
Abstract
During exercise involving a small muscle mass, peak oxygen uptake is thought to be limited by peripheral factors, such as the degree of oxygen extraction from the blood and/or mitochondrial oxidative capacity. Previously, the maximal activity of the Krebs cycle enzyme oxoglutarate dehydrogenase has been shown to provide a quantitative measure of maximal oxidative metabolism, but it is not known whether the increase in this activity after a period of training reflects the elevation in peak oxygen consumption. Fourteen subjects performed one-legged knee extension exercise for 5–7 weeks, while the other leg remained untrained. Thereafter, the peak oxygen uptake by the quadriceps muscle was determined for both legs, and muscle biopsies were taken for assays of maximal enzyme activities (at 25°C). The peak oxygen uptake was 26% higher in the trained than in the untrained muscle (395 vs. 315 ml min−1 kg−1, respectively; P < 0.01). The maximal activities of the Krebs cycle enzymes in the trained and untrained muscle were as follows: citrate synthase, 22.4 vs. 18.2 μmol min−1 g−1 (23%, P < 0.05); oxoglutarate dehydrogenase, 1.88 vs. 1.54 μmol min−1 g−1 (22%, P < 0.05); and succinate dehydrogenase, 3.88 vs. 3.28 μmol min−1 g−1 (18%, P < 0.05). The difference between the trained and untrained muscles with respect to peak oxygen uptake (80 ml min−1 kg−1) corresponded to a flux through the Krebs cycle of 1.05 μmol min−1 g−1, and the corresponding difference in oxoglutarate dehydrogenase activity (at 38°C) was 0.83 μmol min−1 g−1. These parallel increases suggest that there is no excess mitochondrial capacity during maximal exercise with a small muscle mass.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Regular endurance training enhances peak oxygen uptake by muscles, as well as the maximal activities of oxidative enzymes [19, 36], which leads to improvements in physical performance and endurance. In whole-body exercise, maximal oxygen uptake is limited by the capacity of the heart or more precisely the cardiac output [6, 13], although it has been argued that cardiac output is not the only limiting factor in some situations [40]. In contrast, during exercise involving small muscle groups, peripheral factors, such as oxygen diffusion and mitochondrial metabolism, may limit peak oxygen utilisation by the contracting muscles [34, 35].
The capacity of mitochondrial metabolism is considered to be regulated by the flux through the Krebs cycle (see [27]). The first reaction in the cycle is catalysed by citrate synthase (CS) and is one of the regulatory steps; however, the enzyme activity is controlled by the availability of the substrate oxaloacetate. Because this concentration is far below the Km in muscle, variations in oxaloacetate can regulate the enzyme activity and also the flux through the Krebs cycle (see [27]). Another regulatory step in the Krebs cycle is the reaction catalysed by oxoglutarate dehydrogenase (OGDH), but for this enzyme, the maximal activity in various tissues of experimental animals was found to be similar to the maximal flux through the cycle in vivo [14, 31].
In a previous investigation, we found a correlation between maximal oxygen uptake by the quadriceps muscle during one-leg knee extension exercise and the activities of enzymes of the Krebs cycle. However, in agreement with data from experimental animals, only the maximal activity of oxoglutarate dehydrogenase could provide a quantitative assessment of the capacity for oxidative metabolism [9]. In the present study, the question was asked whether the increase in oxygen consumption and the associated elevated flux through the Krebs cycle following a period of training involve a similar enhancement in oxoglutarate dehydrogenase activity.
Intensity and volume play a role in the aerobic training adaptation in skeletal muscle [12, 17]. Thus, our subjects performed either very high intensive, high intensive or moderate intensive training using the one-legged knee extension exercise for 5–7 weeks. At the end of this training period, oxygen uptake by the quadriceps muscle was determined in both the trained and untrained legs during maximal exercise. Biopsies were taken from the quadriceps muscle for assays of oxoglutarate dehydrogenase activity. In addition, two other enzymes of the Krebs cycle, citrate synthase and succinate dehydrogenase (SDH), were assayed, and the fibre type composition and capillary density in both the trained and untrained legs were determined. Our hypothesis was that the training-induced elevation in the activity of oxoglutarate dehydrogenase would correspond quantitatively to the enhancement in peak oxygen uptake of a small limb muscle group during exercise.
Materials and methods
Subjects
The 14 participants, including 13 males and one female, had a mean age (±SE) of 25 ± 0.9 years, mean height of 185 ± 1.6 cm and mean weight of 85 ± 3.4 kg. They were all recreationally active but did not take part in exercise training on a regular basis. For nine of the male subjects, maximal oxygen uptake was determined and averaged 48 (range, 39–54) ml kg−1 min−1. The subjects were informed about the purpose of the study and possible risks prior to giving their oral consent. The experimental protocol was approved by the Copenhagen and Frederiksberg Ethics Committee in Denmark and performed in accordance with the principles outlined in the Declaration of Helsinki. Thirteen of the 14 subjects also participated in investigations described previously [16, 23, 26].
The training protocol
Each subject took part in 3–5 weekly training sessions for 5–7 weeks involving one-legged knee extension exercise using a modified Monark ergometer that permitted the exercise to be confined to the quadriceps muscle of the kicking leg [2]. Straps were placed around the hip joint and distal part of the upper leg to prevent the use of the trunk. Five of the subjects performed 1 h of training at approximately 70% of their pre-determined one-legged peak work rate five times a week for 5 weeks (submaximal aerobic training; total training volume, 6,290 kJ, ∼1,260 kJ per week). Four others trained three times each week for 6 weeks, with each 1-h session consisting of 40 1-min bouts of exercise at approximately 100% of maximal single leg oxygen uptake, separated by 30-s rest periods (aerobic intermittent training; total training volume, 2,500 kJ, ∼420 kJ per week). Another five participants trained on an average of four times per week for 7 weeks, with each 1-h session consisting of 15 1-min bouts of exercise at 150% of the maximal single leg oxygen uptake, separated by 3-min rest periods (anaerobic intermittent training; total training volume, 2,610 kJ, ∼370 kJ per week). In all three training regimes, the work rate was increased gradually throughout the training period, and the contralateral thigh did not perform any exercise during these same periods.
The experimental protocol
Two days after completion of the training protocol, the subjects arrived at the laboratory at 8 a.m. following an overnight fast. While the subject was resting in a supine position, catheters were inserted into the femoral artery of one leg (approximately 2 cm below the inguinal ligament) and femoral vein of both legs (4 cm distal to the inguinal ligament). Thermistors were placed into both venous catheters for measurements of blood flow.
After the catheters were positioned, the participants rested for approximately 30 min in the supine position before their blood and muscle samples were taken. Muscle biopsies were obtained from the vastus lateralis in both legs, employing the needle biopsy technique described by Bergström [5]. The subjects then moved to the knee extension chair to perform incremental exercise until maximal capacity was attained. Nine individuals began at 20 or 30 W for 3 min, followed by an elevation of 5 W every 30 s, until their maximal work rate (defined as the highest rate at which the kicking frequency could be kept above 50 kicks/min) was reached and maintained for at least 1 min. Thereafter, following a 15- to 30-min rest period, exercise with the contralateral leg was commenced. In five others, exercise started at 50 W for 4 min, followed by a 10-W increase every 2 min, and the trained and untrained legs were tested on separate days [23]. In this case, muscle biopsies were collected on the same day as the maximal test for that specific leg. The trained and untrained legs were tested in random order. The two incremental tests that were utilized are both common in the literature for the determination of peak leg oxygen uptake. Previous work has demonstrated that repeated intense knee extension exercise elicits the same quadriceps muscle peak oxygen uptake [4], indicating that performing exercise with the trained and untrained legs on the same day will not influence peak oxygen uptake.
Blood flow in the femoral vein was monitored repeatedly during exercise utilizing the thermodilution technique described by Andersen and Saltin [2]. To minimize mixing with blood from the lower leg during measurement of blood flow and sampling of blood, a cuff was placed just below the knee of the working leg and inflated to a pressure of 240 mmHg. Towards the end of the incremental exercise test, repeated blood samples were drawn simultaneously from the arterial and venous catheters for measurements of haemoglobin, oxygen saturation (Radiometer OSM-3 Hemoximeter, Copenhagen, Denmark) and oxygen tension (ABL 30, Radiometer, Copenhagen, Denmark). The oxygen contents of the arterial and venous blood were calculated from these measurements.
Measurements of muscle mass
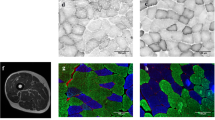
In four subjects, the masses of the trained and untrained quadriceps muscles were determined after the period of training using magnetic resonance images (MRI) from the patella to the anterior inferior iliac spine. Twenty-eight scans, each 3 mm thick, were taken 17.1 mm apart. To calculate the muscle volume, the area of each scan was multiplied by the distance between sections, and these results from all scans were added together to attain the total volume. In nine other cases, the volumes of the trained and untrained quadriceps muscles were estimated anthropometrically [22, 24] and corrected based on a comparison between MRI scanning and anthropometry with an expected difference of 0–9% [24], and in one subject, computerized tomography (model Prospeed VX, General Electric, Paris, France) was employed [33]. The volume was converted into mass assuming a specific density of 1.043 kg l−1 [42].
Enzyme activities
For measurements of enzyme activities, the muscle biopsies were frozen immediately in liquid nitrogen and stored at −80°C until being weighed and homogenized in ten volumes of ice-cooled extraction medium (50 mM Tris–HCl, 5 mM MgCl2 and 1 mM EDTA at pH 8.2) using a ground-glass homogenizer. The maximal activities of oxoglutarate dehydrogenase [7], citrate synthase [1] and succinate dehydrogenase [14] following incubation of the homogenate with succinate for 30 min at 30°C were assayed under optimal conditions as described previously. Measurements were performed in a Beckman DU 640 spectrophotometer at 25°C. The intra-assay coefficient of variation was 5.5%, 5.0% and 5.4% for oxoglutarate dehydrogenase, succinate dehydrogenase and citrate synthase, respectively. For comparison to the flux through the Krebs cycle during maximal exercise, enzyme activities at 38°C were calculated using the Arrhenius equation, assuming approximately a doubling of activity for every 10°C rise in temperature (see [9]). We estimate the muscle temperature to be ∼38°C, approximately 0.5°C higher than the venous temperature [18], which was recorded to be 37.5–38°C.
Histochemical analysis of the muscle
For the histochemical analyses, one portion of the muscle biopsy was mounted in an embedding medium (Tissue Tek® O.C.T. Compound) and frozen in isopentane cooled to its freezing point in liquid nitrogen. Serial 10-μm cross-sections were subsequently prepared in a cryostat at −20°C, preincubated at pH 4.3, 4.6 and 10.3 and then stained for myosin ATPase at pH 9.4 at 37°C [10, 11]. This approach allows the two major fibre types and two subgroups of fast fibres (with high myosin ATPase activity) to be distinguished from one another. These fibre types were originally designated as types I, IIA and IIB, but we chose to apply the new terminology of types I, IIA and IIX, since human skeletal muscle does not contain the fast type IIB fibres present in small animals (see [37]). Capillaries were visualized according to Qu et al. [29]. Fibre type composition was measured in 13 subjects and capillaries in the nine subjects from whom sufficient muscle tissue was available.
Statistical analyses
The values presented in the text are means ± standard errors of the mean (SE). A one-way repeated measures analysis of variance (ANOVA) was employed to compare the training-induced change in circulatory variables, muscle mass and enzyme activities in the three groups of subjects. When a significant main effect of training status (trained vs. untrained leg) was detected, Fisher’s least significant difference post hoc test was utilized to verify where the difference occurred. When no significant differences between training protocols were detected, Student’s t test for paired observations was employed for comparisons between the trained and untrained legs in the whole group of subjects. Correlations were evaluated utilizing Pearson’s linear correlation coefficient. A P value less than 0.05 was considered to be statistically significant.
Results
Peak oxygen uptake
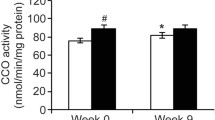
The three different types of exercise employed in the training, submaximal aerobic, intermittent high-intensity aerobic and anaerobic training, produced an average increase of 32% in peak leg oxygen uptake, ranging from 26% in the intermittent high-intensity aerobic exercise to 36% with submaximal aerobic exercise (P > 0.05). The mean peak oxygen uptake in the untrained and trained leg was 815 and 1,075 ml min−1, respectively. The muscle mass of the trained leg was 5.8% higher, and the corresponding elevation in peak oxygen uptake (normalized to the quadriceps muscle mass) was 26% (19–31% in the different groups), i.e. 315 and 395 ml min−1 kg−1 in the untrained and trained legs (Table 1, Fig. 1).

Peak oxygen uptake (a) and maximal activity of OGDH (b) in the trained (T) and untrained (UT) muscles in the three training regimes. § P < 0.01 for between-group difference in the ANOVA
Oxygen uptake by the muscle reflects the flux through the Krebs cycle, when only glucose or glucose derived from glycogen is the sole fuel source. This assumption is supported by the observation that leg respiratory exchange ratio is >1 during exhaustive one-leg knee extension exercise [3]. Complete oxidation of one molecule of glucose produces two molecules of acetyl-coenzyme A and consumes six molecules of oxygen. Consequently, the flux through the Krebs cycle is equal to one third of the oxygen uptake. At a muscle temperature of 38°C (see “Materials and methods” section), the volume of 1 mol of oxygen is 25.5 l, according to the General Law for gases. The difference of 80 ml min−1 kg−1 muscle mass in peak oxygen uptake by the trained and untrained legs (see above) therefore corresponds to an alteration of 1.05 μmol min−1 g−1 in the flux through the Krebs cycle.
Maximal enzyme activities
The maximal activities of the three enzymes of the Krebs cycle assayed here were increased similarly by an average of 18–23% in the trained muscle. The values for oxoglutarate dehydrogenase were 1.88 versus 1.54 μmol min−1 g−1, those for succinate dehydrogenase were 3.88 versus 3.28 μmol min−1 g−1, and those for citrate synthase were 22.4 versus 18.2 μmol min−1 g−1 for the trained versus untrained muscles, respectively (Table 2). The increase in oxoglutarate dehydrogenase activity, 0.34 μmol min−1 g−1 measured at 25°C, would correspond to an increase of 0.83 μmol min−1 g−1 in Krebs cycle flux at 38°C. The increases in succinate dehydrogenase and citrate synthase activities, 0.60 and 4.2 μmol min−1 g−1, respectively, correspond to increases in the Krebs cycle rate of 1.46 and 10.2 μmol min−1 g−1, respectively, at 38°C (Table 3).
The correlation between the training-induced increase (i.e. difference between the trained and untrained muscles) in maximal activity of oxoglutarate dehydrogenase and peak oxygen uptake is illustrated in Fig. 2. The correlation was analysed on 12 subjects (r = 0.60, P < 0.05). The values from two subjects deviated considerably from the others (68 and 0.78, and 51 and 1.04 for peak oxygen uptake and enzyme activity, respectively) and were therefore excluded from this analysis.

Correlation between the difference in peak oxygen uptake and maximal activity of OGDH in the trained (T) and untrained (UT) muscles. Analyses were performed in 12 subjects (see “Results” section)
In agreement with previous observations [9], peak oxygen uptake and the maximal activities of enzymes in the Krebs cycle were correlated here. Succinate dehydrogenase (r = 0.59, P < 0.05) and citrate synthase (r = 0.56, P < 0.05) were analysed for all 14 subjects, whereas oxoglutarate dehydrogenase was analysed separately for subjects who underwent the same training programme because of the between-group difference in the enzyme level (Table 2, Fig. 1), an observation which we have no obvious explanation for. The correlation coefficient varied between 0.38 (intermittent aerobic), 0.52 (intermittent anaerobic) and 0.61 (submaximal aerobic programme), with the number of subjects in each group being too small to justify a statistical analysis.
Muscle fibre composition
The training did not significantly alter the proportion of type I and II fibres in the vastus lateralis muscle, with type I fibres constituting 49 ± 3.8% and 53 ± 3.6% of the total in the untrained and trained legs, respectively. However, the proportion of type IIA fibres was higher (36 ± 2.4% versus 28 ± 1.8%, P < 0.05), while that of type IIX fibres was lower (11 ± 2.1% versus 23 ± 2.8%, P < 0.05) in the trained leg.
There were weak correlations between the maximal activities of oxoglutarate dehydrogenase and the percentages of type I fibres in both the untrained (r = 0.47, P < 0.1) and trained muscles (r = 0.37, P < 0.1), as well as for succinate dehydrogenase activity and the percentage of type I fibres in the trained muscle (r = 0.46, P < 0.1) but not in the untrained muscle (r = 0.14, P > 0.05), whereas no correlations between the maximal activities of citrate synthase and percentage of type I fibres were detected (r = 0.1, P > 0.05, in the untrained muscle and r = 0.28, P > 0.05, in the trained muscle).
Muscle capillaries and selected blood and vascular parameters
In the nine subjects from whom sufficient muscle tissue for assessment of capillaries was available, the capillary density was 28% higher in the trained leg (566 ± 68 versus 441 ± 44 capillaries mm−2, P < 0.05). The difference in peak oxygen uptake between the legs in these nine subjects (77 ml kg−1 min−1) was similar to the corresponding difference for the entire group (80 ml kg−1 min−1) as was the relative difference (23% versus 26%, respectively), as well as the difference in peak blood flow (27% versus 30%). Oxygen extraction (73% versus 74.5%, respectively) and the arterio-venous oxygen difference (144 ± 3.6 versus 149 ± 2.3 ml l−1) were virtually the same across the untrained and trained legs.
Additional evidence for the lack of any effect on oxygen extraction was provided by the values for femoral venous pO2 and saturation, which were 22.2 ± 2.7 (untrained) and 21.8 ± 1.9 (trained) mmHg, and 36.9 ± 2.8% (untrained) and 35.3 ± 3.3% (trained), respectively. With almost identical relative differences in capillary density and peak blood flow per unit muscle, the estimated mean transit times (see [34]) during peak effort were essentially the same in both legs. Measurements on four subjects indicated that the mean arterial blood pressure was the same when the participants exercised maximally with either leg, trained or untrained, suggesting that the differences in blood flow and conductance observed were due to enhanced vasodilation.
Discussion
The major novel finding in the present study was that the training-induced elevation in the maximal flux through the Krebs cycle was quite similar when calculated on the basis of the activity of oxoglutarate dehydrogenase or oxygen consumption by the maximally exercising muscle. Furthermore, the relative increase in the peak oxygen uptake by the quadriceps muscle (26%) was similar to the enhancement in the activities of the Krebs cycle enzymes (18–23%). Parallel increases in the activities of citrate synthase and succinate dehydrogenase in the skeletal muscle of experimental animals following prolonged periods of training have been reported previously [20]. The finding that also oxoglutarate dehydrogenase activity was increased to a similar extent differs from the study on rat muscle: after 3 months of endurance training, oxoglutarate dehydrogenase activity was elevated to a lesser extent (50%) than the activities of citrate synthase and succinate dehydrogenase (100%) [20]. However, no comparison to peak oxygen uptake was performed in this investigation.
Consistent with our hypothesis, the difference between oxoglutarate dehydrogenase activity in the trained and untrained muscles (0.83 μmol min−1 g−1) was quite similar to the elevation in the flux through the Krebs cycle calculated on the basis of oxygen uptake (1.05 μmol min−1 g−1). The enhancement in succinate dehydrogenase activity (1.46 μmol min−1 g−1) was 39% higher, and that in citrate synthase (10.2 μmol min−1 g−1), tenfold higher (Table 3). These findings confirm our previous conclusion that only the activity of oxoglutarate dehydrogenase provides a reliable quantitative measure of the maximal flux through the Krebs cycle [9]. Excess activity of citrate synthase (15 times) and succinate dehydrogenase (three times) was also demonstrated in isolated mitochondria from the human quadriceps muscle in relation to the rate of oxygen uptake by the same muscle during maximal exercise [30]. Furthermore, the activity of a respiratory chain enzyme (cytochrome aa3) was also in considerable excess relative to maximal oxygen uptake [30].
Peak oxygen uptake in the untrained and trained muscles was 315 and 395 ml min−1 kg−1, respectively, corresponding to Krebs cycle fluxes of 4.11 and 5.16 μmol min−1 g−1. These values are quite similar to the corresponding maximal activities of oxoglutarate dehydrogenase at 38°C in the untrained (3.74) and trained muscles (4.57 μmol min−1 g−1). These parallel elevations in peak oxygen uptake and the activities of Krebs cycle enzymes after a period of training indicate that the maximal mitochondrial oxidation equals the peak oxygen uptake and may limit oxygen uptake during exercise involving a small muscle mass. The role of mitochondrial metabolism in regulating peak oxygen uptake can also be examined by increasing the oxygen supply to the muscle, which should enhance peak oxygen uptake provided that the enzyme activities do not limit the maximal flux of the Krebs cycle. In three studies, the effect of hyperoxia on peak oxygen uptake during one-leg knee extension exercise has been investigated. Richardson and colleagues [32] found that the peak oxygen uptake by the quadriceps muscle increased by 17% and concluded that this uptake is not limited by mitochondrial metabolism. In contrast, no enhancement in peak oxygen uptake by the quadriceps muscle during hyperoxia was detected in two other studies [26, 28]. These latter reports indicate that during exercise involving a small muscle mass mitochondrial metabolism is maximal, i.e. that enhancement of peak oxygen uptake during such exercise requires more mitochondrial oxidative capacity. There is no obvious explanation for the divergent effect of hyperoxia in the former versus the latter two studies. However, when comparing the effect on trained subjects that was studied both by Richardson et al. [32] and Mourtzakis et al. [26], work rate and blood flow at maximal exercise look very similar in the two studies. This enables a comparison also between peak oxygen uptake, which in fact was lower in the normoxic condition in the former study (1.24 vs. 1.34 l min−1), mainly due to a 6% lower arterial content, and a similarly lower arterial–venous difference. The higher peak oxygen uptake during hyperoxia in the study by Richardson et al. [32] can therefore to some extent be a consequence of lower oxygen uptake in the normoxic condition.
Regular exercise is known to enhance both the maximal oxygen uptake and levels of oxidative enzymes in the exercising muscles [8, 19, 36, 38]. When whole-body exercise is considered, the effects of endurance training on central and peripheral parameters differ to a large extent from what is observed in small limb muscle exercise. For example, maximal oxygen uptake increased by 19% while mitochondrial enzymes (succinate dehydrogenase and cytochrome oxidase) increased by 32–35% following 8 weeks of endurance training (similar training period as in the present study) [19]. On the other hand, similar increases in mitochondrial content in the vastus lateralis and maximal power output during cycling exercise after 6 weeks of endurance training have been reported [21]. In addition, the calculated oxygen uptake required to achieve the observed increase in maximal power output during 30-min cycling was the same as the observed increase in whole-body oxygen uptake per kilogramme body mass [21]. However, it should be emphasized that muscle performance is not equivalent to maximal oxygen uptake. Furthermore, whole-body maximal oxygen uptake is predominantly limited by cardiac output, whereas during exercise with a small muscle group, peripheral factors become most critical, and the oxygen uptake is primarily limited by peripheral factors [15, 25, 34].
Despite the considerably lower weekly training volume in the intermittent high-intensity training groups (370 and 420 kJ vs. 1,260 kJ during submaximal aerobic training), no significant differences in training response were detected. The average increase in peak oxygen uptake varied between 19% and 31%, and the increase in maximal activity of oxoglutarate dehydrogenase, between 14% and 37% for the three training regimes. Although the number of subjects participating in the different training programmes is small, the findings agree with previous reports showing similar muscular adaptations, including increases in muscle oxidative capacity and expression of mitochondrial markers, as well as enhanced maximal oxygen uptake and performance after high-intensity interval and submaximal endurance training [12, 17, 39, 41].
Although data are available only on a limited number of subjects, the parallel elevations in capillary density and peak blood flow in the trained leg highlight the significance of an enlarged microcirculatory bed for oxygen delivery in connection with exercise involving a small muscle group. It is also noteworthy that, despite the enlarged capillary surface area and elevation in mitochondrial respiratory capacity, the degree of oxygen extraction was unaffected, i.e. without this training-induced enlargement in capillary density, oxygen extraction could actually have been reduced.
In conclusion, the activities of the three Krebs cycle enzymes citrate synthase, succinate dehydrogenase and oxoglutarate dehydrogenase were elevated to similar extents (18–23%) following a period of knee extension exercise. The increases in peak oxygen uptake and flux through the Krebs cycle were paralleled by the enhancement in the maximal activity of the regulatory enzyme oxoglutarate dehydrogenase, suggesting a lack of any excess mitochondrial oxidative capacity during exercise involving a small muscle mass.
References
Alp PR, Newsholme EA, Zammit VA (1976) Activities of citrate synthase and NAD+-linked and NADP+-linked isocitrate dehydrogenase in muscle from vertebrates and invertebrates. Biochem J 154:689–700
Andersen P, Saltin B (1985) Maximal perfusion of skeletal muscle in man. J Physiol 366:233–249
Bangsbo J, Graham T, Johansen L, Strange S, Christensen C, Saltin B (1992) Elevated muscle acidity and energy production during exhaustive exercise in humans. Am J Physiol Regul Integr Comp Physiol 263:R891–R899
Bangsbo J, Krustrup P, González-Alonso J, Saltin B (2001) ATP production and efficiency of human skeletal muscle during intense exercise: effect of previous exercise. Am J Physiol Endocrinol Metab 280:E956–E964
Bergström J (1962) Muscle electrolytes in man. Scand J Clin Lab Invest 14 (suppl 68):1–110
Bergh U, Ekblom B, Åstrand PO (2000) Maximal oxygen uptake“classical” versus“contemporary” viewpoints. Med Sci Sports Exerc 32:85–88
Blomstrand E, Challiss RAJ, Cooney GJ, Newsholme EA (1983) Maximal activities of hexokinase, 6-phosphofructokinase, oxoglutarate dehydrogenase and carnitine palmitoyltransferase in rat and avian muscle. Biosci Rep 3:1149–1153
Blomstrand E, Ekblom B, Newsholme EA (1986) Maximum activities of key glycolytic and oxidative enzymes in human muscle from differently trained individuals. J Physiol 381:111–118
Blomstrand E, Rådegran G, Saltin B (1997) Maximum rate of oxygen uptake by human skeletal muscle in relation to maximal activities of enzymes in the Krebs cycle. J Physiol 501:455–460
Brooke MH, Kaiser KK (1969) Some comments on the histochemical characterization of muscle adenosine triphosphatase. J Histochem Cytochem 17:431–432
Brooke MH, Kaiser KK (1970) Three “myosine adenosine-triphosphatase” systems: the nature of their pH lability and sulfhydryl dependence. J Histochem Cytochem 18:670–672
Burgomaster KA, Howarth KR, Phillips SM, Rakobowchuk M, Macdonald MJ, McGee SL, Gibala MJ (2008) Similar metabolic adaptations during exercise after low volume sprint interval and traditional endurance training in humans. J Physiol 586:151–160
Calbet JA, Jensen-Urstad M, van Hall G, Holmberg HC, Rosdahl H, Saltin B (2004) Maximal muscular vascular conductances during whole body upright exercise in humans. J Physiol 558:319–331
Cooney GJ, Taegtmeyer H, Newsholme EA (1981) Tricarboxylic acid cycle flux and enzyme activities in the isolated working rat heart. Biochem J 200:701–703
Di Prampero PE (1985) Metabolic and circulatory limitations to VO2max at the whole animal level. J Exp Biol 115:319–331
Frandsen U, Höffner L, Betak A, Saltin B, Bangsbo J, Hellsten Y (2000) Endurance training does not alter the level of neuronal nitric oxide synthase in human skeletal muscle. J Appl Physiol 89:1033–1038
Gibala KJ, Little JP, van Essen M, Wilkin GP, Burgomaster KA, Safdar A, Raha S, Tarnopolsky MA (2006) Short-term sprint interval versus traditional endurance training: similar initial adaptations in human skeletal muscle and exercise performance. J Physiol 575:901–911
González-Alonso J, Quistorff B, Krustrup P, Bangsbo J, Saltin B (2000) Heat production in human skeletal muscle at the onset of intense dynamic exercise. J Physiol 524:603–615
Henriksson J, Reitman JS (1977) Time course of changes in human skeletal muscle succinate dehydrogenase and cytochrome oxidase activities and maximal oxygen uptake with physical activity and inactivity. Acta Physiol Scand 99:91–97
Holloszy JO, Oscai LB, Don IJ, Molé PA (1970) Mitochondrial citric acid cycle and related enzymes: adaptive response to exercise. Biochem Biophys Res Commun 30:1368–1373
Hoppeler H, Howald H, Conley K, Lindstedt SL, Claassen H, Vock P, Weibel ER (1985) Endurance training in humans: aerobic capacity and structure of skeletal muscle. J Appl Physiol 59:320–327
Jones PRM, Pearson J (1969) Anthropometric determination of leg fat and muscle plus bone volumes in young male and female adults (abstract). J Physiol 204:36P
Krustrup P, Hellsten Y, Bangsbo J (2004) Intense interval training enhances human skeletal muscle oxygen uptake in the initial phase of dynamic exercise at high but not at low intensities. J Physiol 559:335–345
Krustrup P, Söderlund K, Mohr M, González-Alonso J, Bangsbo J (2004) Recruitment of fibre types and quadriceps muscle portions during repeated, intense knee-extensor exercise in humans. Pflügers Arch Eur J Physiol 449:56–65
Mortensen SP, Dawson EA, Yoshiga CC, Dalsgaard MK, Damsgaard R, Secher NH, González-Alonso J (2005) Limitations to systemic and locomotor limb muscle oxygen delivery and uptake during maximal exercise in humans. J Physiol 566:273–285
Mourtzakis M, Gonzáles-Alonso J, Graham TE, Saltin B (2004) Hemodynamics and O2 uptake during maximal knee extensor exercise in untrained and trained human quadriceps muscle: effects of hyperoxia. J Appl Physiol 97:1796–1802
Newsholme EA, Leech TR (2010) Functional biochemistry in health and disease. Wiley, Chichester
Pedersen PK, Kiens B, Saltin B (1997) Hyperoxia does not increase peak muscle oxygen uptake in small muscle group exercise. Acta Physiol Scand 166:309–318
Qu Z, Andersen JL, Zhou S (1997) Visualisation of capillaries in human skeletal muscle. Histochem Cell Biol 107:169–174
Rasmussen UF, Rasmussen HN, Krustrup P, Quistorff B, Saltin B, Bangsbo J (2001) Aerobic metabolism of human quadriceps muscle: in vivo data parallel measurements on isolated mitochondria. Am J Physiol Endocrinol Metab 280:E301–E307
Read G, Crabtree B, Smith GH (1977) The activities of 2-oxoglutarate dehydrogenase and pyruvate dehydrogenase in hearts and mammary glands from ruminants and non-ruminants. Biochem J 164:349–355
Richardson RS, Grassi B, Gavin TP, Haseler J, Tagore K, Roca J, Wagner PD (1999) Evidence of O2 supply-dependent VO2max in the exercise-trained human quadriceps. J Appl Physiol 86:1048–1053
Rådegran G, Blomstrand E, Saltin B (1999) Peak muscle perfusion and oxygen uptake in humans: importance of precise estimates of muscle mass. J Appl Physiol 87:2375–2380
Saltin B (1985) Malleability of the system in overcoming limitations: functional elements. J Exp Biol 115:345–354
Saltin B, Calbet JA (2006) Point: in health and in a normoxic environment, VO2max is limited primarily by cardiac output and locomotor muscle blood flow. J Appl Physiol 100:744–745
Saltin B, Gollnick P (1983) Skeletal muscle adaptability: significance for metabolism and performance. In: Handbook of physiology: skeletal muscle, sect. 10. Am. Physiol. Soc., Bethesda, pp. 555–631
Schiaffino S, Reggiani C (1996) Molecular diversity of myofibrillar proteins: gene regulation and functional significance. Physiol Rev 76:371–423
Simoneau J-A, Lortie G, Boulay MR, Marcotte M, Thibault M-C, Bouchard C (1987) Effects of two high-intensity intermittent training programs interspaced by detraining on human skeletal muscle and performance. Eur J Appl Physiol 56:516–521
Tabata I, Nishimura K, Kouzaki M, Hirai Y, Ogita F, Miyachi M, Yamamoto K (1996) Effect of moderate-intensity endurance and high-intensity intermittent training on anaerobic capacity and VO2max. Med Sci Sports Exerc 28:1327–1330
Wagner PD (2006) Counterpoint: in health and in a normoxic environment, Vo2max is not limited primarily by cardiac output and locomotor muscle blood flow. J Appl Physiol 100:745–747
Wang L, Psilander N, Tonkonogi M, Ding S, Sahlin K (2009) Similar expression of oxidative genes after interval and continuous exercise. Med Sci Sports Exerc 41:2136–2144
Von Döbeln W (1956) Human standard and maximal metabolic rate in relation to fat-free body mass. Acta Physiol Scand 37(suppl 126):1–79
Acknowledgements
The study was supported by grants from the Danish National Research Foundation and the Swedish National Centre for Research in Sports. The authors have no conflicts of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Blomstrand, E., Krustrup, P., Søndergaard, H. et al. Exercise training induces similar elevations in the activity of oxoglutarate dehydrogenase and peak oxygen uptake in the human quadriceps muscle. Pflugers Arch - Eur J Physiol 462, 257–265 (2011). https://doi.org/10.1007/s00424-011-0978-6
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00424-011-0978-6