
Abstract
Background and aims
In view of the increasing numbers of old and very old people in the general population, we evaluated the short-term outcomes of laparoscopic colorectal surgery for differences between younger and older patients.
Methods
A total of 4823 patients with complete data sets from a prospective, clinical observational multicentre study initiated by the “Laparoscopic Colorectal Surgery Study Group” were analysed for this investigation.
Results
Of the patients, 909 (18.8%) were older and 3914 (81.2%) younger than 75 years. In the older patient group, malignant disease was a significantly more common indication for surgery. As was expected, the rate of general complications (pneumonia, cardiopulmonary problems, urinary tract infection) was significantly higher in the older patient group with its greater prevalence of preoperative comorbidity, but there no differences in terms of intraoperative or postoperative surgical complications or conversion rate between the groups.
Conclusion
The higher rate of postoperative complications resulting from preoperative comorbidity in the older patients makes it necessary that the indication for surgery be established with care. In view of the advantages of the laparoscopic approach with regard to the postoperative course, the preferential use of laparoscopy for the treatment of colorectal problems requiring surgery in older patients should receive serious consideration.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
In all Western industrialized countries, the constantly changing age pyramid with a growing proportion of elderly and old persons is giving rise to much discussion about medical services. The elderly/old patient also keeps cropping up in discussions about basic therapeutic/surgical measures.
We now have more than 10 years of experience in the field of laparoscopic colorectal surgery, and the feasibility of numerous different procedures has been demonstrated.
Against the above-mentioned background of the universal and extensive use of laparoscopic colorectal surgery, the question arises as to whether, in a large population of patients, differences are to be found between younger and older patients with regard both to the indication spectrum and intra- and postoperative complications.
Materials and methods
Since 1 September 1995, hospitals in Germany, Austria, Switzerland and Italy (currently 105 in all) have been recording the data of all those consecutive patients in whom a laparoscopic colorectal intervention was performed or initiated (intention-to-treat principle). The data are collected by the respective hospital using appropriate forms and are then sent to the study centre, where they are examined for plausibility and completeness and entered into an SPSS data bank by the staff of the Institute for Quality Control in Operative Medicine (An-Institute) at the Otto-von-Guericke University of Magdeburg. The specific analysis of the data is then effected using the statistical applications of the SPSS programme.
Statistical examination for significance of the individual parameters for the different age groups is then done with the chi-square test and the two-sided Fisher’s exact test. A p value of <0.05 was taken to be significant.
Following the practice of numerous authors, the cut-off point between younger and older patients was, for this analysis, selected to be 75 years [4, 9, 10, 13, 15].
Results
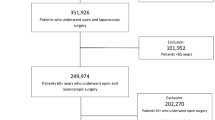
During the observation period, the data of a total of 4823 patients from 69 of the participating hospitals were checked for completeness and plausibility, entered into the data bank and analysed. Breakdown by age revealed 909 patients (18.8%) older than 75 years and 3914 patients (81.2%) younger than 75 years.
The analysis of the spectrum of procedures in both age groups revealed highly significant differences for two indication groups. Although the older patients had a clearly disproportionately higher number of malignant diseases (statistically significant for both colon and rectal carcinomas, but also for prolapse), the younger patients had a statistically significant preponderance of inflammatory bowel diseases (diverticulitis, Crohn’s disease, ulcerative colitis). Equal distributions were observed only for adenomas and the less common indications for surgery (Table 1).
With regard to the course of the operation, no age-specific differences were to be found. The rates of conversion to an open procedure [58 (6.4%) for patients >75 years vs 226 (5.8%) for patients <75 years; n.s.], as also that of intraoperative complications were distributed equally in both groups (Table 2). Nor did an analysis of the individual complications reveal significant differences for any of the various complications, irrespective of the procedure involved, between older and younger patients. An analysis of the postoperative complications of the overall population revealed a highly significant statistical difference between the two age groups for virtually all of the individual complications (Table 3). This significant difference between older and younger patients, favouring the latter, was also observed for postoperative mortality [37 (4.1%) for patients >75 years vs 27 (0.7%) for patients <75 years; p<0.001]. This led logically to the question as to whether a selective consideration of individual typically commonly performed procedures would also reveal this obvious difference in postoperative morbidity and mortality.
A subgroup analysis of postoperative complications and mortality was then performed for the most common diseases (sigmoid diverticulitis, curatively operated sigmoid carcinoma, curatively operated rectal carcinoma) in both groups.
For all three comparisons the results were identical, the older patients always had a statistically significantly higher rate of general complications (pneumonia, cardiopulmonary diseases, urinary tract infection). An analysis of postoperative mortality also showed a higher rate for the older patients (Table 4). No significant difference was found for complications directly associated with the procedure and necessitating re-operation (bleeding, anastomotic leak, postoperative ileus). This also applied to the surgical complications that were treatable by conservative means (Tables 5, 6, and 7). The sole deviation from this situation was a significant increase in the number of older patients with postoperative ileus requiring re-operation after surgery for diverticulitis.
Discussion
The changing age structure of the population in the industrialized countries resulting in an ever larger proportion of elderly and old persons has focused more attention on this age group. This development, in combination with ever improving diagnostic procedures and demands for comprehensive care, has led to the fact that hospitalized patients are becoming ever older. This applies in equal measure to the indication for colorectal interventions.
Despite the reported appreciably more common multimorbidity in patients older than 75 or 80 years, and the higher rate of postoperative complications [1–3, 5], there is a general consensus that advanced age is in itself not a contraindication for colorectal surgery [5, 6, 8–10, 12]. It is however obvious that the establishment of the indication for a particular procedure must be more strictly applied [7, 21]. As a logical result of this, there has been a shift in the indication spectrum towards life-saving procedures, that is, in which there is an absolute necessity for taking action. This compulsion to act applies in the case of cancer and, to a relatively lesser degree, to diseases with a major impact on the patient’s quality of life, such as rectal prolapse. This shift in the indication spectrum was also to be observed in our own patient population in which there was a significantly higher percentage of cancer cases, and also patients with prolapse in the older patient group. Elective operations such as those for recurrent diverticulitis, in contrast, decreased significantly. This phenomenon was also reported by Schwandner et al. [19]. This picture is certainly not due to selection; rather, the differences in the incidence of the various indications can be explained by a variation in the prevalence of the individual diseases in the different age groups. The sole exception here is cancer, in which the higher rate of surgery in the older patients is possibly due to the fact that the age-related general reservations against curative colorectal surgery in the old patient with an associated limited life expectancy recede somewhat into the background.
An analysis of the complications consistently shows that intraoperative complications are no more frequent in the older patient than in the younger patient. This observation was confirmed not only by us, but also by Schwandner et al., Payne et al., Poon et al. and the Colorectal Cancer Collaborative Group [5, 15, 16, 19]. A plausible explanation for this observation is the fact that the intervention is not tailored to the individual age of the patient, but that a standardized procedure, for example, for the treatment of colorectal carcinoma, can be performed, with no compromising of quality, in the elderly patient, too.
In addition, with regard to the postoperative surgical complications, the consensus of opinion is that the specific problems directly associated with the surgical procedure are not increased by advanced age. This applies equally to all specific complications (ileus, transit disorders, wound healing disturbances, afterbleeds) as also to anastomotic leaks [5, 14–16, 21]. The reports in the literature thus clearly support the results of our own study. The sole, and thus highly relevant, difference between the younger and older age groups is in preoperative comorbidity. Older patients have a clearly increased rate of accompanying diseases of every kind [1, 2, 11, 14, 21]. Of these, cardiopulmonary and respiratory diseases occupy a central position [1, 2, 5, 11, 14, 15, 19]. In the opinion of the above-mentioned authors, these accompanying diseases are the underlying basis for the general postoperative morbidity. It therefore follows that patients with a higher rate of accompanying diseases must also have a higher rate of general complications. This has proved to be the case in the patients investigated in the Study Group Laparoscopic Colorectal Surgery, as also, in identical manner, in other patient groups investigated [2, 5, 7, 14, 21].
There is also a general consensus of opinion that laparoscopic colorectal procedures can be carried out with good intraoperative and postoperative complication rates in older patients too [17, 21]. In particular, in comparison with the open approach, laparoscopic procedures appear to have clear postoperative advantages due to the modified access in colorectal disease. Thus, Peters, reporting on 108 patients older than 65 years, observed a clear advantage for the laparoscopic approach, particularly with regard to hospitalization [17]. In 72 patients older than 60 years, Reissman, too, reported a definitive advantage of the laparoscopic approach with regard to postoperative ileus and hospital stay [18]. This advantage of laparoscopy is almost certainly a contributory reason why, in his patient population, Schwandner, like us in the Study Group Laparoscopic Colorectal Surgery, observed a clear shift in the indications [19]. As a result of this shift, the younger patients more frequently presented with inflammatory bowel diseases (Crohn’s disease, ulcerative colitis, recurrent sigmoid diverticulitis), whereas the older patients more frequently had pelvic problems and colorectal cancer. This observation, however, also appears to confirm that in cancer patients, the generally observed reservations against curative colorectal surgery on account of the advanced age of the patients and their associated limited life expectancy appear to fade into the background, and that these patients, in particular—presumably also on account of its advantages in terms of postoperative course—preferentially receive a laparoscopic procedure [7, 20, 21].
References
Adloff M, Ollier JC, Schloegel M, Arnaud JP (1993) Colorectal cancer in patients over the age of 80 years. Ann Chir 47:492–496
Arnaud JP, Schloegel M, Ollier JC, Adloff M (1991) Colorectal cancer in patients over 80 years of age. Dis Colon Rectum 34:896–898
Avital S, Kashtan H, Hadad R, Werbin N (1997) Survival of colorectal carcinoma in the elderly. A prospective study of colorectal carcinoma and a five-year follow-up. Dis Colon Rectum 40:523–529
Bader TF (1986) Colorectal cancer in patients older than 75 years of age. Dis Colon Rectum 29:728–732
Colorectal Cancer Collaborative Group (2000) Surgery for colorectal cancer in elderly patients: a systematic review. Colorectal cancer collaborative group. Lancet 356:968–974
Damhuis RA, Wereldsma JC, Wiggers T (1996) The influence of age on resection rates and postoperative mortality in 6457 patients with colorectal cancer. Int J Colorectal Dis 11:45–48
Delgado S, Lacy AM, Garcia Valdecasas JC, Balague C, Pera M, Salvador L, Momblan D, Visa J (2000) Could age be an indication for laparoscopic colectomy in colorectal cancer? Surg Endosc 14:22–26
Edna TH, Bjerkeset T (1998) Colorectal cancer in patients over 80 years of age. Hepatogastroenterology 45:42–45
Fabre JM, Rouanet P, Ele N, Fagot H, Guillon F, Deixonne B, Balmes M, Domergue J, Baumel H (1993) Colorectal carcinoma in patients aged 75 years and more: factors influencing short and long-term operative mortality. Int Surg 200–203
Hessman O, Bergkvist L, Strom S (1997) Colorectal cancer in patients over 75 years of age—determinants of outcome. Eur J Surg Oncol 23:13–19
Houry S, Amenabar J, Rezvani A, Huguier M (1994) Should patients over 80 years old be operated on for colorectal or gastric cancer? Hepatogastroenterology 41:521–525
Kemeny MM, Busch-Devereaux E, Merriam LT, O’Hea BJ (2000) Cancer surgery in the elderly. Hematol Oncol Clin North Am 14:169–192
Makela JT, Kiviniemi H, Laitinen S (2000) Survival after operations for colorectal cancer in patients aged 75 years or over. Eur J Surg 166:473–479
Marusch F, Koch A, Schmidt U, Rhode S, Koeckerling F, Gastinger I, Lippert H (2003) Die Bedeutung des Alters für die frühpostoperativen Ergebnisse in der Chirurgie des kolorektalen Karzinoms. In: Köckerling F (ed) Komplikationen in der kolorektalen Chirurgie. Sperber Science Med, Hannover
Payne JE, Chapuis PH, Pheils MT (1986) Surgery for large bowel cancer in people aged 75 years and older. Dis Colon Rectum 29:733–737
Poon RT, Law WL, Chu KW, Wong J (1998) Emergency resection and primary anastomosis for left-sided obstructing colorectal carcinoma in the elderly. Br J Surg 1539–1542
Roseano M, Eramo R, Tonello C (1997) Evaluation of the surgical risk and preparation to major surgical intervention in geriatric surgery. Ann Ital Chir 68:67–72
Sargent DJ, Goldberg RM, Jacobson SD, Macdonald JS, Labianca R, Haller DG, Shepherd LE, Seitz JF, Francini G (2001) A pooled analysis of adjuvant chemotherapy for resected colon cancer in elderly patients. N Engl J Med 345:1091–1097
Schwandner O, Schiedeck TH, Bruch HP (1999) Advanced age—indication or contraindication for laparoscopic colorectal surgery? Dis Colon Rectum 42:356–362
Stewart BT, Stitz RW, Lumley JW (1999) Laproscopically assisted colorectal surgery in the elderly. Br J Surg 86:938–941
Uccheddu A, Cois A, Dessena M, Gromo C, Cagetti M (1994) Colorectal cancer in old age. Our experience. Minerva Chir 49:1215–1220
Acknowledgements
This study was supported by Ethicon Endosurgery, Norderstedt, Germany, and Takeda Pharma, Aachen, Germany.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Scheidbach, H., Schneider, C., Hügel, O. et al. Laparoscopic surgery in the old patient: do indications and outcomes differ?. Langenbecks Arch Surg 390, 328–332 (2005). https://doi.org/10.1007/s00423-005-0560-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00423-005-0560-9