
Abstract
Increasing numbers of solitary fibrous tumors (SFTs) in the meninges have been reported since this entity was first recognized. While most cases previously reported were considered to be benign, the malignant potential of extrathoracic SFTs has not been excluded. The authors report a rare case of a meningeal SFT with malignant behavior occurring in a Japanese female patient, initially resected when she was 44 years old and recurring in the same place four times during a 26-year follow-up period. A metastatic tumor to the right lung arose 25 years after the resection of the first meningeal tumor and focal invasion into the cerebellum was also observed with her last (5th) meningeal tumor. Immunohistochemical analysis showed all tumors to be diffusely positive for CD34 and negative for EMA, with a so-called “patternless” histological pattern, featuring thin collagen fibers between tumor cells. A focal “staghorn” vascular pattern was also observed. Ki67 (MIB-1) labeling indices and mitosis rates were 3.1±1.2% and less than 1/10 high power fields (HPF) in the first meningeal tumor and 16.1±6.4% and 6/10HPF in the last (5th) one, respectively. Thus, the present case suggests that meningeal SFTs possess malignant potential so that careful long-term follow up is required.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The solitary fibrous tumor (SFT) is an uncommon spindle-cell neoplasm, first described as a pleural lesion in 1931 [17]. Extrathoracic SFTs [31] have also been increasingly recognized, including examples in the meninges [1, 2, 4, 5, 7, 8, 10, 15, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30]. Characteristic histological and immunohistochemical features of SFTs in any region are a “patternless” growth pattern, with spindle cells and keloid-like hyalinization, the lesions being intensely and diffusely positive for CD34 antigen and negative for EMA antigen [16]. In the meninges, fibrous meningioma and hemangiopericytoma (HPC) have been recognized as major tumors requiring differential diagnosis from SFTs [5, 10, 24, 29]. Most fibrous meningiomas are positive for EMA antigen, and HPCs are generally only focally and weakly positive for CD34 antigen [24]. The majority of extrathoracic SFTs, including those of meningeal origin, have been described as benign tumors. However, among about forty reported cases of meningeal SFTs, local recurrence was found in six [5, 22, 29, 30], including one case complicated with metastases to the lung and soft tissue [22]. We present here a case of malignant meningeal SFT which progressed after a very long (26 years) and indolent course featuring frequent recurrence and ultimate metastasis to the lung (Table 1). To our knowledge, this is only the second case in the English or Japanese literatures of a meningeal SFT which developed distant metastasis.
Materials and methods
All surgically resected tissues were routinely fixed in 10% formalin, embedded in paraffin and prepared for histological observation. Immunohistochemical analyses were performed by the avidin-biotin-peroxidase complex technique using a Vectastain ABC Elite Kit (Vector Laboratories Inc., Burlingame, CA) and diaminobenzidine for visualization of binding. The following antibodies were employed: anti-keratin (AE1/AE3, DakoCytomataion, Glostrup, Denmark, 1:50, with heat-pretreatment), anti-EMA (Zymed Laboratories Inc., South San Francisco, CA, 1:1), anti-vimentin (Ventana Medical Systems, Tucson, AZ, 1:1, with protease-pretreatment), anti-CD34 (Nichirei, Tokyo, Japan, 1:50), anti-Leu-7 (CD57, Ventana, 1:1, with heat-pretreatment), anti-S-100 protein (Dako, 1:400, with trypsin-pretreatment), anti-CD99 (12E7, Dako, 1:100), anti-CD99 (O-13, Santa Cruz Biotechnology Inc., Sant Cruz, CA, 1:40), anti-p53 (CM1, Novocastra Laboratories Ltd., Newcastle upon Tyne, UK, 1:100) and anti-Ki67 (MIB-1, Novocastra, 1:3000, with heat-pretreatment). Labeling indices for p53 and Ki67 and cellularity were generated from counts under a light-microscope in three randomly selected areas (with scale on the ocular, 0.252 mm×3 sights, which covered totally 1500~2000 cells) of each tumor, then expressed as mean values with standard deviation.
Case Report
This 70-year-old Japanese woman has been followed up as suffering from repeated local recurrence of atypical meningiomas in her left tentorial area and treated by repeated excision since 1976, when she was 44 years old (Table 1). To date, she has undergone six surgical resections of tumors, including five operations in the left tentoreal area (1976, 1984, 1995, 1999, 2002) and one in the lung (2001) (Fig. 1). Specimens from the last excision of the recurrent meningeal tumor showed histological and immunohistochemical characteristics of SFT, and, therefore, all of the previous slides of meningeal and pulmonary tumors were reviewed histologically and immunohistochemically. The immunohistochemical analyses demonstrated the lesions to be CD34 positive and EMA negative, suggesting a SFT rather than a meningioma. Histologically, a so-called patternless pattern was recognized, with focal staghorn-like vascular channels and no whirl formation, in line with the diagnosis as SFT. The pulmonary lesion was diagnosed as a metastatic tumor.

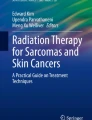
Magnetic resonance imaging (MRI) observation of the meningeal and lung tumors. a Third meningeal tumor found in left tentorium area in 1995. b Fourth meningeal tumor found in the same area in1999. c Lung metastatic tumor in the right upper lobe in 2001. d Fifth meningeal tumor of the left suboccipital region in 2002
Clinical history
In 1976, when the patient was 44 years old, she first visited a hospital with the complaint of headache persisting from 2 years previously. At that time, she walked with a shift to her right side and demonstrated an elevation of intra-cranial pressure (over 200 mmH2O), congestion of the retinal papilla and hemorrhage in her eyeground. A solid tumor, estimated to be 3 cm in diameter, was evident in her left tentorium on computed tomography (CT) scanning. Total resection of the tumor was performed and then histopathological diagnosis of a meningioma with immature features was given. The second meningeal tumor in the same region was noted 7.5 years later when she was 52 years old and again was totally resected. With continuous follow-up and magnetic resonance imagine (MRI) examination, the third (Fig. 1a) and fourth (Fig. 1b) local recurrent tumors were found when she was 63 years and 67 years old, respectively, and resected when they became 3 cm in diameter. She expressed only slight headaches before the operations. When she was 69 years old, a fifth tumor was apparent as a round and well-bordered abnormal shadow in the upper lobe of her right lung on chest X-rays, and CT and MRI confirmed the presence of a 1.8-cm diameter lesion (Fig. 1c). With histological observation of frequent mitosis and atypia indicative of malignancy in frozen sections, the right upper lobe was removed. The sixth tumor in her left sub-occipital region was resected 20 months later, when she was 70 years old (Fig. 1d).
Pathological findings
As shown above and in Fig. 2 and Fig. 3, all six tumors showed basically the same histological character, consisting of moderately hypercellular spindle cells with a “patternless” growth pattern, without apparent whirled cell arrangement or psammoma bodies. The tumors had thick collagen bundles with a hyaline appearance and intercellular collagen (Fig. 2a) and a reticulin network recognized with silver staining. Staghorn-like vascular channels were focally evident (Fig. 2b). Immunohistological analysis (Fig. 2c and d) showed the tumor cells to be completely negative for keratin and EMA and diffusely positive for vimentin and CD34. S-100 protein was negative and Leu-7 was positive. The staining results with anti-CD99 antibodies were contradictory, being positive with the 12E7 clone but negative with the O-13 clone. The lung tumor also had similar histological features with more apparent necrosis, with no attachment to the pleura.

Histopathological and immunohistochemical findings for the fifth meningeal tumor. a Collagen bundles with a hyaline appearance are evident. b Staghorn-like vascular channels are focally present. c Tumor cells are negative for EMA. d Tumor cells are diffusely positive for CD34

Histological findings of the sequentially resected tumors (a, c, e; HE staining and b, d, f; anti-Ki67 immunohistochemical staining). a, b The primary meningeal tumor resected in 1976. Note the hypercellular fibrous nature with a “pattern-less” pattern and a few Ki67 positive cells. c, d The metastatic tumor found in left lung in 2001. The lesion demonstrates necrosis and pressure on the surrounding lung tissue with many Ki67 positive cells. e, f The fifth meningeal tumor resected in 2002. Partial invasion into the cerebellum and many Ki67 positive cells are apparent
Sequential changes in malignant and/or proliferative features are summarized in Table 1. Focal cysts and/or necroses were more or less observed in all the tumors. The second meningeal tumor and the lung metastatic tumor had larger areas of necrosis (Fig. 3c). All tumors were well demarcated but the last meningeal tumor slightly invaded into the cerebellum (Fig. 3e). Cellularity was mildly high from the first tumor but the Ki67 index and mitosis index were low in the first and third tumors and higher in the later lesions (Table 1 and Fig. 3b, d, f). Labeling indices for p53 protein varied considerably.
Discussion
We have presented here a case of meningeal malignant SFT, which locally relapsed four times, metastasized to the lung and invaded in the cerebellum over a period of 26 years. The histopathological and immunohistochemial features of the tumors fit those for SFTs described in previous literature [31], including examples originating in the meninges [5, 24]. Since the first report by Carnerio and co-workers in 1996 [5], retrospective reviews of pathology files of meningioma and/or HPC of the meninges revealed that approximately 30 cases should be reclassified as SFT [5, 29, 30], and overall more than 40 cases have now been reported [1, 2, 4, 5, 6, 7, 8, 10, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30]. Of these, only one case showed metastasis to other organs (lung and soft tissue) [22]. In terms of the biological behavior of SFT, the pathological criteria for determining malignant potential are of obvious clinicopathological interest for pathologists.
Histological features associated with local or distant recurrence of intrathoracic SFTs are reported to include high cellularity, mitotic activity (>4/10 HPF), nuclear pleomorphism, and necrosis [13, 31, 33]. In extrathoracic SFTs, such as those occurring in the abdomen/pelvis, retroperitoneum, groin, trunk, and upper arm, these factors are associated with, but are not by themselves predictive of, aggressive clinical behavior [31]. It seems that there is no strict correlation between morphology and biology [14, 15, 19, 31]. The results of a recent karyotyping study showing tetrasomy 8 to be associated with malignant behavior in the SFT of the pleura [11] might provide a new solution to this issue. In the present case, the first tumor showed hypercellularity and some mitoses. Therefore, according to the histological criteria mentioned above, the tumors had an aggressive nature and malignant potential from the beginning. Of importance is the very long duration between surgical removal of the first tumor and the second tumor occurrence, and between the first tumor and lung metastasis (7.5 years and 25 years, respectively). The mitotic index and the Ki67 labeling index were medium in the first tumor and tended to gradually increase with shortening of the interval before recurrence. However, the patient is now (2003, 2 years after surgical excision of the metastatic tumor in the lung) clinically free from distant metastasis. This might mean that the biological nature of meningeal SFT is very indolent, even when atypical histological features are evident. However, meningeal SFT cases with malignant features are very low in number, and the follow-up duration has not been sufficiently long in most cases. Therefore, further clinicopathological analyses are required for clarification.
The confusion surrounding the relationship between the SFT and the HPC may be particularly due to the fact that both show “staghorn” sinusoidal vessels and CD34 positive immunoreactivity, even though HPCs react less strongly and diffusely for CD34 than do SFTs [24]. The tissue patterns of the two lesions appear to coexist in occasional cases, and the border between them is blurred [14]. It is the present consensus that small foci of HPC-like tissue can be accepted in SFT, but the histological overlap is not yet clear. Moreover, while not observed in the present case, not only intrathoracic but also extrathoracic HPC [3, 9] as well as SFT [12] may be sources of hypoglycemia due to the production of an insulin-like growth factor. Intracranial HPCs are reported to have a relatively high rate of recurrence (60–83%) and metastasis (23–28%) [18, 30] and it is difficult to predict malignant potential from cell proliferation indices such as Ki67 or PCNA [32]. Further comparative analysis of links between the presence of HPC-like tissue in a meningeal SFT and malignant behavior is necessary. Another tumor to be differentiated from meningeal SFT is fibrous meningioma but this can generally be achieved on the basis of its positivity for EMA and only weak or negative CD34 staining.
In conclusion, we have experienced a case of SFT derived from the meninges with malignant potential. In such lesions, even mitotic and Ki67 indices are quite low, caution and careful follow-up are therefore needed. Regarding meningeal SFTs in the previous literature, so far one case having both recurrence and metastasis to the soft tissues and lungs [22] and five cases having local recurrence [5, 29, 30] have been reported. Considering that the first recurrence was observed 7 years after resection of the primary tumor in the present case, it is conceivable that follow-up in some of the previous cases may not have been long enough to allow the conclusion that they did not recur.
References
Ahn JY, Shim JY, Yang WI, Kim TS (2001) Meningeal solitary fibrous tumor as an unusual cause of exophthalmos: case report and review of the literature. Neurosurgery 48:1362–1366
Barron J, Lownie SP, Lee DH, Hammond RR (2001) June 2001: 61 year old woman with confusion and obtundation. Brain Pathol 11:485–487
Bommer G, Altenähr E, Kühnau J, Jr., Klöppel G (1976) Ultrastructure of hemangiopericytoma associated with paraneoplastic hypoglycemia. Z Krebsforsch 85:231–241
Brunori A, Cerasoli S, Donati R, Giangaspero F, Chiappetta F (1999) Solitary fibrous tumor of the meninges: two new cases and review of the literature. Surg Neurol 51:636–640
Carneiro SS, Scheithauer BW, Nascimento AG, Hirose T, Davis DH (1996) Solitary fibrous tumor of the meninges: a lesion distinct from fibrous meningioma. A clinicopathologic and immunohistochemical study. Am J Clin Pathol 106:217–224
Cassarino DS, Auerbach A, Rushing EJ (2003) Widely invasive solitary fibrous tumor of the sphenoid sinus, cavernous sinus, and pituitary fossa. Ann Diagn Pathol 7:169–173
Castilla EA, Prayson RA, Stevens GH, Barnett GH (2002) Brain-invasive solitary fibrous tumor of the meninges: report of a case. Int J Surg Pathol 10:217–221
Challa VR, Kilpatrick SE, Ricci P, Wilson JA, Kelly DLJ (1998) Solitary fibrous tumor of the meninges. Clin Neuropathol 17:73–78
Cotterill AM, Holly JM, Davies SC, Coulson VJ, Price PA, Wass JA (1991) The insulin-like growth factors and their binding proteins in a case of non-islet-cell tumour-associated hypoglycaemia. J Endocrinol 131:303–311
Cummings TJ, Burchette JL, McLendon RE (2001) CD34 and dural fibroblasts: the relationship to solitary fibrous tumor and meningioma. Acta Neuropathol 102:349–354
de Leval L, Defraigne J-O, Hermans G, Dôme F, Boniver J, Herens C (2003) Malignant solitary fibrous tumor of the pleura: report of a case with cytogenetic analysis. Virchows Arch 442:388–392
Dotan ZA, Mor Y, Olchovsky D, Aviel-Ronen S, Engelberg S, Pinthus J, Shefi S, Leibovitch I, Ramon J (1999) Solitary fibrous tumor presenting as perirenal mass associated with hypoglycemia. J Urol 162:2087–2088
England DM, Hochholzer L, McCarthy MJ (1989) Localized benign and malignant fibrous tumors of the pleura. A clinicopathologic review of 223 cases. Am J Surg Pathol 13:640–658
Guillou L, Fletcher JA, Fletcher CDM, Mandahl N (2002) Extrapleural solitary fibrous tumor and hemangiopericytoma. In: CDM Fletcher, KK Unni, F Mertens (eds) World Health Organization Classification of Tumors Pathology and Genetics of Tumors of Soft Tissue and Bone. IARC Press, Lyon, pp 86–90
Hasegawa T, Matsuno Y, Shimoda T, Hasegawa F, Sano T, Hirohashi S (1999) Extrathoracic solitary fibrous tumors: their histological variability and potentially aggressive behavior. Hum Pathol 30:146–173
Kempson RL, Fletcher CDM, Evans HL, Hendrickson MR, Sibley RK (2001) Solitary fibrous tumor of the soft tissues. In: J Rosai (ed) Tumors of the soft tissue. A.F.I.P., Washington, D.C., pp 52–55
Klemperer P, Rabin CB (1931) Primary neoplasms of the pleura: a report of five cases. Arch Pathol 11:385–412
Mena H, Ribas JL, Pezeshkpour GH, Cowan DN, Parisi JE (1991) Hemangiopericytoma of the central nervous system: a review of 94 cases. Hum Pathol 22:84–91
Morimitsu Y, Nakajima M, Hisaoka M, Hashimoto H (2000) Extrapleural solitary fibrous tumor: clinicopathologic study of 17 cases and molecular analysis of the p53 pathway. APMIS 108:617–625
Nawashiro H (2000) Intracranial solitary fibrous tumor of the meninges. Hum Pathol 31:1536
Nawashiro H, Nagakawa S, Osada H, Katoh H, Ohnuki A, Tsuzuki N, Miyazawa T, Shima K, Ogata S, Aida S (2000) Solitary fibrous tumor of the meninges in the posterior cranial fossa: magnetic resonance imaging and histological correlation—case report. Neurol Med Chir 40:432–434
Ng HK, Choi PCL, Wong CW, To KF, Poon WS (2000) Metastatic solitary fibrous tumor of the meninges. Case report. J Neurosurg 93:490–493
Nikas DC, De Girolami U, Folkerth RD, Bello L, Zamani AA, Black PM (1999) Parasagittal solitary fibrous tumor of the meninges. Case report and review of the literature. Acta Neurochir 141:307–313
Perry A, Scheithauer BW, Nascimento AG (1997) The immunophenotypic spectrum of meningeal hemangiopericytoma: a comparison with fibrous meningioma and solitary fibrous tumor of meninges. Am J Surg Pathol 21:1354–1360
Prayson RA, McMahon JT, Barnett GH (1997) Solitary fibrous tumor of the meninges. Case report and review of the literature. J Neurosurg 86:1049–1052
Rodriguez L, Lopez J, Marin A, Cardozo D, Molina O, Cardozo J (2000) Solitary fibrous tumor of the meninges. Clin Neuropathol 19:45–48
Sanno N, Shimura T, Maeda S, Teramoto A (2001) A case of solitary fibrous tumor of the meninges. Brain Tumor Pathol 18:43–47
Slavik T, Bentley RC, Gray L, Fuchs HE, McLendon RE (1998) Solitary fibrous tumor of the meninges occurring after irradiation of a mixed germ cell tumor of the pineal gland. Clin Neuropathol 17:55–60
Suzuki SO, Fukui M, Nishio S, Iwaki T (2000) Clinicopathological features of solitary fibrous tumor of the meninges: an immunohistochemical reappraisal of cases previously diagnosed to be fibrous meningioma or hemangiopericytoma. Pathol Int 50:808–817
Tihan T, Viglione M, Rosenblum MK, Olivi A, Burger PC (2003) Solitary fibrous tumors in the central nervous system. A clinicopathologic review of 18 cases and comparison to meningeal hemangiopericytomas. Arch Pathol Lab Med 127:432–439
Vallat-Decouvelaere A-V, Dry SM, Fletcher CDM (1998) Atypical and malignant solitary fibrous tumors in extrathoratic locations. Evidence of their comparability to intra-thoracic tumors. Am J Surg Pathol 22:1501–1511
Vuorinen V, Sallinen P, Haapasalo H, Visakorpi T, Kallio M, Jaaskelainen J (1996) Outcome of 31 intracranial haemangiopericytomas: poor predictive value of cell proliferation indices. Acta Neurochir (Wien) 138:1399–1408
Witkin GB, Rosai J (1989) Solitary fibrous tumor of the mediastinum: a report of 14 cases. Am J Surg Pathol 13:547–557
Acknowledgements
We appreciate the valuable comments of Dr. Christopher D.M. Fletcher, Brigham and Women’s Hospital, Harvard Medical School. This work was supported in part by a grant from the Society for Promotion of Toxicological Pathology of Nagoya, Japan.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Ogawa, K., Tada, T., Takahashi, S. et al. Malignant solitary fibrous tumor of the meninges. Virchows Arch 444, 459–464 (2004). https://doi.org/10.1007/s00428-004-0991-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00428-004-0991-7