
Abstract
To determine which immunohistochemical markers are useful for the identification of neoplastic myoepithelial cells in adenomyoepithelioma of the breast, the expression of seven myoepithelial markers (α-smooth muscle actin (α-SMA), calponin, p63, CD10, cytokeratin 5/6, cytokeratin 14, and S-100) was examined in 19 lesions from 16 patients. The lesion consisted of seven spindle and 12 clear cell lesions. For normal myoepithelial cells, α-SMA, calponin, and p63 were significantly more sensitive than cytokeratin 5/6, cytokeratin 14, and S-100. There was no significant difference in the expression of α-SMA, calponin, p63, and CD10 in neoplastic myoepithelial cells of adenomyoepithelioma regardless of spindle or clear cell types. In spindle cell lesions, high-molecular weight cytokeratins (HMWCK; cytokeratin 5/6 and cytokeratin 14) tended to show higher staining scores and S-100 showed lower staining scores than other markers. In clear cell lesions, HMWCK showed significantly lower staining scores than the other five markers. There was no significant difference in staining scores among the other five markers. HMWCK showed a unique paradoxical staining pattern in clear cell lesions, with diffusely positive inner epithelial cells and completely negative outer myoepithelial cells. Although the sensitivity of HMWCK in clear cell lesions is low, with this unique paradoxical staining pattern and relatively high sensitivity in spindle cell lesions, HMWCK could be useful in diagnosing adenomyoepithelioma. In choosing immunohistochemical markers, any of the seven markers are useful, but combining HMWCK and any one of α-SMA, calponin, and p63 would be a good panel for the diagnosis of adenomyoepithelioma.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Adenomyoepithelioma of the breast is a rare type of breast tumor characterized by both epithelial and myoepithelial proliferation [1]. The term “adenomyoepithelioma,” originally used for a sweat gland tumor [2], was first applied to a breast counterpart by Hamperl [3]. Adenomyoepithelioma is a well-circumscribed mass, and complete surgical excision alone is usually an adequate treatment [4, 5]. Recurrences and distant metastasis of “benign” adenomyoepithelioma after inadequate resection have been reported [6]. There have been reports of malignant counterpart and/or malignant transformation [7–10] and rare cases of tumor-related death [8, 9]. Either the epithelial or myoepithelial component or both components can participate in malignant transformation [9, 11, 12], and in some cases, the biphasic pattern is maintained at the site of metastasis [8, 9].
Although adenomyoepithelioma is a biphasic tumor, myoepithelial proliferation is usually prominent. For distinction from myoepithelial hyperplasia, significant myoepithelial proliferation, resulting in nests or nodules of myoepithelial cells or compression of epithelial components, supports the diagnosis of adenomyoepithelioma [5]. The histologic appearance of adenomyoepithelioma is heterogeneous due to the variety of myoepithelial morphology and architectural patterns [13]. Tavassoli classified adenomyoepithelioma into three categories based on mixed architectural patterns and cytomorphological features of myoepithelial cells [14]. The spindle cell type is composed of solid proliferation of spindle myoepithelial cells with a minor component of epithelial-lined spaces [15, 16]. The tubular pattern is characterized by proliferation of tubular structures with inner epithelial and outer myoepithelial cells. The myoepithelial cells have characteristic clear cytoplasm, and their proliferation is prominent, often to the extent to which they obscure the inner epithelial component. The lobular type shows solid proliferation of clear, eosinophilic, or plasmacytoid myoepithelial cells and has a thick collagenous capsule that extends and lobulates the tumor cell proliferation.
Identification of myoepithelial proliferation sometimes requires immunohistochemistry. There have been several descriptions of myoepithelial marker expression in the neoplastic myoepithelial cells of adenomyoepithelioma [8, 10, 12, 14, 16–18], in which expression of a few classical myoepithelial markers, such as actin, S-100, and cytokeratins, were briefly described. The only systematic evaluation of myoepithelial marker expression on neoplastic myoepithelial cells of adenomyoepithelioma was provided by Popnikolov et al. [19] and Hungermann et al. [20]. Popnikolov et al. studied myoepithelial marker expression in eight cases of adenomyoepithelioma and found invariable expression of cytokeratin, maspin, smooth muscle actin, and S-100 in the myoepithelial component of adenomyoepithelioma and less frequent expression of CD10 (50 %) and myosin (75 %) [19]. Hungermann et al. analyzed expression of various cytokeratins, p63, α-smooth muscle actin, and vimentin in a series of 27 adenomyoepithelial tumors of the breast. They showed various degree and combination of expression of these markers in tumor cells [20].
In the present study, we examined the expression of seven commonly used myoepithelial markers in adenomyoepithelioma and clarified which myoepithelial markers should be used to appropriately identify the myoepithelial component of adenomyoepithelioma. We also examined whether the expression of myoepithelial markers differed between different myoepithelial morphologies, such as spindle cells and clear cells.
Materials and methods
A total of 16 adenomyoepithelioma cases were included in the present study. We only used surgically resected cases in which the entire lesion could be evaluated. Three cases from April 2000 to April 2013 were retrieved from the surgical pathology files of Nagoya Medical Center. Six cases during a similar period were retrieved from the surgical pathology files of Aichi Cancer Center. Seven cases were retrieved from the consultation files of SI and SM.
The study cases were classified into three types based on the morphology of the neoplastic myoepithelial cells: spindle cell type in which 90 % or more of the myoepithelial cells showed spindle cell morphology, clear cell type in which 90 % or more of the myoepithelial cells had clear cytoplasm and showed an epithelioid arrangement, or mixed type in which spindle cells and clear cells were mixed and each component accounted for more than 10 % of the myoepithelial cells. There were no cases in which non-spindle eosinophilic or plasmacytoid myoepithelial cells occupied a significant proportion (10 % or more) of the tumor.
Four-micrometer serial sections were cut from the representative paraffin block of each case. For immunohistochemical evaluation, we selected seven markers, α-smooth muscle actin (α-SMA), calponin, CD10, p63, cytokeratin 5/6, cytokeratin 14, and S-100 protein, which are commonly used in many institutions for routine practice. Details of the antibodies are summarized in Table 1. Signals were detected by using a Benchmark XT automated immunostainer (Ventana Medical System, Tucson, AZ, USA). The proportion of neoplastic myoepithelial cells that were positive for a marker was grossly scored as follows: (−), completely negative; (1+), less than 10 %; (2+), 10–49 %; (3+), 50–69 %; and (4+), 70 % or more. In cases of mixed-type morphology, spindle cell and clear cell areas were evaluated separately. Signal intensity was not taken into consideration. The positive signals were scored at cytoplasm for α-SMA, calponin, cytokeratin 5/6, and cytokeratin 14; at the cell membrane for CD10; at the nuclei for p63; and at both cytoplasm and nuclei for S-100. The staining pattern of myoepithelial cells surrounding normal ducts and lobules in the same specimens, if adequately present, was also evaluated as non-neoplastic positive controls. For one clear cell type case, which was a consultation case, cytokeratin 14 could not be stained because there were an insufficient number of unstained slides.
The results of the staining patterns were statistically analyzed with the Kruskal-Wallis test and Mann-Whitney’s U test. P values <0.05 were regarded as statistically significant.
Results
There were four cases of spindle cell type, nine cases of clear cell type, and three cases of mixed type. In the spindle cell type tumors, spindle myoepithelial cells predominated over the epithelial components, and a schwannoma-like palisading pattern was prominent in one case (Fig. 1a, b). In the clear cell type, clear myoepithelial cells surrounded tubular structures, often compressing epithelial components (Fig. 2a, c). The epithelial components had an eosinophilic appearance at least focally in all nine cases. The neoplastic myoepithelial cells in one of the three mixed-type cases consisted of 80 % spindle cells and 20 % clear cells. One case had a focal pleomorphic adenoma-like area occupying 20 % of the tumor. Spindle and clear cells occupied 50 and 30 % of the remaining part of the tumor, respectively. The other mixed-type case was considered to be malignant because the tumor metastasized to the lung 2 years after surgery. The neoplastic myoepithelial cells consisted of 80 % clear cells and 20 % spindle cells. Both myoepithelial and epithelial components had nuclear atypia, mitoses, and focal necrosis. A biphasic pattern was maintained in the metastatic site. Minor components of non-clear neoplastic myoepithelial cells in an epithelioid arrangement were present in 6 of 16 cases.

Adenomyoepithelioma, spindle cell type. a Nuclear palisading simulating schwannoma was prominent in this case. b Neoplastic myoepithelial cells predominate over the epithelial components. c Cytokeratin 14 and d cytokeratin 5/6 in the same area of b. More than 90 % of the neoplastic spindle cells are positive

Adenomyoepithelioma, clear cell type. a, c Myoepithelial cells have abundant clear cytoplasm and are arranged in an epithelioid pattern surrounding the inner epithelial layer. b, d cytokeratin 5/6. The inner epithelial layer is strongly positive, and the outer clear myoepithelial cells are completely negative. e calponin. f p63. Calponin and p63 are diffusely positive in the outer clear myoepithelial cells
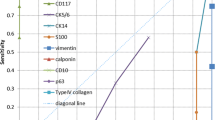
Expression of the seven myoepithelial markers in myoepithelial cells of normal ducts and acini was evaluated in 15 of 16 cases (Table 2). The staining pattern of these myoepithelial markers in the normal myoepithelial cells differed significantly among the seven markers (Kruskal-Wallis test: P < 0.01). The staining pattern of α-SMA, calponin, and p63 were graded as (4+) in all 15 cases. α-SMA, calponin, and p63 had significantly higher staining scores as compared to cytokeratin 14 (Mann-Whitney’s U test: P = 0.029), cytokeratin 5/6 (P = 0.016), and S-100 (P < 0.01). CD10 showed significantly higher staining scores as compared to S-100 (Mann-Whitney’s U test: P < 0.01). No significant difference was seen between CD10 and cytokeratin 14 (P = 0.118) and between CD10 and cytokeratin 5/6 (P = 0.053). α-SMA, calponin, p63, and CD10 were not expressed in normal luminal epithelial cells; however, cytokeratin 5/6, cytokeratin 14, and S-100 were expressed in various proportions of normal luminal epithelial cells. Non-neoplastic spindle stromal cells were frequently positive for α-SMA and calponin. CD10 was also expressed in stromal cells, but both the signal intensity and number of positive cells were much less than for α-SMA and calponin. Stromal cells were not positive for S-100, p63, cytokeratin 14, or cytokeratin 5/6.
For evaluation of myoepithelial markers in adenomyoepithelioma, a total of seven spindle cell lesions (four cases of spindle cell type and three cases of mixed type) and 12 clear cell lesions (nine cases of clear cell type and three cases of mixed type) were examined. Expression of the seven myoepithelial markers in each lesion is shown in Table 3. There was no significant difference in the expression of myoepithelial markers in total (Kruskal-Wallis test, P = 0.122) and in spindle cell types (P = 0.958). However, in spindle cell types, high-molecular weight cytokeratins (HMWCK; cytokeratin 5/6 and cytokeratin 14) tended to have higher scores than other markers (Fig. 1c, d). Cytokeratin 5/6 had significantly higher scores than CD10 (Mann-Whitney’s U test, P < 0.01) and S-100 (P < 0.01), and cytokeratin 14 had significantly higher scores than S-100 (P = 0.013).
There was a significant difference in the expression of myoepithelial markers in clear cell types (Kruskal-Wallis test, P < 0.01). HMWCK had significantly lower scores than any other myoepithelial marker (Mann-Whitney’s U test, P < 0.01). There was no significant difference in myoepithelial marker expression among α-SMA, calponin, p63, CD10, and S-100 in clear cell types.
Expression of HMWCK in clear cell type lesions was significantly lower than in spindle cell type lesions (Mann-Whitney’s U test, P < 0.01). Seven lesions (100 %) of the spindle cell type were graded as (4+) for cytokeratin 5/6 (Fig. 2), but 7 of 12 clear cell lesions (58 %) were completely negative. Six of seven spindle cell type lesions (86 %) were graded as (4+) for cytokeratin 14, but 5 of 11 clear cell lesions (45 %) were completely negative. Five of 12 clear cell lesions (42 %) were completely negative for both cytokeratin 5/6 and cytokeratin 14. Five of 7 cytokeratin 5/6-completely negative cases were completely negative for cytokeratin 14. One cytokeratin 5/6-completely negative case was graded as (2+) for cytokeratin 14. Cytokeratin 14 immunostaining was not available for the other cytokeratin 5/6-completely negative case. These completely negative lesions showed a unique paradoxical staining pattern; the inner luminal epithelial cells were diffusely positive for HMWCK, and the outer clear myoepithelial cells were completely negative (Fig 2a–d). The inner epithelial cells positive for HMWCK had deep eosinophilic cytoplasm in hematoxylin and eosin (HE) sections (Fig. 2a, c). Epithelial cells without deep eosinophilic cytoplasm did not show diffuse HMWCK expression. Lesions with a paradoxical staining pattern were positive for other myoepithelial markers (Fig 2e, f).
S-100 expression was also significantly different between spindle cell and clear cell type lesions (Mann-Whitney’s U test, P = 0.03). The S-100 staining scores were significantly higher in the clear cell type than in the spindle cell type. One mixed-type case with a pleomorphic adenoma-like area was diffusely positive for S-100 in the myoepithelial cells of the entire tumor, regardless of the cytomorphology of the myoepithelial cells, including the pleomorphic adenoma-like area.
There was no difference in the expression of α-SMA, calponin, p63, and CD10 between spindle cell and clear cell type lesions (P = 0.155∼0.439).
We compared the expression of myoepithelial markers in normal and neoplastic myoepithelial cells. The staining scores of α-SMA, calponin, p63, CD10, and cytokeratin 14 were significantly decreased in neoplastic myoepithelial cells as compared to normal myoepithelial cells (Mann-Whitney’s U test, P = 0.019, 0.035, 0.035, 0.030, and 0.034, respectively). There was no significant difference in the staining scores of cytokeratin 5/6 and S-100 between normal and neoplastic myoepithelial cells (P = 0.901 and 0.084, respectively).
Discussion
In addition to classical myoepithelial markers, actin [21] and S-100 [22], numerous myoepithelial markers are useful for immunohistochemical studies of formalin-fixed paraffin-embedded tissues. These markers recognize different antigens in myoepithelial cells, and their sensitivity and specificity are variable [23–28]. Among them, calponin, p63, CD10, and HMWCK are effective in routine practice due to their sensitivity, specificity, and ease of interpretation [23]. In the present study, we evaluated the usefulness of α-SMA, S-100, calponin, p63, CD10, cytokeratin 5/6, and cytokeratin 14 for the identification of the neoplastic myoepithelial components of adenomyoepithelioma.
First, we found that the seven myoepithelial markers had various degrees of positive staining, even in normal myoepithelial cells. The most sensitive markers for normal myoepithelial cells were α-SMA, calponin, and p63, followed by CD10, cytokeratin 14, cytokeratin 5/6, and S-100. Recently, Hilson et al. reported that expression of myoepithelial markers was decreased in non-neoplastic myoepithelial cells surrounding ductal carcinoma in situ (DCIS) and benign sclerosing lesions [29, 30]. They suggested that the sensitivities of myoepithelial markers varied and that the sensitivity of the same marker could also be different in different pathologic conditions. High sensitivity of α-SMA and low sensitivity of cytokeratin 5/6 in our data from normal myoepithelial cells were comparable to the data of Hilson et al. [29, 30]. Because of the low sensitivity and specificity of HMWCK and S-100 in identifying normal myoepithelial cells, we consider that these markers should not be used alone when the presence or absence of myoepithelial cells is critical for diagnosis.
Next, we evaluated myoepithelial marker expression in neoplastic myoepithelial cells of adenomyoepithelioma. Compared to the staining scores in normal myoepithelial cells, most of the markers, except for cytokeratin 5/6 and S-100, had decreased staining scores in neoplastic cells. This decreased expression of myoepithelial markers may reflect decreased functional differentiation in neoplastic cells. There was no significant difference in staining scores in adenomyoepithelioma among the seven myoepithelial markers in total. α-SMA, calponin, p63, and CD10, which are sensitive markers of normal myoepithelial cells, are also useful and sensitive markers of neoplastic myoepithelial cells, regardless of spindle or clear cell types.
Several notable differences were seen in the staining scores of myoepithelial markers, especially between HMWCK and other markers, when comparing these markers in spindle cell and clear cell type lesions. The sensitivity of HMWCK to identify neoplastic spindle myoepithelial cells is higher than other markers, especially significantly higher than CD10 and S100. Considering the absence of cross-reactivity with non-neoplastic spindle stromal cells, HMWCK are considered to be superior to α-SMA, calponin, and CD10 in identifying neoplastic spindle myoepithelial cells. On the other hand, the sensitivity of HMWCK in clear cell type lesion was significantly lower than that of other markers. The lower sensitivity of HMWCK in adenomyoepithelial tumor has hitherto not been reported. Hungermann et al. examined expression of HMWCK, p63, and SMA in 27 cases of adenomyoepithelioma of the breast and showed constant expression of HMWCK and p63 in these tumors [20]. The striking difference on the sensitivity of HMWCK seems to be partly due to the difference of evaluation method between the two studies. In our study, we strictly focused on myoepithelial marker expression in neoplastic myoepithelial cells and did not count the expression of these markers in neoplastic epithelial cells. In the study of Hungermann et al., they did not mention which component of adenomyoepithelial tumor expressed HMWCK.
The most notable result on the expression of HMWCK is that the HMWCK produced a very unique paradoxical staining pattern in clear cell type lesions. The inner epithelial layer was diffusely positive, and the outer myoepithelial layer was completely negative. The inner epithelial cells that were positive for HMWCK had characteristic deep eosinophilic cytoplasm. HMWCK expression in luminal epithelial cells is well known [23, 31–34]. The predominance of luminal expression of HMWCK and very weak HMWCK expression of myoepithelial cells in the normal acini was also described [32]. It should be noted that there is considerable variation in HMWCK expression in normal breast even within the same breast [32]. The paradoxical staining pattern of clear cell lesions might recapitulate the staining pattern of normal acini. The other possibility is that the unique relationship between inner HMWCK-positive neoplastic epithelial cells and outer negative neoplastic myoepithelial cells might reflect the special interaction between the two neoplastic components that is deviated from the normal cellular interaction. Although the exact biological mechanism and significance are unknown, the recognition of this unique staining pattern of HMWCK can assist in the practical pathological diagnosis of adenomyoepithelioma.
Among seven myoepithelial markers in the present study, p63 and HMWCK are also known to be expressed in basal/progenitor cells which lack specific lineage markers, and both markers were reported to be co-expressed [35–37]. In this study, we found p63-positive and HMWCK-negative population in both normal basal/myoepithelial cells and neoplastic clear myoepithelial component in adenomyoepithelioma. The presence and the implication of this phenotype have not been reported. One possibility is the difference in the clone of antibody. We used D5/6, but D5/16B4 was used by several other studies [36, 37]. As most of the HMWCK-negative/p63-positive cases were positive for other myoepithelial markers such as α-SMA and calponin, another interpretation is that HMWCK-negative and p63-positive myoepithelial cells might reflect slightly more differentiated myoepithelial cells which have lost immature basal/progenitor phenotype. The presence of HMWCK-negative and SMA-positive myoepithelial cells was described in the study using in situ triple immunofluorescence lineage/differentiation tracing [37].
Although the S-100 staining score in normal myoepithelial cells and adenomyoepithelioma of the spindle cell type was lower than for other markers, its expression in adenomyoepithelioma of the clear cell type was almost identical to that of α-SMA, calponin, p63, and CD10. Notably, diffuse and intense expression of S-100 throughout the tumor tissue was seen in one mixed-type case with pleomorphic adenoma-like areas. Pleomorphic adenoma of the breast is a very rare neoplasm that has similarities to adenomyoepithelioma in that it exhibits epithelial and myoepithelial differentiation. Its origin is considered to be a single cell that has the potential for divergent differentiation [38]. S-100 expression in all cell types of pleomorphic adenoma of the breast has been demonstrated [38, 39]. Boecker et al. recently confirmed that both pleomorphic adenoma and epithelial-myoepithelial tumor of the breast and salivary gland differentiate from keratin K5/K14-positive p63-positive progenitor cells [37]. Although the lack of myxoid or chondromyxoid stroma differentiates adenomyoepithelioma from pleomorphic adenoma, these two lesions could be closely related, as exemplified by the single case of the present study that had features of both tumor types within one lesion.
In conclusion, any of the seven myoepithelial markers are useful for the diagnosis of adenomyoepithelioma. Considering the relatively high sensitivity of α-SMA, calponin, and p63 in both spindle and clear cell lesions and the unique paradoxical staining pattern and relatively high sensitivity of HMWCK in spindle cell lesions, it is reasonable to choose one or several markers from each group for the immunohistochemical panel of adenomyoepithelioma. It is also important to consider the morphology of the lesion (i.e., spindle or clear cell) when choosing immunohirstochemical markers.
References
Lakhani SR, Hayes M, Eusebi V (2012) Adenomyoepithelioma and adenomyoepithelioma with carcinoma. In: Lakhani SR, Ellis IO, Schnitt SJ et al (eds) WHO Classification of Tumours of the Breast. IARC, Lyon, pp 122–123
Hartz PH (1946) Adenomyoepithelioma of sweat gland; report of a case. Am J Clin Pathol 16:385–390
Hamperl H (1970) The myoepithelia (myoepithelial cells): normal state, regressive changes, hyperplasia, tumors. Curr Top Pathol 53:161–221
Rosen PP (1987) Adenomyoepithelioma of the breast. Hum Pathol 18:1232–1237
McLaren BK, Smith J, Schuyler PA, Dupont WD, Page DL (2005) Adenomyoepithelioma: clinical, histologic, and immunohistologic evaluation of a series of related lesions. Am J Surg Pathol 29:1294–1299
Nadelman CM, Leslie KO, Fishbein MC (2006) “Benign”, metastasizing adenomyoepithelioma of the breast. A report of 2 cases. Arch Pathol Lab Med 130:1349–1353
Kiaer H, Nielsen B, Paulsen S, Sørensen IM, Dyreborg U, Blichert-Toft M (1984) Adenomyoepithelial adenosis and low-grade malignant adenomyoepithelioma of the breast. Virchows Arch A 405:55–67
Loose JH, Patchefsky AS, Hollander IJ, Lavin LS, Cooper HS, Katz SM (1992) Adenomyoepithelioma of the breast. A spectrum of biologic behavior. Am J Surg Pathol 16:868–876
Rasbridge SA, Millis RR (1998) Adenomyoepithelioma of the breast with malignant features. Virchows Arch 432:123–130
Hayes MM (2011) Adenomyoepithelioma of the breast: a review stressing its propensity for malignant transformation. J Clin Pathol 64:477–484
Dorpe JV, Pauw AD, Moerman P (1998) Adenoid cystic carcinoma arising in an adenomyoepithelioma of the breast. Virchows Arch 432:119–122
Ahmed AA, Heller DS (2000) Malignant adenomyoepithelioma of the breast with malignant proliferation of epithelial and myoepithelial elements. A case report and review of the literature. Arch Pathol Lab Med 124:632–636
Zarbo RJ, Oberman HA (1983) Cellular adenomyoepithelioma of the breast. Am J Surg Pathol 7:863–870
Tavassoli FA (1991) Myoepithelial lesions of the breast. Myoepitheliosis, adenomyoepithelioma, and myoepithelial carcinoma. Am J Surg Pathol 15:554–568
Cameron HM, Hamperl H, Warambo W (1974) Leiomyosarcoma of the breast originating from myothelium (myoepitehlium). J Pathol 114:89–92
Weidner N, Levine JD (1988) Spindle-cell adenomyoepithelioma of the breast. A microscopic, ultrastructural, and immunohistochemical study. Cancer 62:1561–1567
Choi JS, Bae JY, Jung WH (1996) Adenomyoepithelioma of the breast. Its diagnostic problems and histogenesis. Yonsei Med J 37:284–289
Catena F, Santini D, Saverio SD, Ansaloni L, Taffurelli M (2008) Adenomyoepithelioma of the breast: an intricate diagnostic problem. Breast Care 3:125–127
Popnikolov NK, Ayala AG, Graves K, Gatalica Z (2003) Benign myoepithelial tumors of the breast have immunophenotypic characteristics similar to metaplastic matrix-producing and spindle cell carcinomas. Am J Clin Pathol 120:161–167
Hungermann D, Buerger H, Oehlschlegel C, Herbst H, Boecker W (2005) Adenomyoepithelial tumours and myoepithelial carcinomas of the breast—a spectrum of monophasic and biphasic tumours dominated by immature myoepithelial cells. BMC Cancer 5:92
Mukai K, Schollmeyer JV, Rosai J (1981) Immunohistochemical localization of actin. Application in surgical pathology. Am J Surg Pathol 5:91–97
Nakajima T, Kameya T, Watanabe S, Hirota T, Sato Y, Shimosato Y (1982) An immunoperoxidase study of S-100 protein distribution in normal and neoplastic tissues. Am J Surg Pathol 6:715–727
Dewar R, Fadare O, Gilmore H, Gown AM (2011) Best practices in diagnostic immunohistochemistry. Myoepithelial markers in breast pathology. Arch Pathol Lab Med 135:422–429
Lazard D, Sastre X, Frid MG, Glukhova MA, Thiery JP, Koteliansky VE (1993) Expression of smooth muscle-specific proteins in myoepithelium and stromal myofibroblasts of normal and malignant human breast tissue. Proc Natl Acad Sci 90:999–1003
Barbareschi M, Pecciarini L, Cangi MG, Macrí E, Rizzo A, Viale G, Doglioni C (2001) p63, a p53 homologue, is a selective nuclear marker of myoepithelial cells of the human breast. Am J Surg Pathol 25:1054–1060
Reis-Filpho JS, Schmitt FC (2002) Taking advantage of basic research: p63 is a reliable myoepithelial and stem cell marker. Adv Anat Pathol 9:280–289
Moritani S, Kushima R, Sugihara H, Bamba M, Kobayashi TK, Hattori T (2002) Availability of CD10 immunohistochemistry as a marker of breast myoepithelial cells on paraffin sections. Mod Pathol 15:397–405
Gillett CE, Bobrow LG, Millis RR (1990) S100 protein in human mammary tissue immunoreactivity in breast carcinoma, including Paget’s disease of the nipple, and value as a marker of myoepithelial cells. J Pathol 160:19–24
Hilson JB, Schnitt SJ, Collins LC (2009) Phenotypic alterations in ductal carcinoma in situ-associated myoepithelial cells. Biologic and diagnostic implications. Am J Surg Pathol 33:227–232
Hilson JB, Schnitt SJ, Collins LC (2010) Phenotypic alterations in myoepithelial cells associated with benign sclerosing lesions of the breast. Am J Surg Pathol 34:896–900
Otterbach F, Bánkfalvi Ά, Bergner S, Decker T, Krech R, Boecker W (2000) Cytokeratin 5/6 immunohistochemistry assists the differential diagnosis of atypical proliferations of the breast. Histopathology 37:232–240
Gusterson BA, Ross DT, Heath VJ, Stein T (2005) Basal cytokeratins and their relationship to the cellular origin and functional classification of breast cancer. Breast Cancer Res 7:143–148
Su L, Morgan PR, Lane B (1996) Expression of cytokeratin messenger RNA versus protein in the normal mammary gland and in breast cancer. Hum Pathol 27:800–806
Clarke CL, Sandle J, Parry SC, Reis-Filho JS, O’Hare MJ, Lakhani SR (2004) Cytokeratin 5/6 in normal human breast: lack of evidence for a stem cell phenotype. J Pathol 204:147–152
Nylander K, Vojtesek B, Nenutil R, Lindgren B, Roos G, Zhanxiang W, Sjöström B, Dahlqvist Å, Coates PJ (2002) Differential expression of p63 isoforms in normal tissues and neoplastic cells. J Pathol 198:417–427
Reis-Filho JS, Simpson PT, Martins A, Preto A, Gärtner F, Schmitt FC (2003) Distribution of p63, cytokeratin 5/6 and cytokeratin 14 in 51 normal and 400 neoplastic human tissue samples using TARP-4 multi-tumor tissue microarray. Virchows Arch 443:122–132
Boecker W, Stenman G, Loening T, Andersson MK, Bankfalvi A, Holstein S, Heegaard S, Lange A, Berg T, Samoilova V, Tiemann K, Buchwalow I (2013) Mod Pathol 26:1086–1100
Diaz NM, McDivitt RW, Wick MR (1991) Pleomorphic adenoma of the breast: a clinicopathologic and immunohistochemical study of 10 cases. Hum Pathol 22:1206–1214
Sato K, Ueda Y, Shimasaki M, Ozaki M, Nitta N, Chada K, Ishikawa Y, Katsuda S (2005) Pleomorphic adenoma (benign mixed tumor) of the breast: a case report and review of the literature. Pathol Res Pract 201:333–339
Acknowledgments
This study was supported by a Grant-in-Aid for Clinical Research from the National Hospital Organization.
Conflict of interest
The authors declare that they have no conflicts of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Moritani, S., Ichihara, S., Yatabe, Y. et al. Immunohistochemical expression of myoepithelial markers in adenomyoepithelioma of the breast: a unique paradoxical staining pattern of high-molecular weight cytokeratins. Virchows Arch 466, 191–198 (2015). https://doi.org/10.1007/s00428-014-1687-2
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00428-014-1687-2