
Abstract
Purpose
This study compared cardio-pulmonary responses between incremental concentric and eccentric cycling tests, and examined factors affecting the maximal eccentric cycling capacity.
Methods
On separate days, nine men and two women (32.6 ± 9.4 years) performed an upright seated concentric (CON) and an eccentric (ECC) cycling test, which started at 75 W and increased 25 W min−1 until task failure. Gas exchange, heart rate (HR) and power output were continuously recorded during the tests. Participants also performed maximal voluntary contractions of the quadriceps (MVC), squat and countermovement jumps.
Results
Peak power output was 53% greater (P < 0.001, g = 1.77) for ECC (449 ± 115 W) than CON (294 ± 61 W), but peak oxygen consumption was 43% lower (P < 0.001, g = 2.18) for ECC (30.6 ± 5.6 ml kg min−1) than CON (43.9 ± 6.9 ml kg min−1). Maximal HR was not different between ECC (175 ± 20 bpm) and CON (182 ± 13 bpm), but the increase in HR relative to oxygen consumption was 33% greater (P = 0.01) during ECC than CON. Moderate to strong correlations (P < 0.05) were observed between ECC peak power output and CON peak power (r = 0.84), peak oxygen consumption (r = 0.54) and MVC (r = 0.53), while no significant relationships were observed between ECC peak power output and squat as well as countermovement jump heights.
Conclusion
Unexpectedly, maximal HR was similar between CON and ECC. Although ECC power output can be predicted from CON peak power output, an incremental eccentric cycling test performed after 3–6 familiarisation sessions may be useful in programming ECC training with healthy and accustomed individuals.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Eccentric cycling was first introduced in a scientific journal in 1952 and repetitively confirmed that the metabolic load is lower during eccentric than concentric cycling at the same power output (Abbott et al. 1952; Dufour et al. 2004; Peñailillo et al. 2013). Several studies have since shown the potent effects of eccentric cycling training on muscle function and strength (Lastayo et al. 1999; LaStayo et al. 2000; Leong et al. 2013). With several review papers highlighting the importance of low-intensity, high volume eccentric exercise (LaStayo et al. 2013; Hoppeler and Herzog 2014; Hoppeler 2016), and more eccentric cycling and stepping ergometers available on the market, it is probable that eccentric cycling training will become more popular. Thus, it is necessary to establish a protocol to determine eccentric cycling capacity, and to safely and effectively prescribe eccentric cycling to different populations.
Several studies have examined cardio-pulmonary responses to continuous eccentric cycling, and shown greater increases in cardiac output (Thomson 1971) and heart rate (Knuttgen et al. 1971; Hesser et al. 1977) for any oxygen consumption, when compared with concentric cycling at low intensities. Furthermore, two studies have examined physiological responses during an incremental eccentric cycling protocol (Dufour et al. 2004; Lechauve et al. 2014). In both studies power output during eccentric cycling was increased until participants reached the maximal power output achieved during concentric cycling. As a result participants achieved only 256–330 W at a heart rate of 106.5–117 bpm during eccentric cycling. The later indicate that volitional exhaustion and maximal eccentric cycling performance were clearly not achieved, thus not providing any information about unique characteristics of maximal eccentric cycling capacity. To the best of our knowledge, no previous research has examined the potentially unique physiological responses to eccentric cycling until exhaustion, and as such little is known with regards to the factors that limit maximal eccentric cycling capacity.
Previous studies that examined the effectiveness of eccentric cycling exercise training set the intensity based on maximal heart rate or age-predicted heart rate (LaStayo et al. 2000; Elmer et al. 2012), peak power output (Mueller et al. 2009; Leong et al. 2013) or rating of perceived exertion (RPE) (Flann et al. 2011; Laroche et al. 2013) measured during an incremental concentric cycling test to task failure. Despite the uniquely low metabolic load of eccentric cycling at submaximal intensities, all previous studies have prescribed eccentric cycling training based on the information from a concentric cycling test. It may be that an incremental eccentric cycling test to task failure provides more information on the factors limiting eccentric cycling capacity, and that peak power output obtained from an eccentric cycling test is more specific for eccentric cycling prescription. For a comprehensive understanding of the performance during an eccentric cycling test, factors that determine peak power output should also be considered. However, we are not aware of any studies that have examined factors limiting eccentric cycling performance.
Conversely, possible factors limiting exercise capacity during maximal concentric cycling have been well documented. Maximal aerobic capacity and peak power output during incremental concentric cycling are typically limited by oxygen delivery and/or oxygen utilisation (Wisløff et al. 2007; Gibala and Jones 2013). Based on these factors, several submaximal tests have been designed to estimate maximal exercise capacity during concentric cycling and other exercise modes (Coquart et al. 2016; Cornelis and Buys 2016). Given the low metabolic cost and greater work achievable during eccentric cycling, it is plausible that peak power output during an eccentric cycling test is more closely associated with neuromuscular rather than cardiovascular function. Neuromuscular function and fatigue have been assessed before and after eccentric exercises by measuring maximal voluntary isometric contraction (MVC) strength (LaStayo et al. 2000; Franchi et al. 2014) or squat and countermovement jumps (Cormie et al. 2010; Bridgeman et al. 2016). Since these measurements have been shown to improve following eccentric exercise training (Sheppard et al. 2008; de Hoyo et al. 2015), they may correlate better with peak power output during incremental eccentric cycling.
Therefore, the present study compared physiological responses (oxygen consumption, minute ventilation, tidal volume, breathing frequency, and heart rate) in relation to power output between an incremental eccentric versus concentric cycling test. Relationships between peak power during eccentric cycling and peak oxygen consumption and peak power output during concentric cycling, MVC torque of the knee extensors, countermovement and squat jump height and their ratio were investigated. The first hypothesis tested was that peak oxygen consumption, minute ventilation, tidal volume, breathing frequency, and peak heart rate at task failure of an incremental cycling test would be greater during concentric than eccentric cycling, while peak power output would be greater during eccentric cycling. The second hypothesis tested was that MVC torque of the knee extensors, countermovement jump height and the countermovement to squat jump ratio would be strong predictors of peak power during eccentric cycling.
Methods
Participants
This study was approved by the institutional human research ethics committee before commencing the research. Eleven healthy men (n = 9) and women (n = 2) were recruited for the study, and their average ± standard deviation (SD) age, height and body mass were 33 ± 9 years, 181.4 ± 8.2 cm, and 81.1 ± 17.1 kg, respectively. They were physically active and/or training recreationally in cycling, cricket or volleyball, but had not performed any specific eccentric exercise beyond those in normal daily activities (i.e., downstairs/downhill walking, sitting down) in the 6 months prior to the study. Participants were not taking any medication and did not have any history of lower limb musculoskeletal injuries. They refrained from exercise, alcohol and caffeine in the 48 h prior to each testing session. They were fully informed of the requirements and risks associated with the study and provided written informed consent before participation. The sample size was estimated using the heart rate data from a previous study (Peñailillo et al. 2013) in which heart rate was compared between eccentric and concentric cycling at submaximal intensities. It was assumed that the difference in heart rate at task failure would be smaller than at submaximal intensities. Thus, based on G*Power (Version 3.0.10, 2008, Kiel, Germany), the effect size was estimated to be 0.9, with an α level of 0.05 and a power of 0.8 (1 − β), it was found that ten participants would suffice.
Study design
For this study participants visited the laboratory on five separate occasions. During the first visit participants performed a concentric cycling test. On the following three visits, participants performed 5, 8 and 10 min of practise continuous eccentric cycling at 30, 30 and 40% of their concentric peak power output, respectively. During the three practise (familiarisation) sessions, cadence was set at 60 rpm and the bike operated in isokinetic mode. These sessions were specifically designed and performed to provide a repeated bout effect without major increases in indirect markers of muscle damage and soreness (Peñailillo et al. 2013). Measurements of MVC knee extension torque and squat and countermovement jump heights were taken before each eccentric cycling session. Before the final session for this study, participants participated in five further separate sessions of interval and continuous eccentric cycling. As no previous study has investigated maximal eccentric cycling performance, these additional eccentric cycling sessions guaranteed that the participants were well familiarised and could reach a “true” maximal eccentric cycling performance. During the last visit to the laboratory participants performed the incremental eccentric cycling test to task failure.
Incremental concentric and eccentric cycling tests
The concentric and eccentric cycling tests were performed in an upright position and the seat height of the ergometers described below was adjusted to the comfort of each participant (a slight bend of the knee joint at knee extension). Prior to the incremental concentric and eccentric cycling tests, participants completed a 3-min warm-up between 50 and 120 W at 60 rpm. Both concentric and eccentric protocols begun at 75 W and increased by 25 W every minute until the participants could no longer cycle at a target power output. The concentric cycling test was performed on an electromagnetically braked cycling ergometer (Velotron, RacerMate, Inc., Seattle, WA, USA) and the eccentric cycling test was performed on an eccentric cycling ergometer (Cyclus2 Eccentric Trainer, RBM Elektronik-Automation GmbH, Leipzig, Germany).
Power output during the concentric and eccentric cycling tests were automatically controlled by the ergometers with the electromagnetic brake during the concentric test (Abbiss et al. 2009) and the motor during the eccentric test. The resistance was adjusted based on cadence of participants. Participants were able to self-select their cadence during the concentric cycling test, with the average cadence during this trial being a target cadence for the eccentric cycling test. The concentric cycling test was terminated when the cadence dropped below 60 rpm for more than 30 s. Given the participants are required to resist against the motor during eccentric cycling, the test was terminated when increased 10 rpm above the target for more than 30 s. During both incremental cycling tests, participants were provided with visual feedback on their power output, cadence and elapsed time. Verbal encouragement was provided during the final stages of both incremental tests.
Expired gases were measured each breath by a TrueOne 2400 metabolic cart (ParvoMedics, Sandy, UT, USA) and averaged every 15 s. Peak oxygen consumption (VO2peak) was taken as the highest value in any 15-s interval. The gas analyser and ventilometer were calibrated before each test using gases of known concentrations and a 3-l syringe (5530 series, Hans Rudolph, Inc., Shawnee, KS, USA). Minute ventilation (VE), tidal volume (Vt) and breathing frequency (Bf) at the task failure were analysed as the average values of 1 min of each protocol. Heart rate was recorded during cycling and measured every 5 s (S610, Polar, Finland). Due to the expected greater power output during eccentric cycling in comparison to concentric cycling, it was assumed that the eccentric protocol will last significantly longer. To avoid the influence of the greater exercise time on the cardio-pulmonary parameters, the analysis of heart rate (HR) relative to oxygen consumption (VO2) was normalised for stages completed. Thus, an average heart rate was calculated for every 10% of exercise time for each condition. To compare between conditions a linear regression that was based on the ten averages was computed and the difference in the slope of both regressions was determined using the provided function in the GraphPad statistical package (Prism version 7.02, GraphPad Software, La Jolla, CA, USA). The slope of the linear regressions was also compared between conditions for the relationship of HR and VO2 to power output. This comparison was averaged for each stage during the incremental test, not for 10% of exercise time like for HR over VO2. Furthermore, the relationship for HR and VO2 over power output for each stage was only computed until the average peak power output achieved during each condition. Selected participants were able to achieve much higher peak power output at task failure.
MVC knee extension torque
Maximal voluntary isometric contractions of the right knee extensors at 70° knee angle were performed on a custom made chair with a load cell (Xtran S1W, Applied Measurements, Melbourne, Australia) to measure knee extensor muscle strength as previously reported (Peñailillo et al. 2014). Participants performed a 5 min warm-up on a cycling ergometer (Monark 828E, Monark Exercise AB, Vansbro, Sweden) at 15% of their concentric peak power output at 60 rpm prior to the measure. Participants then performed three submaximal isometric knee extensions for 3 s at 50, 50 and 80% of a maximal effort, separated by a 1-min passive rest. A total of three 3 s maximal isometric knee extensions were performed, separated by a 1-min passive rest. Participants were advised to contract as fast and as hard as possible. Trials with any countermovement were disregarded and repeated. The torque output was shown on a computer screen, and torque data was sampled at a frequency of 1000 Hz and a digital zero-phase lag finite impulse response low-pass filter with a cut-off frequency of 14 Hz was applied. The trial with the greatest peak torque value was used for further analysis. Verbal encouragement was provided during the measurements.
Squat and countermovement jump
Jump height was measured via a digital vertical jump meter (Vertical Jump Meter T.K.K. 5406, JUMP-MD, Takei Scientific Instruments Co. Ltd., Japan). Participants performed all jumps with hands placed on their hips and a self-chosen squat depth with less than 90° knee flexion. For the squat jumps (SJ), participants were asked to squat down to the depth of their choice, remain in the squat position for 3 s and then jump without any countermovement. For the countermovement jump (CMJ) participants were asked to jump as high as possible from an upright standing position on a count of three. Verbal encouragement was provided before and during both jumps.
Statistical analyses
Data are reported as mean ± SD. Peak values (pulmonary parameters and power output) were compared between concentric and eccentric cycling using paired t tests. Effect size for the difference in the dependent variables between concentric and eccentric cycling was calculated by Hedges’ g (Hedges 1981). The slope of the linear regression calculated for the relationships between HR and VO2, VO2 and peak power output, and HR and peak power output was used to compare differences in these relationships between conditions. Pearson’s correlations were used to assess the relationship between peak power output during eccentric cycling and VO2peak and peak power output during concentric cycling, MVC torque of the knee extensors, countermovement and squat jump heights. Significance was set at P < 0.05 and all statistical analyses were performed using GraphPad statistical package (Prism version 7.02, GraphPad Software, La Jolla, CA, USA).
Results
Heart rate, oxygen consumption and power output during incremental tests
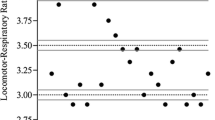
Figure 1 shows changes in heart rate and oxygen consumption during the concentric and eccentric incremental cycling test. The slope of the linear regression for heart rate over power output was not different (P = 0.276) between the eccentric (0.26 ± 0.03) and concentric (0.23 ± 0.01) tests. In contrast, the slope of the linear regression of oxygen consumption over power output was greater (P < 0.0001) for the concentric (0.13 ± 0.004) than the eccentric test (0.047 ± 0.002). As shown in Fig. 2, heart rate relative to oxygen consumption was greater during eccentric than concentric cycling, and the linear regression line was steeper (P = 0.01) for eccentric (3.99 ± 0.30) than concentric cycling (2.99 ± 0.19).

Comparison between concentric (CON) and eccentric cycling (ECC) for changes in heart rate (a) and oxygen consumption (b) over incremental power output stages from 75 W to the average peak power output among participants (CON: 300 W, ECC: 450 W). It should be noted that some participants were able to achieve much higher peak power output at task failure, thus the heart rate and oxygen consumption values shown in the figures are not peak values. *: significant (P < 0.01) difference between the slope of the linear regression for ECC and CON

Comparison between concentric (CON) and eccentric cycling (ECC) for the relationship between heart rate and oxygen consumption normalised by total exercise time in steps of 10%. The vertical bar for the SD of the last data point of ECC is not visible as its size is smaller than the chosen symbol size. *: significant (P < 0.01) difference between the slope of the linear regression for ECC and CON
Comparison of peak values at task failure
Peak power output was greater (P < 0.001; g = 1.77) during eccentric cycling (449 ± 115 W) compared with concentric cycling (294 ± 61 W) (Fig. 3a). The peak power output was 53% greater for eccentric than concentric cycling in average, but the power difference between eccentric and concentric cycling varies among the participants (Fig. 3b). As shown in Fig. 3c, d, maximal heart rate was not different (P = 0.21; g = 0.43) between concentric (182 ± 13 bpm) and eccentric cycling (175 ± 20 bpm). Peak oxygen consumption was lower (P < 0.001; g = 2.18) for eccentric (30.6 ± 5.6 ml kg−1 min−1) than concentric cycling (43.9 ± 6.9 ml kg−1 min−1) (Fig. 3e). The average peak oxygen consumption was 43% lower during eccentric than concentric cycling, yet a large variability in the magnitude of difference among participants was evident (Fig. 3f).

Comparison between eccentric (ECC) and concentric (CON) cycling for peak power output (a), maximal heart rate (c) and peak oxygen consumption (e) in the incremental tests, and the difference between ECC and CON for each variable is shown in b, d, and f, respectively. For each figure, individual data, and the average (long line) and ± 1SD (short lines) of 11 participants shown. P values based on t test and effect size (g) for the comparison between ECC and CON are shown
VE (P = 0.0008, g = 1.89; Fig. 4a) and Vt (P < 0.0001, g = 2.53; Fig. 4c) at task failure were lower for eccentric cycling (65 ± 22 l.min−1; 1.8 ± 0.4 l) than concentric cycling (110 ± 28 l.min−1; 2.8 ± 0.4 l). On average, VE was 41% lower (Fig. 4b) and Vt was 37% lower (Fig. 4d) for eccentric than concentric cycling. However, Bf was not different (P = 0.07, g = 0.74) between eccentric and concentric cycling. The comparison of pulmonary parameters at 50% peak power output during each condition (221 ± 51 W during eccentric cycling versus 149 ± 30 W during concentric cycling) showed that VE and Vt were lower (P < 0.01) during eccentric than concentric cycling, but breathing frequency was not different between conditions (P = 0.393).

Comparison between eccentric (ECC) and concentric (CON) cycling for minute ventilation (a), tidal volume (c) and breathing frequency (e) in the incremental tests, and the difference between ECC and CON for each variable is shown in b, d, and f, respectively. For each figure, individual data, and the average (long line) and ± 1SD (short lines) of 11 participants shown. P values based on t test and effect size (g) for the comparison between ECC and CON are shown
Correlation between peak eccentric cycling power and other variables
Figure 5 shows correlations between eccentric cycling peak power and other variables. Eccentric peak power was significantly correlated with peak oxygen consumption and peak power during concentric cycling, and isometric peak force of the knee extensors. Peak oxygen consumption explained 30% (P = 0.0839, r = 0.54, R2 = 0.295, Fig. 5a), peak power output during concentric cycling explained 71% (P = 0.0011, r = 0.84, R2 = 0.71, Fig. 5b) and isometric peak force of the knee extensor explained 28% (P = 0.0929, r = 0.53, R2 = 0.28, Fig. 5c) of the variance of peak power output during eccentric cycling. However, countermovement jump height (P = 0.9281, r = 0.03, R2 = 0.001, Fig. 5d), squat jump height (P = 0.8566, r = 0.06, R2 = 0.004, Fig. 5e) and the ratio between the two (P = 0.8343, r = 0.06, R2 = 0.003, Fig. 5f) did not explain the variance for peak power output during eccentric cycling.

Correlations between peak power output during eccentric cycling and peak oxygen consumption during concentric cycling (a), concentric peak power output (b), MVC torque of the knee extensors (c), countermovement jump height (d), squat jump height (e), and countermovement to squat jump height ratio (f). The dotted lines represent the 90% confidence intervals
Discussion
The present study compared heart rate, pulmonary parameters and power output between incremental eccentric and concentric cycling tests to task failure. As expected, oxygen consumption during the eccentric test was lower than that of the concentric test for all stages, and heart rate was lower during submaximal stages for eccentric than concentric cycling (Fig. 1). However, peak heart rate was the same between eccentric and concentric cycling tests, and the slope of the linear regression calculated from the relationship between heart rate and oxygen consumption was 25% greater during eccentric than concentric cycling (Fig. 2). Peak oxygen consumption was 43% smaller, while peak power output was 53% greater for the eccentric than concentric test (Fig. 3). Minute ventilation and tidal volume were 41 and 36% lower during eccentric cycling than concentric cycling at task failure, but breathing frequency showed no difference between modalities (Fig. 4). Interestingly, eccentric peak power output was strongly correlated with concentric peak power, while correlations with concentric VO2peak and MVC strength were moderate (Fig. 5). In contrast to the hypothesis, no significant relationships were observed between eccentric peak power output and countermovement or squat jump heights.
Previous research on a similar cohort of participants and using similar incremental concentric cycling tests to that of the present study have shown comparable values of peak power output, peak heart rate and peak oxygen consumption to those of the present study (Pfeiffer et al. 2005; Cornelis and Buys 2016). Thus, the values obtained in the incremental concentric cycling test of the present study appear to be typical. The average peak power output obtained in the incremental eccentric cycling test (450 W) was 1.5 times greater of that in the incremental concentric cycling test and approximately half of the peak value (~ 1000 W) previously reported during sprint eccentric cycling (Brughelli and Van Leemputte 2013). It should be noted that in the present study eccentric cycling was performed incrementally and with the ergometer set to an isopower mode. In the isopower mode, the cadence is variable and the ergometer adjusts the velocity based on the participants torque production to maintain the pre-set power output. Performing eccentric cycling at a constant cadence in isokinetic mode (Brughelli and Van Leemputte 2013) appears to lead to a greater variation in the power output produced in comparison to the isopower mode. Interestingly, the mean power output (~ 500 W) achieved during the 6 s sprints at 60 rpm in the study by Brughelli and Van Leemputte (2013) was very similar to the average eccentric peak power obtained in the present study. Clearly, further research is needed to better understand the influence of both cadence and the exercise duration on peak eccentric power outputs.
The lower oxygen consumption and heart rate observed during eccentric cycling for the same power output as that of concentric cycling (Fig. 1) are in line with the findings of previous studies (Abbott et al. 1952; Dufour et al. 2004; Peñailillo et al. 2013). When the peak power was achieved in the eccentric test, oxygen consumption was 61–95% of the peak values obtained in the concentric test, and minute ventilation and tidal volume were also 23–94% of the peak values in the concentric cycling, but the heart rate was similar (Figs. 3, 4). The present study is the first to show that both exercise modes lead to similar maximal heart rates at task failure. Additionally, there was a 25% greater increase in heart rate relative to oxygen consumption during eccentric cycling than concentric cycling (Fig. 2). Importantly, the relationship shown in Fig. 2 is normalised for time between conditions, so that every data point represents an average for 10% of exercise time. Therefore, the relationship shows that despite differences in exercise time resulting from the specific protocols used, greater increases in HR occur relative to VO2 during eccentric than concentric cycling. Furthermore, these increases occurred over more stages during eccentric compared with concentric cycling, and thus the same heart rate and oxygen consumption was maintained over a greater range of power outputs. For example, 50% of the eccentric peak power output resulted in a heart rate of 116 ± 30 bpm, which is similar to 115 ± 23 bpm observed at only 30% of the concentric peak power output. At these heart rates oxygen consumption was lower during eccentric cycling (14.7 ± 2.4 ml kg−1 min−1), than concentric cycling (21.3 ± 3 ml kg−1 min−1). Such differences in the relationship between HR and VO2 during concentric and eccentric cycling has previously been reported during submaximal exercise (Dufour et al. 2004; Lechauve et al. 2014). However, this is the first study to show that this difference increases with increasing intensity (Fig. 2). Based on these findings, heart rate zones determined from an incremental concentric cycling test to task failure should not be used to directly prescribe training during eccentric cycling. Preferably, exercise intensity during eccentric cycling should be prescribed from the power outputs achieved specifically during an eccentric cycling test. Although the calculations in this study were successful at normalising for differences in total exercise time, future studies should considered comparing shorter incremental eccentric tests where participants start at a greater intensity to decrease potential influences of exercise time and accumulated fatigue on cardio-pulmonary parameters.
The similar maximal heart rate between the concentric and eccentric incremental cycling tests may be explained by a combination of several factors including differences in thermogenesis, body position, breathing frequency, and recruited muscle mass. It is plausible that greater heat production during eccentric contractions (Nadel et al. 1972) as a result of the high mechanical load required to achieve the high power outputs, may have increased thermal strain leading to an increase in heart rate within the present study. But this difference was found utilising a modification of the Krogh bicycle ergometer (Bonde-Petersen et al. 1973) that consisted of a recumbent seat. The current study used upright seated cycling that required the use of the upper body muscles to work against the bike and remain on the seat in comparison to the recumbent position. Although the differences between upright seated and recumbent eccentric cycling have not been previously investigated, it can be assumed that the back of the seat during the recumbent position will increase stability and generated reaction forces that will decrease the required eccentric force production of the agonist muscles. In that case, the performance during upright seated eccentric cycling is a more precise reflection of true eccentric strength and maximal eccentric cycling capacity as it does not benefit from the additional support. Moreover, breathing frequency was the only pulmonary parameter that was not significantly different between concentric and eccentric cycling at both 50% of peak power output and task failure (Fig. 4). Lechauve et al. (2014) have previously reported a greater breathing frequency during recumbent eccentric cycling than concentric cycling at the same oxygen consumption (2 l min−1), and stated that this could be due to limited increases in the end-inspiratory lung volume because of the required trunk stabilisation. It is also possible that the higher heart rate during eccentric compared with concentric cycling was associated with an increased input from peripheral mechanical (joints and muscles) and chemical receptors (metaboreceptors) (Amann et al. 2010). Further studies are necessary to investigate the mechanisms underpinning the similar maximal heart rate despite large differences in oxygen consumption and peak power output between the concentric and eccentric cycling tests.
It is interesting to note that 71% of the variance of the eccentric peak power output was explained by peak power output during concentric cycling (Fig. 4b). VO2peak during concentric cycling (Fig. 4a) and MVC torque of the knee extensors (Fig. 4d) were only moderately correlated to the eccentric peak power. In contrast to the hypothesis, countermovement and squat jump heights and their ratio had no significant correlation with eccentric peak power output (Fig. 5e, f). Eccentric cycling in this study was performed at a constant and uninterrupted cadence of at least 60 rpm, resulting in an angular velocity of approximately 180° s−1 at the knee. As the knee joint can reach a peak angular velocity of 860° s−1 during a countermovement jump (Bobbert et al. 1986), the countermovement to squat jump ratio (eccentric utilisation ratio) may not be able to characterise eccentric peak power output accordingly. Furthermore, this underlines the questionable assumption that the eccentric utilisation ratio is a valid representation of eccentric “ability”, “skill”, “capacity” or even eccentric strength. Performance during specific skills like jumps or changes of direction are affected by many different factors. Although eccentric strength or coordination could be a factor influencing performance during jumping, one should be careful when generalising relationships between various forms of exercises that include eccentric contractions.
Individuals with a greater concentric strength are able to produce more torque with decreasing concentric velocities and increasing eccentric velocities (Hortobágyi and Katch 1990). For concentrically stronger participants it might have been easier for them to resist an increase in speed of the pedals during the latter stages of the eccentric test. Indeed, with fatigue it would have become more difficult for the participants to resist the motor of the eccentric ergometer that increased the cadence to match the target power output, despite participants attempting to maintain the target cadence. Failure to generate large torque to maintain the target cadence at maximal intensities may be also related to an initial suboptimal cadence choice. It is plausible that optimal and freely chosen cadence may differ between eccentric and concentric cycling. Emanuele et al. (2012) reported that a freely chosen cadence during concentric cycling differed up to 20 rpm among individuals, and this depended on intensity and duration of the exercise. Additionally, the freely chosen cadence may be different from the energetically optimal cadence (Hansen and Smith 2009). Further research is needed to better understand the influence of cadence on eccentric cycling capacity. The moderate correlation between the MVC torque of the knee extensors and eccentric peak power output could be explained by the involvement of other muscles such as iliopsoas, gluteus, gastrocnemius and soleus during eccentric cycling (Elmer et al. 2010). It should be noted that electromyographic activity of the vastus lateralis was reduced after familiarisation to eccentric cycling (LaStayo et al. 2008), but the present study had several familiarisation sessions before the incremental eccentric cycling test.
As presented by the high power outputs achieved by the participants in the present study, the incremental maximal eccentric cycling test appears feasible and safe within this healthy population. However, when this test cannot be performed, other options to determine or estimate eccentric peak power output should be considered. This is especially important for the application of eccentric cycling to older adults and clinical populations. For instance, training intensity of eccentric cycling could be determined based on concentric peak power output, since the concentric peak power correlated reasonably well with the eccentric peak power output (Fig. 4b). Secondly, the efficacy of using submaximal HR, VO2 and power output to predict maximal eccentric cycling performance needs to be established, as has been done in concentric tasks (Coquart et al. 2016). Such submaximal protocols would be suitable for a wide range of populations and would make it easier to set up eccentric cycling protocols. Lastly, due to the novelty of the eccentric cycling in comparison to concentric cycling, which is learned from a young age, could increase the inter-individual differences. It is plausible to assume that participants with greater history of eccentric loading could perform better during eccentric cycling. For example, one participant had a 21% (40 bpm) lower HR and 43% (29 ml kg−1 min−1) lower oxygen consumption (Fig. 3D, E) during eccentric cycling, but reached only 36% greater power output (492 W) than during concentric cycling, which is clearly lower than the average increase of 53%. During concentric cycling he achieved 361 W with a VO2peak of 51 ml kg−1 min−1 (Figs. 1b, 3a), both above the average of the group. As his aerobic capacity was not limiting performance, other factors might: suboptimal eccentric coordination to apply his high isometric strength of 389.84 Nm (Fig. 5c) or a potentially lower stiffness in the muscle–tendon unit as indicated by a countermovement to squat jump height ratio of 1 (Fig. 5f). Specific prior eccentric loading and coordination (Mueller et al. 2009) was not determined in this study, but should be considered as a potential influence on performance outcomes during eccentric cycling in future studies.
In conclusion, this is the first study to present the cardio-pulmonary differences during eccentric and concentric cycling until volitational exhaustion. Although the differences in maximal power output and peak oxygen consumption have been previously reported for submaximal intensities, it is crucial to point out that none of the previous studies (Dufour et al. 2004; Lechauve et al. 2014) have investigated these differences during maximal intensities with accumulated fatigue until exhaustion. Especially the similar maximal heart rate was not expected based on findings from these previous studies investigating differences at submaximal intensities. It is known that such “all-out” intensities result in drastically different cardio-pulmonary responses during concentric exercise in comparison to submaximal intensities. Therefore, the effects of protocols conducted till exhaustion has to be studied during continuous eccentric cycling to truly understand potential maximal eccentric cycling capacity. Thus, the unique findings of the present study indicate that especially the relationship between heart rate and oxygen consumption per power output differ between incremental eccentric and concentric cycling tests till exhaustion. Furthermore, concentric peak power output was the best correlate with eccentric peak power output, but the individual variability in the magnitude of difference in peak parameters between eccentric and concentric cycling has to be considered. Thus, when prescribing eccentric cycle training, after an adequate amount of familiarisation sessions (3–6), an assessment of eccentric peak power from an incremental eccentric cycling test is recommended. The use of heart rate for eccentric cycling prescription requires some caution. Future research should investigate other incremental eccentric cycling test protocols including the effect of cadence on eccentric cycling performance, and set up a standardised protocol to determine eccentric cycling intensity for exercise prescription.
Abbreviations
- B f :
-
Breathing frequency
- CMJ:
-
Countermovement jump
- CON:
-
Incremental concentric cycling test
- ECC:
-
Incremental eccentric cycling test
- g :
-
Hedges’ g
- HR:
-
Heart rate
- MVC:
-
Maximal voluntary isometric contraction
- RPE:
-
Rating of perceived exertion
- SD:
-
Standard deviation
- SJ:
-
Squat jump
- VO2 :
-
Oxygen consumption
- VO2peak :
-
Peak oxygen consumption
- V E :
-
Minute ventilation
- V t :
-
Tidal volume
- VO2 :
-
Oxygen consumption
References
Abbiss CR, Quod MJ, Levin G et al (2009) Accuracy of the Velotron ergometer and SRM power meter. Int J Sports Med 30:107–112. https://doi.org/10.1055/s-0028-1103285
Abbott BC, Bigland B, Ritchie JM (1952) The physiological cost of negative work. J Physiol 117:380–390
Amann M, Blain GM, Proctor LT et al (2010) Group III and IV muscle afferents contribute to ventilatory and cardiovascular response to rhythmic exercise in humans. J Appl Physiol Bethesda Md 1985 109:966–976. https://doi.org/10.1152/japplphysiol.00462.2010
Bobbert MF, Mackay M, Schinkelshoek D et al (1986) Biomechanical analysis of drop and countermovement jumps. Eur J Appl Physiol 54:566–573. https://doi.org/10.1007/BF00943342
Bonde-Petersen F, Henriksson J, Knuttgen HG (1973) Effect of training with eccentric muscle contractions on skeletal muscle metabolites. Acta Physiol Scand 88:564–570. https://doi.org/10.1111/j.1748-1716.1973.tb05485.x
Bridgeman LA, McGuigan MR, Gill ND, Dulson DK (2016) Relationships between concentric and eccentric strength and countermovement jump performance in resistance trained men. J Strength Cond Res. https://doi.org/10.1519/JSC.0000000000001539
Brughelli M, Van Leemputte M (2013) Reliability of power output during eccentric sprint cycling. J Strength Cond Res Natl Strength Cond Assoc 27:76–82. https://doi.org/10.1519/JSC.0b013e31824f2055
Coquart J, Tabben M, Farooq A et al (2016) Submaximal, perceptually regulated exercise testing predicts maximal oxygen uptake: a meta-analysis study. Sports Med 46:885–897. https://doi.org/10.1007/s40279-015-0465-x
Cormie P, McGuigan MR, Newton RU (2010) Changes in the eccentric phase contribute to improved stretch-shorten cycle performance after training. Med Sci Sports Exerc 42:1731–1744. https://doi.org/10.1249/MSS.0b013e3181d392e8
Cornelis N, Buys R (2016) The effects of exercise modality on maximal and submaximal exercise parameters obtained by graded maximal exercise testing. Int J Cardiol 222:538–547. https://doi.org/10.1016/j.ijcard.2016.07.190
de Hoyo M, Pozzo M, Sañudo B et al (2015) Effects of a 10-week in-season eccentric-overload training program on muscle-injury prevention and performance in junior elite soccer players. Int J Sports Physiol Perform 10:46–52. https://doi.org/10.1123/ijspp.2013-0547
Dufour SP, Lampert E, Doutreleau S et al (2004) Eccentric cycle exercise: training application of specific circulatory adjustments. Med Sci Sports Exerc 36:1900–1906
Elmer SJ, Madigan ML, LaStayo PC, Martin JC (2010) Joint-specific power absorption during eccentric cycling. Clin Biomech Bristol Avon 25:154–158. https://doi.org/10.1016/j.clinbiomech.2009.10.014
Elmer S, Hahn S, McAllister P et al (2012) Improvements in multi-joint leg function following chronic eccentric exercise. Scand J Med Sci Sports 22:653–661. https://doi.org/10.1111/j.1600-0838.2011.01291.x
Emanuele U, Horn T, Denoth J (2012) The relationship between freely chosen cadence and optimal cadence in cycling. Int J Sports Physiol Perform 7:375–381. https://doi.org/10.1123/ijspp.7.4.375
Flann KL, LaStayo PC, McClain DA et al (2011) Muscle damage and muscle remodeling: no pain, no gain? J Exp Biol 214:674–679. https://doi.org/10.1242/jeb.050112
Franchi MV, Atherton PJ, Reeves ND et al (2014) Architectural, functional and molecular responses to concentric and eccentric loading in human skeletal muscle. Acta Physiol Oxf Engl 210:642–654. https://doi.org/10.1111/apha.12225
Gibala MJ, Jones AM (2013) Physiological and performance adaptations to high-intensity interval training. Nestlé Nutr Inst Workshop Ser 76:51–60. https://doi.org/10.1159/000350256
Hansen EA, Smith G (2009) Factors affecting cadence choice during submaximal cycling and cadence influence on performance. Int J Sports Physiol Perform 4:3–17
Hedges LV (1981) Distribution Theory for Glass’s Estimator of Effect size and Related Estimators. J Educ Stat 6:107–128. https://doi.org/10.3102/10769986006002107
Hesser CM, Linnarsson D, Bjurstedt H (1977) Cardiorespiratory and metabolic responses to positive, negative and minimum-load dynamic leg exercise. Respir Physiol 30:51–67
Hoppeler H (2016) Moderate load eccentric exercise; a distinct novel training modality. Exerc Physiol 7:483. https://doi.org/10.3389/fphys.2016.00483
Hoppeler HH, Herzog W (2014) Eccentric exercise: many questions unanswered. J Appl Physiol. https://doi.org/10.1152/japplphysiol.00239.2014
Hortobágyi T, Katch FI (1990) Eccentric and concentric torque-velocity relationships during arm flexion and extension. Eur J Appl Physiol 60:395–401. https://doi.org/10.1007/BF00713506
Knuttgen HG, Petersen FB, Klausen K (1971) Oxygen uptake and heart rate responses to exercise performed with concentric and eccentric muscle contractions. Med Sci Sports 3:1–5
Laroche D, Joussain C, Espagnac C et al (2013) Is it possible to individualize intensity of eccentric cycling exercise from perceived exertion on concentric test? Arch Phys Med Rehabil 94:1621.e1–1627.e1. https://doi.org/10.1016/j.apmr.2012.12.012
Lastayo PC, Reich TE, Urquhart M et al (1999) Chronic eccentric exercise: improvements in muscle strength can occur with little demand for oxygen. Am J Physiol 276:R611-615
LaStayo PC, Pierotti DJ, Pifer J et al (2000) Eccentric ergometry: increases in locomotor muscle size and strength at low training intensities. Am J Physiol Regul Integr Comp Physiol 278:R1282-1288
LaStayo P, Pifer J, Pierotti D, Lindstedt S (2008) Electromyographic adaptations elicited by submaximal exercise in those naive to and in those adapted to eccentric exercise: a descriptive report. J Strength Cond Res 22:833–838. https://doi.org/10.1519/JSC.0b013e31816a5825
LaStayo P, Marcus RL, Dibble L et al (2013) Eccentric exercise in rehabilitation: safety, feasibility and application. J Appl Physiol. https://doi.org/10.1152/japplphysiol.00008.2013
Lechauve JB, Perrault H, Aguilaniu B et al (2014) Breathing patterns during eccentric exercise. Respir Physiol Neurobiol 202:53–58. https://doi.org/10.1016/j.resp.2014.07.007
Leong CH, McDermott WJ, Elmer SJ, Martin JC (2013) Chronic eccentric cycling improves quadriceps muscle structure and maximum cycling power. Int J Sports Med. https://doi.org/10.1055/s-0033-1358471
Mueller M, Breil FA, Vogt M et al (2009) Different response to eccentric and concentric training in older men and women. Eur J Appl Physiol 107:145–153. https://doi.org/10.1007/s00421-009-1108-4
Nadel ER, Bergh U, Saltin B (1972) Body temperatures during negative work exercise. J Appl Physiol 33:553–558
Peñailillo L, Blazevich A, Numazawa H, Nosaka K (2013) Metabolic and muscle damage profiles of concentric versus repeated eccentric cycling. Med Sci Sports Exerc. https://doi.org/10.1249/MSS.0b013e31828f8a73
Peñailillo L, Blazevich A, Numazawa H, Nosaka K (2014) Rate of force development as a measure of muscle damage. Scand J Med Sci Sports. https://doi.org/10.1111/sms.12241
Pfeiffer JJ, Quintana R, Parker DL (2005) The influence of graded exercise test selection on Pmax and a subsequent single interval bout. J Exerc Physiol 8:10–17
Sheppard J, Hobson S, Barker M et al (2008) The effect of training with accentuated eccentric load counter-movement jumps on strength and power characteristics of high-performance volleyball players. Int J Sports Sci Coach 3:355–363. https://doi.org/10.1260/174795408786238498
Thomson DA (1971) Cardiac output during positive and negative work. Scand J Clin Lab Investig 27:193–200. https://doi.org/10.3109/00365517109080207
Wisløff U, Støylen A, Loennechen JP et al (2007) Superior cardiovascular effect of aerobic interval training versus moderate continuous training in heart failure patients a randomized study. Circulation 115:3086–3094. https://doi.org/10.1161/CIRCULATIONAHA.106.675041
Acknowledgements
This study was supported by an International Postgraduate Research Scholarship that was awarded the first author.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
There was no conflict of interest.
Additional information
Communicated by Guido Ferretti.
Rights and permissions
About this article

Cite this article
Lipski, M., Abbiss, C.R. & Nosaka, K. Cardio-pulmonary responses to incremental eccentric and concentric cycling tests to task failure. Eur J Appl Physiol 118, 947–957 (2018). https://doi.org/10.1007/s00421-018-3826-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00421-018-3826-y