
Abstract
Purpose
To determine if 8 weeks of periodized strength resistance training (RT) utilizing relatively short rest interval lengths (RI) in between sets (SS) would induce greater improvements in body composition and muscular performance, compared to the same RT program utilizing extended RI (SL).
Methods
22 male volunteers (SS: n = 11, 65.6 ± 3.4 years; SL: n = 11, 70.3 ± 4.9 years) were assigned to one of two strength RT groups, following 4 weeks of periodized hypertrophic RT (PHRT): strength RT with 60-s RI (SS) or strength RT with 4-min RI (SL). Prior to randomization, all 22 study participants trained 3 days/week, for 4 weeks, targeting hypertrophy; from week 4 to week 12, SS and SL followed the same periodized strength RT program for 8 weeks, with RI the only difference in their RT prescription.
Results
Following PHRT, all study participants experienced increases in lean body mass (LBM) (p < 0.01), upper and lower body strength (p < 0.001), and dynamic power (p < 0.001), as well as decreases in percentage body fat (p < 0.05). Across the 8-week strength RT phase, SS experienced significantly greater increases in LBM (p = 0.001), flat machine bench press 1-RM (p < 0.001), bilateral leg press 1-RM (p < 0.001), narrow/neutral grip lat pulldown (p < 0.01), and Margaria stair-climbing power (p < 0.001), compared to SL.
Conclusions
This study suggests 8 weeks of periodized high-intensity strength RT with shortened RI induces significantly greater enhancements in body composition, muscular performance, and functional performance, compared to the same RT prescription with extended RI, in older men. Applied professionals may optimize certain RT-induced adaptations, by incorporating shortened RI.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The effects of planned and systematically progressed (i.e., periodized) resistance training (RT) programs can serve as a countermeasure against the reductions in skeletal muscle mass, strength, power, physical activity, and activities of daily living, which are associated with sarcopenia (Kraemer et al. 1999; Hakkinen et al. 2000; Chodzko-Zajko et al. 2009). Evidence indicates older men are capable of experiencing significant strength gains and enhancements in certain functional tasks (e.g., walking, rising from a chair, balance) in response to long-term RT (Kraemer et al. 1999; Schlicht et al. 2001; Vincent et al. 2002), but studies comparing the effects of different periodized RT programs on body composition and muscular and functional performance are limited (Kraemer et al. 1999; Hakkinen et al. 2000).
Further, previous investigations examining program design optimization have focused on the manipulation of acute RT program variables to obtain a clearer understanding of optimal ways to elicit specific muscular adaptations, both acute and chronic (e.g., acute hormonal responses, strength increases, hypertrophic adaptations) (Smilios et al. 2003; Ahtiainen et al. 2005; Willardson and Burkett 2005; Willardson and Burkett 2006a, b, 2008, Willardson 2006). Resistance exercise (RE) prescription involves combining several acute variables, which include: RE movements used; intensity [% 1-repetition maximum or repetition maximum (RM) load]; volume (sets × repetitions); exercise sequence within an RE bout; repetition velocity; training frequency; and rest interval length between sets (RI) (Kraemer and Ratamess 2004). Among these acute program variables and in older adult cohorts, RI has received the least amount of scientific attention, relative to the volume of research examining the effects and influence of the other resistance exercise prescriptive variables (e.g., sets, reps, intensity). Collectively, the existing research suggests that different RI contribute to the variations in RT protocol-specific acute hormonal responses (Villanueva et al. 2012), and possibly chronic RT-induced adaptations, in the neuromuscular and endocrine systems (Ahtiainen et al. 2005; Willardson and Burkett 2008). While RI is typically prescribed based on training specificity/goal (e.g., hypertrophy, strength, power, and muscular endurance), there are conflicting findings and limitations in the current body of literature, which make identifying appropriate RI challenging (Willardson 2006, American College of Sports Medicine position stand 2009). In general, the recommended RI increases in duration when RT protocols/programs are designed for strength enhancement (e.g., 2–5 min) and decreases in duration when designed to promote hypertrophic/muscular endurance adaptations (e.g., 30–90 s) (Kraemer and Ratamess 2004).
Very few studies have examined the influence of RI on chronic muscular adaptations; for example, hypertrophy and/or strength increases across an 8- to 16-week period of training). Willardson and Burkett (2008) examined strength gains in young men, in the squat exercise, across 13 weeks of periodized RT. They utilized a non-linear progression of training volume and intensity and a 2-day per week training frequency. Comparing 2- versus 4-min RI, Willardson and Burkett found that both RI allowed for significant strength increases in the squat exercise following 13 weeks, which were not significantly different. However, this study also indicated that a 4-min RI allowed for the performance of higher total training volumes in workouts employing higher training intensities, compared to a 2-min RI. Similarly, findings from Robinson et al. (1995) suggest that a longer RI (3 min versus 90 or 30 s) allows for higher training volumes and intensities in the squat exercise, which contribute to significantly greater strength gains in young men over a longer period of RT. Based on these studies, a minimum of a 2-min RI may be needed for greater strength improvements following an extended period of RT, via the maintenance of higher training intensities and volumes.
Importantly, studies examining RI have major limitations. Specifically, conclusions from this body of literature are based predominantly on studies that have examined higher-volume/moderate-intensity hypertrophic protocols (Willardson and Burkett 2005, 2006a, b; Willardson 2006), while fewer studies have examined moderate- to low-volume/higher-intensity strength protocols (de Salles et al. 2010a). Furthermore, very minimal research investigating the effects of RI has been conducted in an older adult population (de Salles et al. 2010b); the consensus in this body of literature is derived predominantly from college-aged men and women. This unquestionably necessitates an examination of RI necessary to enhance acute strength RE performance and physiological responses and to maximize gains in strength across a period of RT in older adult populations.
Therefore, the purpose of this investigation was to examine the influence of RI manipulation within an 8-week periodized strength RT phase aimed at enhancing acute hormonal responses, muscular size and strength, and functional performance in older men. The results of this investigation provide novel insight into: (1) alternative periodization strategies to ameliorate the effects of sarcopenia; (2) the effects of RI within periodized strength RT on body composition changes and chronic muscular and functional performance adaptations; and (3) optimizing RT program design for older adult men.
Experimental approach to the problem
A central premise for this study is derived from previous work in our laboratory suggesting that strength-type/neuronal resistance exercise utilizing relatively short (60 or 90 s) RI can induce significant increases in acute testosterone response patterns lasting up to 30 min post-resistance exercise (Villanueva et al. 2012). In addition, substantial evidence suggests different combinations of volume, intensity, and rest interval length in between sets can influence the acute resistance exercise-induced anabolic hormone response (i.e., testosterone and human growth hormone). However, additional research is needed to fully elucidate if and how rest interval length in between sets may have important implications for modulating short- and long-term adaptations to resistance training, such as muscle protein synthesis, androgen receptor (AR) content and half-life, and/or intramuscular amino acid uptake, leading to improved net protein balance, muscle growth, and/or muscular strength/functional performance gains (Kvorning et al. 2006; Spiering et al. 2009; Vingren et al. 2010).
Novel to this area of research, the comparisons between very dissimilar rest interval lengths in between sets in this investigation assisted in determining the changes in body composition and muscular/functional performance in healthy older men that occur as a result of rest interval length manipulation within an 8-week periodized strength RT phase, following a 4-week periodized hypertrophic RT phase.
Methods
Subjects
Twenty-two men volunteered to participate in this study. The mean (SD) age, height, and weight of the participants were: 68 (±4.1) years, 1.8 (±0.1) m, and 83.9 (±10.3) kg, respectively (Table 1). All subjects were healthy, recreationally active, and none of the subjects were considered competitive weight lifters or engaged in any specific training/training cycle outside of this investigation. Lastly, none of the study participants had a history of non-competitive weight lifting or were taking any dietary or performance enhancing supplements.
Prior to participation in this investigation, all study participants were screened for uncontrolled hypertension, completed a Physical Activity Readiness Questionnaire (PAR-Q) to ensure they were qualified to participate in an exercise program, and provided medical clearance from their physician no more than 3 months prior to study enrollment, indicating they did not have known acute or chronic disease(s). Exclusion criteria included: acute illness, such as infection, recent surgery, and trauma; chronic illness, such as asthma, cardiac disease, kidney disease, liver disease, seizure disorders, anemia, and diabetes; and musculoskeletal injury interfering with the ability to perform resistance training and walking on a treadmill.
Each subject had the risks of the investigation explained to him and signed an informed consent form prior to participation in this study. The University of Southern California Health Sciences Campus Institutional Review Board approved all procedures involved in the study; therefore, this study was approved by the appropriate ethics committee and has been performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki.
Procedures
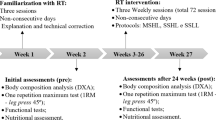
All study subjects completed 36 resistance training sessions, throughout a 12-week periodized resistance training program; the 12-week program consisted of a 4-week muscular endurance/preparatory training phase (Mesocycle I) emphasizing muscular endurance development and hypertrophy, followed by an 8-week strength training phase (Mesocycle II) emphasizing muscular strength and power development. Prior to participating in any training sessions, study subjects completed a 4-week control period, during which they continued to engage in their normal activities of daily living and did not adopt any new, structured resistance training program.
All RE sessions were closely supervised by an exercise specialist. Each training session began with a 5–10 min, low- to moderate-intensity warm-up on a treadmill and optional stretching exercises. Exercise sequence was controlled for during each RE session. The training loads prescribed were individually progressed in a safe and effective manner, to employ a progressive overload/challenge to the subjects’ neuromuscular system and elicit the greatest training-induced neuromuscular adaptations possible. Each RE session lasted between 45 and 60 min. Training logs were carefully maintained for each study participant by the primary investigator, which detailed expected/actual and progressed training loads, sets, and repetitions for each exercise for every training session, in addition to participants’ subjective feedback during each training session (e.g., fatigued, relative ease handling loads, relative difficulty handling loads, etc.).
Performance testing was conducted at week −4 (prior to a 4-week control period), Baseline (post-control period and prior to all training), week 4 (post-12 RE sessions), week 8 (post-24 RE sessions), and week 12 (post-36 RE sessions), to determine body composition, upper and lower body maximum strength, and functional performance capacity.
Proper breathing during training and exercise technique were demonstrated during week −4 testing, Baseline testing, and then again in the first training session. Participants were closely supervised for all testing and training sessions, with proper lifting technique a top priority. Participants were also encouraged to continue normal activities of daily living and eating routines outside of the resistance training program.
Throughout the entire study, all study participants remained healthy, injury free, and did not experience any adverse events.
Resistance training program
All 22 study subjects performed the same progressive total-body resistance training program in Mesocycle I, with a training frequency of 3 days/week for the 4-week training cycle. In Mesocycle I, sets/exercise ranged from 2 to 4, repetitions from 15 to 8, and training bouts were performed with a total of four to six exercises. Following week 4 performance testing, study subjects were paired based on the similarity of their flat bench machine chest press 1-RM and randomly placed into one of the two groups, SS or SL; we chose this strength outcome measure, because previous work from our lab has indicated there is relatively less variability among study participants with chest press 1-RM values, versus leg press 1-RM values, and, therefore, it would allow us to more easily randomize and create two treatment groups that are similar in (upper body maximum) strength. In Mesocycle II, a progressive total-body resistance training program emphasizing development of upper and lower body strength was performed 3 days/week for 8 weeks by both groups (SS and SL), and sets/exercise ranged from 2 to 3, repetitions from 6 to 4, and training bouts were performed with a total of 4–6 exercises. The only difference in program design between the two strength RT groups in Mesocycle II was the rest interval length utilized between sets: 60 s (SS group) versus 4 min (SL group). The resistance exercises utilized in the RT program included: bilateral leg press (45° angle of push; plate-loaded), flat bench machine chest press (bench press; supine; right and left machine handles move independently of each other; plate-loaded), lat pulldown (seated; cable), seated row (non-trunk supported; cable), dumbbell step-ups (free weights; 12- to 18-in. step height), dumbbell Romanian deadlifts (free weights), bilateral knee extension/flexion (seated; machine). Note: day 3 of Mesocycle II emphasized power production, with repetitions ranging from 6 to 4 and performed as “fast” as possible, while maintaining full range of motion and proper lifting technique; participants were encouraged to emphasize their “intent to move loads with as much velocity as possible”.
Throughout the entire resistance training program, all sets were performed maximally for the assigned number of repetitions and with proper lifting technique, and loads were adjusted in accordance with recovery and performance, across the repeated sets progression. Furthermore, it is important to note that study participants were never expected to perform sets to absolute muscular failure; given an appropriate loading progression, with alterations in set/repetition schemes throughout and across microcycles (i.e., a series of 3 training sessions), the repetition maximum assignments allowed for successful completion of the assigned number of repetitions at the load(s) prescribed, across multiple sets, and with minimal need for assistance/“spotting”. Therefore, training loads prescribed throughout the program were individually progressed, as intensely as possible, while attempting to pay full attention to each study participant’s recovery, performance, and safety/technique, in a safe and effective manner, to employ a progressive overload/challenge to the neuromuscular system and elicit the greatest training-induced neuromuscular adaptations possible, without inducing excessive neuromuscular fatigue effects (e.g., as a result of inappropriate overloading and/or training to muscular failure every set/exercise in each training bout). We believe this loading progression across repeated sets prevents musculoskeletal, connective tissue, and/or joint injuries, as well as overreaching/overtraining in this population, possibly by promoting an additive warm-up and/or potentiation effect across repeated sets, as well as promoting enhanced recovery from individual RE bouts and the maintenance of higher-frequency RT by avoiding excessive neuromuscular fatigue effects across a period of RT. In between sets, while resting passively, study participants were allowed to drink water, move around, and/or stretch ad libitum. For this investigation, the compliance rate to the resistance training was established at 85 % (31 out of 36 training sessions completed); the mean compliance rate for all participants in this study was 100 %, with no dropouts due to injury, illness, or personal choice.
Dietary records
At study week −4, Baseline, and study weeks 4 and 12, dietary intake was assessed via a 3-day dietary record, to determine if any changes in the participants’ diet occurred throughout the control period and resistance training intervention period. The diet recalls were analyzed using a commercially available program (Nutritionist Pro, Axxya Systems, Stafford, TX), to determine if the participants maintained similar dietary patterns during the study.
Testing
All testing procedures were conducted by the same assessor, not blinded, in the order below, at study week −4, Baseline, and study weeks 4, 8, and 12, in the Clinical Exercise Research Center (CERC) on the University of Southern California Health Sciences Campus. One outcome assessor was used throughout the study, to allow for maximum consistency and uniformity with all testing procedures. Outcome measures were collected with the utmost precision and attention to detail, with every effort made to completely avoid observer bias.
Body composition
Estimates for lean mass, fat mass, and body fat percentage were measured by whole-body dual-energy X-ray absorptiometry (DEXA). Before scanning, all participants were required to take off all removable objects containing metal (i.e., jewelry and clothing with metal). Scans were performed with the study participants lying in a supine position and properly aligned with the DEXA scanning table’s centerline longitudinal axis. Participants’ hands remained in a pronated or neutral position within the scanning region, participants were asked to remain completely immobile until the completion of the scan as signaled by the technician. For optimum scanning, scan analyses, and study participant safety, we: measured participants’ weight and height accurately; identified artifacts; recorded scan parameters; used standard protocols for consistency and comparability; used correct patient positioning and scan analysis; and ensured the radiation dose was as low as reasonably achievable. The DEXA scans were performed in the CERC; quality assurance testing was performed, prior to every scan, and, from scans performed in our laboratory, the coefficients of variation for fat mass and LBM measurements associated with DEXA are less than 1.7 %, and the reliability of the DXA scans is 0.99.
Functional performance
Star excursion balance test (SEBT)
Measurement of postural control is an important tool in the assessment of both athletic and geriatric populations for establishing levels of neuromuscular function for the purposes of injury prevention and rehabilitation. Postural control is often described as being either static (attempting to maintain a position with minimal movement) or dynamic (maintaining a stable base of support while completing a prescribed movement).
The SEBT was performed with the participants standing in the middle of a grid formed by three lines: (1) extending out directly anterior; (2) 45° posterior and laterally (right); and (3) 45° posterior and laterally (left). The participants were asked to reach as far as possible along each of the three lines with one leg (the reaching leg), while maintaining a single-leg stance with the other leg in the center of the grid, make a light touch on the line with the most distal part of the reaching leg (without allowing the contact to affect overall balance), and return the reaching leg back to the center (to a double-leg stance).
Participants were allowed to practice reaching in each of the three directions six times to minimize the learning effect (Hertel 2000). Following a 3-min rest period, participants performed three trials in each of the three directions. They began with the anterior direction and progressed clockwise around the grid. All participants began with a right stance leg in the center of the grid. After completion of the three trials in the three directions and another 3-min rest period, the test continued with a left stance leg. The same investigator recorded each reach distance with a mark on the tape as the distance from the center of the grid to point of maximum excursion by the reach leg. At the conclusion of all trials, the investigator measured the distances of each excursion with a standard tape measure; the greatest reach distance in each direction for each leg (6 total measurements) was taken as the final measurements. If the investigator felt the participant used the reaching leg for a substantial amount of support at any time, removed his foot from the center of the grid, or was unable to maintain balance on the support leg throughout the trial, the trial was discarded and repeated.
Margaria power test
To measure stair-climbing power, we utilized the Margaria power test (Margaria et al. 1966), which is not threshold limited. Participants ascended a 12-step staircase (each 17.5 cm) as rapidly as possible, without the use of railings, with times recorded by an electronic stopwatch to the nearest 0.01 s upon subject foot contact with the 4th and 8th steps. The same investigator recorded the times during all testing sessions for every participant; three trial times were recorded, with the best time taken as the final measurement. Dynamic Power was determined by calculating the product of the participant’s weight in kilograms, the vertical distance ascended, and acceleration of gravity, divided by the time elapsed. Test–retest reliability is 0.85, with CV’s of 2 %, across 4 weeks of testing.
400-m walk
Traditional tests of habitual gait are sometimes not sufficiently sensitive to detect low levels of dysfunction. Therefore, we utilized an outdoor 400-m timed walk to the nearest 0.01 s, with the participants walking as fast as possible (Cunningham et al. 1982; Walsh et al. 1998). The reliability coefficient is 0.81 (Walsh et al. 1998).
Muscular performance
Dynamic strength testing
Maximum voluntary muscle strength was assessed for the flat bench machine chest press and bilateral, 45° angle leg press exercises with a 1-repetition maximum (1-RM) method and for the narrow/neutral grip lat pulldown and seated unilateral knee extension (dominant leg) exercises with a 3–5-RM indirect method. Dynamic strength testing always proceeded in this order, and the four lifts were separated by 3–5 min of passive rest. In our lab, in this cohort, the coefficients of variation of these dynamic strength testing methods range from 0.8 to 2.4 %.
The 1-RM protocol consisted of three sub-maximal warm-up sets of 6, 4, and 3 repetitions, respectively, each followed by an approximate 1-min rest period, before the first 1-RM attempt. Loads were progressively increased with each 1-RM attempt (~5–20 pounds each attempt), and a 1- to 2-min rest period was given between each subsequent 1-RM attempt; previous published work from our lab and findings from (Matuszak et al. 2003) establish the reliability of, and evidence in support of, our strength/power testing/methodology in older men (Schroeder et al. 2007). Importantly, all study participants needed no more than 2 min (and, typically, around 1 min), to “feel” fully recovered and “ready” for another maximum effort 1-RM attempt/lift; therefore, similar to findings from Matuszak et al. we report that full recovery in between 1-RM attempts/lifts can be achieved with passive rest interval lengths of 1–2 min, in this cohort of older men. A true 1-RM was determined in 2–6 attempts for every study participant, with “failure” on a 1-RM attempt/lift being defined as the study participant being unable to voluntarily move the designated 1-RM load; further, following first-time fails on 1-RM attempts/lifts, study participants were allowed a second attempt/lift (following a rest period between attempts/lifts) (Schroeder et al. 2007). The indirect method involved 3–5 warm-up sets, followed by a working set that allowed completion of (no less than) 3 repetitions to (no more than) 5 repetitions. From the indirect method, the repetition maximum can be used to estimate 1-RM based on an estimated repetition maximum/%1-RM relationship chart.
Statistical analyses
Comparisons of measurements for the control period (week −4 versus week 0) were made using paired t tests. Comparison of group at week 4 (randomization) was performed using independent t tests. Repeated measures ANOVA was used to test within participant change from baseline to week 4 (4-week hypertrophic RT), as well as within and between participant effects from week 4 to week 12 (8-week strength RT). Analyses were performed using SPSS (V.20); α = 0.05. In addition to statistical tests, effect sizes (Cohen’s d; the difference between two means divided by a standard deviation for the data) were computed to determine whether the differences were small (d ~0.2), moderate (d ~0.5) or large (d ~0.7). Additionally, Pearson correlations were performed to determine strength of the association of changes in outcomes from weeks 4 to 12. The sample size for the present investigation was chosen through statistical power analyses, based on pilot data from our lab and previous literature, which indicated that 8–11 study participants per group would lead to significant differences between groups in select outcome measures (e.g., strength).
Results
Subject characteristics and body composition
Following the 4-week control period (week −4 to week 0), all subjects experienced non-significant changes in total body weight, lean body mass (LBM), fat mass, percentage body fat, and most muscular and functional performance outcome measures (p > 0.05); there were significant increases in flat bench machine chest press 1-RM (p < 0.05) and bilateral leg press 1-RM (p < 0.01), as well as a trend toward significant increases in narrow/neutral grip lat pulldown volume load (p = 0.06). Furthermore, there were significant differences in age between SS and SL (Table 1).
Dietary records
At baseline and study week 12, dietary intake was assessed via a 3-day dietary record, to determine if any changes in the participants’ diet occurred throughout the intervention period. Dietary patterns, including protein, carbohydrate, fat, and total caloric intake, were not significantly different between the two treatment groups. It is important to note that the dietary recalls indicated that all study participants consumed >1.0 gram protein/kilogram body weight/day, which likely allowed for maintenance of whole-body leucine metabolism and whole-body composition in this population of older adults (Campbell et al. 2001).
Effects of a 4-week hypertrophic training phase on body composition, muscular performance, and functional performance
After adjusting for values at week −4, statistical analyses revealed 4 weeks of high-volume, moderate-intensity hypertrophic training by all study subjects elicited significant increases in LBM (p < 0.01), flat bench machine chest press 1-RM (p < 0.001), bilateral leg press 1-RM (p < 0.001), narrow/neutral grip lat pulldown volume load (p < 0.001), unilateral knee extension volume load (p < 0.001), Margaria stair-climbing power (p < 0.001), and SEBT right stance anterior and posterior lateral reach distances (p < 0.05). Furthermore, all study subjects experienced significant decreases in percentage body fat (p < 0.05), Margaria stair-climbing time (p < 0.001), and 400-m walking time (p < 0.001). Lastly, there was a trend toward significant decreases in fat mass (p = 0.07).
Following the 4-week hypertrophic training phase, the two treatment groups (SS and SL) were comparable in total body weight, LBM, fat mass, percentage body fat, and all muscular and functional performance outcomes (p > 0.05), with the exception of narrow/neutral grip lat pulldown volume load (p < 0.01), SEBT right stance posterior medial reach distance, left stance posterior medial reach distance, and left stance posterior lateral reach distance (p < 0.05).
Effects of rest interval length manipulation across an 8-week strength training phase on body composition, muscular performance, and functional performance
Because these observations are part of a continuum across 12 weeks of RT, and all participants experienced the same training stimuli from week 0 to week 4, estimates reflect the difference between groups and across time from week 4 to week 12, after adjusting for values at week −4 and week 0, so that the changes within the final 8-week strength RT phase could be isolated. Furthermore, age was adjusted for a priori.
After adjusting for values at week −4 and 0, as well as age, statistical analyses revealed differences between SS and SL as a function of time across the 8-week strength training phase (Table 2). Specifically, from week 4 to week 12, SS experienced significantly greater increases in LBM [p = 0.001; small effect size (ES): 0.37; Fig. 1], flat machine bench press 1-RM (p < 0.001; large ES: 0.65; Fig. 2a), bilateral leg press 1-RM (p < 0.001; large ES: 0.76; Fig. 2b), narrow/neutral grip lat pulldown (p < 0.01; moderate ES: 0.59; Fig. 3a), and Margaria stairclimbing power (p < 0.001; moderate ES: 0.62; Fig. 3b). In addition, by week 12, there was a trend toward significantly greater decreases in Margaria stair-climbing time (0.27 ± 0.11 s versus 0.43 ± 0.14 s; p = 0.09; moderate ES: 0.45) and 400-m walking time (145.64 ± 20.22 s versus 160.91 ± 27.51 s; p = 0.08; small ES: 0.14) by SS, compared to SL.

Absolute values (mean ± SD) for lean body mass showing change from pre- to post-resistance training (week 0–weeks 4, 8, and 12) for SS group (solid circles/solid line), and SL group (solid circles/dashed line). *Significantly different between SS and SL, following the 8-week periodized strength training phase (p < 0.05)

a Absolute values (mean ± SD) for flat bench machine chest press 1-RM showing change from pre- to post-resistance training (week 0–weeks 4, 8, and 12) for SS group (solid circles/solid line), and SL group (solid circles/dashed line). *Significantly different between SS and SL, following the 8-week periodized strength training phase (p < 0.05) b Absolute values (mean ± SD) for bilateral leg press 1-RM showing change from pre- to post-resistance training (week 0–weeks 4, 8, and 12) for SS group (solid circles/solid line), and SL group (solid circles/dashed line). *Significantly different between SS and SL, following the 8-week periodized strength training phase (p < 0.05)

a Absolute values (mean ± SD) for narrow/neutral grip lat pulldown volume load showing change from pre- to post-resistance training (week 0–weeks 4, 8, and 12) for SS group (solid circles/solid line), and SL group (solid circles/dashed line). *Significantly different between SS and SL, following the 8-week periodized strength training phase (p < 0.05). b Absolute values (mean ± SD) for Margaria stair-climbing power showing change from pre- to post-resistance training (week 0–weeks 4, 8, and 12) for SS group (solid circles/solid line), and SL group (solid circles/dashed line). *Significantly different between SS and SL, following the 8-week periodized strength training phase (p < 0.05)
Furthermore, from week 4 to week 12, for group SS: changes in bilateral leg press 1-RM correlated with changes in Margaria stair-climbing power (r = 0.644, p < 0.05); changes in single-leg knee extension strength showed a near significant correlation with changes in SEBT left stance posterior medial reach distance (r = 0.533, p = 0.09) and correlated with 400-m walking time (r = −0.773, p < 0.01); changes in Margaria stair-climbing time correlated with changes in SEBT left stance anterior reach distance (r = 0.666, p < 0.05); changes in Margaria stair-climbing power showed a near significant correlation with changes in SEBT left stance anterior reach distance (r = 0.577, p = 0.06); and changes in 400-m walking time showed a near significant correlation with changes in SEBT right stance posterior medial reach distance (r = −0.583, p = 0.06) and correlated with changes in SEBT left stance posterior medial reach distance (r = −0.723, p < 0.05). Further, from week 4 to week 12, for group SL: changes in bilateral leg press 1-RM showed a near significant correlation with changes in SEBT left stance posterior medial reach distance (r = 0.618, p = 0.06).
Lastly, at week 12, for group SS: lean body mass correlated with flat bench machine chest press 1-RM (r = 0.883, p < 0.01), narrow/neutral grip lat pulldown strength (r = 0.685, p < 0.05), and single-leg knee extension strength (r = 0.686, p < 0.05).
Discussion
The present study demonstrated significant reductions in body fat percentage, increases in LBM, and enhancements in maximum dynamic strength and dynamic power, in response to 4 weeks of periodized hypertrophic RT. SS and SL engaged in the same hypertrophic resistance training phase, during the first 4 weeks of the 12 week periodized training program. Following the 4-week hypertrophic training phase, SS and SL were comparable in total body weight, LBM, fat mass, percentage body fat, and all muscular and dynamic power performance outcomes (p > 0.05), with the exception of narrow/neutral grip lat pulldown volume load; this suggests the hypertrophic phase of training elicited similar effects and rates of adaptation in all study participants between SS and SL.
A linear periodization program, similar to the one prescribed in the current investigation, typically begins with a higher-volume, low- to moderate-intensity phase of training (hypertrophic mesocycle), and then proceeds to a lower-volume, high-intensity phase of training (strength mesocycle) (Prestes et al. 2009). Hypertrophic training promotes muscle growth, improvements in muscular endurance, and enhancements in aerobic fitness (Fleck 1999; Kraemer et al. 1999; Izquierdo et al. 2001; American College of Sports Medicine position stand 2009); these adaptations may be induced, in part, as a result of the high metabolic demand of hypertrophic training and the well-documented acute increases in anabolic hormones (i.e., testosterone and growth hormone) and lactate in response to metabolically demanding protocols, such as hypertrophic/muscular endurance protocols prescribed using low- to moderate-intensities, moderate to high volumes, short rest interval lengths (RI) in between sets, and multi-joint movements that activate large muscle masses (Kraemer et al. 1990; Kraemer and Ratamess 2005; Beaven et al. 2008a, b; McCaulley et al. 2009; Villanueva et al. 2012).
The present investigation found a larger increase in LBM in the SS group than in the SL group, following 8 weeks of lower-volume, high-intensity strength training with very dissimilar RI in between sets (60 s for SS versus 4 min for SL). This finding indicates that strength training with relatively short RI leads to a larger increase in LBM than strength training with relatively long RI, when combined with hypertrophic training in a linear periodized RT program in older men. In the 8-week strength training phase, volume (sets × reps) was equated between SS and SL, and the only difference in programming was the RI prescription. As previously mentioned, importantly, the intensity/load(s) lifted allowed for successful completion of the assigned number of repetitions at the load(s) prescribed, across multiple sets, and with an extremely minimal need for assistance/“spotting”. Therefore, training loads prescribed throughout the program were individually progressed in a safe and effective manner, to employ an individualized and progressive overload/challenge to a participant’s neuromuscular system, elicit the greatest training-induced neuromuscular adaptations possible for each study participant, and maintain equal training volumes between SS and SL (i.e., no variability between groups in the number of sets and repetitions performed, in all training sessions). The prescription of relatively short RI for SS in the strength training phase is in drastic opposition to the traditionally prescribed and investigated RI of 3-5 min. Short RI are traditionally prescribed in hypertrophic training protocols/programs, and contribute to greater acute increases in anabolic hormones, hypertrophy, and enhancements in the metabolic demand of the resistance training (Kraemer et al. 1990, 1999; Ahtiainen et al. 2005; Kraemer and Ratamess 2005; Beaven et al. 2008a, b; McCaulley et al. 2009; Villanueva et al. 2012). Moreover, the greater increase in LBM experienced by SS is inconsistent with findings from studies examining the effects of high-intensity/low-volume strength training programs, which indicate these programs elicit significant improvements in muscular strength, but not muscle growth (Kraemer et al. 1999; Hakkinen et al. 2000; Goto et al. 2004; Beaven et al. 2008a, b). Therefore, utilization of relatively short RI in both hypertrophic and strength resistance training protocols/programs may be critical to optimizing muscle growth and strength adaptations with resistance training; however, given conflicting findings in the current literature, more research in warranted, particularly in older adults, to affirm this. For example, (de Salles et al. 2010a) examined younger, trained men and found that prescribing longer RI (i.e., 3–5 min) results in significantly greater increases in upper (bench press) and lower (leg press) body strength, versus shorter RI (i.e., 1 min), across 16 weeks of resistance training. These authors suggested that shorter RI can be effective for eliciting strength increases in less trained muscles or exercises; therefore, this may apply to novice/untrained older adults, as in the present investigation, as opposed to advanced lifters/athletes. Lastly, the authors also suggested that longer RI (e.g., up to 5 min) are best applied in highly trained muscles and exercises, as the window for adaptation narrows (i.e., across training periods exceeding 8 weeks); however, in the present study, participants were not highly trained, and the strength phase of the 12-week intervention was 8 weeks in length.
Increases in flat bench machine chest press 1-RM, bilateral leg press 1-RM, and narrow/neutral grip lat pulldown volume load were also larger in the SS group than the SL group, following the 8-week strength training phase. This indicates that strength training with relatively short RI was more effective in improving maximal dynamic strength than strength training with relatively long RI. Resistance training programs designed to enhance muscular strength typically emphasize distinct acute factors that influence strength performance/enhancement: (1) the maintenance of training intensity (i.e., the load lifted) and/or (2) the maintenance of training volume (i.e., maintenance of the number of repetitions performed each set, over repeated sets, and across multiple strength training sessions) (Willardson 2006). Current research suggests that “strength” RT programs employ longer RI in between sets, such as 3–5 min, to optimize repetition performance and/or maintain training intensity over repeated sets/across multiple training sessions, which, hypothetically, will optimize strength improvement/development (de Salles et al. 2009). Studies that have specifically examined maintenance of repetitions over repeated sets indicate that resting less than 3 min in between sets can result in a substantial decrease in repetitions (Kraemer 1997; Richmond and Godard 2004; Willardson and Burkett 2005, 2006a, b, 2008 Willardson 2006; de Salles et al. 2009), but the present investigation reveals, for the first time, that strength training (i.e., low-volume, high-intensity RT) with relatively short RI not only allows for maintenance of volume and intensity across repeated sets/multiple training sessions, but also leads to augmented maximal dynamic strength following an 8-week periodized strength training mesocycle.
Dynamic power was assessed in the present study by measuring stair-climbing time and stair-climbing power output, in addition to 400-m walking time. Increases in stair-climbing power output were larger in the SS group, following the 8-week strength training phase, while there was a trend toward significantly greater decreases in Margaria stair-climbing time (p = 0.09) and 400-m walking time (p = 0.08) by SS, compared to SL. Improvements in dynamic strength can potentially contribute to improvements in dynamic power (Hunter et al. 2004; Marsh et al. 2006), and the current study suggests that enhancing strength adaptations to training by utilizing relatively short RI may potentially elicit greater improvements in dynamic power performance in older men; correlation analyses indicated a strong relation between maximal dynamic strength enhancement and improvements in functional performance capacity (i.e., SS group/training). In addition, the 400-m walking test is a test of multiple performance qualities, which include: dynamic power, anaerobic power, cardiovascular endurance, and muscular endurance. Evidence suggests that high-volume/low- to moderate-intensity hypertrophic/muscular endurance resistance training is most commonly prescribed to effectively improve muscular and aerobic endurance (Fleck 1999; Kraemer and Ratamess 2004; American College of Sports Medicine position stand 2009). Accordingly, in the present study, the 4-week hypertrophic training phase induced significant increases in stair-climbing power output and significant decreases in stair-climbing time and 400-m walking time. However, by the end of the final 8-week strength training phase, muscular performance in short-duration, high-intensity activities (i.e., stair climbing and 400-m walking) was enhanced to a significantly greater extent in the SS group compared to the SL group. These findings suggests that the metabolic and neural demands of strength training with short RI may potentially be enhanced, compared to strength training with extended RI, which may lead to an augmented complimentary series of muscular performance adaptations, including dynamic maximal strength and dynamic power, as well as anaerobic, metabolic, and aerobic conditioning.
Measurement of postural control is an important tool in the assessment of both athletic and geriatric populations, to establish levels of neuromuscular function for the purposes of injury prevention and rehabilitation. Single-limb dynamic balance was assessed in the present study by the star excursion balance test (SEBT). SL demonstrated significantly greater SEBT right stance anterior reach distance, compared to SS (p < 0.05), following the 8-week strength RT phase, but there were no other statistically significant differences in any SEBT reach distance measure between SS and SL as a function of time across the 8-week strength training phase. Importantly, both SS and SL demonstrated gains in lower body (bilateral leg press) dynamic maximal strength during the entire 12-week training program (from week 0 to week 12) and improved dynamic balance. Correlation analyses also suggest a positive correlation between increased lower body dynamic maximal strength (e.g., compound movements involving activation of the quadriceps, gluteal, and/or hamstrings muscle groups) and improvements in dynamic postural control/balance.
Following the 8-week strength training mesocycle, the increase in LBM was higher in the SS group than in the SL group. This finding suggests that hypertrophic adaptations to strength resistance training can be facilitated and enhanced by employing relatively short RI in between sets (SS training), as opposed to traditionally prescribed extended RI in between sets (SL training). Although the exact mechanism underlying the influence of RI manipulation demonstrated in the present study remains to be elucidated, we have also reported that acute strength resistance exercise protocols employing relatively short 60-s RI, similar to the protocols utilized in SS training, elicit significantly greater acute increases in total testosterone and human growth hormone, compared to protocols employing relatively long 4-min RI, similar to the protocols utilized in SL training (Villanueva et al. 2012). Therefore, we provide compelling evidence that significant acute increases in blood total testosterone and human growth hormone concentrations from pre-(resting) to immediately post-resistance exercise in response to strength protocols utilizing relatively short RI contribute to maximization of muscle growth and strength development in strength phases of resistance training. Furthermore, from correlation analyses, we speculate that these enhancements in LBM in response to strength training with relatively short RI play a significant role in the augmentation of dynamic strength/power during strength training phases.
In this investigation, there were significant differences in age between SS and SL. We acknowledge that this is a notable limitation of this study; however, there are several points to consider, regarding this limitation. SS and SL had similar lean body mass, strength levels, and performance capabilities at week 0, prior to the 12-week RT program, and at week 4, prior to the 8-week strength RT phase. Furthermore, SS and SL had similar rates of adaptation for body composition and muscular/functional performance throughout the 4-week hypertrophic RT phase. Therefore, even after adjusting statistically for the age difference between groups a priori, the age difference did not influence body composition and performance outcomes, and SS and SL demonstrated equal performance capacities and abilities to experience adaptive responses to the RT program. It is important to note that all participants were individually supervised during all RE sessions, and loading was individually progressed across all 12 weeks of training. Participants were challenged with loads that allowed them to successfully complete a specific repetition maximum assignment each working set, without a need to excessively provide assistance (“spotting”) and, thus, without participants reaching absolute muscle failure during sets. If participants successfully completed all repetitions during a working set, depending on the participants’ perceived level of exertion during that set and their fatigue level at that given time point in the RE session, the load either remained the same or was increased for the subsequent working set. This individualized progression was maintained for all participants, throughout the 12-week RT program (Table 3).
Further, training logs were maintained in detail for each study participant, which detailed expected/actual training loads, sets, and repetitions for each resistance exercise for every training session, in addition to participants’ subjective feedback during each training session (e.g., fatigued, relative ease handling loads, relative difficulty handling loads, etc.). Given an appropriate loading progression, with alterations in set/repetition schemes throughout and across training weeks (microcycles), the repetition maximum assignments allowed for successful completion of the assigned number of repetitions at the load(s) prescribed, across multiple sets, and, as previously emphasized, with minimal need for assistance/“spotting”, which is known to influence various factors related to acute RE performance (e.g., acute hormonal responses, acute fatigue effects). Therefore, training loads used throughout the program were individually progressed in a safe and effective manner, to employ a progressive overload/challenge to the neuromuscular system and elicit the greatest training-induced neuromuscular adaptations possible, without inducing excessive neuromuscular fatigue effects, specifically, as a result of inappropriate overloading and/or training to failure every set/exercise in each resistance exercise bout. It is likely that minimizing excessive neuromuscular fatigue facilitated participants’ ability to tolerate higher-frequency resistance training and maintain optimal training performance, adequately recover from high-intensity training stresses, and, importantly, prevent musculoskeletal injury.
Collectively, the results from our study confirm that periodized resistance training is a highly effective countermeasure to age-related losses in skeletal muscle mass, muscular performance, and functional capacity, but these findings also indicate that future research is needed with a larger sample size and longer resistance training intervention to determine if the effects of rest interval length manipulation can lead to enhanced chronic body re-composition, muscular performance adaptations, and functional capacity over a longer period of time. The present study was limited by a small number of study participants in each group (n = 11), and future investigations should incorporate larger sample sizes to allow for maximal statistical power. Furthermore, the present study only examined older, untrained, men, so future research should include investigations of young- and middle-aged men, women, and clinical cohorts, untrained and trained. Lastly, the acute resistance training protocols in the present study utilized “RM loads”, which are commonly prescribed in addition to “%1-RM loads”, and this study did not include a determination of the molecular mechanisms contributing to the adaptive responses observed. Therefore, future research should aim to compare acute hormonal responses, acute gene/protein expression, body composition changes, and muscular/functional performance changes to longer-term strength resistance training protocols with very dissimilar rest interval lengths between sets, to more definitively establish the efficacy and effectiveness of the present periodization strategy and the mechanism(s) contributing to the changes in body composition, muscular performance, and functional capacity following long-term resistance training.
In terms of practical applications that can be derived from the present investigation, the results of the current investigation offer a novel strategy for prescribing strength resistance training in a population of healthy older men, as well as a model for periodization that may potentially optimize both hypertrophic and neural adaptations to long-term periodized resistance training. Prescribing strength resistance exercise and periodized strength resistance training for older men with relatively short rest interval lengths in between sets may optimize hypertrophic and performance adaptations to short-term strength resistance training and, therefore, maximally offset the age-related declines in lean body mass, strength, and power.
Abbreviations
- ANOVA:
-
Analysis of variance
- AR:
-
Androgen receptor
- CERC:
-
Clinical Exercise Research Center
- CV:
-
Coefficient of variance
- DEXA:
-
Dual-energy X-ray absorptiometry
- ES:
-
Effect size
- LBM:
-
Lean body mass
- RM:
-
Repetition maximum
- RE:
-
Resistance exercise
- RT:
-
Resistance training
- RI:
-
Rest interval length in between sets
- SEBT:
-
Star excursion balance test
References
Ahtiainen JP, Pakarinen A, Alen M, Kraemer WJ, Hakkinen K (2005) Short vs. long rest period between the sets in hypertrophic resistance training: influence on muscle strength, size, and hormonal adaptations in trained men. J Strength Cond Res 19(3):572–582
American College of Sports Medicine position stand (2009) Progression models in resistance training for healthy adults. Med Sci Sports Exerc 41(3):687–708
Beaven CM, Cook CJ, Gill ND (2008a) Significant strength gains observed in rugby players after specific resistance exercise protocols based on individual salivary testosterone responses. J Strength Cond Res 22(2):419–425
Beaven CM, Gill ND, Cook CJ (2008b) Salivary testosterone and cortisol responses in professional rugby players after four resistance exercise protocols. J Strength Cond Res 22(2):426–432
Campbell WW, Trappe TA, Wolfe RR, Evans WJ (2001) The recommended dietary allowance for protein may not be adequate for older people to maintain skeletal muscle. J Gerontol A Biol Sci Med Sci 56(6):M373–M380
Chodzko-Zajko WJ, Proctor DN, Fiatarone Singh MA, Minson CT, Nigg CR, Salem GJ, Skinner JS, American College of Sports Medicine position stand (2009) Exercise and physical activity for older adults. Med Sci Sports Exerc 41(7):1510–1530
Cunningham DA, Rechnitzer PA, Pearce ME, Donner AP (1982) Determinants of self-selected walking pace across ages 19 to 66. J Gerontol 37(5):560–564
de Salles BF, Simao R, Miranda F, Novaes Jda S, Lemos A, Willardson JM (2009) Rest interval between sets in strength training. Sports Med 39(9):765–777
de Salles BF, Maior AS, Polito M, Novaes J, Alexander J, Rhea M, Simão R (2010a) Influence of rest interval lengths on hypotensive response after strength training sessions performed by older men. J Strength Cond Res 24(11):3049–3054
de Salles BF, Simão R, Miranda H, Bottaro M, Fontana F, Willardson JM (2010b) Strength increases in upper and lower body are larger with longer inter-set rest intervals in trained men. J Sci Med Sport 13(4):429–433
Fleck SJ (1999) Periodized strength training: A critical review. J Strength Cond Res 13(1):82–89
Goto K, Nagasawa M, Yanagisawa O, Kizuka T, Ishii N, Takamatsu K (2004) Muscular adaptations to combinations of high- and low-intensity resistance exercises. J Strength Cond Res 18(4):730–737
Hakkinen K, Pakarinen A, Kraemer WJ, Newton RU, Alen M (2000) Basal concentrations and acute responses of serum hormones and strength development during heavy resistance training in middle-aged and elderly men and women. J Gerontol A Biol Sci Med Sci 55(2):B95–B105
Hertel J (2000) Functional instability following lateral ankle sprain. Sports Med 29(5):361–371
Hunter GR, McCarthy JP, Bamman MM (2004) Effects of resistance training on older adults. Sports Med 34(5):329–348
Izquierdo M, Hakkinen K, Anton A, Garrues M, Ibanez J, Ruesta M, Gorostiaga EM (2001) Maximal strength and power, endurance performance, and serum hormones in middle-aged and elderly men. Med Sci Sports Exerc 33(9):1577–1587
Kraemer WJ (1997) A series of studies: the physiological basis for strength training in American football: fact over philosophy. J Strength Cond Res 11(3):131–142
Kraemer WJ, Ratamess NA (2004) Fundamentals of resistance training: progression and exercise prescription. Med Sci Sports Exerc 36(4):674–688
Kraemer WJ, Ratamess NA (2005) Hormonal responses and adaptations to resistance exercise and training. Sports Med 35(4):339–361
Kraemer WJ, Marchitelli L, Gordon SE, Harman E, Dziados JE, Mello R, Frykman P, McCurry D, Fleck SJ (1990) Hormonal and growth factor responses to heavy resistance exercise protocols. J Appl Physiol 69(4):1442–1450
Kraemer WJ, Hakkinen K, Newton RU, Nindl BC, Volek JS, McCormick M, Gotshalk LA, Gordon SE, Fleck SJ, Campbell WW, Putukian M, Evans WJ (1999) Effects of heavy-resistance training on hormonal response patterns in younger vs. older men. J Appl Physiol 87(3):982–992
Kvorning T, Andersen M, Brixen K, Madsen K (2006) Suppression of endogenous testosterone production attenuates the response to strength training: a randomized, placebo-controlled, and blinded intervention study. Am J Physiol Endocrinol Metab 291(6):E1325–E1332
Margaria R, Aghemo P, Rovelli E (1966) Measurement of muscular power (anaerobic) in man. J Appl Physiol 21(5):1662–1664
Marsh AP, Miller ME, Saikin AM, Rejeski WJ, Hu N, Lauretani F, Bandinelli S, Guralnik JM, Ferrucci L (2006) Lower extremity strength and power are associated with 400-meter walk time in older adults: the InCHIANTI study. J Gerontol A Biol Sci Med Sci 61(11):1186–1193
Matuszak ME, Fry AC, Weiss LW, Ireland TR, McKnight MM (2003) Effect of rest interval length on repeated 1 repetition maximum back squats. J Strength Cond Res 17(4):216–221
McCaulley GO, McBride JM, Cormie P, Hudson MB, Nuzzo JL, Quindry JC, Travis Triplett N (2009) Acute hormonal and neuromuscular responses to hypertrophy, strength and power type resistance exercise. Eur J Appl Physiol 105(5):695–704
Prestes J, Frollini AB, de Lima C, Donatto FF, Foschini D, de Cassia Marqueti R, Figueira A Jr, Fleck SJ (2009) Comparison between linear and daily undulating periodized resistance training to increase strength. J Strength Cond Res 23(9):2437–2442
Richmond SR, Godard MP (2004) The effects of varied rest periods between sets to failure using the bench press in recreationally trained men. J Strength Cond Res 18(4):846–849
Robinson JM, Stone MH, Johnson RL, Penland CM, Warren BJ, Lewis RD (1995) Effects of different weight training exercise/rest intervals on strength, power, and high intensity exercise endurance. J Strength Cond Res 9(4):216–221
Schlicht J, Camaione DN, Owen SV (2001) Effect of intense strength training on standing balance, walking speed, and sit-to-stand performance in older adults. J Gerontol A Biol Sci Med Sci 56(5):M281–M286
Schroeder ET, Wang Y, Castaneda-Sceppa C, Cloutier G, Vallejo AF, Kawakubo M, Jensky NE, Coomber S, Azen SP, Sattler FR (2007) Reliability of maximal voluntary muscle strength and power testing in older men. J Gerontol Series A: Biol Sci Med Sci 62(5):543–549
Smilios I, Pilianidis T, Karamouzis M, Tokmakidis SP (2003) Hormonal responses after various resistance exercise protocols. Med Sci Sports Exerc 35(4):644–654
Spiering BA, Kraemer WJ, Vingren JL, Ratamess NA, Anderson JM, Armstrong LE, Nindl BC, Volek JS, Hakkinen K, Maresh CM (2009) Elevated endogenous testosterone concentrations potentiate muscle androgen receptor responses to resistance exercise. J Steroid Biochem Mol Biol 114(3–5):195–199
Villanueva MG, Lane CJ, Schroeder ET (2012) Influence of rest interval length on acute testosterone and cortisol responses to volume-load-equated total body hypertrophic and strength protocols. J Strength Cond Res 26(10):2755–2764
Vincent KR, Braith RW, Feldman RA, Magyari PM, Cutler RB, Persin SA, Lennon SL, Gabr AH, Lowenthal DT (2002) Resistance exercise and physical performance in adults aged 60 to 83. J Am Geriatr Soc 50(6):1100–1107
Vingren JL, Kraemer WJ, Ratamess NA, Anderson JM, Volek JS, Maresh CM (2010) Testosterone physiology in resistance exercise and training: the up-stream regulatory elements. Sports Med 40(12):1037–1053
Walsh M, Woodhouse LJ, Thomas SG, Finch E (1998) Physical impairments and functional limitations: a comparison of individuals 1 year after total knee arthroplasty with control subjects. Phys Ther 78(3):248–258
Willardson JM (2006) A brief review: factors affecting the length of the rest interval between resistance exercise sets. J Strength Cond Res 20(4):978–984
Willardson JM, Burkett LN (2005) A comparison of 3 different rest intervals on the exercise volume completed during a workout. J Strength Cond Res 19(1):23–26
Willardson JM, Burkett LN (2006a) The effect of rest interval length on bench press performance with heavy vs. light loads. J Strength Cond Res 20(2):396–399
Willardson JM, Burkett LN (2006b) The effect of rest interval length on the sustainability of squat and bench press repetitions. J Strength Cond Res 20(2):400–403
Willardson JM, Burkett LN (2008) The effect of different rest intervals between sets on volume components and strength gains. J Strength Cond Res 22(1):146–152
Acknowledgments
The authors would like to thank the study participants, University of Southern California Clinical Exercise Research Center staff, and Adriana Del Padilla for their contribution to the successful completion of the experimental protocol. This study was funded by the National Strength and Conditioning Association Foundation (NSCAF). The results of the present study do not constitute endorsement by NSCA.
Conflict of interest
For all authors, there are no conflicts of interest, which might lead to bias in this manuscript.
Author information
Authors and Affiliations
Corresponding author
Additional information
Communicated by Michael Lindinger.
Rights and permissions
About this article

Cite this article
Villanueva, M.G., Lane, C.J. & Schroeder, E.T. Short rest interval lengths between sets optimally enhance body composition and performance with 8 weeks of strength resistance training in older men. Eur J Appl Physiol 115, 295–308 (2015). https://doi.org/10.1007/s00421-014-3014-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00421-014-3014-7