
Abstract
Purpose
Adrenal venous sampling is generally considered the gold standard to identify unilateral hormone production in cases of primary hyperaldosteronism. The aim of this study is to evaluate whether the iodine-131-6-β-iodomethyl-19-norcholesterol (NP-59) test may represent an alternative in selected cases.
Methods
Patients submitted to laparoscopic adrenalectomy for suspected primary hyperaldosteronism (n = 27) were retrospectively reviewed. When nuclear medicine tests were preoperatively performed, their results were compared with the histopathologic findings and clinical improvement.
Results
Nuclear medicine tests were realized in 13 patients. In 11 (84.6%), a planar anterior and posterior NP-59 scintigraphy was performed and a SPECT/TC in two (15.4%). Scintigraphy indicated a preoperative lateralization in 12 out of 13 patients (92.3%). When the value of NP-59 tests was based on pathologic results, it showed a sensitivity of 90.9% and a positive predictive value of 83.3%. When the nuclear medicine test’s performance was based on postoperative blood pressure control, both sensitivity and positive predictive value were 91.6%.
Conclusions
Nuclear medicine tests represent a useful tool in the preoperative localisation of primary hyperaldosteronism with a high sensitivity and positive predictive value. In patients with contraindications to adrenal venous sampling like contrast allergies, or when it is inconclusive, scintigraphy can represent a useful and non-invasive alternative.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The prevalence of primary hyperaldosteronism (PA) among hypertensive patients is reported to range from 1 to 20% [1]. In 30–40% of PA, the hormone hyperproduction is attributable to a unilateral aldosterone-producing adenoma (APA). The other frequent cause is idiopathic bilateral adrenal hyperplasia (IAH), while familiar syndromes, adrenocortical carcinoma and unilateral adrenal hyperplasia (UAH) represent other less frequent aetiologies [2, 3]. Laparoscopic adrenalectomy is the treatment of choice when the increased production of aldosterone shows a unilateral pattern, as in APA, carcinomas or selected nodular UAH, while for IAH the treatment is pharmacologic [4, 5]. Thus, once the PA has been confirmed through biochemical tests, the subtype of the PA needs to be identified. Computed tomography (CT) and/or magnetic resonance imaging (MRI) are performed to exclude large masses that may represent adrenocortical carcinomas, but they are not a reliable way to diagnose APA for several reasons [6]. Small lesions represent the most frequent form of unilateral PA, and sometimes they are not detected by radiologic test; a nodule in older patients could just be an incidentaloma and not the cause of the PA, and in addition to this, bilateral nodularity does not help to differentiate an APA from IAH. For this reason, CT or MRI findings alone are not sufficient to differentiate APA from IAH [7–9]. Therefore, a differentiation between a unilateral adrenal hormone-producing lesion, suggesting of APA or UAH and a bilateral one indicative of an IAH, is required. Adrenal venous sampling (AVS) represents the gold standard to identify unilateral hormone production, as long as surgical treatment is practicable and desired by the patients [10, 11]. However, sometimes is not possible to practise AVS, or its results can be non-conclusive. In these scenarios, NM tests such as iodine-131-6-β-iodomethyl-19-norcholesterol (NP-59) scintigraphy could represent valuable diagnostic tools.
The aim of this study is to analyse the sensitivity and positive predictive value (PPV) of nuclear medicine tests when performed in patients suspected of unilateral PA.
Material and methods
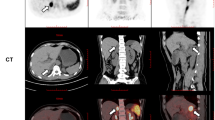
We retrospectively reviewed 27 patients submitted to laparoscopic adrenalectomy for suspected APA in the University Hospital of La Princesa from 1999 to 2014. A preoperative diagnostic of PA was performed by aldosterone-to-renin ratio (ARR) and suppression saline test when needed. The initial preoperative study of lesions was realized by radiologic tests such as CT and/or MRI. Our centre has recently incorporated AVS (from 2011) as a routine preoperative test. Before its introduction, nuclear medicine (NM) tests such as NP-59 planar scintigraphy or single-photon emission computed tomography (SPECT/CT) (Fig. 1) were performed as localisation preoperative tests, in cases of equivocal findings on cross-sectional imagining, especially in patients younger than 50 years old or with small nodules.

NP-59 SPECT/CT showing a left adrenal hypercapting nodule in coronal (a) and axial (b) plane
Three days before and five after the NP-59 intravenous injection, patients took 6 mg of oral dexamethasone daily, in order to suppress normal adrenal uptake of cholesterol. Each patient received an intravenous injection of 37 MBq (1 mCi) of NP-59. Both anterior and posterior planar images were taken 3 and 5 days after the tracer injection. The planar and SPECT/CT images of the lumbar region were taken using a dual-head SPECT/CT gamma camera.
A radiologist who was experienced in adrenal imaging and did not know the results of the other tests interpreted each radiologic test. A nuclear medicine physician, independently, analysed the NP-59 planar scintigraphy and SPECT/CT.
All patients underwent laparoscopic adrenalectomy via a lateral transperitoneal approach by an experienced surgeon. All patients had been clearly informed of the risks and benefits of a wrong preoperative localisation as well as risks related to the surgical procedure. An experienced pathologist evaluated each surgical specimen.
The control of blood pressure (BP) levels or a decrease in the number of anti-hypertensive drugs administered to the patients after the surgery was defined as clinical postoperative improvement. The BP was considered controlled if it decreased to 140/90 mmHg, with the absence of hypertensive crises or headache episodes, even if the patient was still under antihypertensive drugs. The BP was considered normalized when antihypertensive drugs were not required during the first year after adrenalectomy and BP maintained a steady level less than 140/90 mmHg.
The main variable of the study is the ability of the NM test to identify lateralization, which was confirmed in accordance with the histopathologic results and clinical improvement based on BP control. Data are expressed as a percentage or median and interquartile range. The sensitivity was defined as true positive over true positive plus false negative TP/(TP+FN) and the positive predictive value (PPV) as true positive over true positive plus false positive TP/(TP+FP). The comparison of data was realized with the exact Fisher test and the Mann Whitney U test. The differences were considered significant at p < 0.05. Statistical analysis was performed using SPSS® version 21 (SPSS, Chicago, IL, USA).
Results
The study included 27 patients. Median age was 53.6 ± 11.8 years; 15 patients were female (56%) and 12 male (44%). All of the patients suffered with hypertension, 15 (55%) with preoperative hypopotassemia. In these ones, median potassium level was 2.75 ± 0.1 mg/dL, 9 (25.9%) had presented previous episodes of headache and 7 (25.9%) hypertensive crises (Table 1).
All the patients had undergone a radiologic test, either CT or MRI, prior to surgery. AVS was performed in the last four cases (14.8%) of our series, NM tests in 13 (48.1%). Of these, 11 (84.6%) were represented by planar NP-59 scintigraphy and two (15.4%) by SPECT/CT. NM tests show preoperative lateralization in 12 out of 13 patients (92.3%). Pathologic reports described 23 adenomas (85.1%) and 4 hyperplasia (14.9%), even though 3 of them corresponded to a nodular hyperplasia (NH) (Table 2).
The mean length of the postoperative stay of patients was 3.73 ± 0.27 days. Complications were observed in 2 out of 27 patients (7.4%), all of them inferior to grade IIIa of the Clavien-Dindo classification. One patient presented a mild pancreatitis after a left adrenalectomy which settled with conservative management, the other a wound infection, which required oral antibiotics (Clavien-Dindo grades I and II, respectively)
Median follow-up was 48 months (40–60); two patients attended follow-up in other hospitals; therefore, we lost their data. We observed a control of BP in 23 out of 27 patients (85.1%); 18 (66.6%) showed a decrease in the number of anti-hypertensive drugs administered and 6 (22.2%) normalized BP levels in the absence of antihypertensive drugs. Patients with a preoperative MN test done had a median age of 49 years, the median pathologic size was 1.7 cm, 11 (84.6%) had an adenoma and 12 (91.3%) presented a postoperative BP control.
When the value of NP-59 imaging was based on pathologic results it produced 10 true positive TP, 2 false positive FP and 1 false negative FN. On balance, it showed a sensitivity of 90.9% and a PPV of 83.3% (Table 3). CT presented a sensitivity and a PPV of 69.1% while MRI showed a PPV of 90% but the sensitivity could not be calculated due to the absence of FN.
When the value of NP-59 imaging was based on clinical improvement, it showed a sensitivity of 91.7% and a PPV of 91.7% (Table 4). CT presented a sensitivity of 80.9%; MRI showed a PPV of 80.0%.
Discussion
PA represents the most frequent and curable cause of secondary hypertension, when it is detected before causing irreversible damage to the cardiovascular system [12]. Surgery is a potentially curative treatment in unilateral disease, and in patients with APA or less frequently in carcinomas or selected unilateral nodular IAH [10, 13]. In cases of bilateral IAH, antihypertensive treatment is usually adequate for BP control. Therefore, establishing a lateralization is a critical step towards deciding the correct management of PA. AVS represents the gold standard for this purpose. Nevertheless, it is an expensive and invasive test and can occasionally be unavailable, inconclusive or contraindicated in patients with contrast allergy or chronic renal failure. In this scenario, the NM test can be a useful tool to explore the nature of PA.
Asian experience and some other isolated reports showed that dexamethasone-suppression adrenocortical scintigraphy based on NP-59 can identify unilateral uptake of radio-cholesterol and so distinguish a potential APA from an IAH [14, 15]. On the other hand, there has been variable accuracy in different series, ranging from 47 to 94% [16–23]. These limitations can be overcome by SPECT with a better image resolution and the integrated SPECT/CT systems, fusing SPECT technology with CT images, and so providing both functional and anatomic information [17, 18, 24]. It is not only a non-invasive test, but also avoids the use of iodine intravenous contrast agents, which benefits patients with allergies or chronic kidney diseases.
Our series highlights the high sensitivity and PPV of NP-59 NM tests. Only short series based on retrospective studies have been described so far in the literature. Yen et al. [17] described a sensitivity of 81.8% for NP-59 SPECT/CT and a PPV of 85.6% when the precision of NM tests was based on pathologic results. Nevertheless, values of sensitivity and PPV grow up to 100% when the analysis was based on clinical response. In our series, NP-59 NM tests were used in patients with equivocal findings on cross-sectional imaging, especially in small lesion and in patients younger than 50 years old. They represented an important decision-making tool, showing a sensibility and specificity of 91.7% based on clinical improvement.
However, dexamethasone-suppression scintigraphy shows some practical limitations. It is a test that requires additional effort, both before and after the test. The duration of dexamethasone suppression must be sufficient, and patients have to suspend antihypertensive medication that may affect the 131I tracer before scanning. In addition to this, the NM test requires multiple imaging sessions after the tracer injection, normally on days three and five.
Recent interest has been focused on the potential utility of PET/CT using 11C-metomidate as tracer [25, 26]. It is a potent inhibitor of aldosterone synthase, which binds to the adrenal cortex receptor with high affinity. Paulsen et al. [27] showed a ratio of tumour maximum standarized uptake values (SUVmax) to normal background adrenal gland greater than 1.25 afforded optimal sensitivity (76%) and specificity (87%). Moreover, specificity increased to 100% in patients with a SUVmax ratio >1.25 and absolute tumour SUVmax >17. In addition to this, Hahner et al. [28] recently evaluated another etomidate derivate, 123iodometomidate, in adrenal lesions. The big limitation 11C-metomidate is its short half-life (20 min), restricting its usage to PET centres with access to an on-site cyclotron. 123Iodometomidate, presents the advantage of a longer half-life than 11C-metomidate, with a shorter duration of imaging procedure than NP-59 test. It showed a sensitivity of 89% and a specificity of 85% for the characterization of adrenal masses ≥2 cm, but its accuracy with APA has not been investigated yet. There is a lack of evidence in the literature about this argument, since most studies focus on the importance of AVS and do not compare either SPECT/CT or PET/CT with AVS.
Another important aspect to consider is that, in our series, patients with a postoperative pathologic report of UAH showed clinical outcome comparable to APA. This finding suggests that UAH could represent an adequate surgical candidate. For this reason, it is likely that the accuracy of the preoperative functional test should be based not only on pathologic reports but also on clinical outcomes.
However, our study had some limitations; it was retrospective and was based on two different types of NM tests. Furthermore, it did not compare the lateralization accuracy of AVS and the NM test. In addition to this, patients with negative NM tests or with a good response to medical treatment were not included in the analysis. Future prospective studies with larger samples are needed. Using PASS® version 14 (PASS, NCSS, LLC. Kaysville, UT, USA) we estimated that 132 subjects with disease are needed to achieve 90% power to detect a change in sensitivity from 90% (H0) to 80% (H1) and 100% power to detect a change in specificity from 90% (H0) to 80% (H1) using a two-sided binomial test and assuming a significance level of 0.05.
Conclusion
Our series demonstrate that NP-59 tests represent a useful tool in the preoperative localisation of PA with a high sensitivity and PPV. NM tests are useful and non-invasive tool, in patients with contraindications to AVS, or when the test is inconclusive. Nevertheless, prospective studies with larger samples comparing AVS with SPECT/CT are needed.
Abbreviations
- NP-59:
-
Iodine-131-6-β-iodomethyl-19-norcholesterol
- PA:
-
Primary hyperaldosteronism
- IAH:
-
Idiopathic bilateral adrenal hyperplasia
- UAH:
-
Unilateral adrenal hyperplasia
- CT:
-
Computed tomography
- MRI:
-
Magnetic resonance imaging
- AVS:
-
Adrenal Venous Sampling
- PPV:
-
Positive predictive value
- ARR:
-
Aldosterone-to-renin ratio
- NM:
-
Nuclear medicine
- SPECT-CT:
-
Single-photon emission computed tomography
- BP:
-
Blood pressure
- TP:
-
True positive
- FN:
-
False negative
- FP:
-
False positive
- NH:
-
Nodular hyperplasia
- SUVmax :
-
Maximum standarized uptake values
References
Harvey AM (2014) Hyperaldosteronism: diagnosis, lateralization, and treatment. Surg Clin North Am 94:643–656
Mulatero P, Stowasser M, Loh KC, Fardella CE, Gordon RD, Mosso L et al (2004) Increased diagnosis of primary aldosteronism, including surgically correctable forms, in centers from five continents. J Clin Endocrinol Metab 89:1045–1050
Carey RM (2012) Primary aldosteronism. J Surg Oncol 106:575–579
Economopoulos KP, Phitayakorn R, Lubitz CC, Sadow PM, Parangi S, Stephen AE et al (2016) Should specific patient clinical characteristics discourage adrenal surgeons from performing laparoscopic transperitoneal adrenalectomy? Surgery 159:240–249
McKenzie TJ, Lillegard JB, Young WF Jr, Thompson GB (2009) Aldosteronomas—state of the art. Surg Clin North Am 89:1241–1253
Funder JW, Carey RM, Fardella C, Gomez-Sanchez CE, Mantero F, Stowasser M et al (2008) Case detection, diagnosis, and treatment of patients with primary aldosteronism: an endocrine society clinical practice guideline. J Clin Endocrinol Metab 93:3266–3281
White ML, Gauger PG, Doherty GM, Cho KJ, Thompson NW, Hammer GD et al (2008) The role of radiologic studies in the evaluation and management of primary hyperaldosteronism. Surgery 144:926–933 discussion 33
Rossi GP, Sacchetto A, Chiesura-Corona M, De Toni R, Gallina M, Feltrin GP et al (2001) Identification of the etiology of primary aldosteronism with adrenal vein sampling in patients with equivocal computed tomography and magnetic resonance findings: results in 104 consecutive cases. J Clin Endocrinol Metab 86:1083–1090
Hammarstedt L, Muth A, Wangberg B, Bjorneld L, Sigurjonsdottir HA, Gotherstrom G et al (2010) Adrenal lesion frequency: a prospective, cross-sectional CT study in a defined region, including systematic re-evaluation. Acta Radiol 51:1149–1156
Rossi GP, Auchus RJ, Brown M, Lenders JW, Naruse M, Plouin PF et al (2014) An expert consensus statement on use of adrenal vein sampling for the subtyping of primary aldosteronism. Hypertension 63:151–160
Aronova A, Iii TJ, Zarnegar R (2014) Management of hypertension in primary aldosteronism. World J Cardiol 6:227–233
Abad-Cardiel M, Alvarez-Alvarez B, Luque-Fernandez L, Fernandez C, Fernandez-Cruz A, Martell-Claros N (2013) Hypertension caused by primary hyperaldosteronism: increased heart damage and cardiovascular risk. Rev Esp Cardiol (Engl Ed) 66:47–52
Sigurjonsdottir HA, Gronowitz M, Andersson O, Eggertsen R, Herlitz H, Sakinis A et al (2012) Unilateral adrenal hyperplasia is a usual cause of primary hyperaldosteronism. Results from a Swedish screening study BMC Endocr Disord 12:17
Chao CT, Wu VC, Kuo CC, Lin YH, Chang CC, Chueh SJ et al (2013) Diagnosis and management of primary aldosteronism: an updated review. Ann Med 45:375–383
Nishikawa T, Omura M, Satoh F, Shibata H, Takahashi K, Tamura N et al (2011) Guidelines for the diagnosis and treatment of primary aldosteronism—the Japan Endocrine Society 2009. Endocr J 58:711–721
Lumachi F, Marzola MC, Zucchetta P, Tregnaghi A, Cecchin D, Favia G et al (2003) Non-invasive adrenal imaging in primary aldosteronism. Sensitivity and positive predictive value of radiocholesterol scintigraphy, CT scan and MRI. Nucl Med Commun 24:683–688
Yen RF, Wu VC, Liu KL, Cheng MF, Wu YW, Chueh SC et al (2009) 131I-6beta-iodomethyl-19-norcholesterol SPECT/CT for primary aldosteronism patients with inconclusive adrenal venous sampling and CT results. J Nucl Med 50:1631–1637
Chen YC, Su YC, Wei CK, Chiu JS, Tseng CE, Chen SJ et al (2011) Diagnostic value of I-131 NP-59 SPECT/CT scintigraphy in patients with subclinical or atypical features of primary aldosteronism. J Biomed Biotechnol 2011:209787
Sarkar SD, Cohen EL, Beierwaltes WH, Ice RD, Cooper R, Gold EN (1977) A new and superior adrenal imaging agent, 131I-6beta-iodomethyl-19-nor-cholesterol (NP-59): evaluation in humans. J Clin Endocrinol Metab 45:353–362
Nocaudie-Calzada M, Huglo D, Lambert M, Ernst O, Proye C, Wemeau JL et al (1999) Efficacy of iodine-131 6beta-methyl-iodo-19-norcholesterol scintigraphy and computed tomography in patients with primary aldosteronism. Eur J Nucl Med 26:1326–1332
Kazerooni EA, Sisson JC, Shapiro B, Gross MD, Driedger A, Hurwitz GA et al (1990) Diagnostic accuracy and pitfalls of [iodine-131]6-beta-iodomethyl-19-norcholesterol (NP-59) imaging. J Nucl Med 31:526–534
Ikeda DM, Francis IR, Glazer GM, Amendola MA, Gross MD, Aisen AM (1989) The detection of adrenal tumors and hyperplasia in patients with primary aldosteronism: comparison of scintigraphy, CT, and MR imaging. AJR Am J Roentgenol 153:301–306
Gross MD, Shapiro B, Grekin RJ, Freitas JE, Glazer G, Beierwaltes WH et al (1984) Scintigraphic localization of adrenal lesions in primary aldosteronism. Am J Med 77:839–844
Chen YC, Wei CK, Chen PF, Tzeng JE, Chuang TL, Wang YF (2009) Seeking the invisible: I-131 NP-59 SPECT/CT for primary hyperaldosteronism. Kidney Int 75:663
Hennings J, Sundin A, Hagg A, Hellman P (2010) 11C-metomidate positron emission tomography after dexamethasone suppression for detection of small adrenocortical adenomas in primary aldosteronism. Langenbeck’s Arch Surg 395:963–967
Burton TJ, Mackenzie IS, Balan K, Koo B, Bird N, Soloviev DV et al (2012) Evaluation of the sensitivity and specificity of (11)C-metomidate positron emission tomography (PET)-CT for lateralizing aldosterone secretion by Conn’s adenomas. J Clin Endocrinol Metab 97:100–109
Powlson AS, Gurnell M, Brown MJ (2015) Nuclear imaging in the diagnosis of primary aldosteronism. Curr Opin Endocrinol Diabetes Obes 22:150–156
Hahner S, Kreissl MC, Fassnacht M, Haenscheid H, Bock S, Verburg FA et al (2013) Functional characterization of adrenal lesions using [123I]IMTO-SPECT/CT. J Clin Endocrinol Metab 98:1508–1518
Authors’ contributions
Study conception and design: MDM, IGS. Acquisition of data: MDM, CMC. Analysis and interpretation of data: MDM, JMdN, LDG. Drafting of manuscript: MDM, LDG, MMM. Critical revision of manuscript: IGS.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethical approval
This study was merely observational and it does not contain any studies with human participants or animals performed by any of the authors.
Funding
None.
Conflict of interest
The authors declare that they have no conflict of interest.
Human and animal rights and informed consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Di Martino, M., García Sanz, I., Muñoz de Nova, J.L. et al. NP-59 test for preoperative localization of primary hyperaldosteronism. Langenbecks Arch Surg 402, 303–308 (2017). https://doi.org/10.1007/s00423-017-1561-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00423-017-1561-1