
Abstract
Background
Entero-atmospheric fistula (EAF) is an enteric fistula occurring in the setting of an open abdomen, thus creating a communication between the GI tract and the external atmosphere. Management and nursing of patients suffering EAF carries several challenges, and prevention of EAF should be the first and best treatment option.
Purpose
Here, we present a novel modified classification of EAF and review the current state of the art in its prevention and management including nutritional issues and feeding strategies. We also provide an overview on surgical management principles, highlighting several surgical techniques for dealing with EAF that have been reported in the literature throughout the years.
Conclusions
The treatment strategy for EAF should be multidisciplinary and multifaceted. Surgical treatment is most often multistep and should be tailored to the single patient, based on the type and characteristics of the EAF, following its correct identification and classification. The specific experience of surgeons and nursing staff in the management of EAF could be enhanced, applying distinct simulation-based ex vivo training models.
Similar content being viewed by others



Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The idea that abdomen can be left open after an emergent laparotomy started growing at the beginning of the twentieth century, when Pringle first described the open abdomen strategy in case of traumatic massive hepatic hemorrhage [1]. With the introduction of antibiotics and the advances of intensive care medicine, the open abdomen (OA) became increasingly often used and nowadays is recognized as a cornerstone step of damage control surgery (DCS) [2, 3].
Currently accepted indications for OA [4, 5] are trauma, abdominal sepsis, severe acute pancreatitis, loss of abdominal wall (either traumatic or after necrotizing fascitis), intra-abdominal hypertension or abdominal compartmental syndrome (ACS), and acute mesenteric ischemia.
Although DCS and OA have certainly helped in saving lives, the exposure of abdominal viscera carries itself a significant and unavoidable burden of morbidity; the most feared complication in this setting is the entero-atmospheric fistula (EAF). The onset of an EAF within open abdomen represents a surgical nightmare, carrying several extremely challenging issues in the field of critical care and nutritional management; EAF is therefore associated with significant morbidity and mortality. Despite the advances in OA management and the subsequent decrease of the initial reported mortality rates of 70 %, EAF’s mortality is nowadays still as high as up to 40 % [6, 7].
Definition
Entero-atmospheric fistula is an enteric fistula occurring within an open abdomen, thus creating a communication between the GI tract and external atmosphere. This scenario carries several challenging problems in the management because, instead of an entero-cutaneous fistula, there is neither a proper fistula tract nor skin or a well-vascularized tissue surrounding or overlying the fistula opening; all these factors making the spontaneous closure of the fistula almost impossible to achieve.
Incidence and etiology
With the increasing use of DCS and OA, EAF incidence is actually growing. The real incidence of EAF is not known, but a recent meta-analysis by Atema et al. [8] reported rates of fistula ranging from 5.7 to 17.2 % in non-trauma patients. In a large series of OA for the management of abdominal sepsis, the incidence of EAF was even higher, reaching 54.5 % [9].
The significant variability in the incidence rates may be explained by the etiology of EAF that can vary widely. Obviously, any trauma to the bowel occurring during the index operation or at the time of dressing changes can result in EAF formation, especially when the bowel is desiccated and dehydrated due to the exposure to the atmospheric air; for this reason, every attempt should be made to achieve as soon as possible the definitive closure of the open abdomen, because the longer the abdomen is left open, the greater is the risk of EAF [10]. Additionally, anastomotic leakage, ongoing bowel ischemia, distal bowel obstruction, and adhesion of the bowel to the fascia may cause an EAF.
The risk factors associated with EAF development are still largely undetermined. Two recent studies have attempted to answer the question about possible risk factors of EAF; the first is a multicenter prospective observational study by Bradley et al. [11] and demonstrated that large-bowel resection, large-volume resuscitation, and an increasing number of re-explorations were statistically significant predictors for development of a fistula in an open abdomen after trauma, and the second study is a retrospective dual-center analysis by Richter at al [7], who found that bowel perforation, anastomotic leakage, and ACS showed a significant association with the occurrence of EA fistulas, but the only significant predisposing factor for fistula formation was the presence of diverticulitis.
Classification
EAFs are classified according to different criteria. In first instance, EAF can either be deep or superficial. A deep EAF (Fig. 1) is a truly challenging situation, with the fistula arising deeply inside the OA and draining directly inside the peritoneal cavity, thus causing an ongoing peritonitis; whereas a superficial EAF (Fig. 2) drains on top of a granulating abdominal wound and, as a consequence, is easier to approach and manage, a superficial EAF is mainly associated with challenges in the stoma/wound management.

Image of a deep EAF which is a truly challenging situation, with a fistula arising deeply inside the OA and draining directly inside the peritoneal cavity

Image of a superficial EAF, draining on top of a granulating abdominal wound
The anatomic classification is based on the segment of GI tract involved, if the fistula that originates from stomach, duodenum, jejunum, or proximal ileus is classified as proximal; otherwise, if the fistula did onset from distal ileus or colon, it is classified as distal.
EAF can be also divided into the following three categories according to the daily output: low output (<200 ml/24 h), moderate output (200–500 ml/24 h), and high output (>500 ml/24 h) [12–14].
These classifications are extremely important for planning the optimal management, because distal and low-output EAFs are well known to be more likely able to close spontaneously when compared to those more proximal and high-output EAFs. Moreover, the location deep in the peritoneal cavity is considered to be a surgical emergency due to the ongoing peritonitis and should be treated immediately [13].
Furthermore, the onset of an EAF represents the worst higher grade of open abdomen, according to Bjork classification [15], depicting the worst possible scenario for an open abdomen.
A further criterion for classifying EAF (Table 1) is the presence of single (Fig. 1) vs multiple (Fig. 2) fistula openings, as described by Di Saverio et al. [41], because the number of fistula openings and their distance from each other have significant implications in the decision of the best suitable management option and in achieving an effective control and diversion of their output.
Prevention
As expected, the best treatment option for EAF is primary prevention. As for entero-cutaneous fistulas, knowing the causes and risk factors for fistula formation represents the most effective measure for prevention and definitive treatment. The factors associated with development and maintenance of entero-cutaneous fistulas (ECFs) are traditionally listed in the mnemonic acronym FRIENDS (F foreign body, R radiation, I infection or inflammatory bowel disease, E epithelialization, N neoplasm, D distal obstruction, and S short tract <2 cm); on the opposite, the factors associated with development of EAF during an open abdomen are less clearly determined and multiple factors can be recognized such as anastomotic disrupture, deserosalization, exposure of dehydrated and desiccated bowel to equipments and material used for temporary abdominal closure, adhesions, severe wound infections, severe trauma, bowel ischemia, visceral trauma during dressing changes, and negative pressure wound therapy (NPWT). The multidisciplinary team, which is in charge for the care of patients with OA, must be aware of the possibility of EAF formation, and every attempt should be made to prevent fistula formation. Desiccation of bowel loops and unrecognized micro-trauma occurring during dressing changes seems to be the trigger factor most frequently associated with fistula formation. Any rough and/or direct contact between the viscera and the devices used for temporary abdominal closure must be avoided or minimized, and the use of the greater omentum to cover the bowel as well as protecting the viscera with a fenestrated plastic sheet extended from one paracolic gutter to the other are all viable strategies; non-absorbable prosthetic meshes are not recommended, as they can erode the abdominal viscera leading to fistula formation. Whatever dressing is chosen to apply, the treating surgeons must pay attention to the complete sealing of the abdominal cavity from the outside environment; this should preclude the exposure of bowel loops to the atmospheric air and prevent their desiccation. Aggressive tissue preparation and extensive debridement should be performed only when absolutely necessary for interrupting or controlling the ongoing sepsis process. Early split thickness skin graft or cadaveric skin graft over the granulating viscera surrounding the fistula can help to protect the viscera and facilitate the EAF management. Furthermore, dressing changes should be carefully planned and should be performed only, or at least supervised, by senior attending surgeons with specific expertise in OA management, in order to decrease the risk of accidental bowel injury. Given the rarity of EAF, gaining a specific expertise in EAF management is hard to achieve in vivo on the patients, except for the few surgeons who are working in high-volume mature trauma and acute care surgery centers or in tertiary referral centers. A new concept for developing a simulation-based, ex vivo, training device for open abdomen management, with the aim to help the junior or un-experienced surgical and nursing staff in gaining a specific expertise in dressing and nursing within the setting of an open abdomen, might be beneficial.
Closing the abdomen as soon as possible remains the best strategy for preventing EAF formation, because any prolonged duration of the bowel exposure to the outside environment invariably results in an increased rate of complications, including EAF formation [10].
The most frequently used temporary abdominal closure technique in OA management is the NPWT [16]. It was hypothesized that NPWT may be associated to and facilitate the development of EAF, but this controversy has now largely been contradicted [17, 18]. However, in an animal study performed by Lindstedt et al., higher levels of negative pressure suction resulted in a measurable reduction in bowel blood flow; this may ultimately induce ischemia and secondary necrosis in the intestinal wall, which could finally promote the development of intestinal fistulae [19, 20]. Although the clinical impact of this observation is still uncertain, there is a tendency toward a word of caution and use of lower pressures in suction [21].
Risk factors for fistula formation and practical suggestions for any corresponding preventive measures are summarized in Table 2.
Nutritional issues and management nutritional strategies
Patients with EAF always need a multidisciplinary approach for achieving an optimal multifaceted management, because of their extremely complex anatomical and pathophysiology derangements. As early as 1964, Chapman et al. [22] noted that malnutrition was the leading cause of death in patients with ECF and mortality was considerably reduced with a daily intake of at least 1500 Kcal; since then, nutritional support has gained a pivotal role in the management of the critically ill patients with enteric fistulas. Patients with OA and EAF are not different than those with ECF; they are in a virtually endless hypercatabolic state, secondary not only to the loss of fluids and bowel contents but also to the ongoing peritonitis and activation of the stress response. Furthermore, the high amounts of fluid and nutrient losses from fistula output invariably lead to fluid depletion, electrolyte imbalance, and acid/base disturbances as well as malnourishment status [14, 23, 24].
For several decades, total parenteral nutrition (TPN) has been the standard of care for severely injured patients, because of the widespread common belief that these patients are intolerant to enteral nutrition (EN) or that EN is contraindicated; traditionally, patient with OA have been maintained nil-per-mouth until enough time has passed after closure of the abdominal fascia, because of the concerns about paralytic ileus, bowel edema, additional delays, and difficulties of fascial closure due to bowel distension and the fear of micro-aspiration, resulting in a significantly higher potential risk of aspiration and inhalation pneumonia. In the last decade, however, numerous studies have challenged this belief and the management of open abdomen and EAF have significantly changed following the evolution of the concepts about enteral nutritional support; in fact, multiple studies have demonstrated the beneficial effect of EN and its feasibility even in patients with OA and EAF, showing a protective effect of EN from infectious complications without affecting the feasibility of fascial closure [25, 26].
Despite the great advances in parenteral and enteral formulations, nutrition of patients with OA and EAF can be really challenging and some basic principles should be kept in mind.
-
The initial step of nutritional management must be the stabilization of the patients with aggressive treatment of sepsis, by either surgical or medical techniques, and rapid correction of any fluids, electrolytes, and acid–base imbalances.
-
Hydration and volume status should be meticulously monitored throughout the entire length of hospital stay; properly, accurate vacuum-assisted closure (VAC) dressings could be truly helpful, because they allow the correct quantification of fluid losses and may significantly reduce the evaporation across the open wound [27].
-
Interval nutrition with TPN should be started as soon as possible.
-
A correct definition of the anatomy of EAF is mandatory for a proper patients’ nutrition; the critical target of this phase is to determine the total length of the remaining bowel and how much continuous bowel surface or functioning absorbing bowel is available for EN. Determining the fistula anatomy and accurate measurement of bowel length can be particularly challenging in case of multiple EAF, and it can be accomplished with the aid of computed tomography, magnetic resonance enterography, fistulography, ingestion of dye or charcoal, and passage of enteric tubes used as landmarks during subsequent re-imaging [28]. Furthermore, the knowledge of the electrolytes composition of the GI fluids is also necessary [29].
-
Obtaining a functioning and effective feeding access can be extremely challenging; TPN requires a central venous access, bringing itself a great burden of complications, either infectious, thrombotic, or related to the insertion site. Alternative central routes are associated to lesser infectious complications and can be maintained for longer periods such as “tunneled” cuffed central venous catheter (CVC) (including HICKMAN™ and BROVIAC™) or tunneled non-cuffed CVCs. Other alternative options can be percutaneously inserted central catheters (PICCs) or midline catheters. Nonetheless, EN access should be safer and easier to establish and maintain, using as many small-bowel segments for absorption as possible [30]. Thus, enteral feeding access should be tailored upon specific patient characteristic and multiple possibilities are available; nasogastric or nasojejunal tubes, jejunostomy or fistuloclysis, are the most commonly used [31, 32].
-
A reliable nutritional assessment and monitoring and the creation of a nutritional plan play of pivotal importance. There are different nutritional markers currently available for a reliable estimation, such as the Harris-Benedict equation, which can be used for the initial evaluation; corrections should be made to the basal energy expenditure obtained from empiric equations in accordance to the specific characteristics of the single patient. High-output fistula will usually require 1.5–2 times the usual calories, because of ongoing losses; supplementation of vitamins and trace elements is crucial, and a correction of 2 g of nitrogen per liter of abdominal fluid lost from the OA is necessary to maintain a positive nitrogen balance [33].
-
Enteral feeding should be started as soon as possible; the benefits of early EN compared to TPN are well known and supported by a great body of literature [25–31, 33–36]. These advantages include preservation of the intestinal mucosal barrier and its immunological function [36] and a reduced rate of infectious complications.
-
The ultimate aim in feeding patients with EAF is not just to prevent or treat malnutrition but also to manipulate the stress response to injury and infection and improve the patient’s outcome [37].
-
EN can increase EAF output, so the greatest efforts must be made to obtain the complete and effective diversion of fistula effluent.
In this scenario, the reduction of gastrointestinal secretions could be helpful in reducing fistula output and facilitate effluent control; gastric secretion can be decreased using H2 receptor antagonists or proton pump inhibitors [38], while somatostatine and its analogues [36, 38–40] are used to reduce pancreatic and gastric secretion, mesenteric blood flow, and gastric and gallbladder emptying. These drugs are usually effective in reducing fistula output, but caution must be used because they can also inhibit the secretion of insulin and glucagon.
Management
Principles of management
If all above-cited precautions fail and an EAF develops, many of the principles used for ECF management can also be applied in managing EAF. Assuming that the best therapeutic option, i.e., a proximal bowel diversion, is almost invariably impossible for several reasons, such as mesentery retraction and edema, “frozen abdomen,” and abdominal wall tissue loss or retraction; the main target of the treatment is to completely divert the fistula output, protecting surrounding viscera and allowing clean granulation of the exposed bowel. A high degree of heterogeneity remains among the several surgical techniques described in the literature, and no single approach would prove to be ideal in every circumstance; the clinical algorithm for EAF management is constantly changing. For this reason, we hereby suggest a modified and improved version (Fig. 11) of the previous clinical algorithm we have recently proposed [41] in an attempt to further rationalize the approach to EAF. All the available surgical options for fistula diversion are listed in the following paragraph.
Surgical techniques for fistula management
EAF has unique features, therefore making its spontaneous closure almost impossible to achieve; for this reason, the management of the fistula should be aimed to completely divert the fistula output, thus allowing a clean granulation of the exposed bowel and promoting the fistula to become a chronic but well-controlled fistula. This result is hard to achieve, because of the extreme frailty of the tissues surrounding the fistula; those tissues are, most times, conglutinated in a “frozen abdomen” prohibiting any surgical maneuver, furthermore associated with presence of relevant systemic derangements of the patient, driven by severe dehydration, hypercatabolic status, and ongoing sepsis caused by the spillage of enteric content directly into the peritoneal cavity.
When an EAF appears, a careful exploration of the abdominal cavity must be performed to exclude the presence of other hidden un-diagnosed fistulas that can maintain the sepsis and to rule out every condition which can possibly preclude the closure of the fistula such as the presence of a foreign body, an inflammatory bowel disease, a neoplasm, or a distal obstruction; if present, these underlying conditions must be treated either medically or surgically to increase the chances of fistula closure and to facilitate the control of fistula effluent. After that, and before placing any dressing over the open abdomen, a proper thorough irrigation of the abdominal cavity should be performed to reduce peritoneal contamination and limit the ongoing sepsis.
A large spectrum of techniques and surgical devices is described in literature; every surgeon usually develops his own technique, and none of those can perfectly fit well in every kind of clinical situation. After an accurate review of the literature about EAF management, below is listed a short summary of the techniques described so far:
-
1.
NPWT—for many years, it has been considered the only option for EAF management [18, 42], and some studies demonstrate that in a small proportion of cases, the fistula can spontaneously heal during NPWT [9]. This method is the easiest to apply and represents the base of initial treatment for most of the other following techniques.
-
2.
Primary suture/fibrin glue or cyanoacrylates/biological dressing (i.e., human acellular dermal matrix or cadaveric split-thickness skin graft) [43–45]—the combination of these three methods can achieve good results, especially in case of small fistulas and deserosalizations (Fig. 3 is showing an attempt of sealing with primary suture and cyanoacrylates).
Fig. 3 
Initial attempt of sealing EAF with primary suture repair and cyanoacrylates
-
3.
Floating stoma [46]—this is the first reported attempt to manage EAF by diverting fistula output and allowing the abdominal viscera to granulate. Concerns arise about the traumatic impact on the friable bowel of the running suture used to create this so called “floating stoma.”
-
4.
Fistula VAC [47]—this method represents the first application of VAC therapy to EAF management and is relatively easy and quick to realize. A number of refinements to this technique are present in the literature, aiming to obtain a better sealing of fistula area from the rest of the wound, thus avoiding pooling of enteric contents under the sponge [48–51].
-
5.
Tube VAC [52]—the EAF is intubated with Malecot catheters having a size roughly corresponding to the size of the fistula; the wound is then covered with a polyurethane sponge. The Malecot catheters are pulled through it, and the entire device is then sealed and a continuous negative pressure is applied.
-
6.
Pepe’s technique [53]—a hole is made in the central part of the VAC foam so as to insert three drains. The sponge surface overlying the bowel wall is covered with the polyethylene drape to avoid injury of the viscera. The hole with the drains is placed over the EAF, and the VAC pad is placed above it in order to directly drain the intestinal effluent toward the aspiration system.
-
7.
Silo VAC [54]—the inside wall of a syringe plastic barrel is wrapped with a petroleum gauze. The stoma paste is placed on the outer edges of the barrel in order to get a better sealing. The VAC system is then applied around the silo on the open abdomen surface, and bowel effluent is drained into a collection bag placed over the plastic barrel (Fig. 4; silo VAC in a simulation model ex vivo—courtesy of Dr. D. A. Walczak)
Fig. 4 
Silo VAC technique for EAF management in a simulation model ex vivo. Courtesy of Dr. D. A. Walczak
-
8.
Fistula intubation and conversion to an ECF [55]—the EAF is intubated with Malecot catheter which is then tunneled through adjacent mobilized skin-subcutaneous flaps, converting the EAF to a sort of ECF with a long channel, surrounded by a well-vascularized tissue. Finally, this fistula tract may be further injected with a fibrin glue to promote healing.
-
9.
Nipple VAC [56]—a baby nipple is placed over the fistula opening, a catheter is placed through the tip of the nipple, a round layer of colostomy paste is spread under the silicon nipple edges, and the entire wound is covered by any commercially available VAC dressing. This method has the great advantage of being completely atraumatic, but the nipple-tube complex can be easily displaced, especially during the maneuvers for nursing the patient (Fig. 5). A further advantage of this technique is the possibility of being used for controlling multiple fistula openings, either in close proximity or distant from each other, because the baby nipple and the attached Pezzer tube are versatile and can be moved over multiple and distant fistula openings (Fig. 6).
Fig. 5 
Nipple VAC technique for EAF management and diversion. A baby nipple is placed over the fistula opening, a catheter is placed through the tip of the nipple, a round layer of colostomy paste is spread under the silicon edges of the nipple, and the entire wound is covered by any commercially available VAC dressing. This method is completely atraumatic, but the nipple-tube complex can be easily displaced, especially during nursing maneuvers of the patient
Fig. 6 
Nipple VAC technique for EAF management and diversion A further advantage of this technique is the possibility of being used for controlling multiple fistula openings, either in close proximity or distant from each other, because the baby nipple and the attached Pezzer tube are versatile and can be moved over multiple and distant fistula openings
-
10.
Baby bottle nipple diversion—this is a refinement [57] of the previous technique, where a small-size Foley catheter is inserted into the fistula hole and the balloon is gently inflated; this improvement is aimed to obtain a better seal and a more effective fistula diversion (Fig. 7). The Foley catheter, inflated and secured inside the fistula, may be helpful in better preventing the dislodgment of the baby nipple from over the fistula opening (Fig. 8).
Fig. 7 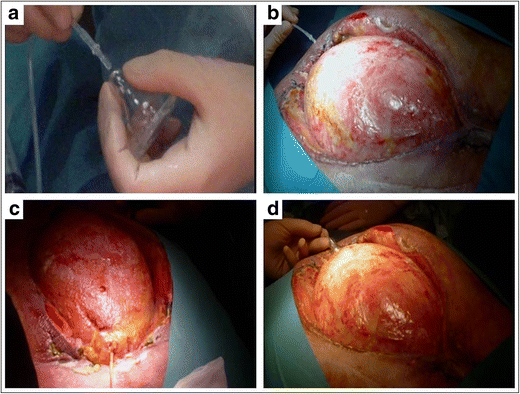
A small-size Foley catheter can be inserted into the fistula hole, and the balloon is gently inflated; this improvement aimed to obtain a better seal and prevent leaks, therefore obtaining a better fistula diversion
Fig. 8 
A Foley catheter can be inflated and secured inside the fistula, for better preventing the dislodgment of the baby nipple from over the fistula opening
-
11.
VAC chimney [58]—a chimney is created with a white sponge dressing, and the base of this handmade device can cover the adjacent healthy tissue to avoid leakage of bowel effluent; the entire dressing is then covered with a conventional VAC dressing, placing the connector to the pump directly over the chimney (Fig. 9; VAC chimney in a simulation ex vivo model—courtesy of Dr. D. A. Walczak)
Fig. 9 
VAC chimney technique for EAF management in a simulation ex vivo model. Courtesy of Dr. D. A. Walczak
-
12.
VAC collapsible fistula isolation device [59]—the base of collapsible fistula isolation device (wound crown and fistula solution) is cut open to fit around the fistula, and the VAC sponge dressing is placed around the isolation device to create a channel for collecting the fistula effluent; an ostomy pouch is placed over the channel and can be also connected to continuous suction, for a better control of very high output fistulas.
-
13.
Fistula patch [60]—this technique is the first technique attempting to seal the fistula from inside the bowel lumen; a soft, flexible gel lamellar is shaped in order to obtain a round shape and is then folded and pushed into the fistula. Once inside the bowel, it will unwrap, working like a patch. This dressing will remain in place until definitive fistula takedown surgery.
-
14.
Fistula plug [61]—this method is also aiming to seal the fistula from inside; a silicone plug is rolled and inserted into the fistula hole. When the fistula is closed, the thread will be cut off and the silicon plug will be discharged at the time of defecation.
-
15.
Pedicle flap—multiple types of flaps are currently described in literature [62–67]; however, because they require a well-nourished patient and a stabilized physiological homeostasis, they are good methods for approaching EAF in a later stage and after the acute phase has resolved.
-
16.
Suspension/stoma conversion [65, 68]—in selected cases, the fistula edges can be mobilized and fixed to the lateral dermis and converted into a usual bowel ostomy.







It is easy to figure out that EAFs being single, small, distal, superficial, and of low output are more likely to close spontaneously; in this group of fistulas, it may be worth an initial attempt of primary closure with sutures and different types of sealants (fibrin glue and cyanoacrylates) [43, 45]. In contrast, when dealing with large, deep, proximal, and high-output fistulas, or with multiple openings, primary closure is absolutely unlikely to be successful; furthermore, the fistula should be exteriorized as much as possible outside the abdominal cavity, thus creating a flat surface where a diversion device can be applied more easily. Finally, as already stated, the possible presence of multiple fistula openings can make the local situation even more complicated to manage and requires a surgical technique for controlling the output which should be easy and quick to apply and occupying only small space in the OA; this aim can be achieved by using the nipple VAC or the baby bottle nipple diversion technique.
All these management options are aimed to bridge the patient to a delayed definitive treatment when the sepsis and the peritonitis are resolved and the surrounding bowel has granulated enough to allow the definitive “closure” of the wound either by skin grafting or use of any other biological materials.
Definitive surgery for fistula resection and abdominal wall reconstruction should be delayed for at least 8–12 months, to allow proper loosening of the visceral adhesions, and should be performed only when the patient is well nourished and has reached a well-balanced physiological homeostasis. Multiple surgical approaches for definitive fistula takedown and abdominal bowel reconstruction may be required in a multistep fashion, and several strategies are described in literature [13, 63, 69–72].
Simulation-based training for the surgical management and nursing of EAFs
Since the management and good outcomes of patients with EAF are clearly related to an optimal management performed by experienced surgeons and specifically trained nursing staff, confident in the management of such rare but challenging situations, the idea of a training device to get the surgeons and nurses staff becoming more experienced in dealing with this condition would be definitely beneficial. Such educational system may improve the hands-on ability in handling EAF and subsequently improve the outcomes. The new concept for developing a simulation-based, ex vivo, training, with the aim to help the junior or un-experienced surgical and nursing staff in gaining a specific expertise, might be therefore beneficial. A specific OA and EAF simulation trainer has been created and developed by Walczak D. A. et al. from the John Paul II Memorial Hospital, Belchatow, Poland, which is able to reproduce a reliable simulation of an OA situation, with or without concomitant EAF, and therefore to make every surgeon or nursing staff able to become confident with all the currently available techniques for EAF management and to practice the dressing of such conditions. Planning specific studies and obtaining future clinical data on the outcomes achieved before and after specific training sessions and gain of expertise with such a simulation trainer might be able to eventually demonstrate a reduction in the incidence of EAF and/or improvements in their management and long-term outcomes (Fig. 10; simulation device for ex vivo training in surgical technique management and nursing of EAF—courtesy of Dr. D. A. Walczak).

Simulation device of an open abdomen with EAF for ex vivo training in surgical technique management and nursing of EAF. Courtesy of Dr. D. A. Walczak

An updated algorithm for EAF management
Conclusions
Prevention and management of EAF are extremely challenging and should be targeted upon the specific patients’ characteristic on a case-by-case model; key points of the treatment are (1) diversion of fistula effluent, blocking the contamination of the peritoneal cavity, and the associated sepsis and (2) prevention of malnutrition, dehydration, and electrolyte imbalance with a proper parenteral/enteral nutrition.
A multidisciplinary approach is mandatory, with close collaboration among surgeon, anesthetist and ICU attending, nutritionist, psychologist, and specialized nurses.
A great degree of confusion characterizes the EAF management, and the variety of techniques proposed, as well as the continuous release of new review articles [13, 73] trying to summarize the several surgical techniques and treatment strategies, are still not able to clarify which one is the optimal strategy in case of EAF onset. Although it is almost impossible performing randomized controlled clinical trials for such a complex condition, the need for prospective observational studies and multiinstitutional prospectively collected registries, with a clear description of included patients and thorough data collection, including indications and management for OA, classification and management of EAF, and outcomes and follow-up, is noteworthy for achieving definite improvements in the outcomes of such patients. Meanwhile, for optimal management of EAFs, we strongly suggest planning a multidisciplinary and multifaceted treatment strategy, with the choice of a multistep surgical treatment which should be better tailored on the type and characteristics of the EAF, based on their correct identification and precise classification (following our updated algorithm shown in Fig. 11).
References
Pringle JH (1908) V. Notes on the arrest of hepatic hemorrhage due to trauma. Ann Surg 48:541–9
Rotondo MF, Schwab CW, McGonigal MD, Phillips GR, Fruchterman TM, Kauder DR, Latenser BA, Angood PA (1993) Damage control: an approach for improved survival in exsanguinating penetrating abdominal injury. J Trauma: Injury, Infec Crit Care 35:375–82, discussion 82–3
Rotondo MF, Zonies DH (1997) The damage control sequence and underlying logic. Surg Clin North Am 77:761–77
Coccolini F, Biffl W, Catena F, Ceresoli M, Chiara O, Cimbanassi S, Fattori L, Leppaniemi A, Manfredi R, Montori G, Pesenti G, Sugrue M, Ansaloni L (2015) The open abdomen, indications, management and definitive closure. World J Emerg Surg 10:32
Schecter W, Ivatury R, Rotondo M, Hirshberg A (2006) Open abdomen after trauma and abdominal sepsis: a strategy for management. J Am Coll Surg 203:390–6
Becker HP, Willms A, Schwab R (2007) Small bowel fistulas and the open abdomen. Scand J Surg 96:263–71
Richter S, Dold S, Doberauer JP, Mai P, Schuld J (2013) Negative pressure wound therapy for the treatment of the open abdomen and incidence of enteral fistulas: a retrospective bicentre analysis. In: Gastroenterology Research and Practice 1–6
Atema JJ, Gans SL, Boermeester MA (2014) Systematic review and meta-analysis of the open abdomen and temporary abdominal closure techniques in non-trauma patients. In: World J Surg 912–25
Kirshtein B, Mizrahi S (2014) Vacuum-assisted management of enteroatmospheric fistula within the open abdomen. Am Surg 80:209–10
Miller RS, Morris JA, Diaz JJ, Herring MB, May AK (2005) Complications after 344 damage-control open celiotomies. Journal Trauma: Injury, Infec Critical Care 59:1365–71, Discussion 71–4
Bradley MJ, Dubose JJ, Scalea TM, Holcomb JB, Shrestha B, Okoye O, Inaba K, Bee TK, Fabian TC, Whelan JF, Ivatury RR, Group AOAS (2013) Independent predictors of enteric fistula and abdominal sepsis after damage control laparotomy: results from the prospective AAST open abdomen registry. JAMA Surg 148:947–54
Schecter WP, Hirshberg A, Chang DS, Harris HW, Napolitano LM, Wexner SD, Dudrick SJ (2009) Enteric fistulas: principles of management. ACS 209:484–91
Marinis A, Gkiokas G, Argyra E, Fragulidis G, Polymeneas G, Voros D (2013) “Enteroatmospheric fistulae”-gastrointestinal openings in the open abdomen: a review and recent proposal of a surgical technique. Scand J Surg 102:61–8
Evenson A, Fischer J (2006) Current management of enterocutaneous fistula. J Gastrointest Surg 10:455–64
Björck M, Bruhin A, Cheatham M, Hinck D, Kaplan M, Manca G, Wild T, Windsor A (2009) Classification—important step to improve management of patients with an open abdomen. World J Surg 33:1154–7
Quyn AJ, Johnston C, Hall D, Chambers A, Arapova N, Ogston S, Amin AI (2012) The open abdomen and temporary abdominal closure systems—historical evolution and systematic review. Color Dis Offi J Assoc Coloproctology of Great Britain and Ireland 14:e429–38
Carlson GL, Patrick H, Amin AI, McPherson G, MacLennan G, Afolabi E, Mowatt G, Campbell B (2013) Management of the open abdomen: a national study of clinical outcome and safety of negative pressure wound therapy. Ann Surg 257:1154–9
Navsaria P, Nicol A, Hudson D, Cockwill J, Smith J (2013) Negative pressure wound therapy management of the “open abdomen” following trauma: a prospective study and systematic review. World J Emerg Surg 8:4
Lindstedt S, Malmsjö M, Hlebowicz J, Ingemansson R (2015) Comparative study of the microvascular blood flow in the intestinal wall, wound contraction and fluid evacuation during negative pressure wound therapy in laparostomy using the V.A.C. abdominal dressing and the ABThera open abdomen negative pressure therapy system. In: International wound journal: Blackwell Publishing Ltd 83–8.
Hlebowicz J, Hansson J, Lindstedt S (2012) Microvascular blood flow response in the intestinal wall and the omentum during negative wound pressure therapy of the open abdomen. Int J Colorectal Dis 27:397–403
Bruhin A, Ferreira F, Chariker M, Smith J, Runkel N (2014) Systematic review and evidence based recommendations for the use of negative pressure wound therapy in the open abdomen. Int J Surg 12:1105–14
Chapman R, Foran R, Dunphy JE (1964) Management of intestinal fistulas. AJS 108:157–64
Schecter WP (2011) Management of enterocutaneous fistulas. Surg Clin North Am 91:481–91
Davis KG, Johnson EK (2013) Controversies in the care of the enterocutaneous fistula. Surg Clin North Am 93:231–50
Dissanaike S, Pham T, Shalhub S, Warner K, Hennessy L, Moore EE, Maier RV, O’Keefe GE, Cuschieri J (2008) Effect of immediate enteral feeding on trauma patients with an open abdomen: protection from nosocomial infections. J Am Coll Surg 207:690–7
Byrnes MC, Reicks P, Irwin E (2010) Early enteral nutrition can be successfully implemented in trauma patients with an “open abdomen”. Am J Surg 199:359–62, discussion 63
Friese RS (2012) The open abdomen: definitions, management principles, and nutrition support considerations. Nutr Clin Pract 27:492–8
Polk TM, Schwab CW (2012) Metabolic and nutritional support of the enterocutaneous fistula patient: a three-phase approach. World J Surg 36:524–33
Majercik S, Kinikini M, White T (2012) Enteroatmospheric fistula: from soup to nuts. In: Nutrition in Clinical Practice 507–12
Tsuei BJ, Magnuson B, Swintosky M, Flynn J, Boulanger BR, Ochoa JB, Kearney PA (2003) Enteral nutrition in patients with an open peritoneal cavity. In: Nutrition in Clinical Practice 253–8.
Yin J, Wang J, Yao D, Zhang S, Mao Q, Kong W, Ren L, Li Y, Li J (2014) Is it feasible to implement enteral nutrition in patients with enteroatmospheric fistulae? A single-center experience. Nutr Clin Pract 29:656–61
Willcutts K, Mercer D, Ziegler J (2015) Fistuloclysis: an interprofessional approach to nourishing the fistula patient. J Wound Ostomy Continence Nurs 42:549–53
Cheatham ML, Safcsak K, Brzezinski SJ, Lube MW (2007) Nitrogen balance, protein loss, and the open abdomen. Crit Care Med 35:127–31
Moore FA, Feliciano DV, Andrassy RJ, McArdle AH, Booth FV, Morgenstein-Wagner TB, Kellum JM, Welling RE, Moore EE (1992) Early enteral feeding, compared with parenteral, reduces postoperative septic complications. The results of a meta-analysis. In: Annals of Surgery 172–83
Kudsk KA, Croce MA, Fabian TC, Minard G, Tolley EA, Poret HA, Kuhl MR, Brown RO (1992) Enteral versus parenteral feeding. Effects on septic morbidity after blunt and penetrating abdominal trauma. In: Annals of Surgery: Lippincott, Williams, and Wilkins 503-11 discussion 11–3.
Yuan Y, Ren J, Gu G, Chen J, Li J (2011) Early enteral nutrition improves outcomes of open abdomen in gastrointestinal fistula patients complicated with severe sepsis. In: Nutrition in Clinical Practice 688–94
Weissenfluh GM, Brundage SI, Spain DA (2006) Early enteral nutrition after abdominal trauma: effects on septic morbidity and practicality. In: Nutrition in Clinical Practice 479–84
Lloyd DA, Gabe SM, Windsor AC (2006) Nutrition and management of enterocutaneous fistula. Br J Surg 93:1045–55
Stevens P, Foulkes RE, Hartford-Beynon JS, Delicata RJ (2011) Systematic review and meta-analysis of the role of somatostatin and its analogues in the treatment of enterocutaneous fistula. In: European Journal of Gastroenterology & Hepatology 912–22
Ren J, Yuan Y, Zhao Y, Gu G, Wang G, Chen J, Fan C, Wang X, Li J (2014) Open abdomen treatment for septic patients with gastrointestinal fistula: from fistula control to definitive closure. In: Am Surg 339–47
Di Saverio S, Tarasconi A, Inaba K, Navsaria P, Coccolini F, Costa Navarro D, Mandrioli M, Vassiliu P, Jovine E, Catena F, Tugnoli G (2015) Open abdomen with concomitant enteroatmospheric fistula: attempt to rationalize the approach to a surgical nightmare and proposal of a clinical algorithm. In: Journal of the American College of Surgeons: Elsevier e23-33.
Navsaria PH, Bunting M, Omoshoro-Jones J, Nicol AJ, Kahn D (2003) Temporary closure of open abdominal wounds by the modified sandwich-vacuum pack technique. Br J Surg 90:718–22
Girard S, Sideman M, Spain DA (2002) A novel approach to the problem of intestinal fistulization arising in patients managed with open peritoneal cavities. AJS 184:166–7
Jamshidi R, Schecter WP (2007) Biological dressings for the management of enteric fistulas in the open abdomen: a preliminary report. Arch Surg 142:793–6
Bhat YM, Banerjee S, Barth BA, Chauhan SS, Gottlieb KT, Konda V, Maple JT, Murad FM, Pfau PR, Pleskow DK, Siddiqui UD, Tokar JL, Wang A, Rodriguez SA, Committee AT (2013) Tissue adhesives: cyanoacrylate glue and fibrin sealant. Gastrointest Endosc 78:209–15
Subramaniam MH, Liscum KR, Hirshberg A (2002) The floating stoma: a new technique for controlling exposed fistulae in abdominal trauma. J Trauma: Injury, Infec Critical Care 53:386–8
Goverman J, Yelon JA, Platz JJ, Singson RC, Turcinovic M (2006) The “fistula VAC,” a technique for management of enterocutaneous fistulae arising within the open abdomen: report of 5 cases. J Trauma: Injury, Infec Critical Care 60:428–31
D’Hondt M, Devriendt D, Van Rooy F, Vansteenkiste F, D’Hoore A, Penninckx F, Miserez M (2011) Treatment of small-bowel fistulae in the open abdomen with topical negative-pressure therapy. AJS 202:e20–e4
Piazza R, Armstrong S, Vanderkolk W, Eriksson E, Ringler S (2009) A modified “fistula-VAC” technique: management of multiple enterocutaneous fistulas in the open abdomen. Plastic and Reconstructive Surgery 124:453e-5e
Pang TC, Morton J, Pincott S (2012) Novel technique for isolating and dressing enteroatmospheric fistulae. ANZ J Surg 82:747–9
Timmons J, Russell F (2013) The use of negative-pressure wound therapy to manage enteroatmospheric fistulae in two patients with large abdominal wounds. In: International Wound Journal 723–9
Al-Khoury G, Kaufman D, Hirshberg A (2008) Improved control of exposed fistula in the open abdomen. J Am Coll Surg 206:397–8
Pepe G, Magalini S, Callari C, Persiani R, Lodoli C, Gui D (2014) Vacuum assisted closure (VAC) therapy (TM) as a Swiss knife multi-tool for enteric fistula closure: tips and tricks: a pilot study. In: Eur Rev Med Pharmacol Sci 2527–32
Verhaalen A, Watkins B, Brasel K (2010) Techniques and cost effectiveness of enteroatmospheric fistula isolation. In: Wounds 212–7
Ramsay PT, Mejia VA (2010) Management of enteroatmospheric fistulae in the open abdomen. In: Am Surg 637–9
Layton B, DuBose J, Nichols S, Connaughton J, Jones T, Pratt J (2010) Pacifying the open abdomen with concomitant intestinal fistula: a novel approach. Am J Surg 199:e48–e50
Di Saverio S, Villani S, Biscardi A, Giorgini E, Tugnoli G (2011) Open abdomen with concomitant enteroatmospheric fistula: validation, refinements, and adjuncts to a novel approach. J Trauma: Injury, Infec Critical Care 71:760–2
Rekstad LC, Wasmuth HH, Ystgaard B, Stornes T, Seternes A (2013) Topical negative-pressure therapy for small bowel leakage in a frozen abdomen. J Trauma and Acute Care Surg 75:487–91
Heineman JT, Garcia LJ, Obst MA, Chong HS, Langin JG, Humpal R, Pezzella PA, Dries DJ (2015) Collapsible enteroatmospheric fistula isolation device: a novel, simple solution to a complex problem. ACS 1–8
Wang G, Ren J, Liu S, Wu X, Gu G, Li J (2013) “Fistula patch”: making the treatment of enteroatmospheric fistulae in the open abdomen easier. J Trauma and Acute Care Surg 74:1175–7
Ozer MT, Sinan H, Zeybek N, Peker Y (2014) A simple novel technique for enteroatmospheric fistulae: silicone fistula plug. Int Wound J 11(Suppl 1):22–4
Sriussadaporn S, Sriussadaporn S, Kritayakirana K, Pak-art R (2006) Operative management of small bowel fistulae associated with open abdomen. Asian J Surg 29:1–7
Wind J, van Koperen PJ, Slors JFM, Bemelman WA (2009) Single-stage closure of enterocutaneous fistula and stomas in the presence of large abdominal wall defects using the components separation technique. AJS 197:24–9
Stephensen B, Brown J, Lambrianides A (2012) A novel method for managing enterocutaneous fistulae in the open abdomen using a pedicle flap. J Surg Case Rep 2012:5
Al-Nahawi M (2013) A rare approach to entero-atmospheric fistula. In: Am J Case Rep 476–80.
Gupta R, Singh H, Talukder S, Verma GR (2015) A new technique of closing a gastroatmospheric fistula with a rectus abdominis muscle flap. In: BMJ Case Rep bcr2015209309-bcr.
Lambe G, Russell C, West C, Kalaiselvan R, Slade DAJ, Anderson ID, Watson JS, Carlson GL (2012) Autologous reconstruction of massive enteroatmospheric fistulation with a pedicled subtotal lateral thigh flap. In: Br J Surg 964–72
Clark CE, Walker T, Bacon L, McCoy J, Babaloa O (2013) Staged suspension of an enteroatmospheric fistula: a novel surgical approach. Am Surg 79:E139–40
Krpata DM, Stein SL, Eston M, Ermlich B, Blatnik JA, Novitsky YW, Rosen MJ (2013) Outcomes of simultaneous large complex abdominal wall reconstruction and enterocutaneous fistula takedown. AJS 205:354–9
Dionigi G, Dionigi R, Rovera F, Boni L, Padalino P, Minoja G, Cuffari S, Carrafiello G (2008) Treatment of high output entero-cutaneous fistulae associated with large abdominal wall defects: single center experience. Int J Surg 6:51–6
Demetriades D (2003) A technique of surgical closure of complex intestinal fistulae in the open abdomen. J Trauma: Injur Infect Crit Care 55:999–1001
Latifi R, Joseph B, Kulvatunyou N, Wynne JL, O’Keeffe T, Tang A, Friese R, Rhee PM (2011) Enterocutaneous fistulas and a hostile abdomen: reoperative surgical approaches. In: World J Surg 516–23.
Terzi C, Egeli T, Canda AE, Arslan NC (2014) Management of enteroatmospheric fistulae. Int Wound J 11(Suppl 1):17–21
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
This study received no funds.
Conflict of interest
All authors declare that they have no conflict of interest.
Human and animal rights and informed consent
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Rights and permissions
About this article

Cite this article
Di Saverio, S., Tarasconi, A., Walczak, D.A. et al. Classification, prevention and management of entero-atmospheric fistula: a state-of-the-art review. Langenbecks Arch Surg 401, 1–13 (2016). https://doi.org/10.1007/s00423-015-1370-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00423-015-1370-3