
Abstract
Impact reduction has become a factor of interest in the prevention of running-related injuries such as stress fractures. Currently, the midfoot strike pattern (MFS) is thought as a potential way to decrease impact. The purpose was to test the effects of two long-term interventions aiming to reduce impact during running via a transition to an MFS: a foot strike retraining versus a low-drop/low-heel height footwear. Thirty rearfoot strikers were randomly assigned to two experimental groups (SHOES and TRAIN). SHOES progressively wore low-drop/low-heel height shoes and TRAIN progressively adopted an MFS, over a 3-month period with three 30-min running sessions per week. Measurement sessions (pre-training, 1, 2 and 3 months) were performed during which subjects were equipped with three accelerometers on the shin, heel and metatarsals, and ran for 15 min on an instrumented treadmill. Synchronized acceleration and vertical ground reaction force signals were recorded. Peak heel acceleration was significantly lower as compared to pre-training for SHOES (−33.5 ± 12.8 % at 2 months and −25.3 ± 18.8 % at 3 months, p < 0.001), and so was shock propagation velocity (−12.1 ± 9.3 %, p < 0.001 at 2 months and −11.3 ± 4.6 %, p < 0.05 at 3 months). No change was observed for TRAIN. Important inter-individual variations were noted in both groups and reported pains were mainly located at the shin and calf. Although it induced reversible pains, low-drop/low-heel height footwear seemed to be more effective than foot strike retraining to attenuate heel impact in the long term.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Given the extent of the phenomenon over the years, an increasing amount of research has focused on running-related injuries, which present an incidence of 19.4–92.4 % (van Gent et al. 2007). Among them, stress fractures represent 20 % of all sport injuries (Snyder et al. 2006), the most frequent being tibial stress fractures (Brukner et al. 1996). According to Shorten and Mienjtes (2011), impact force is characterized by a force pulse transmitted through the foot over a short duration and thus with high frequencies. An optimal level of impacts is appropriate to develop and maintain bone tissue health without causing overuse injuries (Fuchs et al. 2001; Fuchs and Snow 2002). However, repetitive impact shocks generated at each running step have been reported as a mechanical cause of stress fractures (Dickinson et al. 1985). As a consequence, the recent studies focused on how to reduce the impact level in running. Among the experimentally measurable mechanical features of impact during the running step, loading rate (LR), time to impact peak (\(t_{{f}_{z1}}\)) and peak accelerations are thought the most directly related to the magnitude of the foot–ground impact shock (Samozino et al. 2008; Derrick and Mercer 2004). Nigg (1986) revealed, using acceleration measurements performed during running, that heel acceleration overall corresponds to impact forces. However, LR and \(t_{{f}_{z1}}\) also integrate the low frequency components of VGRF signal that correspond to ‘non-impact’ components transmitted to both the heel and distal foot, and should therefore be interpreted with caution (Shorten and Mienjtes 2011). There is an ongoing controversy about the link between bone injuries (e.g. stress fractures) and VGRF parameters. Although some authors found no relationship (Crossley et al. 1999; Bennell et al. 2004), LR, identified as the average time derivative of vertical ground reaction force (VGRF) within the first milliseconds of the support phase, is thought to influence the risk of stress fractures (Davis et al. 2004; Milner et al. 2006; Zapdoor and Nikooyan 2011). It was also observed that previously injured runners exhibited higher LR and peak tibial acceleration than uninjured runners (Hreljac 2004). Consequently, bone injuries prevention is becoming synonymous with minimized impact, the latter being possibly quantified/objectivized through LR and peak accelerations.
To potentially reduce the running-related injury risk and/or attenuate impact in running, orthotic insoles (Mattila et al. 2011) as well as footwear cushioning systems (Schwellnus et al. 1990; Richards et al. 2009; Squadrone and Gallozzi 2009; Lohman et al. 2011; Goss and Gross 2012b) were shown ineffective. Alternatively, barefoot runners potentially reduce the impact magnitude at the heel (Squadrone and Gallozzi 2009; Lieberman et al. 2010; Lieberman 2012) by a “flatter” foot incline at landing and thus by a shift from a rearfoot strike pattern (RFS) to a midfoot/forefoot strike pattern (MFS/FFS). This ‘impact-reduction running pattern’ results in lower step length and contact time (t c), a higher plantarflexion due to a higher pre-activation of triceps surae muscles, and a lower activation of the tibialis anterior (De Wit et al. 2000; Goss and Gross 2012b; von Tscharner et al. 2003; Divert et al. 2005; Giandolini et al. 2013). Barefoot running also induces a complete removal of the impact peak and a markedly reduced LR (Dickinson et al. 1985; Lieberman et al. 2010; Hamill et al. 2011; Goss and Gross 2012b). However, although trendy and potentially interesting for specific injury prevention, barefoot running presents obvious environmental limits and provides no benefit in terms of energetic cost, compared to wearing light shoes (~150 g) (Franz et al. 2012). Recently, Giandolini et al. (2013) observed a 50 % reduction in LR associated with a higher gastrocnemius lateralis pre-contact activation and a lower tibialis anterior activation during a 5-min MFS shod trial in habitually RFS recreational runners. In parallel, Daoud et al. (2012) observed that RFS cross-country runners faced approximately twice as many repetitive stress-related injuries as FFS runners. The lower foot–ground impact shock associated with MFS/FFS pattern has been proposed as contributing to a lower risk of running-related injuries. That said, performance is the main motivation for many runners, and a transition to MFS appears conceivable only if it does not alter performance.
Reduced vertical oscillations of the center of mass associated with short step length and t c (Anderson 1996), and the use mechanism of storage–restitution of elastic energy in the lower limb musculotendinous structures (Ker et al. 1987; Anderson 1996; Saunders et al. 2004) are known to improve running economy and thus running performance in most cases. In this regard, MFS and FFS induce lower step length and t c (Squadrone and Gallozzi 2009; De Wit et al. 2000), and thus decrease vertical oscillations (Goss and Gross 2012b). A higher use of elastic structures with an FFS was also reported by Ardigo et al. (1995). This suggests that MFS is not detrimental for running economy (Perl et al. 2012) and might even be beneficial. Hasegawa et al. (2007) observed among elite-half-marathon runners that the percentage of MFS runners increased when running speed increased. More recently, Kasmer et al. (2012) showed during a marathon that non-RFS runners (i.e. MFS, FFS and asymmetrical patterns) were better ranked after 8 km than rearfoot strikers. However, this seems to be not true for recreational marathon runners (Larson et al. 2011), probably due to the higher triceps surae activation which might be hard to maintain. Consequently, a transition towards MFS could reduce the overall impact at each step and in turn the risk of bone injuries without altering performance.
Among the strategies for an acute MFS transition that have been studied, gait retraining has been investigated several times (Davis 2005; Crowell et al. 2010; Crowell and Davis 2011). These authors observed that the acute use of real-time visual feedback based on a tibial accelerometer signal allowed subjects to change their pattern and run with a reduced tibial shock, even after the feedback was removed (Davis 2005; Crowell et al. 2010). Similarly, a two-week gait retraining (eight sessions of 15–30 min on instrumented treadmill) with real-time feedback (tibial acceleration) and oral instruction (‘run softer’) resulted in 20–50 % lower tibial acceleration and LR in rearfoot strikers (Crowell and Davis 2011). No injury was reported during the training period except localized pains at the triceps surae probably associated with tissue adaptation. It is worth mentioning that these studies were not focused on running technique but only on impact reduction. Moreover, a transition from RFS to MFS could induce calf and Achilles tendon pains because of unusual and higher triceps surae activation, which justifies the importance of progressivity in gait retraining programs (Daoud et al. 2012). An RFS-to-MFS transition seems therefore possible through a progressive and adapted foot strike retraining program.
Last, shoe midsole geometry has recently been tested as a potential solution to induce changes in the running pattern. Hamill et al. (2011) observed that various midsole thicknesses (heel/forefoot height: 4/0, 12/8 and 20/16 mm) had no effect on running kinetics and kinematics over a 25-m trial in ten rearfoot strikers. Contrastingly, Horvais and Samozino (2013) highlighted the acute effect of low heel drop (difference between heel and forefoot midsole thickness) and low-heel height midsole on running pattern in twenty rearfoot strikers: positive correlations between heel drop and foot angle at ground contact and between heel thickness and foot angle were found. These authors concluded on the complementary effects of low drop and low heel height on the transition toward a MFS: wearing shoes with a low drop and/or a low heel height led RFS runners to adopt a more MFS pattern, this alteration being more pronounced with 0-mm drop and heel height. Consequently, a flatter midsole geometry (i.e. low-drop/low-heel height) is also possibly useful to induce RFS-to-MFS transition.
Conclusions on impact intensity in different footwear conditions or with different running patterns are still debated, notably because of the disparity between experimental protocols (subjects’ degree of familiarization, type of shoes, distance and duration of the testing trials, acute or chronic interventions). Progressive foot strike retraining and low-drop/low-heel height shoes, hereafter called ‘flat-midsole shoes’, have nevertheless been shown as effective solutions for an RFS-to-MFS transition. However, these strategies have only been investigated separately and in acute conditions. Consequently, their long-term effects on running mechanics and on musculoskeletal structures are unknown. The purpose of this study was to compare in RFS recreational runners the effects of foot strike retraining and flat-midsole footwear during a 3-month period on overall impact, and associated pain and/or injury onset. In light of the previous findings, we hypothesized that both solutions investigated would lead rearfoot strikers to reduce impact magnitude through the 3-month intervention by a progressive alteration of their running pattern. The relative extents of these changes (if observed) were the main focus of this study.
Methods
Subjects
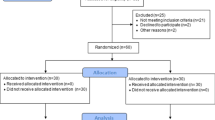
Thirty young healthy adults, 22 males and 8 females (18.3 ± 4.5 years, 166 ± 41 cm, 65.5 ± 16.9 kg), were included and gave their written informed consent to participate in the study, which was approved by the local ethical committee and conducted in agreement with the Declaration of Helsinki. All subjects were rearfoot strikers (see below) and practiced various sports (7.1 ± 3.1 h week−1), including recreational running. Except for the required efforts and the running sessions and conditions involved, they did not know the exact aim of the study (i.e. comparing the long-term effects of flat-midsole footwear and MFS). They were not presenting recent muscular, joint or bone injuries, or receiving any medication, as confirmed by the medical examination performed during the inclusion session.
Experimental protocol
A familiarization and inclusion session was first conducted. It consisted in a 10-min run at 3 m s−1 on an instrumented treadmill during which a 20-s sampling of data was performed without informing subjects about the exact moment of sampling and the variables studied (Morin et al. 2009). This allowed us to confirm the RFS pattern of the subjects according to whether or not an impact peak was present on the VGRF signal for at least nine steps out of ten. After their inclusion, subjects were randomly assigned to two experimental groups, while keeping males and females parity: TRAIN (19.7 ± 1.3 years, 177 ± 79 cm, 70.7 ± 9.0 kg, 7 ± 3 h week−1) and SHOES (18.9 ± 0.7 years, 175 ± 91 cm, 67.2 ± 10.7 kg, 8 ± 3 h week−1). The TRAIN group was instructed to progressively adopt an MFS pattern (‘land with the midfoot, with a flatter foot strike’), and wore standardized shoes (Salomon XT Wings™, mass 400 g, heel height 30 mm, drop 10 mm). The SHOES group was instructed to progressively wear flat-midsole shoes (Salomon Sense S-Lab™, mass 200 g, heel height 20 mm, drop 4 mm) and received no instruction about running technique.
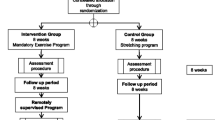
For both groups, 39 running sessions composed the 13-week program (three 30-min sessions per week). The instructions were gradually adopted (see “Appendix” for more details). Throughout the 3 months, TRAIN ran on an average 13.7 ± 2.1 h with the MFS pattern and SHOES ran on average 16.4 ± 1.5 h with the flat-midsole shoes. Subjects trained (excepted for the first training session performed with the experimenters) in the field on flat and various surfaces, at their preferred running speed (PRS, see below) and at an intensity controlled by means of a heart rate monitor (Kalenji CW300, Villeneuve d’Ascq, France). An instruction and training log was given to the subjects, wherein they were asked to systematically report all their comments, feelings, pains (during or after their training sessions), injuries and session heart rate. This pain report was used to identify the consequences of such interventions. When necessary, a medical examination was immediately planned to decide whether or not the subject could resume the training program.
Four measurement sessions were performed: pre-training, and after 1, 2, and 3 months (post-training), with running mechanics and PRS assessments at each session. During these sessions TRAIN subjects wore the standardized shoes and SHOES subjects wore the low-drop/low-heel height shoes. For the measurement of PRS, subjects were equipped with a heart rate monitor (Polar RS800, Kempele, Finland) and started to run at 2.5 m s−1 for 2 min; after 2 min they were free to increase or decrease their speed to a self-selected pace with no feedback provided on its value (Heiderscheit et al. 2011), while keeping an intensity of ~80–85 % of their estimated maximal heart rate (220—age). The heart rate corresponding to this PRS was then communicated to the subjects for their training sessions. This procedure was repeated each month to monitor a possible change in PRS due to an alteration of the running pattern, MFS pattern being supposed to possibly increase subjects’ PRS. Then, subjects performed a 15-min run on an instrumented treadmill at their pre-training PRS for each measurement session. Subjects were equipped with three uniaxial accelerometers securely fixed with Dual Lock™ (3M, St. Paul, USA) and strapped (1) on the anteromedial aspect of the distal third of the tibia (from medial malleolus to femoral condyle), with the skin shaved and cleaned beforehand, and above the midsole (2) at the heel and (3) at the fifth metatarsal head level (Fig. 1). A synchronized acquisition (10 s at 1,000 Hz) between VGRF and accelerometers’ signals was performed after 15 min, without subjects being informed about the exact moment of sampling (Morin et al. 2009).

Placement of the three accelerometers on the left leg of the subject: on the tibia (at the distal third from medial malleolus to great trochanter on the bone’s anteromedial aspect), on the external side of the shoe at the fifth metatarsal’s head (above the midsole) and on the back of the shoe at the heel (above the midsole). Accelerometers were firmly taped with strapping and Dual Lock™
Mechanical and acceleration variables
Running kinetics and kinematics were quantified from the three-dimensional ground reaction forces data collected during the 10-s acquisitions performed on an instrumented treadmill (HEF Tecmachine, Andrézieux-Bouthéon, France, Belli et al. 2001; Divert et al. 2005). VGRF signal was sampled at 1,000 Hz and low-pass filtered (fourth-order Butterworth filter, 30 Hz). This allowed us to determine t c, t a, F z1 (force impact peak), \(t_{{f}_{z1}}\) (time to impact peak) and LR (vertical mean loading rate), which was calculated as the mean value of the time-derivate of VGRF signal within the first 24 ms of the support phase and expressed in BW s−1 (e.g. De Wit et al. 2000). Step frequency (F q, in Hz) was calculated from t c and t a as F q = 1/(t c + t a).
Acceleration signal was sampled at 1,000 Hz during a 10-s acquisition and low-pass filtered (50 Hz). Acceleration variables are presented in Fig. 2. Peak acceleration at the heel (PHA), tibia (PTA) and metatarsal levels (PMA) were measured by three uniaxial accelerometers (ADXL150, Analog Device, USA). The shock wave propagation velocity between heel and tibia (SPV, in m s−1) was calculated from the moment of PHA and the moment of PTA as \( {\text{SPV}}\; = \Updelta d/\Updelta t \) with ∆d the distance between the heel and tibia accelerometers (in m) and ∆t the time between PHA and PTA (s). The time between PHA and PMA was also calculated (T hm, in s) to describe the foot strike pattern. We hypothesized that a positive T hm indicated an RFS pattern, whereas a negative T hm indicated an FFS pattern. Thus, in theory, a T hm equal to zero would indicate a MFS pattern. Accelerometers data were recorded with an 12 bit A/D acquisition card (DAS8, National Instruments, USA), and synchronized with VGRF signal with LabChart 7.3 software (ADInstruments, Bella Vista, Australia).

Synchronized acceleration (full lines) and vertical ground reaction force (broken line) signals for the first 100 ms of a typical step, and acceleration parameters: peak tibial acceleration (PTA), peak heel acceleration (PHA), peak metatarsal acceleration (PMA) and time from PHA to PMA (T hm)
Data analysis and statistics
Descriptive statistics are presented as mean ± SD. All mechanical parameters were averaged for ten consecutive steps. Normal distribution was checked by the Shapiro–Wilk’s normality test and variance homogeneity was tested by the Fisher’s F test. In the case of normality and homogenous variance, intersession comparison for each group was performed with repeated-measures ANOVA associated with the Newman–Keuls post hoc test. Intergroup comparisons for each session were performed using Student t tests. In the case of non-normality and/or non-homogenous variance, intersession comparisons were performed with the Friedman test and intergroup comparisons were performed with the Mann–Whitney test associated with Bonferroni’s correction. Intergroup comparisons were analyzed through relative changes from the pre-training session values because of many significant differences between the two groups in the pre-training session (in \(t_{{f}_{z1}}\), PHA, PTA, T hm and SPV) despite the randomized allocation. The significant level was set at p < 0.05.
Results
Data of twenty-eight subjects were analyzed, two female TRAIN subjects being unable to complete the program (see below). No statistical difference was found for heart rate between the two groups. All subjects together, grand averages for heart rate were 175 bpm at pre-training and 3-month, and 173 bpm at 1, 2 months and during their training session. We can thus reasonably assume that all the subjects ran at their PRS and at the same intensity throughout the 3 months.
Running mechanics
In SHOES subjects, PHA decreased at 2- and 3-month from pre-training by 33.5 ± 12.8 % (p < 0.001) and 25.3 ± 18.8 % (p < 0.001), respectively. A decrease in T hm between 1 and 2 months was also observed (p < 0.01). At 2 and 3 months, SPV was approximately 11 % lower as compared to pre-training and 1 month (p < 0.05, Table 1). Concerning kinetics, only F z1 decreased by 4.8 ± 11.4 % (p = 0.02) at 3 months as compared to pre-training (Table 2). When concerning kinematics, at 1 month t c and t a were, respectively, higher (2.9 ± 4.7 %, p < 0.05) and lower (−4.4 ± 9.2 %, p < 0.05) as compared to pre-training. Surprisingly, \(t_{{f}_{z1}}\) was lower at 2 and 3 months by 12.8 ± 25.9 and 13.3 ± 6.3 % (p < 0.0001), respectively (Table 3). For TRAIN, no change in the mechanical parameters studied was observed, except a decrease in PRS at 2 and 3 months as compared to pre-training and 1 month (p < 0.03, Table 3). Besides, important inter-individual variations were noted as shown by the high SD for relative changes (Tables 1, 2, 3).
Reported pains and injuries
Two female TRAIN subjects were excluded from the study after medical examination: one because of an injury at the back (independent from the protocol), and one for recurrent shin splints, an injury previously experienced by this subject. Among the painful symptoms reported, the most frequent were localized at the shin (tibial periosteum) and calf (triceps surae) representing 30.8 and 25.0 % of all reported pains in TRAIN and SHOES groups, respectively (Table 4). The main localizations were shin and hip (46.2 and 23.0 %, respectively) for TRAIN and calf and shin (28.2 and 25.6 %, respectively) for SHOES subjects. The overall seven shin pains were reported during the first month, eight during the second month and only one during the third month. Five calf pains were noted during the first month and four through the second and the third. Other reported pains, although much less frequent, were localized at the ankle, knee, hip and back. Generally, fewer comments and pains were reported during the second and third months.
Discussion
The purpose of this study was to test the effectiveness of two chronic interventions (flat-midsole footwear and foot strike retraining) to reduce the overall impact in recreational runners. No change in LR variation was observed during the 3 months both in SHOES and TRAIN groups. Similarly, the foot strike retraining program induced no variation in peak accelerations at the heel, tibia and metatarsal levels. Thus, this 3-month RFS-to-MFS intervention seemed to have no effect on the impact magnitude. Contrastingly, the flat-midsole footwear intervention induced a decrease in peak heel acceleration (−33.5 ± 12.8 % at 2 months and −25.3 ± 18.8 % at 3 months, p < 0.001) and in shock wave propagation speed (−12.1 ± 9.33 % at 2 months and −11.3 ± 14.6 % at 3 months, p < 0.03).
The shoes worn by SHOES subjects could be described as an intermediate model between minimalist shoes like Vibram FiveFingers™ characterized by an ~0-mm drop and classical cushioned shoes such as those used by the TRAIN subjects. Specifically, the Salomon Sense S-Lab™ is a light and flexible shoe, and its midsole only offers a sufficient protection for running on rough terrains. When compared with pre-training, PHA decreased by 33.5 % at 2 months (4.27 ± 0.89 g, p < 0.001) and by 25.3 % at 3 months (4.98 ± 1.61 g, p < 0.001). In parallel, SPV was reduced by 12.1 % at 2 months (6.08 ± 1.34 m s−1) and 11.3 % at 3 months (6.22 ± 1.28 m s−1) as compared to pre-training (p < 0.03). Taken together, these results clearly show a reduction in the impact intensity at the heel and a lower shock wave propagation speed (Fig. 3). Hamill et al. (2011) recently reported a higher LR when heel drop increases by 4 mm (barefoot versus three 4-mm drop shoes). These observations are different from the present ones, because we observed no LR variation with a 4-mm drop. Moreover, a few parameters (t c, t a, T hm) significantly differed only at 1 month before going back to pre-training values, as if the first month of training with flat-midsole shoes induced a temporary adaptation that was measurable at 1 month (decreases in PHA and SPV) and likely completed at 2 months. Our likely explanation is that subjects managed to adapt to their new footwear and the very low drop and thickness of the midsole, as compared to their usual personal running footwear. A large inter-individual variability was further observed in the SHOES group. For instance, post-training 95 % confidence interval for relative changes was ranged from −46.0 to 52.8 % for PMA. Individuals would respond differently to flat-midsole shoes. A decrease in PHA and SPV was observed post training for thirteen subjects out of fifteen. We could therefore hypothesize that to decrease shock magnitude under the heel, the part of the foot that is less protected with the experimental shoes, some of the subjects would adopt a flatter foot landing, which generated changes in shock acceleration magnitude (higher PMA concomitant with a lower PHA). This flatter landing could be possibly characterized by a decreased T hm (low duration between heel and metatarsals strike), this parameter presenting a high post-training inter-individual variability (95 % confidence interval for relative change from −28.3 to 30.1 %). This interpretation is consistent with the observations of Squadrone and Gallozzi (2009) and Hennig and Milani (1995) who concluded that footwear influenced foot mechanics. More precisely, Squadrone and Gallozzi (2009) observed that peak pressure under the heel decreased, while that under the forefoot increased when subjects ran barefoot or with Vibram FiveFingers™, hence with a lower drop and lower heel height. Alternatively, the other subjects would opt for a more ‘controlled’ RFS aiming to moderate impact at foot strike (lower PMA and PHA). To our knowledge, this ‘controlled rearfoot strike’ theory, which supposes a more vertical tibia placement at the moment of foot landing while keeping a heel strike, has not been investigated yet. Video analysis could help verify this hypothesis. However, it remains that in the present study, the flat-midsole shoes used, which offers no protection under the heel, led the runners to decrease shock acceleration beneath the heel and shock propagation between the heel and the tibia.

Evolution through the 3-month period of vertical ground reaction force (a), tibial acceleration (b), heel acceleration (c) and metatarsal acceleration (d) for the most typical subject of the SHOES group (male 73.4 kg, PRS 3.14 m s−1) at each measurement session. Relative changes from pre-training at 1, 2 and 3 months for this subject were, respectively, −1.1, −32.6 and −39.2 % for PHA; 13.6, 11.8 and 1.6 % for PMA; −0.8, 47.8 and 7.9 % for PTA; 5.3, −10.5 and 5.3 % for T hm; −4.4, −15.5 and −17.1 % for SPV
The MFS running pattern has specific, consistently observed characteristics: absence of impact peak (Dickinson et al. 1985; Altman and Davis 2011; Giandolini et al. 2013); lower LR (Lieberman et al. 2010; Giandolini et al. 2013); higher triceps surae activity concomitant with a lower tibialis anterior activity, which induces a more plantarflexed landing (De Wit et al. 2000; Lieberman et al. 2010; Giandolini et al. 2013); higher peak pressure underneath the metatarsal heads/midfoot parallel to a lower pressure beneath the heel/rearfoot (De Wit et al. 2000; Hennig and Milani 1995; Squadrone and Gallozzi 2009). The conscious and progressive adoption of a MFS over the 3-month intervention had no effect on any of the mechanical variables studied (be it kinematics or impact variables). It seems that subjects strived to midfoot strike but they never naturally adopted a consistent and systematic MFS pattern. These results are different than those presented by Davis (2005), Crowell et al. (2010) and Crowell and Davis (2011), who used a gait retraining on treadmill with real-time feedback (tibial peak acceleration). These authors consistently observed decreases in LR and tibial peak acceleration during 5- and 10-min running bouts using real-time visual feedback (Davis 2005; Crowell et al. 2010). They also observed a 20–50 % decrease in these two parameters between the completion of a 2-week, eight-session lab retraining and 1-month post-retraining. However, in this study, subjects were instructed not to run outside of their training sessions during the 2-week retraining period and to run at least 16 km with their new ‘reduced loading gait pattern’ before they returned for their one-month post-retraining analysis. This gait retraining protocol is therefore very different from the one used here which aimed to be a simple, accessible and easy-to-perform method for the subjects. It is also worth mentioning that these studies never considered the running pattern but only focused on impact reduction. Moreover, the decrease in PRS observed here in TRAIN at 2 and 3 months (−4.39 ± 3.81 and −7.36 ± 4.94 %, p < 0.03, respectively) remains somewhat difficult to explain. Besides, the protocol itself could explain the lack of kinetic and kinematic changes in TRAIN subjects. The only focus on the foot strike pattern could be a limit of the retraining program proposed here, which neglected all the other features of the MFS pattern. As recently detailed by Rothschild (2012) for a transition from shod to barefoot running (which is, from a foot strike pattern point of view, a situation comparable to a RFS-to-MFS transition), it is useful to focus the gait retraining on all the specific features of MFS: flatter touchdown, higher stride frequency, higher ankle flexibility, higher triceps surae activation. Thus, a painless and efficient transition towards a midfoot pattern should be achieved with specific preparatory exercises and drills allowing pluralistic tissue adaptations (for more details, see Rothschild 2012). Although not observed in the present study, it seems that a complete and progressive gait retraining could lead to a change of running pattern. As for the other group, our results showed important inter-individual difference indicating that individuals reacted very differently to the intervention proposed. For instance, post-training 95 % confidence intervals for relative changes were ranged from −51.7 to 48.7 % for PMA, from −28.8 to 27.7 % for PHA, from −47.3 to 44.4 % for PTA and from −34.2 to 30.1 % for LR. In contrast with gait retraining, our findings highlight the likely efficiency of flat-midsole footwear in the impact reduction beneath the heel. It should be noted that basically both groups kept a RFS through the 3 months, this being highlighted by a sustained impact peak on the VGRF curves.
Subjects’ medical and postural follow-up was an important part of our study. Most of the subjects reported calf, knee and/or shin pains, and muscle soreness during the first month of the protocol (Table 4). The main painful sites reported over the 3-month program by both SHOES and TRAIN subjects were shin (30.8 %) and calf (25.0 %). However, these pains were endurable and rarely stopped subjects in their training process. They were largely attenuated during the last 2 months. Only one female subject of the TRAIN group had to stop the experiment after twelve training sessions because of painful shin splints, an injury she had suffered several months before the inclusion session. It is also worth mentioning that an increase in overall postural alterations was observed in both groups. At 1 month, the osteopathic follow-up showed postural alterations in both groups (data not presented). This alteration was even larger at 2 and 3 months, especially in the TRAIN group. It seems that, in the long-term, both flat-midsole footwear and foot strike retraining had effects on subjects’ posture and also on the musculoskeletal system and more particularly on the triceps surae and tibial periosteum. A systematic review by Moen et al. (2009) shows that shin splints, described as pains in the medial aspect of the tibia during or after exercise and characterized by a periosteum inflammation, could be caused by an important traction of the soleus, tibialis posterior and flexor digitorum longus muscles on the periosteum. A study performed on three cadavers showed a higher strain on the periosteum in parallel with higher tensions applied on the tendons of these three muscles (Bouche and Johnson 2007). In addition, these muscles contribute to ankle plantarflexion, a motion that is more pronounced in MFS pattern. Interestingly, a case report by Cibulka et al. (1994) highlighted a possible link between shin splints development and FFS pattern. As a consequence, it cannot be ruled out that an RFS-to-MFS transition could potentially expose subjects to shin splints. Note that Moen et al. (2009) reported that the risk of shin splints is increased by a higher plantarflexion, and that women and people with history of shin splints are more exposed to this type of injury. It is therefore interesting to point out that the only subject excluded from the present protocol was a female with a recent history of shin splints, who was randomly assigned to the MFS group, i.e. instructed to adopt a more plantarflexed running pattern. The other subjects who reported symptomatic pains of medial tibial stress syndrome (shin splints) seemed to have correctly adapted to the new shoe or to the new pattern imposed. Other extrinsic risk factors of shin splints had been highlighted by Moen et al. (2009), but not investigated: duration, intensity, surface and footwear. The present study brings new insights into the latter factor: an important footwear change (especially as to the drop height) should be progressive in order to avoid overuse injuries such as shin splints. Even if no tendinopathy was reported here, the increase in triceps surae activity characterizing the MFS pattern (Giandolini et al. 2013) is thought to potentially induce Achilles tendonitis (Daoud et al. 2012; Goss and Gross 2012b). That said, it seems that the progressive program used here allowed us to limit the ‘calf and tendons pains’ and in turn the onset of associated injuries.
A recent systematic review (Lopes et al. 2012) discusses the main running-related musculoskeletal injuries. Most of them are related to overuse (i.e. overloading the musculoskeletal structures). In sprinters, middle-distance and marathon runners, medial tibial stress syndrome and Achilles tendonitis have an incidence ranging from 13.6 to 20 % and from 9.1 to 10.9 %, respectively, and a prevalence of 9.5 % for medial tibial stress syndrome and ranging from 6.2 to 9.5 % for Achilles tendonitis. Contrastingly, tibial stress fractures have an incidence of 9.1 % and a prevalence of 4.5 %. In ultra-marathon runners of a 5- to 8.5-day race, the prevalence of medial tibial stress syndrome prevalence was 7.8 % and that of Achilles tendonitis was ranging from 2.0 to 18.5 %. Taking all racing distances together, medial tibial stress syndrome and Achilles tendinopathy are the main running-related musculoskeletal injuries with plantar fasciitis (Lopes et al. 2012). This highlights that ‘supposed MFS/FFS-related injuries’ (e.g. shin splints and tendinopathies) are more common than ‘supposed RFS-related injuries’ (e.g. tibial stress fractures), and raises the question of the risk-advantage ratio of a complete and permanent foot strike pattern transition that might shift the anatomical location of potential injury sites. However, according to Lopes et al. (2012), the main ultra-marathon running-related injuries are Achilles tendinopathy and patellofemoral syndrome (prevalence ranging from 7.4 to 15.6 %). Thus, knee injuries are among the most frequent running-related injuries in ultra-marathon runners. According to Goss and Gross (2012b), knee joint moment decreases when runners midfoot strike because of an increased knee flexion at foot landing. Furthermore, it was observed that experimented minimalist runners were using a more anterior foot strike pattern and were approximately three times less likely to sustain running-related injuries (especially at the knee) than runners wearing classic cushioned shoes (Goss and Gross 2012a). This MFS pattern may be useful for decreasing the overall impact but an RFS-to-MFS transition might, however, be done with extreme caution in order avoid a sudden overstress of soft tissues.
One of the main limits of this study is the impossibility to individually follow the subjects during their training sessions, especially for the TRAIN group. It is worth mentioning that there is a risk that some of the TRAIN subjects consciously decided and tried to adopt an MFS (as required to by the experimenters), but did not succeed, in fact. Indeed, it was observed that 31 % of runners are wrong when asked to report their actual running pattern (Goss and Gross 2012a). The content of the program for TRAIN subjects (only focused on foot strike) may also represent a limit since total effective running time with the intervention was ~15 % lower (see “Methods”), but this emphasizes the necessity of a more complete retraining, as advocated by Rothschild (2012). Last, we cannot rule out that performing the measurements on a treadmill while subjects did their running program on the field may also have influenced the results. However, subjects were their own controls for the long-term interventions tested (TRAIN and SHOES), and our protocol design mixing field training and treadmill measurements likely did not influence the comparisons studied. Furthermore, it must be noticed that the present study is among the rare ones to propose a long-term follow-up and not focus only on acute changes. We think that the drawbacks listed here are outweighed by the advantage of possibly discussing adaptations to a 3-month intervention, which had hitherto not been done. Last, our findings show that SHOES subjects seemed to adapt to the new shoes after an ~6-h training period (total effective running time) wearing the shoes. To our knowledge, the previous studies investigated footwear principally in acute conditions (e.g. Hennig and Milani 1995; De Wit et al. 2000; Hamill et al. 2011; Giandolini et al. 2013). We would therefore recommend a longer habituation period for future researches about the effect of footwear on running mechanics.
Conclusion
Running with flat-midsole footwear (i.e. low-drop/low-heel height shoes) during 3 months resulted in an ~30 % lower shock magnitude at the heel, and an ~12 % lower shock wave propagation speed. These results were observed from the second month only, as if subjects needed a significant period of time to adapt to the new footwear. In addition, during the first month, the intervention altered their running pattern. On the opposite, the foot strike retraining proposed, aiming at an RFS-to-MFS transition, induced no change on average for the group, despite the high intra-individual variability in the responses observed, which suggests that runners individually adopted very different strategies while given the same instruction. Concerning the effects on musculoskeletal structures, even if several subjects reported pains mainly located at the shin and calf, likely resulting from natural tissue adaptations, the long-term interventions proposed seem to have been progressive enough to avoid the onset of running-related injuries. Reported pains and observed postural disorders, however, occurred as a consequence of the alterations conducted by the two interventions but tended to normalize after 2 months. That said, in view of the obvious risk of collateral injuries, we strongly recommend athletes and practitioners to consider a progressive change in foot strike pattern on an individual basis, according to whether or not this transition one could be really beneficial for the runner in terms of injury prevention and/or reduction.
Abbreviations
- BW:
-
Body weight
- F max :
-
Maximal vertical ground reaction force
- F q :
-
Step frequency
- F z1 :
-
Magnitude of impact force peak
- LR:
-
Vertical mean loading rate
- MFS:
-
Midfoot strike
- PHA:
-
Peak heel acceleration
- PMA:
-
Peak metatarsal acceleration
- PTA:
-
Peak tibial acceleration
- PRS:
-
Preferred running speed
- RFS:
-
Rearfoot strike
- SPV:
-
Shock propagation velocity between heel and tibia
- t c :
-
Contact time
- t a :
-
Aerial time
- \(t_{{f}_{z1}}\) :
-
Time to impact peak
- T hm :
-
Time between heel and metatarsals peak accelerations
- VGRF:
-
Vertical ground reaction force
References
Altman AR, Davis IS (2011) Comparing barefoot running to an altered strike patterns. Med Sci Sports Exerc 43(5):S717
Anderson T (1996) Biomechanics and running economy. Sports Med 22(2):76–89
Ardigo LP, Lafortuna C, Minetti AE, Mognoni P, Saibene F (1995) Metabolic and mechanical aspects of foot landing type, forefoot and rearfoot strike, in human running. Acta Physiol Scand 155(1):17–22
Belli A, Bui P, Berger A, Geyssant A, Lacour JR (2001) A treadmill ergometer for three-dimensional ground reaction forces measurement during walking. J Biomech 34(1):105–112
Bennell K, Crossley K, Jayarajan J, Walton E, Warden S, Kiss ZS, Wrigley T (2004) Ground reaction forces and bone parameters in female with tibial stress fracture. Med Sci Sports Exerc 36(3):397–404
Bouche RT, Johnson CH (2007) Medial tibial stress syndrome (tibial fasciitis): a proposed pathomechanical model involving fascial traction. J Am Podiatr Med Assoc 97(1):31–36
Brukner P, Bradshaw C, Khan KM, White S, Crossley K (1996) Stress fractures: a review of 180 cases. Clin J Sport Med 6(2):85–89
Cibulka MT, Sinacore DR, Mueller MJ (1994) Shin splints and forefoot contact running: a case report. J Orthop Sports Phys Ther 20(2):98–102
Crossley K, Bennell KL, Wrigley T, Oakes BW (1999) Ground reaction forces, bone characteristics, and tibial stress fracture in male runners. Med Sci Sports Exerc 31(8):1088–1093
Crowell HP, Davis IS (2011) Gait retraining to reduce lower extremity loading in runners. Clin Biomech (Bristol, Avon) 26(1):78–83
Crowell HP, Milner CE, Hamill J, Davis IS (2010) Reducing impact loading in running with the use of real visual time feedbacks. J Orthop Sports Phys Ther 40(4):206–213
Daoud AI, Geissler GJ, Wang F, Saretsky J, Daoud YA, Lieberman DE (2012) Foot strike and injury rates in endurance runners: a retrospective study. Med Sci Sports Exerc 44(7):1325–1334
Davis IS (2005) Gait retraining in runners. Orthop Pract 17:8–13
Davis I, Milner C, Hamill J (2004) Does increased loading rate lead to tibial stress fractures? A prospective study. Med Sci Sports Exerc S36:S58
De Wit B, De Clercq D, Aerts P (2000) Biomechanical analysis of the stance phase during barefoot and shod running. J Biomech 33(3):269–278
Derrick TR, Mercer JA (2004) Ground/foot impacts: measurement, attenuation, and consequences. Med Sci Sports Exerc 36(5):830–831
Dickinson JA, Cook SD, Leinhardt TM (1985) The measurement of shock waves following heel strike while running. J Biomech 18(6):415–422
Divert C, Mornieux G, Baur H, Mayer F, Belli A (2005) Mechanical comparison of barefoot and shod running. Int J Sports Med 26(7):593–598
Franz JR, Wierzbinski CM, Kram R (2012) Metabolic cost of running barefoot versus shod: is lighter better? Med Sci Sports Exerc 44(8):1519–1525
Fuchs RK, Snow CM (2002) Gains in hip bone mass from high-impact training are maintained: a randomized controlled trial in children. J Pediatr 141(3):357–362
Fuchs RK, Bauer JJ, Snow CM (2001) Jumping improves hip and lumbar spine bone mass in prepubescent children: a randomized controlled trial. J Bone Miner Res 16(1):148–156
Giandolini M, Arnal PJ, Millet GY, Peyrot N, Samozino P, Dubois B, Morin JB (2013) Impact reduction during running: efficiency of simple acute interventions in recreational runners. Eur J Appl Physiol 113(3):599–609
Goss DL, Gross MT (2012a) Relationships among self-reported shoe type, footstrike pattern, and injury incidence. US Army Med Dep, 25–30
Goss DL, Gross MT (2012b) A review of mechanics and injury trends among various running styles. US Army Med Dep, 62–71
Hamill J, Russell EM, Gruber AH, Miller R (2011) Impact characteristics in shod and barefoot running. Footwear Sci 3(1):33–40
Hasegawa H, Yamauchi T, Kraemer WJ (2007) Foot strike patterns of runners at the 15-km point during an elite-level half marathon. J Strength Cond Res 21(3):888–893
Heiderscheit BC, Chumanov ES, Michalski MP, Wille CM, Ryan MB (2011) Effects of step rate manipulation on joint mechanics during running. Med Sci Sports Exerc 43(2):296–302
Hennig EM, Milani TL (1995) In-shoe pressure distribution for running in various types of footwear. J Appl Biomech 11:299–310
Horvais N, Samozino P (2013) Effect of midsole geometry on foot strike pattern and running kinematics. Footwear Sci (in press)
Hreljac A (2004) Impact and overuse injuries in runners. Med Sci Sports Exerc 36(5):845–849
Kasmer ME, Liu XC, Roberts KG, Valadao JM (2012) Foot-strike pattern and performance in a marathon. Int J Sports Physiol Perform (in press)
Ker RF, Bennett MB, Bibby SR, Kester RC, Alexander RM (1987) The spring in the arch of the human foot. Nature 325(7000):147–149
Larson P, Higgins E, Kaminski J, Decker T, Preble J, Lyons D, McIntyre K, Normile A (2011) Foot strike patterns of recreational and sub-elite runners in a long-distance road race. J Sports Sci 29(15):1665–1673
Lieberman DE (2012) What we can learn about running from barefoot running: an evolutionary medical perspective. Exerc Sport Sci Rev 40(2):63–72
Lieberman DE, Venkadesan M, Werbel WA, Daoud AI, D’Andrea S, Davis IS, Mang’eni RO, Pitsiladis Y (2010) Foot strike patterns and collision forces in habitually barefoot versus shod runners. Nature 463(7280):531–535
Lohman EB 3rd, Balan Sackiriyas KS, Swen RW (2011) A comparison of the spatiotemporal parameters, kinematics, and biomechanics between shod, unshod, and minimally supported running as compared to walking. Phys Ther Sport 12(4):151–163
Lopes AD, Hespanhol Junior LC, Yeung SS, Costa LO (2012) What are the main running-related musculoskeletal injuries? A systematic review. Sports Med 42(10):891–905
Mattila VM, Sillanpää PJ, Salo T, Laine HJ, Mäenpää H, Pihlajamäki H (2011) Can orthotic insoles prevent lower limb overuse injuries? A randomized-controlled trial of 228 subjects. Scand J Med Sci Sports 21(6):804–808
Milner CE, Ferber R, Pollard CD, Hamill J, Davis IS (2006) Biomechanical factors associated with tibial stress fracture in female runners. Med Sci Sports Exerc 38(2):323–328
Moen MH, Tol JL, Weir A, Steunebrink M, De Winter TC (2009) Medial tibial stress syndrome: a critical review. Sports Med 39(7):523–546
Morin JB, Samozino P, Peyrot N (2009) Running pattern changes depending on the level of subjects’ awareness of the measurements performed: a “sampling effect” in human locomotion experiments? Gait Posture 30(4):507–510
Nigg BM (1986) Biomechanics of running shoes. Human Kinetics Publishers, Windsor, pp 140–141
Perl DP, Daoud AI, Lieberman DE (2012) Effects of footwear and strike type on running economy. Med Sci Sports Exerc 44(7):1335–1343
Richards CE, Magin PJ, Callister R (2009) Is your prescription of distance running shoes evidence-based? Br J Sports Med 43(3):159–162
Rothschild C (2012) Running barefoot or in minimalist shoes: evidence or conjecture? Natl Strength Cond Assoc 34(2):8–17
Samozino P, Morin J-B, Mermet V, Barla C, Ouillon R, Baly L, Belli A (2008) What is the best parameter to quantify shocks during heel-toe running? 13 h annual congress of the European College of Sport Science. Estoril, Portugal
Saunders PU, Pyne DB, Telford RD, Hawley JA (2004) Factors affecting running economy in trained distance runners. Sports Med 34(7):465–485
Schwellnus MP, Jordaan G, Noakes TD (1990) Prevention of common overuse injuries by the use of shock absorbing insoles. A prospective study. Am J Sports Med 18(6):636–641
Shorten MR, Mientjes MIV (2011) The ‘heel impact’ force peak during running is neither ‘heel’ nor ‘impact’ and does not quantify shoe cushioning effects. Footwear Sci 3(1):41–58
Snyder RA, Koester MC, Dunn WR (2006) Epidemiology of stress fractures. Clin Sports Med 25(1):37–52
Squadrone R, Gallozzi C (2009) Biomechanical and physiological comparison of barefoot and two shod conditions in experienced barefoot runners. J Sports Med Phys Fitness 49(1):6–13
van Gent RN, Siem D, van Middelkoop M, van Os AG, Bierma-Zeinstra SM, Koes BW (2007) Incidence and determinants of lower extremity running injuries in long distance runners: a systematic review. Br J Sports Med 41(8):469–480
von Tscharner V, Goepfert B, Nigg BM (2003) Changes in EMG signals for the muscle tibialis anterior while running barefoot or with shoes resolved by non-linearly scaled wavelets. J Biomech 36(8):1169–1176
Zapdoor AB, Nikooyan AA (2011) The relationship between lower-extremity stress fractures and the ground reaction force: a systematic review. Clin Biomech 26:23–28
Acknowledgments
We are grateful to Drs. Pascal Edouard, Jean-Claude Chatard, Amaury Mazet, and David Hupin, from the Service de Physiologie Clinique, Médecine du Sport—Myologie, CHU Bellevue, Saint-Etienne for their help in the inclusion sessions and medical follow-up of the study. Salomon SAS supported this study through an MSc studentship grant allocated to Marlène Giandolini.
Author information
Authors and Affiliations
Corresponding author
Additional information
Communicated by Jean-René Lacour.
Appendix
Appendix
See Fig. 4.

Description of training programs through the thirty-nine training sessions for TRAIN (a) and SHOES (b). For TRAIN, black and grey bars refer to the running times (within the 30-min training session) with a MFS pattern (intervention) and with a freely chosen pattern (i.e. natural RFS pattern), respectively. For SHOES, black and grey bars refer to the running times (within the 30-min training session) with the low-drop/low-heel height shoes (intervention) and with the subjects’ usual shoes, respectively. Measurement sessions (pre-training, 1, 2 and 3 months) are also presented
Rights and permissions
About this article
Cite this article
Giandolini, M., Horvais, N., Farges, Y. et al. Impact reduction through long-term intervention in recreational runners: midfoot strike pattern versus low-drop/low-heel height footwear. Eur J Appl Physiol 113, 2077–2090 (2013). https://doi.org/10.1007/s00421-013-2634-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00421-013-2634-7