
Abstract
The aim of this study was to examine and compare the effects of different resistance training protocols on bone marker concentrations in older men. Thirty-seven healthy older male subjects were assigned to one of three groups: high-intensity resistance training (HI-RT, age = 57.5 ± 0.8); low-intensity resistance training with vascular restriction (LI-VRT, age = 59.9 ± 1.0); and control (CON, age = 57.0 ± 1.1). Blood samples were collected before and after 6 weeks of resistance training to measure the changes in bone formation [bone alkaline phosphatase, (Bone ALP)] and resorption (C-terminal cross-linking telopeptide of Type-I collagen, CTX) marker concentrations. A significant main effect for time was detected in Bone ALP to CTX ratio for the exercise groups (p < 0.05). There was a significant group effect for percentage changes in serum Bone ALP (21% for LI-VRT, 23% for HI-RT, and 4.7% for CON) and post hoc analysis identified significant increases in serum Bone ALP concentrations in LI-VRT (p = 0.03) and HI-RT (p = 0.02) when compared with CON. The exercise groups had significantly (p < 0.01) greater strength increases in all upper body and leg exercises compared with CON with no significant differences between the exercise groups except for leg extension strength (HI-RT > LI-VRT, p < 0.05). Serum concentrations of Bone ALP and Bone ALP to CTX ratio improved in both resistance training protocols, suggesting increased bone turnover with a balance favoring bone formation. Therefore, despite using low mechanical load, LI-VRT is a potentially effective training alternative to traditional HI-RT for enhancing bone health in older men.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Aging is associated with several unavoidable changes such as loss of skeletal muscle mass (Bross et al. 1999) and bone mass (Martin 1993; Russo et al. 2003), which may result in functional limitation due to decreases in muscular strength (Baumgartner et al. 1998; Candow 2008; Lexell et al. 1988) and osteoporosis due to decreases in bone mineral density (BMD) (Honig 2010; Martin 1993), respectively. Bone remodeling occurs through a coupled process of removing existing bone (resorption) and the formation of new bone (Clarke 2008). An uncoupled increased concentration of formation markers such as bone alkaline phosphatase (Bone ALP) indicates an increase in bone formation rate and is associated with increased BMD (Cosman et al. 1996; Delmas et al. 2000). Bone marker responses to training are more rapid than BMD responses to training (Harris et al. 1993); therefore, they have been used to determine the bone turnover status and the effectiveness of training programs to improve bone metabolism. Lester et al. (2009) found that 8 weeks of combined resistance and aerobic training and resistance training alone have stimulated increases in bone formation markers (Bone ALP and osteocalcin). Bone resorption responses were less clear, as tartrate-resistant acid phosphatase (TRACP) decreased and deoxypyridinoline (DPD) increased in both the training and control groups. There were also significant increases in volumetric and areal BMD in the aerobic and combined groups, respectively. Fujimura et al. (1997) also reported significant increases in markers of bone formation (serum osteocalcin and serum Bone ALP), but no significant changes in a marker of bone resorption (C-terminal cross-linking telopeptide of Type-I collagen, CTX) in the training group following 4 months resistance training.
Even though aging is related to negative changes in bone structure and bone mass, bone can adapt positively to meet the demands when it is challenged and when the appropriate training techniques are followed. The impact of mechanical loading (Menkes et al. 1993; Ryan et al. 1994; Vincent and Braith 2002) and high-impact exercises (Bemben et al. 2004; Vainionpaa et al. 2005) on bone adaptation has been investigated by a number of studies and results have suggested that high-intensity loading might be better to create optimal stress for increasing bone quality (Bemben et al. 2004; Kohrt et al. 2004; Ryan et al. 1994; Vainionpaa et al. 2005; Vincent and Braith 2002). Ryan et al. (1994) reported increases in BMD and strength in older males (mean age = 61 year) following a 16-week heavy (5 repetition maximum, 5-RM) strength-training program. Menkes et al. (1993) also conducted a study to train older men (mean age = 59 year) for 16 weeks using high-intensity strength training and reported significant increases in bone formation marker concentrations, however, no significant changes were observed in BMD.
The study by Vincent et al., reported that high-intensity resistance training (HI-RT, 80% 1-RM) was more effective than low-intensity (50% 1-RM) resistance training to improve BMD (Vincent and Braith 2002). Another study suggested that a logical prediction of the effect of an exercise protocol on bone osteogenic potential can be made by using the information on intensity (the ground reaction force through the leg during running) and volume of exercises used (Turner and Robling 2003). However, new evidence has challenged the findings reported and has suggested that low-impact slow walk training combined with vascular restriction (VR) may elicit increases in bone formation marker concentrations (Beekley et al. 2005). It was reported that 3 weeks of walk training at 50 m/min with VR resulted in a significant increase in Bone ALP concentration by 10.8% for the VR-walk group, but only a 0.3% increase for the no-VR-walk group (Beekley et al. 2005). Bemben et al. (2007) also reported significant decreases in bone resorption markers (cross-linked N-telopeptide of Type-I collagen) following a single bout of low-intensity resistance training exercises with VR. It is worth mentioning that low-intensity resistance exercise (i.e., 20% 1-RM) in combination with VR was also found to be very effective to increase muscle size (Abe et al. 2006; Beekley et al. 2005; Takarada and Ishii 2002; Takarada et al. 2000a, 2002) and strength (Shinohara et al. 1998; Takarada and Ishii 2002; Takarada et al. 2002). However, no previous studies examined the effectiveness of low-intensity resistance exercise (i.e., 20% 1-RM) training combined with VR on bone markers; therefore, the aim of this study was to investigate the effects of two different resistance training protocols on bone markers in older men. Since previous studies reported that VR training protocols were successful to increase skeletal muscle strength (Abe et al. 2005, 2006; Shinohara et al. 1998; Takarada and Ishii 2002; Takarada et al. 2000b, 2002) to a similar or even greater extent than traditional resistance training protocols (Goto et al. 2004; Häkkinen et al. 2001; McCall et al. 1999) and since improvements in muscular strength can exert more force on bony attachments and muscular contractions are the primary source of bone loading (Frost 2001), it was hypothesized that low-intensity VR training protocol would improve the markers of bone turnover in older men.
Methods
Subjects
Healthy middle-aged adult males (n = 37, mean age = 56.8 ± 0.6 years) volunteered to participate in this study. Participants who had a Body Mass Index (BMI) greater than 40 kg/m2, were not capable of undergoing physical strength testing and training, or had a history of participation in a regular resistance training program within the last 4 months prior to study were excluded from the study. After obtaining medical clearance from their own physicians, each subject completed the informed consent, questionnaires, and pre-testing prior to participation in the study. The details about group assignments and the training protocols can be found in the resistance training regimen section below. The investigation was approved by the University of Oklahoma Institutional Review Board for Human Subjects.
Dual energy X-ray absorptiometry
Total and regional body composition and total body areal bone mineral density (aBMD) and bone mineral content (BMC) were measured from two total body scans (1 pre- and 1 post-training) using dual energy X-ray absorptiometry (DXA) (GE Medical Systems, Lunar Prodigy enCORE software version 10.50.086, Madison, WI) by a trained technician. Quality assurance (QA) and spine phantom calibration testing was performed daily prior to scanning to ensure no machine drift occurred during the study. For the total body scan, the participant lay in the supine position, with arms close to the sides. The participant’s legs were fastened together by Velcro straps to ensure that the legs remained still and relaxed. Subjects with an abdominal thickness at the umbilicus of ≤25 cm were scanned at the Standard speed and subjects with an abdominal thickness of >25 cm were scanned at the slower Thick speed. The in vivo precision for total body BMD in our laboratory was 0.62%.
Peripheral quantitative computed tomography
All subjects had their volumetric bone mineral density (vBMD) and bone characteristics (BMC, area, cortical thickness (CTh), strength–strain index (SSI) assessed at 4 and 66% of the limb length proximal to the bony endplate of the right tibia and at 50% of the limb length proximal to the bony endplate of the right femur using a peripheral quantitative computed tomography (pQCT) scanner XCT 3000 with software version 6.00 (Stratec Medizintechnik GmbH, Pforzheim, Germany) with a voxel size of 0.4 mm and a scan speed of 20 mm/s. To perform the scan, the participant was seated in the scanning chair with the right leg in the support straps and positioned in the center of the scanning area, and the participant was asked to remain very still. A scout view scan was run to determine the exact location of the end of the bone (tibia for lower leg scans and femur for upper thigh scans). Analysis modes and thresholds are set to separate cortical from trabecular bone to allow for total, cortical, and trabecular bone analysis. Contour mode (Contmode) 1 and Peel mode 2 are threshold driven analysis modes. Cortmode 2 is a threshold driven cortical mode with an included filter for the cortical shell. Thresholds used on the distal tibia were Contmode 1, Peelmode 2, Threshold1 169, Threshold2 650, Cortmode 2, and Threshcrt 480. Thresholds used on the tibia 66% site were Contmode 1, Peelmode 2, Threshold1 710, Threshold2 710, Cortmode 2, Threshcrt 710. The pQCT CVs range from 0.27 to 1.93% for the total bone variables; 0.45–1.12% for distal trabecular bone variables; 1.07–4.99% for diaphyseal trabecular bone variables; 1.19–3.21% for cortical bone distal variables; and 0.51–1.65% for diaphyseal cortical variables.
Bone markers
Serum concentrations of Bone ALP and CTX were assessed as markers for bone formation and resorption, respectively. Pre and post-training resting blood samples were obtained by venipuncture by a nurse following an 8-h overnight fast between 8:30 and 10 a.m. Samples collected were allowed to clot at room temperature and serum was separated by centrifugation and transferred into polystyrene tubes and stored in a −80°C freezer until assay analyses were performed in duplicate.
Serum concentration of Bone ALP was assessed to determine the process of bone formation by using the Metra Bone ALP enzyme immunoassay (EIA) (Quidel Corporation, Mountain View, CA). The minimum detection limit of assay was 0.7 U/L. The intra-assay and inter-assay coefficient of variation was less than 9 and 11%, respectively.
The concentration of serum CTX was assessed to determine the process of bone resorption by using an enzyme-linked immunosorbent assay (ELISA) (Nordic Bioscience Diagnostics, Denmark). The minimum detection limit of assay was 0.02 ng/mL. The intra-assay and inter-assay coefficient of variation was less than 7.2 and 3.7%, respectively.
One repetition maximum (1-RM) testing
Resistance training exercises and muscular strength tests were performed on CYBEX weight machines (Medway, MA). Maximum strength was measured by performing 1-RM testing at baseline, every 2 weeks to adjust the loads used during the training program, and after completion of the study. The participants were instructed with proper lifting technique and were asked to perform a warm-up set comprised of 3–5 repetitions for each exercise at 50% of their perceived maximal effort. The weight was then increased progressively until reaching the maximum weight that could be lifted for one repetition with a 1.5 min rest interval between trials and 1-RM was determined within five attempts.
Blood flow restriction
For LI-VRT group, elastic belts (50 mm in width) that were positioned around the most proximal portion of the thighs to apply pressure have pneumatic bags along the inner surface connected to an electronic air pressure control system (KAATSU-Master, Sato Sports Plaza, Tokyo, Japan). Prior to progressive increases in pressure to reach the target pressure (TRP, the highest pressure used during training), each participant was seated on a chair, and initial restrictive cuff pressure (IRP, tightness of the cuffs before inflating with air) was set around 40 mmHg. Then the cuffs were inflated to reach the approximate normal resting systolic blood pressure (120 mmHg) for a healthy adult. The pressure was held at 120 mmHg for 30 s and released for 10 s. Then the pressure was increased by 20 mmHg while holding for 30 s at each pressure and releasing for 10 s between increments until the TRP of 160 mmHg was reached. The cuff pressures were increased for the next training session when the whole sets and repetitions (reps) are completed and when the level of exertion such as rated perceived exertion (RPE) was below 16 or decreased when the whole sets and reps were not completed during the previous training session. Following successful training sessions, the cuff pressures were increased progressively to pressures between 45 and 55 mmHg for the IRP and between 160 and 180 mmHg for the TRP. The highest pressure reached for initial and target pressures were ~70 and 240 mmHg, respectively. The average initial pressure, target pressure, and RPE values were 62.3 ± 5.1 mmHg, 205.4 ± 15.6 mmHg, and 16.5 ± 1.8, respectively. The cuff pressures were maintained during 30 s rest between sets, but the cuffs were deflated for about 5 to 10 min between the leg exercises. The cuffs were inflated before the first leg exercise and deflated immediately after completion of the leg exercises. The total time that the cuffs stayed inflated was between 6 and 8 min. The rest periods between sets and exercises ranged between 30 and 90 s for the HI-RT group.
Resistance training regimen
Following baseline testing and familiarization with the training protocol, the participants were trained three times a week for 6 weeks. Training participants were divided into two groups by allowing them to choose a training session that fits in their time schedules without knowing what training protocol was assigned to each training session. After performing baseline testing, the participants in the control group were asked not to change anything in their normal daily physical activities, then returned to the laboratory 6 weeks later to complete post-testing.
Total duration to perform lower body exercises was taking less than 5 min including rest periods between sets, therefore three upper body exercises were added for the convenience of the participants. Training sessions were preceded by a 5-min standardized warm-up on cycle ergometer or treadmill. Both the HI-RT group and LI-VRT group performed the same upper body exercises (latissimus pull down, shoulder press, and biceps curl) for 3 sets of 8 repetitions at 80% 1-RM. The HI-RT group performed two lower body exercises (leg press and knee extension) for 3 sets of 8 repetitions at 80% 1-RM, but the LI-VRT group performed these lower body exercises with VR for 1 set of 30 repetitions, followed by 2 sets of 15 repetitions at 20% 1-RM. Qualified personnel were present during all training sessions to make sure proper lifting techniques were used for each exercise. Training loads for both exercise groups and for each exercise were adjusted based on 1-RM testing performed every 2 weeks.
Statistical analyses
Baseline between-group differences and percent (%) changes from pre- to post-training were determined by one-way analysis of variance (ANOVA). When there were no significant differences between groups at baseline, two-way repeated measures ANOVA [time (pre vs. post) × condition (LI-VRT vs. HI-RT vs. CON)] was utilized to determine differences between the group means. When the ANOVA indicated a significant difference, LSD comparison test was performed for a post hoc analysis. Even though there were no statistical differences between groups at baseline in most of the dependent variables, analysis of covariance (ANCOVA) was used on all outcome variables to correct for initial group differences at the conclusion of the study. When the baseline values significantly contributed to the outcome, then the values for the between-group comparison by ANCOVA were reported. All data are expressed as mean ± SE in the text, figures, and tables. Significance was assigned to p values of ≤0.05 for all comparisons. The data was analyzed using SPSS 16 for Windows (SPSS Inc., Chicago, IL).
Results
Descriptive statistics (Table 1) indicate that there were no significant differences between groups for age, height, and weight. Of the initial group of LI-VRT, one subject dropped out during the training program. The adherence rate remained high throughout the training programs (93% for the LI-VRT and 100% for HI-RT groups).
Bone measurements
DXA
No significant differences between groups were detected in aBMD and BMC at baseline. A significant main effect for time (p = 0.01) was observed for aBMD, however, post hoc analyses did not reveal any significant differences between groups. There were no group x time interaction (p = 0.42) for aBMD. There were no significant main effect for time (p = 0.42) or group x time interaction (p = 0.98) for BMC. Table 2 displays baseline and post-training values of aBMD and BMC for each group.
pQCT
There were not any significant differences between groups for total volumetric density (ToD), total area (ToA), trabecular volumetric density (TrD), trabecular area (TrA), cortical volumetric density (CoD), cortical area (CoA), CTh, strength–strain index (SSI) values at baseline. Following training, there were significant main effect for time (p = 0.01) and group × time interaction (p = 0.03) for ToD, significant main effect for time (p = 0.04), but no group × time interaction (p = 0.49) for ToA, no significant main effect for time (p = 0.16) or group × time interaction (p = 0.46) for TrD, no significant main effect for time (p = 0.82) or group × time interaction (p = 0.98) for ToA at 4% of the limb length proximal to the bony endplate of the right tibia. However, post hoc analyses did not reveal any significant group differences for ToD and ToA. No significant main effect for time (p value was ranged from 0.31 to 0.70) or group × time interaction (p value was ranged from 0.37 to 0.64) were observed for ToD, for ToA, CoD, CoA at 66% of the limb length proximal to the bony endplate of the right tibia. There were no significant main effect for time (p value was ranged from 0.35 to 0.84) or group × time interaction (p value ranged from 0.32 to 0.98) for ToD, ToA, CoD, CoA, CTh, and SSI at 50% of the limb length proximal to the bony endplate of the right femur. Table 3 displays baseline and post-training values for the aforementioned variables for each group.
Muscle strength
The exercise groups gained significant amount of strength in all upper and lower body exercises compared with CON (p < 0.01). Strength changes following training for the exercise groups were similar (p > 0.05) except for the changes in leg extension strength, where the HI-RT group experienced greater strength gains than both the LI-VRT and CON groups (p < 0.05). The percentage changes in lat pull-down strength from baseline were 15.9 and 13.2%, in shoulder press strength 9.6 and 8.6%, and in biceps curl strength 19.3 and 22.9% for the LI-VRT and HI-RT groups, respectively. Leg press strength and leg extension strength increased by 19.3 and 20.4% and by 19.1 and 31.2% for the LI-VRT and HI-RT groups, respectively [for more details refer to study by Karabulut et al. (2009)].
Bone marker responses to training
There were no significant differences between groups for Bone ALP values at baseline. In the HI-RT group, one participant had large decreases in Bone ALP and increases in CTX values from baseline. After having a detailed conversation with the participant about his medical history, it appeared that he was using some medications because of his knee problem, which was not reported at baseline. Unexpected changes in serum bone markers for that subject were thought to be due to the medications that the participant was on or unknown medical problems such as liver problems resulting in compromised liver functions. In the CON group, one participant was not able to go for post-training blood draw due to changes in his job duty. The data for serum Bone ALP and CTX were analyzed and reported without those 2 subjects. Table 4 displays baseline and post-training serum Bone ALP and CTX concentrations and the ratio of Bone ALP to CTX for each group.
There was a significant main effect for time (p < 0.01) for Bone ALP and a trend for a group × time interaction (p = 0.06) was observed indicating that there might be training-induced changes in serum BAP concentrations. The differences in the changes of percentages of serum Bone ALP concentrations were a 21.0% increase for LI-VRT, a 23% increase for HI-RT and a 4.7% increase for CON, respectively. There were significant group differences in percentage changes in serum Bone ALP concentrations from baseline (p = 0.04) and the follow-up tests detected significant increases in serum Bone ALP concentrations in LI-VRT (p = 0.03) and HI-RT (p = 0.02) compared with CON (Fig. 1).

Bone-specific alkaline phosphatase (Bone ALP) percentage change after 6 weeks of training. LI-VRT (low-intensity vascular restriction training group, n = 13); HI-RT (high-intensity traditional resistance training group, n = 12); CON (control group, n = 10). aSignificantly different (p < 0.05) from control. Values reported as mean ± SE
There were no significant main effects for time (p = 0.20) or group × time interaction (p = 0.12). No significant group differences in percentage change in serum CTX level from baseline were detected (p = 0.43). The differences in the changes of percentages of serum CTX concentrations were a 7.7% decrease for LI-VRT, a 4.1% decrease for HI-RT and a 3.3% increase for CON, respectively. The percentage of serum CTX concentration from baseline decreased for the exercise groups and increased for the CON group; however, no significant differences were observed between groups (Fig. 2).

C-telopeptide of Type-I collagen (CTX) percentage change from baseline to the end of the study. LI-VRT (low-intensity vascular restriction training group, n = 13); HI-RT (high-intensity traditional resistance training group, n = 12); CON (control group, n = 10).Values reported as mean ± SE
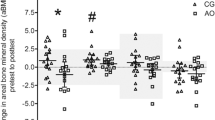
At baseline, no significant group differences were detected in serum Bone ALP to CTX ratio by one-way ANOVA (p = 0.94). There was a significant main effect for time (p < 0.01), but there was no group × time interaction (p = 0.39). The differences between baseline ratio of Bone ALP to CTX and post-training ratio of Bone ALP to CTX were 19.7 for LI-VRT, 21.4 for HI-RT, and 5 for CON. Figure 3 displays the ratio of the marker of bone formation (Bone ALP) to the marker of bone resorption (CTX) providing information about the effectiveness of the training protocols and the metabolic state of bone.

The ratio of serum bone alkaline phosphatase (Bone ALP) to C-telopeptide of Type-I collagen (CTX) at baseline and the end of the study. LI-VRT (low-intensity vascular restriction training group, n = 13); HI-RT (high-intensity traditional resistance training group, n = 12); CON (control group, n = 10). aSignificantly different (p < 0.05) from control. Values reported as mean ± SE
Discussion
To our knowledge, our study is the first to report that the low-intensity resistance training with VR may be as effective as the HI-RT protocol to improve bone health, as indicated by significant increases in Bone ALP concentrations from baseline and Bone ALP/CTX ratio following training for the training groups. Both training protocols resulted in significant amount of strength increases in all upper and lower body exercises compared with CON. As expected, the present study failed to detect significant changes in DXA assessed aBMD and BMC. Similarly, the study also failed to find significant changes in pQCT measured ToD, ToA, TrD at 4% and ToD, ToA, CoD, CoA at 66% of the limb length proximal to the bony endplate of the right tibia, and ToD, ToA, CoD, CoA, CTh, and SSI at 50% of the limb length proximal to the bony endplate of the right femur. It was not expected to observe any significant training related increases in mineral properties at these sites following the short period of resistance training (Heaney 1994).
Conflicting findings about bone marker responses to resistance training have been previously reported (Ryan et al. 1994); however, the findings of the present study were consistent with the other studies (Beekley et al. 2005; Fujimura et al. 1997; Lester et al. 2009; Menkes et al. 1993; Vincent and Braith 2002) observing significant increases in the biochemical markers of bone remodeling. Lester et al. (2009) reported that the Combined (resistance and aerobic training) and the Resistance training groups had significant increases in serum concentrations of Bone ALP (15.8 and 16.6%, respectively) and osteocalcin (8.5 and 19.8%, respectively) following 8 weeks of training. Another investigation (1997) revealed significant increases in the markers of bone formation (serum Bone ALP and osteocalcin) in the training group following 4 months resistance training. Findings of the present study about the changes in the markers of bone resorption also paralleled with the data reported by Lester et al. (2009) and Fujimura et al. (1997) that the decreases in markers of bone resorption did not reach level of statistical significance. Similarly, a study by Vincent and Braith (2002) reported increases in Bone ALP following a 6-month resistance exercise training program in middle-aged men and women (68 years old). The subjects were randomly assigned to a control group or one of two training groups performing exercises either at 80% 1-RM for 8 repetitions (the high-intensity group) or at 50% 1-RM for 13 repetitions (low-intensity group). There were 25 and 39% increases in osteocalcin concentrations for low-intensity and high-intensity exercise groups, respectively, but Bone ALP increased significantly by 7.1% in high-intensity exercise group only. The baseline and post-training ratios of Bone ALP to pyridinoline cross-link (PYD, catabolic indicator) were 16.2 and 11.8 for control, 12.8 and 13.8 for low-intensity, and 14.3 and 17.2 for high-intensity group. Even though PYD was measured to determine the level of catabolic activity, the ratio of Bone ALP to PYD was also similar to the ratio of Bone ALP to CTX observed in the current study. Menkes et al. (1993) also reported significant increases in bone turnover markers following a 16-week strength-training program. The magnitude of changes in the bone formation markers of osteocalcin (19%) and skeletal alkaline phosphatase (26%) were also somewhat similar with the amount of changes observed in the present study.
Even though the training protocol used by Ryan et al. (1994) was similar with the one used by Menkes et al. (1993), who reported significant increases in bone markers in older men, Ryan et al. (1994) reported no significant increases in osteocalcin or skeletal alkaline phosphatase following a 16-week strength-training program in postmenopausal women. The exact reasons of conflicting results remain unclear and speculative, but possible factors contributing to this inconsistent variability might be: type of assay kits used, the subjects’ different initial activity level, gender, and seasonal variation. There are not many studies investigating the effects of this new VR training method on markers of bone formation and resorption available; therefore, it is worth noting and comparing the findings from the present study with those from the only study using VR technique with walking. Nine young men (mean age: 21 years) walked on a treadmill for a total of 10 min per session (five bouts of 2 min walk, twice a day), six times per week. A significant increase (10.8%) in serum Bone ALP concentrations after 3 weeks of training indicates that even though the intensity of exercise was low, VR technique caused changes in physiological systems resulting in significant changes in markers of bone formation (Beekley et al. 2005).
In conclusion, significant changes in Bone ALP concentrations and Bone ALP to CTX ratio indicates increased osteoblastic activity (Fujimura et al. 1997) favoring bone formation following resistance training and the LI-VRT technique was almost as successful as the HI-RT technique. Both the magnitude and pattern of change of bone marker concentrations were similar for both exercise groups suggesting that increases in muscular strength could be one of the factors resulting in improvements in bone remodeling process due to the changes in the amount of force exerted on bony attachments (Frost 2001). Several other hypotheses also exist for the similar relative efficacy of LI-VRT for bone metabolism change. Capillary endothelial cells have an impact on bone remodeling by synthesizing and releasing different molecules including free radicals, local regulatory factors (e.g., interleukin-6, nitric oxide), and growth factors that may inhibit osteoclast activity and stimulate osteoblast activity (McCarthy 2006; Parfitt 2000), therefore blood flow restriction in combination with resistance exercise might be affecting the secretory function of the endothelial cells leading to improvements in bone remodeling. Furthermore, even though the magnitude of mechanical loading during LI-VRT training sessions was low, fluid shifts occurring during muscular contractions (Caulkins et al. 2009) may stimulate piezoelectric potentials on osteocytes to stimulate remodeling (Frost 2001). Finally, endocrine responses to resistance training (Kraemer and Ratamess 2005) may either directly affect bone metabolism, or may alter the mechanosensitivity of bone cells, leading to decreases in bone resorption. Therefore, while high-intensity resistance training and activities with impact loading are effective for increasing muscular strength and BMD, considerable evidence supports the hypothesis that this new training technique might be an alternative training method to improve muscular strength and bone health in older males and individuals who are unable to participate in high-intensity physical activities. It is worthwhile mentioning that the equipment used to restrict blood flow is not available in stores for the general public at the moment; however, this new training technique may be utilized by qualified personnel to train individuals at gymnasiums and rehabilitative settings in the future. The present study reveals a need for future studies to clarify the physiology of the underlying factors and to investigate the long-term effects of LI-VRT on bone density and muscular strength for older males and females.
References
Abe T, Yasuda T, Midorikawa T, Sato Y, Kearns CF, Inoue K, Koizumi K, Ishii N (2005) Skeletal muscle size and circulating IGF-1 are increased after two weeks of twice daily “KAATSU” resistance training. Int J KAATSU Train Res 1:6–12
Abe T, Kearns CF, Sato Y (2006) Muscle size and strength are increased following walk training with restricted venous blood flow from the leg muscle, Kaatsu-walk training. J Appl Physiol 100:1460–1466
Baumgartner RN, Koehler KM, Gallagher D, Romero L, Heymsfield SB, Ross RR, Garry PJ, Lindeman RD (1998) Epidemiology of sarcopenia among the elderly in New Mexico. Am J Epidemiol 147:755–763
Beekley MD, Sato Y, Abe T (2005) KAATSU-walk training increases serum bone-specific alkaline phosphatase in young men. Int J KAATSU Train Res 1:77–81
Bemben DA, Buchanan TD, Bemben MG, Knehans AW (2004) Influence of type of mechanical loading, menstrual status, and training season on bone density in young women athletes. J Strength Cond Res 18:220–226
Bemben DA, Palmer IJ, Abe T, Sato Y, Bemben MG (2007) Effects of a single bout of low intensity KAATSU resistance training on markers of bone turnover in young men. Int J Kaatsu Train Res 3:21–26
Bross R, Storer T, Bhasin S (1999) Aging and muscle loss. Trends Endocrinol Metab 10:194–198
Candow DG (2008) The impact of nutritional and exercise strategies for aging bone and muscle. Appl Physiol Nutr Metab 33:181–183
Caulkins C, Ebramzadeh E, Winet H (2009) Skeletal muscle contractions uncoupled from gravitational loading directly increase cortical bone blood flow rates in vivo. J Orthop Res 27:651–656
Clarke B (2008) Normal bone anatomy and physiology. Clin J Am Soc Nephrol 3(Suppl 3):S131–S139
Cosman F, Nieves J, Wilkinson C, Schnering D, Shen V, Lindsay R (1996) Bone density change and biochemical indices of skeletal turnover. Calcif Tissue Int 58:236–243
Delmas PD, Hardy P, Garnero P, Dain M (2000) Monitoring individual response to hormone replacement therapy with bone markers. Bone 26:553–560
Frost HM (2001) From Wolff’s law to the Utah paradigm: insights about bone physiology and its clinical applications. Anat Rec 262:398–419
Fujimura R, Ashizawa N, Watanabe M, Mukai N, Amagai H, Fukubayashi T, Hayashi K, Tokuyama K, Suzuki M (1997) Effect of resistance exercise training on bone formation and resorption in young male subjects assessed by biomarkers of bone metabolism. J Bone Miner Res 12:656–662
Goto K, Nagasawa M, Yanagisawa O, Kizuka T, Ishii N, Takamatsu K (2004) Muscular adaptations to combinations of high- and low-intensity resistance exercises. J Strength Cond Res 18:730–737
Häkkinen K, Kraemer WJ, Newton RU, Alen M (2001) Changes in electromyographic activity, muscle fibre and force production characteristics during heavy resistance/power strength training in middle-aged and older men and women. Acta Physiol Scand 171:51–62
Harris ST, Gertz BJ, Genant HK, Eyre DR, Survill TT, Ventura JN, DeBrock J, Ricerca E, Chesnut CH 3rd (1993) The effect of short term treatment with alendronate on vertebral density and biochemical markers of bone remodeling in early postmenopausal women. J Clin Endocrinol Metab 76:1399–1406
Heaney RP (1994) The bone-remodeling transient: implications for the interpretation of clinical studies of bone mass change. J Bone Miner Res 9:1515–1523
Honig S (2010) Osteoporosis—new treatments and updates. Bull NYU Hosp Jt Dis 68:166–170
Karabulut M, Abe T, Sato Y, Bemben MG (2009) The effects of low-intensity resistance training with vascular restriction on leg muscle strength in older men. Eur J Appl Physiol 108:147–155
Kohrt WM, Bloomfield SA, Little KD, Nelson ME, Yingling VR (2004) American College of Sports Medicine Position Stand: physical activity and bone health. Med Sci Sports Exerc 36:1985–1996
Kraemer WJ, Ratamess NA (2005) Hormonal responses and adaptations to resistance exercise and training. Sports Med 35:339–361
Lester ME, Urso ML, Evans RK, Pierce JR, Spiering BA, Maresh CM, Hatfield DL, Kraemer WJ, Nindl BC (2009) Influence of exercise mode and osteogenic index on bone biomarker responses during short-term physical training. Bone 45:768–776
Lexell J, Taylor CC, Sjostrom M (1988) What is the cause of the ageing atrophy? Total number, size and proportion of different fiber types studied in whole vastus lateralis muscle from 15- to 83-year-old men. J Neurol Sci 84:275–294
Martin B (1993) Aging and strength of bone as a structural material. Calcif Tissue Int 53(Suppl 1):S34–S39 discussion S39–S40
McCall GE, Byrnes WC, Fleck SJ, Dickinson A, Kraemer WJ (1999) Acute and chronic hormonal responses to resistance training designed to promote muscle hypertrophy. Can J Appl Physiol 24:96–107
McCarthy I (2006) The physiology of bone blood flow: a review. J Bone Joint Surg Am 88(3):4–9
Menkes A, Mazel S, Redmond RA, Koffler K, Libanati CR, Gundberg CM, Zizic TM, Hagberg JM, Pratley RE, Hurley BF (1993) Strength training increases regional bone mineral density and bone remodeling in middle-aged and older men. J Appl Physiol 74:2478–2484
Parfitt AM (2000) The mechanism of coupling: a role for the vasculature. Bone 26:319–323
Russo CR, Lauretani F, Bandinelli S, Bartali B, Di Iorio A, Volpato S, Guralnik JM, Harris T, Ferrucci L (2003) Aging bone in men and women: beyond changes in bone mineral density. Osteoporos Int 14:531–538
Ryan AS, Treuth MS, Rubin MA, Miller JP, Nicklas BJ, Landis DM, Pratley RE, Libanati CR, Gundberg CM, Hurley BF (1994) Effects of strength training on bone mineral density: hormonal and bone turnover relationships. J Appl Physiol 77:1678–1684
Shinohara M, Kouzaki M, Yoshihisa T, Fukunaga T (1998) Efficacy of tourniquet ischemia for strength training with low resistance. Eur J Appl Physiol Occup Physiol 77:189–191
Takarada Y, Ishii N (2002) Effects of low-intensity resistance exercise with short interset rest period on muscular function in middle-aged women. J Strength Cond Res 16:123–128
Takarada Y, Takazawa H, Ishii N (2000a) Applications of vascular occlusion diminish disuse atrophy of knee extensor muscles. Med Sci Sports Exerc 32:2035–2039
Takarada Y, Takazawa H, Sato Y, Takebayashi S, Tanaka Y, Ishii N (2000b) Effects of resistance exercise combined with moderate vascular occlusion on muscular function in humans. J Appl Physiol 88:2097–2106
Takarada Y, Sato Y, Ishii N (2002) Effects of resistance exercise combined with vascular occlusion on muscle function in athletes. Eur J Appl Physiol 86:308–314
Turner CH, Robling AG (2003) Designing exercise regimens to increase bone strength. Exerc Sport Sci Rev 31:45–50
Vainionpaa A, Korpelainen R, Leppaluoto J, Jamsa T (2005) Effects of high-impact exercise on bone mineral density: a randomized controlled trial in premenopausal women. Osteoporos Int 16:191–197
Vincent KR, Braith RW (2002) Resistance exercise and bone turnover in elderly men and women. Med Sci Sports Exerc 34:17–23
Conflict of interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Additional information
Communicated by Klaas R Westerterp.
Rights and permissions
About this article
Cite this article
Karabulut, M., Bemben, D.A., Sherk, V.D. et al. Effects of high-intensity resistance training and low-intensity resistance training with vascular restriction on bone markers in older men. Eur J Appl Physiol 111, 1659–1667 (2011). https://doi.org/10.1007/s00421-010-1796-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00421-010-1796-9