
Abstract
During voluntary contractions, motor neurone activity is modulated by descending input and sensory feedback. Impaired excitatory afferent feedback with ageing may, therefore, alter motor control. This study investigated the age-related changes in afferent feedback through the recording of reflex responses during voluntary muscle activation. Short- and long-latency components of the stretch reflex and Hoffmann reflex (H-reflex) were recorded during voluntary contractions (10% of maximal voluntary contraction; MVC) of the ankle dorsiflexor muscles of young and elderly adults (≥70 years). Furthermore, the modulation of spinal reflex excitability was analyzed at different torque levels (10–50% MVC). The short-latency stretch reflex and the H-reflex areas were similar in the two age groups at 10% MVC whereas the area of the long-latency component of the stretch reflex augmented with ageing (P < 0.05). However, the area of the H-reflex increased linearly with the level of contraction up to 50% MVC in young adults, whereas it slightly increased to 30% MVC and plateaued thereafter in elderly adults. The absence of age-related changes in the short-latency stretch reflex and H-reflex areas suggests that the reflex circuitry and the sensitivity of the muscle spindles are not substantially affected by ageing. The modest increase in the H-reflex area with the contraction intensity in elderly adults, however, indicates that the modulation of afferent feedback is reduced with advancing age. This observation, associated with a greater long-latency stretch reflex, suggests that elderly adults rely more on central than peripheral mechanisms to regulate motor output of the dorsiflexor muscles.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The age-related decline in motor function (Enoka et al. 2003; McNeil et al. 2007; Nardone et al. 1995; Stelmach et al. 1989; Tang and Woollacott 1998, 1999) is not only associated with alterations affecting the muscular (McNeil et al. 2007) but also the neural system (Enoka et al. 2003). During voluntary contractions and responses to sudden perturbations of a limb or whole body, motor neurone activity is modulated by both the descending input and sensory feedback (Nielsen 2004). In that context, it is well known that the excitatory afferent input from the muscle spindles are intensified during muscle activation, thereby, contributing to increased motor neurone activity (Macefield et al. 1993; Nielsen 2004). However, this afferent feedback is specifically modulated, depending on the task being performed (Angulo-Kinzler et al. 1998; Burke et al. 1978; Doemges and Rack 1992; Zehr and Stein 1999), by presynaptic inhibitory mechanisms (Pierrot-Desseilligny and Burke 2005; Stein 1995). Therefore, due to the important role of excitatory afferents in motor control, their impairment with advancing age may contribute to declines in motor skills and performance.
In humans, an indirect way to measure changes in excitatory afferents from muscle spindles during voluntary activation is to record reflex responses, obtained through a rapid stretch of the active muscle. The reflex response is composed of a short-latency component involving a spinal pathway (Pierrot-Desseilligny and Burke 2005) and a long-latency component involving a supraspinal pathway, at least in upper limb muscles (Matthews 1991) and in the tibialis anterior (Petersen et al. 1998). Studies investigating the effect of ageing reported contradictory results as the size of the short-latency stretch reflex either decreased (Corden and Lippold 1996) or did not change in elderly adults (≤70 years; Kawashima et al. 2004; Lin and Sabbahi, 1998; Obata et al. 2010). Similarly, the size of the long-latency stretch reflex increased (Kawashima et al. 2004; Lin and Sabbahi 1998; Obata et al. 2010) or did not change with ageing (Corden and Lippold 1996).
Another way to investigate changes in excitability of this spinal reflex pathway is to record the H-reflex induced by electrical stimulation of the Ia fibres (Pierrot-Desseilligny and Burke 2005). The advantage of the H-reflex is that it bypasses the muscle spindles and more directly probes changes in motor neurones excitability and synaptic transmission. As for the stretch reflex, reports on the effect of ageing on the H-reflex amplitude, normalized to the maximal muscle motor potential (M max), are divergent. Indeed, some authors reported a decrease (Angulo-Kinzler et al. 1998; Kido et al. 2004; Sabbahi and Sedgwick 1982) whereas others did not observe any significant difference between young and elderly adults (Kawashima et al. 2004; Scaglioni et al. 2003).
The discrepancy between the results of these studies may be due to factors such as the inter-subject variability of reflex responses, differences in subjects’ age and physical condition, the contraction levels, and the muscle group tested. Changes in reflex responses with advancing age have been extensively investigated in the ankle plantar flexor muscles (Angulo-Kinzler et al. 1998; Kawashima et al. 2004; Kido et al. 2004; Lin and Sabbahi 1998; Obata et al. 2010; Sabbahi and Sedgwick 1982; Scaglioni et al. 2003). Surprisingly, very little is known about the adaptation of the dorsiflexor muscles during ageing (Obata et al. 2010). However, these muscles play an important role in locomotion (Ceccato et al. 2009; Hase and Stein 1998; Zehr and Stein 1999) by lifting the foot during the swing phase and preventing tripping. They are also involved in postural responses to stance perturbations (Nardone et al. 1995; Stelmach et al. 1989) and unexpected slips during walking (Tang and Woollacott 1998, 1999). In that context, it has been suggested that the decline in their maximal capacity of torque production with advancing age contributes to increase the risk of fall (Billot et al. 2010; Daubney and Culham 1999).The ability to adjust their activation as a function of the task being performed is thus essential for activities of daily life.
The purpose of the present study was therefore to improve the understanding of age-related changes (≥70 years) in lower limb muscles by comparing electrically and mechanically induced reflexes and the modulation of afferent feedback in the tibialis anterior muscle of elderly and young adults.
Materials and methods
Subjects
Fourteen young adults (seven women; aged 20–35 years; height 1.75 ± 0.09 m) and fourteen elderly adults (eight women; aged 70–87 years; height 1.69 ± 0.07 m) were recruited for the study. All subjects participated in two sessions, one for familiarization and one for data collection. During the familiarization session, subjects practiced the different isometric contractions levels, and also experienced electrical stimulation. Subjects were not engaged in any strenuous locomotor activity for at least 24 h before the experimental session. All subjects were healthy and without neuromuscular disorders at the time of participation in the investigation. Elderly adults were living at home, walked daily without the use of an assistive device and were able to do light household activities by themselves. The protocol of the current study was approved by local Ethics Committee and all subjects gave informed consent prior to participate in the investigation.
Experimental apparatus
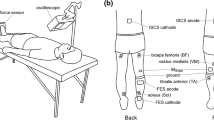
A motor-driven, computer-controlled ergometer (type HDX 115C6; Hauser Compax 0260 M-E2; Offenburg, Germany), adapted for the ankle joint, was used in this study. The device, which was equipped with a footplate fixed to the rotational axis of the motor, was used to record the angular displacement, the torque generated and to induce a quick stretch of the dorsiflexor muscles by a rapid angular displacement of the ankle joint. During the experimental session, the subject sat on a chair in a slightly reclined position with the foot of the right leg tightly attached to the footplate and held in place by a heel block. The plate was inclined at an angle of 45° to the floor, and the subject’s position was adjusted to obtain ankle and knee angles of about 90° (neutral position) and 50–60° (full extension = 0°), respectively.
Mechanical and electromyographic recordings
A linear potentiometer and strain-gauge transducer (sensitivity: 0.018 V/N m; linear range: 0–200 N m) mounted on the rotational axis of the motor were used to measure the angular displacement of the ankle attached to the footplate and the torque produced by the dorsiflexor muscles during voluntary contractions, respectively. The surface electromyographic (EMG) activity was recorded from the tibialis anterior muscle by means of two silver-disc electrodes (8 mm in diameter) positioned 2 cm apart over the muscle belly. The reference electrode (2 × 3-cm silver plate) was attached between the stimulating electrodes and the EMG recording electrodes. The EMG signals were amplified (×1,000) and filtered (10 Hz–1 kHz) by a custom made differential amplifier. The torque, the displacement and the EMG signals were simultaneously recorded by a computer at a sampling rate of 2,000 Hz and were analyzed offline by using the AcqKnowledge data analysis software (model MP150; Biopac Systems, Santa Barbara, CA).
Experimental protocol
The experimental session started with the recording of two to three isometric maximal voluntary contractions (MVC) of the dorsiflexor muscles and the corresponding EMG activity of the tibialis anterior muscle. After 5 min of rest, the stretch reflex responses were recorded in the tibialis anterior muscle in response to a quick stretch of the dorsiflexor muscles at an angular velocity of 200°/s and a range of motion of 10° while the subject was maintaining an isometric contraction of 10% MVC. This procedure was used to facilitate the reflex occurrence by the activation of α-motor neurones (Burke et al. 1989). The 200°/s velocity was chosen because it evoked clear reflex responses in both elderly and young adults. The ankle rotation was fixed at 10° as it allowed a stretch of sufficient duration (>40 ms) to evoke a long-latency component (Lee and Tatton 1982). To compare stretch reflex responses from young and elderly adults, a total of 40 responses evoked every 5 s were recorded during two successive sets of contractions (10% MVC) separated by a 2-min rest period. For the H-reflex, the same number of responses was recorded during series of two contractions performed at 10, 20, 30, 40 and 50% MVC to investigate its modulation during varying muscle activations. The duration of each contraction was ~20 s and target torques were presented in a counterbalanced order. Reflex responses were induced by a 3-Hz stimulation train (rectangular 1-ms pulses) delivered to the deep peroneal nerve through two electrodes (silver discs, 8-mm diameter), with the cathode located over the deep peroneal nerve close to the head of the fibula and the anode placed on the opposite side of the leg. The stimulation intensity was set at 10–15% above motor threshold (intensity range: 4–10 mA). The stretch reflex and H-reflex responses obtained at each contraction level were then rectified and averaged. M max were also recorded in response to a supramaximal electrical stimulation (intensity range: 8–20 mA) of the deep peroneal nerve.
Measurements
The reflex onset was defined as the first major deflection in the rectified EMG activity at around 40 and 35 ms for the stretch and H-reflex, respectively. The end of the whole reflex response was defined as the time when the EMG activity returned to the mean background EMG activity (BG) corresponding to the contraction level. The stretch reflex was composed of a short-latency (SL) and a long-latency (LLtot) component (Fig. 1). The LLtot component was distinguishable from the SL component by a sudden decrease followed by a sharp increase in EMG activity at ~65 ms (Zuur et al. 2009). For most of the subjects (12 young and 10 elderly), it was possible to subdivide LLtot into two components that were termed, respectively, LL1 and LL2, the latter starting at ~90 ms (Zuur et al. 2009).

Illustration of rectified and averaged 40 EMG responses of the tibialis anterior to a quick stretch of the dorsiflexor muscles (a) and an electrical stimulation of the deep peroneal nerve (H-reflex; b) in a young (grey line) and an elderly (black line) subject. The solid vertical lines in a and b correspond to the onset of the stretch and electrical stimulation, respectively. The stretch reflex is composed of a short- (SL) and a long-latency (LLtot) component. In most of the subjects, LLtot was subdivided into two components (LL1 and LL2). In a, the solid horizontal line corresponds to the EMG baseline when the subject was at rest and the trace below the stretch reflex response represents the ankle angular displacement
The absolute area of each reflex component was calculated as the difference between the rectified reflex response and the area of the BG corresponding to the contraction level measured prior to the stimulus for the same duration as the reflex response (Fig. 1; Lin and Sabbahi 1998; Balestra et al. 1992). Stretch reflexes were then expressed as a percentage of the EMG area measured during a 1-s epoch during the MVC plateau and the H-reflex response was expressed as a percentage of the corresponding M max area since both responses were electrically induced. This procedure controls for differences in muscle membrane ionic processes between elderly and young adults and allowed for the estimation of age-related changes in excitability of the reflex pathway.
Statistics
To test for statistical differences between elderly and young adults, a Student t-test or a non parametric Mann–Whitney test, when data were not normally distributed, was used to compare M max area, reflex areas and latencies recorded at 10% MVC. A two-factor ANOVA (age × contraction level) with repeated measures on contraction level was used to compare changes in the normalized H-reflex area at the different contraction levels. When appropriate, a Tukey post-hoc test was used to determine differences among pairs of means. The rates of increase in average BG for the different contraction levels were compared by an ANCOVA. Data are reported as means ± SD within the text and means ± SE in the figures.
Results
MVC torque and corresponding EMG activity
The mean MVC torque of the dorsiflexor muscles was not significantly (P = 0.17) different between elderly (33.4 ± 8.4 N m) and young subjects (39.0 ± 12.0 N m). The corresponding average EMG activity of the tibialis anterior was similar in the two age groups (349.3 ± 91.4 vs. 320.0 ± 95.9 μV in elderly and young subjects, respectively; P = 0.42).
Stretch reflex
The onset latencies for the SL and LLtot components of the stretch reflex were longer in the elderly compared with the young adults (7.7 and 4.6%, respectively), however, the difference was statistically significant only for SL (Table 1; P < 0.05). In most of the elderly (n = 10) and young (n = 12) subjects, it was possible to clearly distinguish two components (LL1 and LL2) in LLtot. The onset latency for LL2 tended to be longer in elderly than in young adults (Table 1; P = 0.08). The duration of SL was similar in elderly and young adults whereas it was significantly longer (P = 0.05) for LLtot in the aged group (18.4%; Table 1).
The area of the stretch reflex components was also differently affected by ageing. Although SL area did not differ between groups (P = 0.15; Fig. 2), LLtot area was significantly greater in elderly adults (63.1%, P < 0.05; Fig. 3).

EMG area for SL (a) and H-reflex (b) recorded in the tibialis anterior of young and elderly adults. Data are expressed as percentage of maximum during MVC (% EMGMVC)

EMG area for LLtot (a), and LL1 and LL2 (b) recorded in the tibialis anterior of young and elderly adults and expressed as percentage of maximum during MVC (% EMGMVC). LLtot was subdivided in LL1 and LL2 in 12 young and 10 elderly subjects, respectively. LL1 area was similar in both groups whereas LL2 was significantly greater in elderly subjects. *Significant difference between young and elderly adults, P < 0.05
When LLtot was subdivided into LL1 and LL2 components, it appeared clearly that the age-related effect was more pronounced for LL2. Indeed, LL1 area did not change significantly with age (P = 0.44) whereas LL2 area was greater in elderly as compared with young adults (106.7%, P = 0.05; Fig. 3). As a consequence of the different change of SL and LLtot areas with ageing, SL/LLtot ratio was significantly lower in elderly (0.37 ± 0.31) compared with young adults (0.76 ± 0.69, P < 0.05).
H-reflex
The onset latency of the H-reflex was longer in elderly than in young adults (10.9%, P < 0.01) whereas its duration was similar for the two age groups (Table 1). The absolute H-reflex area tended to be smaller with advancing age (0.61 ± 0.50 vs. 0.37 ± 0. 24 μV s in young and elderly subjects, respectively; P = 0.08). However, when the H-reflex area was normalized to the M max area the difference between the two age groups disappeared (Fig. 2). This result is mainly due to the fact that M max area was significantly smaller in the aged group (16.5 ± 5.9 and 11.4 ± 3.6 μV s in young and elderly subjects, respectively; P < 0.05).
The modulation of the H-reflex during contraction levels ranging from 10 to 50% MVC was different in the two age groups (ANOVA age × contraction level, P < 0.001). The normalized H-reflex area increased gradually in young adults throughout the entire range of contraction levels tested (P < 0.05) whereas in elderly adults it increased slightly to 30% MVC (P < 0.05; Fig. 4) and plateaued thereafter. In contrast, the average BG increased linearly in the two age groups as a function of the contraction level (P < 0.001) from 36.2 ± 15.2 μV at 10% MVC to 130.8 ± 61.8 μV at 50% MVC (r = 0.66) and from 48.7 ± 17.7 to 139.3 ± 47.7 μV (r = 0.67), respectively, in young and elderly adults. The rates of increase were similar in the young (2.3 μV/% MVC) and aged groups (2.2 μV/% MVC; ANCOVA, P = 0.85).

Normalized H-reflex area (% M max) expressed as a function of the torque (% MVC) produced by the dorsiflexors of young and elderly adults. H-reflex area increased gradually up to 50% MVC in young adults. In elderly adults it increased slightly to 30% MVC and plateaued thereafter. ANOVA age × contraction level, P < 0.001
Discussion
The main objective of the current study was to compare stretch and electrically induced reflex responses and the modulation of the latter at different levels of muscle activation between young and elderly adults. The main findings are a non significant age-related change in the areas of H-reflex and SL component of the stretch reflex and a lower increase of the H-reflex size in the elderly compared with young adults when muscle activation level was enhanced.
Age-related changes in reflex latencies
The onset latency of the spinal reflex responses recorded while subjects were maintaining a contraction at 10% MVC was greater in the aged group. This observation is in agreement with most of the studies investigating another lower limb muscle (i.e. soleus; Obata et al. 2010; Sabbahi and Sedgwick 1982; Scaglioni et al. 2003). Recently, Obata et al. (2010) also investigated the latency of the tibialis anterior stretch reflex during weak contractions (~10% MVC) and did not observe any significant difference between elderly (66 ms) and young (60 ms) adults. Such long latencies for the tibialis anterior, however, are surprising when compared with our data (~38 and 41 ms in young and elderly subjects, respectively) and those reported for young adults (Petersen et al. 1998; Zuur et al. 2009). Regardless of the discrepancy between studies, the increase in reflex latency with advancing age should be related to the slowing in synaptic transmission and conduction velocity due to degenerative changes affecting sensory and motor fibres (Desmedt and Cheron 1980; Doherty et al. 1994). The smaller change for LLtot latency, compared with SL may reflect differences in central and peripheral age-related alterations of the neural circuits (Desmedt and Cheron 1980).
Age-related changes in the area of the stretch reflex components
In agreement with previous studies investigating the stretch reflex in soleus (Kawashima et al. 2004; Obata et al. 2010) and hand muscles (Corden and Lippold 1996; Lin and Sabbahi 1998), our results showed that the SL and LLtot components of the tibialis anterior recorded at 10% MVC displayed different changes with advancing age. The normalized SL area did not change whereas LLtot area was significantly greater in the elderly compared with young adults. As a consequence, the SL/LLtot ratio was significantly reduced with ageing. When LLtot was subdivided into two components, it appeared that the age-related size increase was mainly observed for the LL2 component (Fig. 3). Results from previous studies combining transcranial magnetic stimulation and stretch reflexes recording, suggest a transcortical pathway for LL2 in the tibialis anterior (Petersen et al. 1998; Zuur et al. 2009), indicating that the greater LL2 area in elderly adults observed in the present study may involve supraspinal mechanisms (Kawashima et al. 2004; Lin and Sabbahi 1998; Obata et al. 2010). The increase of the long-latency reflex component may be an adaptatory mechanism to changes occurring with advancing age. Indeed our results, in agreement with the study of Earles et al. (2001), suggest that elderly adults rely more on the central command than on peripheral mechanisms to regulate motor output. By integrating the response to the somatosensory input at a cortical level, a transcortical reflex pathway may provide an input onto the motor neurone pool more adapted to the specificities of the task than a purely segmental pathway (Chan 1983; Kourtis et al. 2008; Zuur et al. 2009). However, further studies are required to determine the precise neural mechanisms explaining the greater age-related area of the supraspinal reflexes.
Age-related changes in spinal reflexes area
Our results agree with most of previous works that recorded the stretch reflex responses at rest and during low contraction levels and showed non significant age-related difference for the SL component (Kawashima et al. 2004; Lin and Sabbahi 1998; Obata et al. 2010). The absence of a significant age-related decrement in H-reflex area contrasts with some studies (Angulo-Kinzler et al. 1998; Kido et al. 2004; Sabbahi and Sedgwick 1982) but not others (Kawashima et al. 2004; Scaglioni et al. 2003). As already mentioned, this discrepancy may be partly due to the variability of reflex responses, particularly when they are recorded at rest (Toft et al. 1991). For this reason and because it is more functionally relevant (Stein and Thompson 2006), we recorded stretch and H-reflex responses during submaximal contractions. An interesting observation of the current study is that the areas of both SL and H-reflex did not significantly change with advancing age. The pathways involved in these two spinal reflexes differ by the fact that the H-reflex bypasses the muscle spindles while SL does not. A direct comparison of the changes in H-reflex and SL component with ageing can be misleading because spatial and temporal summation of the afferent volleys underlying these two responses and their sensitivity to presynaptic inhibition are different (Pierrot-Desseilligny and Burke 2005; Van Boxtel 1986). However, a conservative interpretation of the absence of significant changes for SL and H-reflex suggests that neither the neural circuit common to the two reflex responses nor the responsiveness of the muscle spindles was significantly affected with ageing. The last hypothesis is supported by Liu et al. (2005), who observed that the number of nuclear bag fibres, responsible for the dynamic sensitivity of primary sensory endings, did not change in human biceps brachii with advancing age. More functional data, showing that the loss of dynamic position sense was smaller than that of static position sense (Verschueren et al. 2002) also support our hypothesis.
Age-related changes in H-reflex modulation
In agreement with data reported in the soleus muscle of young adults by Butler et al. (1993), the H-reflex area increased gradually with muscle torque due to the ‘automatic gain compensation’ mechanism that adjusts the amplitude of reflexes to the contraction level (Matthews 1986). We did not investigate torque levels greater than 50% MVC because previous studies have observed that spinal reflexes size is linearly related with the contraction level up to ~50% MVC (Butler et al. 1993) and to avoid the confounding effect of fatigue. In elderly adults, H-reflex area increased slightly to 30% MVC and plateaued thereafter. This observation is in agreement with studies investigating age-related changes in H-reflex modulation in other muscle groups up to ~15% (Lin and Sabbahi 1998) and ~30% MVC (Angulo-Kinzler et al. 1998). The present results extend these findings to the tibialis anterior muscle for torque levels up to 50% MVC and show that elderly adults modulate differently the excitatory afferents for torque levels greater than 30% MVC. As the BG increased linearly with the contraction intensity (from 10 to 50% MVC) in the two age groups, this difference could be mainly due to mechanisms located before the synapse, between Ia fibres and the motor neurone (i.e. presynaptic mechanism; see Pierrot-Desseilligny and Burke 2005; Stein 1995; Zehr and Stein 1999). A reduced ability to modulate presynaptic inhibition has been indeed suggested in elderly adults (Butchart et al. 1993; Earles et al. 2001).
In conclusion, our results indicate an increase in the latencies of spinal reflexes and different changes in the areas of SL and LL components of the stretch reflex with advancing age which is presumably explained by their partly distinct neural pathways. The non significant change for SL and H-reflex areas suggest that neither the neural circuit common to the two reflex responses nor the responsiveness of the muscle spindles was significantly affected with ageing. Associated with a greater LLtot response in elderly adults, the different age-related modulation of the H-reflex size in function of the intensity of muscle contraction suggests that elderly adults rely more on central than peripheral mechanisms to regulate motor output. However, since task-specific modulation of the excitatory afferent feedback is important for motor control (Macefield et al. 1993; Stein and Thompson 2006; Zehr and Stein 1999), these age-related adaptations in the tibialis anterior muscle may contribute to alter motor skills and postural control in elderly adults.
References
Angulo-Kinzler RM, Mynark RG, Koceja DM (1998) Soleus H-reflex gain in elderly and young adults: modulation due to body position. J Gerontol A 53:M120–M125
Balestra C, Duchateau J, Hainaut K (1992) Effects of fatigue on the stretch reflex in a human muscle. Electroencephalogr Clin Neurophysiol 85:46–52
Billot M, Simoneau EM, Van Hoecke J, Martin A (2010) Age-related relative increases in electromyography activity and torque according to the maximal capacity during upright standing. Eur J Appl Physiol 109:669–680
Burke D, Hagbarth KE, Löfstedt L (1978) Muscle spindle responses in man to changes in load during accurate position maintenance. J Physiol 276:159–164
Burke D, Adams RW, Skuse NF (1989) The effects of voluntary contraction on the H reflex of human limb muscles. Brain 112(Pt 2):417–433
Butchart P, Farquhar R, Part NJ, Roberts RC (1993) The effect of age and voluntary contraction on presynaptic inhibition of soleus muscle Ia afferent terminals in man. Exp Physiol 78:235–242
Butler AJ, Yue G, Darling WG (1993) Variations in soleus H-reflexes as a function of plantarflexion torque in man. Brain Res 632:95–104
Ceccato J, de Sèze M, Azevedo C, Cazalets J (2009) Comparison of trunk activity during gait initiation and walking in humans. PloS One 4:e8193
Chan CWY (1983) Segmental versus suprasegmental contribution to long-latency stretch responses in man. In: Desmedt JE (ed) Motor control mechanisms in health and disease. Raven Press, New York, pp 467–487
Corden DM, Lippold OC (1996) Age-related impaired reflex sensitivity in a human hand muscle. J Neurophysiol 76:2701–2706
Daubney ME, Culham EG (1999) Lower-extremity muscle force and balance performance in adults aged 65 years and older. Phys Ther 79:1177–1185
Desmedt JE, Cheron G (1980) Somatosensory evoked potentials to finger stimulation in healthy octogenarians and in young adults: wave forms, scalp topography and transit times of parietal and frontal components. Electroencephalogr Clin Neurophysiol 50:404–425
Doemges F, Rack PM (1992) Changes in the stretch reflex of the human first dorsal interosseous muscle during different tasks. J Physiol 447:563–573
Doherty TJ, Komori T, Stashuk DW, Kassam A, Brown WF (1994) Physiological properties of single thenar motor units in the F-response of younger and older adults. Muscle Nerve 17:860–872
Earles D, Vardaxis V, Koceja D (2001) Regulation of motor output between young and elderly subjects. Clin Neurophysiol 112:1273–1279
Enoka RM, Christou EA, Hunter SK, Kornatz KW, Semmler JG, Taylor AM, Tracy BL (2003) Mechanisms that contribute to differences in motor performance between young and old adults. J Electromyogr Kinesiol 13:1–12
Hase K, Stein RB (1998) Analysis of rapid stopping during human walking. J Neurophysiol 80:255–261
Kawashima N, Nakazawa K, Yamamoto S, Nozaki D, Akai M, Yano H (2004) Stretch reflex excitability of the anti-gravity ankle extensor muscle in elderly humans. Acta Physiol Scand 180:99–105
Kido A, Tanaka N, Stein RB (2004) Spinal excitation and inhibition decrease as humans age. Can J Physiol Pharmacol 82:238–248
Kourtis D, Kwok HF, Roach N, Wing AM, Praamstra P (2008) Maintaining grip: anticipatory and reactive EEG responses to load perturbations. J Neurophysiol 99:545–553
Lee RG, Tatton WG (1982) Long latency reflexes to imposed displacements of the human wrist: dependence on duration of movement. Exp Brain Res 45:207–216
Lin FM, Sabbahi M (1998) The aging effects on the EMG and mechanical responses of the human wrist flexor stretch reflexes. Electromyogr Clin Neurophysiol 38:323–331
Liu J, Eriksson P, Thornell L, Pedrosa-Domellöf F (2005) Fiber content and myosin heavy chain composition of muscle spindles in aged human biceps brachii. J Histochem Cytochem 53:445–454
Macefield VG, Gandevia SC, Bigland-Ritchie B, Gorman RB, Burke D (1993) The firing rates of human motoneurones voluntarily activated in the absence of muscle afferent feedback. J Physiol 471:429–443
Matthews PB (1986) Observations on the automatic compensation of reflex gain on varying the pre-existing level of motor discharge in man. J Physiol 374:73–90
Matthews PB (1991) The human stretch reflex and the motor cortex. Trends Neurosci 14:87–91
McNeil CJ, Vandervoort AA, Rice CL (2007) Peripheral impairments cause a progressive age-related loss of strength and velocity-dependent power in the dorsiflexors. J Appl Physiol 102:1962–1968
Nardone A, Siliotto R, Grasso M, Schieppati M (1995) Influence of aging on leg muscle reflex responses to stance perturbation. Arch Phys Med Rehabil 76:158–165
Nielsen JB (2004) Sensorimotor integration at spinal level as a basis for muscle coordination during voluntary movement in humans. J Appl Physiol 96:1961–1967
Obata H, Kawashima N, Akai M, Nakazawa K, Ohtsuki T (2010) Age-related changes of the stretch reflex excitability in human ankle muscles. J Electromyogr Kinesiol 20:55–60
Petersen N, Christensen LO, Morita H, Sinkjaer T, Nielsen J (1998) Evidence that a transcortical pathway contributes to stretch reflexes in the tibialis anterior muscle in man. J Physiol 512(Pt 1):267–276
Pierrot-Desseilligny E, Burke DC (2005) The circuitry of the human spinal cord: its role in motor control and movement disorders. Cambridge University Press, Cambridge
Sabbahi MA, Sedgwick EM (1982) Age-related changes in monosynaptic reflex excitability. J Gerontol 37:24–32
Scaglioni G, Narici MV, Maffiuletti NA, Pensini M, Martin A (2003) Effect of ageing on the electrical and mechanical properties of human soleus motor units activated by the H reflex and M wave. J Physiol 548:649–661
Stein RB (1995) Presynaptic inhibition in humans. Prog Neurobiol 47:533–544
Stein RB, Thompson AK (2006) Muscle reflexes in motion: how, what, and why? Exerc Sport Sci Rev 34:145–153
Stelmach GE, Phillips J, DiFabio RP, Teasdale N (1989) Age, functional postural reflexes, and voluntary sway. J Gerontol 44:B100–B106
Tang PF, Woollacott MH (1998) Inefficient postural responses to unexpected slips during walking in older adults. J Gerontol A 53:M471–M480
Tang PF, Woollacott MH (1999) Phase-dependent modulation of proximal and distal postural responses to slips in young and older adults. J Gerontol A 54:M89–M102
Toft E, Sinkjaer T, Rasmussen A (1991) Stretch reflex variation in the relaxed and the pre-activated quadriceps muscle of normal humans. Acta Neurol Scand 84:311–315
Van Boxtel A (1986) Differential effects of low-frequency depression, vibration-induced inhibition, and posttetanic potentiation on H-reflexes and tendon jerks in the human soleus muscle. J Neurophysiol 55:551–568
Verschueren SMP, Brumagne S, Swinnen SP, Cordo PJ (2002) The effect of aging on dynamic position sense at the ankle. Behav Brain Res 136:593–603
Zehr EP, Stein RB (1999) What functions do reflexes serve during human locomotion? Prog Neurobiol 58:185–205
Zuur AT, Christensen MS, Sinkjaer T, Grey MJ, Nielsen JB (2009) Tibialis anterior stretch reflex in early stance is suppressed by repetitive transcranial magnetic stimulation. J Physiol 587:1669–1676
Acknowledgments
The authors are particularly grateful to Dr Mark Jesunathadas for helpful comments on a previous version of this manuscript. This study was supported by a grant of the European Commission (Framework Program V; Better-Ageing project, QLK6-CT-2001-00323) and the Fonds National de la Recherche Scientifique of Belgium.
Author information
Authors and Affiliations
Corresponding author
Additional information
Communicated by Alain Martin.
Rights and permissions
About this article
Cite this article
Klass, M., Baudry, S. & Duchateau, J. Modulation of reflex responses in activated ankle dorsiflexors differs in healthy young and elderly subjects. Eur J Appl Physiol 111, 1909–1916 (2011). https://doi.org/10.1007/s00421-010-1815-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00421-010-1815-x