fig. 3). CIC gene rearrangement was detected in both round cell and epithelioid areas.

CIC split FISH in case 9. Clear split signals of Texas red and fluorescein were observed
RT-PCR
BCOR-CCNB3 and CIC-DUX4 fusion genes were detected in seven and four tumors, respectively. This was in cases 1–5 BCOR exon 15-CCNB3 exon 5 (Fig. 4a), in cases 9, 10, and 12 CIC exon 20-DUX4 exon 1 and in case 11 CIC exon 20-DUX4 exon 2 (Fig. 4b). BCOR-CCNB3/CIC-DUX4 was not detected in cases 8 and 13, and CIC-FOXO4 was not detected in any case.

BCOR-CCNB2 and CIC-DUX4 fusion gene analysis in a case 2 and b case 8. RT-PCR and direct sequencing were performed. The arrows mean true PCR bands of fusion gene products confirmed by direct sequencing
Discussion
CIC-DUX4 sarcomas were first identified in 2009 by Kawamura and Saito using chromosomal analysis, and were initially regarded as Ewing-family tumors [2]. In 2014, Specht et al. analyzed a larger number of these tumors and showed that their histopathological features and immunohistochemical profile are distinct from those of Ewing sarcomas [3]. BCOR-CCNB3 sarcomas were first reported in 2012 by Pierron et al. and also considered as part of the Ewing family. Although these specific fusion gene-positive SRCTs were mostly classified as so-called atypical Ewing sarcoma or Ewing-like sarcomas in the past, recent research suggests that these two tumors are entities distinct from Ewing sarcoma. We reviewed the 164 unclassified tumors that had round tumor cells at least focally, and identified seven BCOR-CCNB3 and nine CIC gene-rearrangement-positive sarcomas. Although both tumors types tended to occur in young patients, our study shows that the tumors, especially those CIC gene-rearrangement-positive, occur not only in pediatric patients but also regularly in adult or senior patients (mean age 37.1 years). Moreover, unlike in a previous investigation, our BCOR-CCNB3 sarcomas series does not show male predominance. [19] In our series, the location of both BCOR-CCNB3 and CIC gene-rearrangement-positive sarcomas varied and showed no predilection for bone. We contend that unclassified small round cell tumors include a small proportion of the above sarcomas.
BCOR-CCNB3- and CIC-associated sarcomas are histological mimics of Ewing sarcomas, although heterogeneous elements unlike EWS have also been reported as minor component [4]. Both tumor types can have myxoid areas as well as a prominent spindle component. In our study, both tumors were composed not only of small round cells but also of short, spindle- or epithelioid-shaped cells, proliferating in multinodular and sheet-like patterns with incomplete fibrous capsules. Interestingly, some of the tumors contained heterogeneous components, i.e. myxoid spindle cells and epithelioid cells in addition to small round cells. These features make for diagnostic pitfalls in the differentiation between BCOR-CCNB3 sarcomas and malignant peripheral nerve sheath tumors, synovial sarcomas, and myxofibrosarcomas. They also make it difficult to differentiate between CIC-DUX4/CIC gene-rearrangement-positive sarcomas and carcinomas, malignant melanomas and epithelioid sarcomas. One of our BCOR-CCNB3 cases was predominantly composed of myxoid spindle cells with small foci of small round cells. Moreover, one CIC-associated sarcoma presented as a wholly epithelioid cell tumor.
These heterogeneous components showed a lower proliferative activity than the small round cell components. One patient with a BCOR-CCNB3 sarcoma (case 2) died due to systemic metastasis of the small round cell component, confirmed by autopsy. These observations underline the heterogeneous nature of both tumor types: a relatively low-grade component composed of myxoid spindle cell/epithelioid cells and a high-grade component composed of small round cells.
CCNB3 is a useful immunohistochemical marker for BCOR-CCNB3 sarcoma [4]. For CIC-associated sarcomas, there is currently no validated immunohistochemical marker. We found in both tumor types focal to diffuse immunostaining for CD56 and TLE1, but no consistent staining for the other antigens. In BCOR-CCNB3 sarcomas, we observed focal or diffuse immunoreactivity for CCNB3, TLE1, and NKX2.2. Most CIC-associated sarcoma cases were WT1-positive. We conclude that even though BCOR-CCNB3 and CIC-associated sarcomas are histological and immunohistochemical mimics of Ewing sarcomas, immunostaining for CCNB3 and WT1 can be used to differentiate them from Ewing sarcoma.
TLE1 is a diagnostic marker of synovial sarcoma, one of the differential diagnoses of small round cell sarcoma, but its specificity has been contested. [21] We observed diffuse TLE1 expression in all cases, but not associated with the SS18-SSX fusion gene. As a consequence, poorly differentiated synovial sarcoma should be carefully ruled out by FISH or RT-PCR.
The differential diagnosis of BCOR-CCNB3/CIC-associated sarcoma covers a broad spectrum. In particular, translocation-associated small round cell tumors need to be excluded. FISH and CCNB3 immunohistochemical staining allowed us to differentiate CIC-DUX4 and BCOR-CCNB3 sarcomas from other SRCSs. In two tumors, we failed to confirm a CIC gene rearrangement by RT-PCR, which suggests that these tumors may have carried other CIC-associated gene aberrations. Genome analysis by FISH or RT-PCR would be necessary for a definitive diagnose of both tumor types. For screening, we recommend a CIC split FISH probe and CCNB3 immunohistochemical staining.
In our institution, a diagnosis of typical Ewing sarcomas was based in the past only on histological findings and extensive surveys of IHC and FISH did not include BCOR-CCNB3− or CIC–associated sarcomas (data not shown). Typical cases of Ewing sarcoma can be distinguished from these sarcomas by histology.
We conclude that BCOR-CCNB3− and CIC–associated sarcomas show a myxoid/epithelioid component in addition to a small round cell component. Moreover, these heterogeneous components showed low mitotic activity. The morphological heterogeneity of these sarcomas may be responsible for misdiagnoses and misguided therapy decisions.
References
Fletcher CDM, Chibon F, Mertens F (2013) Undifferentiated/unclassified sarcoma. In: Fletcher CDM, Bridge JA, Hogendoorn PCW, Mertens F (eds) WHO classification of Tumours of soft tissue and bone. IARC Press, Lyon, pp 236–238
Kawamura-Saito M, Yamazaki Y, Kaneko K et al (2006) Fusion between CIC and DUX4 up-regulates PEA3 family genes in Ewing-like sarcomas with t (4;19)(q35;q13) translocation. Hum Mol Genet 15:2125–2137
Graham C, Chilton-MacNeill S, Zielenska M, Somers GR (2014) Distinct transcriptional signature and immunoprofile of CIC-DUX4 fusion-positive round cell tumors compared to EWSR1-rearranged Ewing sarcomas: further evidence toward distinct pathologic entities. Genes Chromosomes Cancer. 53:622–633
Puls F, Niblett A, Marland G et al (2014) BCOR-CCNB3 (Ewing-like) sarcoma: a clinicopathologic analysis of 10 cases, in comparison with conventional Ewing sarcoma. Am J Surg Pathol 38:1307–1318
Graham C, Chilton-MacNeill S, Zielenska M et al (2012) The CIC-DUX4 fusion transcript is present in a subgroup of pediatric primitive round cell sarcomas. Hum Pathol 43:180–189
Italiano A, Sung YS, Zhang L et al (2012) High prevalence of CIC fusion with double-homeobox (DUX4) transcription factors in EWSR1-negative undifferentiated small blue round cell sarcomas. Genes Chromosomes Cancer 51:207–218
Kajtár B, Tornóczky T, Kálmán E, Kuzsner J, Hogendoorn PC, Szuhai K (2014) CD99-positive undifferentiated round cell sarcoma diagnosed on fine needle aspiration cytology, later found to harbour a CIC-DUX4 translocation: a recently described entity. Cytopathology 25:129–132
Choi EY, Thomas DG, McHugh JB et al (2013) Undifferentiated small round cell sarcoma with t(4;19)(q35;q13.1) CIC-DUX4 fusion: a novel highly aggressive soft tissue tumor with distinctive histopathology. Am J Surg Pathol 37:1379–1386
Machado I, Cruz J, Lavernia J et al (2013) Superficial EWSR1-negative undifferentiated small round cell sarcoma with CIC/DUX4 gene fusion: a new variant of Ewing-like tumors with locoregional lymph node metastasis. Virchows Arch 463:837–842
Antonescu C (2014) Round cell sarcomas beyond Ewing: emerging entities. Histopathology 64:26–37
Panagopoulos I, Gorunova L, Bjerkehagen B, Heim S (2014) The “grep” command but not FusionMap, FusionFinder or chimera scan captures the CIC-DUX4 fusion gene from whole transcriptome sequencing data on a small round cell tumor with t(4;19)(q35;q13). PLoS One 9:e99439
Bielle F, Zanello M, Guillemot D et al (2014) Unusual primary cerebral localization of a CIC-DUX4 translocation tumor of the Ewing sarcoma family. Acta Neuropathol 128:309–311
Haidar A, Arekapudi S, DeMattia F, Abu-Isa E, Kraut M (2015) High-grade undifferentiated small round cell sarcoma with t(4;19)(q35;q13.1) CIC-DUX4 fusion: emerging entities of soft tissue tumors with unique histopathologic features--a case report and literature review. Am J Case Rep 16:87–94
Tardío JC, Machado I, Navarro L et al (2015) Ewing-like sarcoma with CIC-DUX4 gene fusion in a patient with neurofibromatosis type 1. A hitherto unreported association. Pathol Res Pract 211:877–882
Sugita S, Arai Y, Tonooka A et al (2014) A novel CIC-FOXO4 gene fusion in undifferentiated small round cell sarcoma: a genetically distinct variant of Ewing-like sarcoma. Am J Surg Pathol 38:1571–1576
Solomon DA, Brohl AS, Khan J, Miettinen M (2014) Clinicopathologic features of a second patient with Ewing-like sarcoma harboring CIC-FOXO4 gene fusion. Am J Surg Pathol 38:1724–1725
Pierron G, Tirode F, Lucchesi C et al (2012) A new subtype of bone sarcoma defined by BCOR-CCNB3 gene fusion. Nat Genet 44:461–466
Cohen-Gogo S, Cellier C, Coindre JM et al (2014) Ewing-like sarcomas with BCOR-CCNB3 fusion transcript: a clinical, radiological and pathological retrospective study from the Société Française des Cancers de L'Enfant. Pediatr Blood Cancer 61:2191–2198
Peters TL, Kumar V, Polikepahad S et al (2015) BCOR-CCNB3 fusions are frequent in undifferentiated sarcomas of male children. Mod Pathol 28:575–586
Shibayama T, Okamoto T, Nakashima Y et al (2015) Screening of BCOR-CCNB3 sarcoma using immunohistochemistry for CCNB3: a clinicopathological report of three pediatric cases. Pathol Int 65:410–414
Kosemehmetoglu K, Vrana JA, Folpe AL (2009) TLE1 expression is not specific for synovial sarcoma: a whole section study of 163 soft tissue and bone neoplasms. Mod Pathol 22:872–878
Acknowledgements
Technical support for the experimental trials was provided by the following laboratory assistants: Motoko Tomita, Mami Nakamizo, Juri Godo, Kozue Matsuda, Naomi Tateishi, Hisami Matsumoto, and Noriko Aoki. We also appreciate the technical assistance of the Research Support Center, Kyushu University Graduate School of Medical Sciences.
Case selection and review were accomplished by the following MDs and PhDs: Kiyoshi Saeki, Shinichi Tsuruta, Yuki Kuma, Izumi Kinoshita, Takeshi Iwasaki, Kayoko Nakano, Tatsurou Abe, Naoki Mochidome, Yu Nakaji, Kazuki Takada, Nobuko Yasutake, Yuki Tateishi, Masanobu Sato, Keigo Ozono, Atsushi Abe, Kang-Ring Wang, Risa Hida, Yukihiko Okumura, Tomoko Shinozaki, Kaai Shida, Masaaki Sugimoto, Tetsuyuki Miyazaki, Toshimitsu Nishijima, Hiroshi Koga, Reiko Kumagai, Yukiko Kohno, Yoshiteru Kumagae, Hiroko Imamura, Murasaki Aman, Minako Hirahashi, and Yoshihiro Ohishi.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
This study was approved by the Ethics Committee of Kyushu University (Nos. 25-111, 25-143) and conducted according to the principles embodied in the Declaration of Helsinki. Informed consent was obtained from the subjects or guardians.
Funding
This study was supported by a JSPS KAKEN Grant (No. 25293088) and by funds from the Scholarship Program of the Takeda Science Foundation.
Conflict of interest
The authors declare that they have no conflict of interest.
Rights and permissions
About this article

Cite this article
Yamada, Y., Kuda, M., Kohashi, K. et al. Histological and immunohistochemical characteristics of undifferentiated small round cell sarcomas associated with CIC-DUX4 and BCOR-CCNB3 fusion genes. Virchows Arch 470, 373–380 (2017). https://doi.org/10.1007/s00428-017-2072-8
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00428-017-2072-8