
Abstract
Optimal levels of membrane fluidity are essential for numerous cell functions including cell growth, solute transport and signal transduction. Since exercise enhances free radical production, our aim was to evaluate in healthy male subjects the effects of an acute bout of maximal and submaximal exercise on the erythrocyte membrane fluidity and its possible relation to the oxidative damage overproduction due to exercise. Subjects (n = 34) performed three cycloergometric tests: a continuous progressive exercise, a strenuous exercise until exhaustion and an acute bout of exercise at an intensity corresponding to 70% of maximal work capacity for 30 min. Venous blood samples were collected before and immediately after these exercises. Erythrocyte membrane fluidity was assessed by fluorescence spectroscopy. Plasma malondialdehyde (MDA) and 4-hydroxyalkenals (4-HDA) concentrations and carbonyl content of plasmatic proteins were used as an index of lipid and protein oxidation, respectively. Exercise produced a dramatic drop in the erythrocyte membrane fluidity as compared to resting time, but this was not accompanied by significant changes in the plasmatic MDA and 4-HDA concentrations. The highest erythrocyte membrane rigidity was detected immediately after strenuous exercise until exhaustion was performed. Protein carbonyl levels were higher after exhaustive exercises than at rest. Continuous progressive and strenuous exercises until exhaustion, but not submaximal workload, resulted in a significant enhanced accumulation of carbonylated proteins in the plasma. These findings are consistent with the idea that exercise exaggerates oxidative damage, which may contribute, at least partially, to explain the rigidity in the membrane of the erythrocytes due to acute exercise.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Numerous processes in or among cells, including signal transduction, solute transport and cell–cell interaction, are membrane mediated (Derby and Gleeson 2007; Sudhahar et al. 2008). Cell membranes are complex bilayer structures compiled of a variety of lipids and proteins. According to the fluid-mosaic model proposed by Singer and Nicolson (1972), membrane lipids form a fluid bilayer where the incorporated proteins as well as the lipids themselves are free to diffuse laterally. Today, we are aware that both membrane structural intactness and adequate dynamics of the lipid bilayer are indispensable requirements for optimal functioning of cells (Stubbs and Smith 1984). Thus, measurements of the membrane fluidity reflect the biophysical and biochemical characteristics of the biological membranes and are an indicator of membrane function (Li et al. 1999).
Over the last few decades, intensive research in the field of oxidative stress indicates that exercise exacerbates free radical and other reactive oxygen species generation (Bloomer and Fisher-Wellman 2008; Powers and Jackson 2008). A free radical is any species capable of existence containing one or more unpaired electrons (Halliwell 1991). Aerobic organisms produce free radicals as a consequence of oxygen metabolism and, obviously, exercise causes an increase in oxygen consumption in the mitochondria. During intense exercise, the whole body oxygen uptake increases 20-fold above resting levels and 100-fold in active muscles (Asmussen et al. 1939). Although the relative role of mitochondria to the pro-oxidative stress during exercise is now under discussion, several potential alternative sources of free radicals, such as oxidase systems associated with membranes, nitric oxide production and phagocytic processes, have been proposed and contribute significantly to the overproduction of free radicals (Powers and Jackson 2008).
There is a general consensus that free radical generation during exercise occurs predominantly in skeletal and heart muscles; however, the invasive nature of obtaining biopsies from exercising humans limits their access. Therefore, some reports have claimed that several oxidative damage markers increase their plasmatic concentrations immediately after acute exercise (Ashton et al. 1998; Pialoux et al. 2009). Basically, the mature erythrocytes (RBC) are considered a simple biological bag enveloping a solution of hemoglobin, the main function of which is to act as a vehicle for oxygen transport. In terms of cell membrane structure and function, erythrocyte cell membranes are comparable to those of the plasmatic membranes of most eukaryotic cells (Ponizovsky et al. 2003). Thus, cell membranes isolated from RBC may reflect, at least partially, processes ongoing at various sites in the organism such as skeletal muscles. For this reason and because of its ready availability, membranes isolated from RBC have been used to perform experimental studies on the membrane function in animals (Motta et al. 2009; Portier et al. 2006) and in humans (Brzeszczynska et al. 2008). None of these studies have compared different types of exercise and correlated the membrane function with the plasma oxidative damage.
The purpose of this study was to primarily explore the impact of three different protocols of acute exercise on the erythrocyte membrane fluidity in healthy humans, estimated by changes in the fluorescence polarization of 1-(4-trimethylammoniumphenyl)-6-phenyl-1,3,5-hexatriene-p-toluene sulfonate (TMA-DPH). Since the in vitro association between membrane rigidity and oxidative damage has been widely reported (García et al. 1997), in this study we also relate this physiological occurrence in the erythrocyte membrane to the fluctuations in the plasma of the protein carbonyls contents and the concentrations of malondialdehyde (MDA) plus 4-hydroxyalkenals (4-HDA), two frequently used measurements that reflect protein and lipid oxidation, respectively.
Materials and methods
Subjects
A total of 34 healthy untrained male subject volunteers aged 19–29 years (23.0 ± 0.41) were involved in this study. Only males were included to avoid any distortion in the hormonal response to physical exercise caused by sex differences (Bloomer and Fisher-Wellman 2008). The anthropometric characteristics of these subjects are summarized in Table 1. None of them participated regularly in any kind of sportive competition and did not engage in any form of vigorous exercise or take medications for 24 h before the study was carried out. All subjects underwent an extensive previous medical evaluation that included a history and physical examination, electrocardiogram and biochemical profile to discard possible pathologies. Subjects gave their informed written consent to participate in the study, and it was designed according to the principles of the Declaration of Helsinki. The experimental protocol was approved by Aragón Ethical Committee for Clinical Research (reference CP02/2010).
Experimental procedures
Exercise was performed on an electronically braked cycloergometer between 8:00 and 10:30 a.m. after an overnight fast. All subjects pedaled at an established cadence of 60 rounds per minute. Three ergometric tests were performed on each subject at random order at intervals of at least 1 week. Firstly, the maximal oxygen consumption (VO2max) and the maximal working capacity (MWC) were determined using a continuous progressive exercise test where the work load was increased by 10 W every minute until exhaustion (Carta et al. 1991). The oxygen uptake was determined using a “breath by breath” gas exchange analyzer, CPX Express (MedGrafics®). Secondly, all subjects performed a strenuous test until exhaustion. The initial load was 100 W less than the MWC determined according to the first test (Caputo and Denadai 2004). Finally, the subjects pedaled for 30 min at a submaximal workload chosen at about 70% of the expected maximum for each individual (Bloomer et al. 2006).
Peripheral venous blood samples obtained before exercise (A) and immediately post-exercise trials (B, C and D, respectively) were drawn by antecubital veinpuncture and collected into lithium heparin-containing tubes; 10 mL of blood was collected at each sampling time. Blood samples were immediately centrifuged at 1,000×g for 10 min in a Beckman Allegra 64R refrigerated centrifuge (Fullerton, USA). Plasma was stored in 250 μL aliquots at −80ºC until carbonyl content in the proteins and MDA + 4-HDA concentrations were measured. The RBC phase at the bottom was washed three times with 10 mL of saline solution (0.9% NaCl) and was finally dissolved in 1:6 w/v in 10 mM hypotonic TRIS–HCl buffer (pH = 7.4) and, thus, hemolyzed to isolate the membranes from the RBC.
Analytical procedures
All the chemicals and solvents, of the highest grade available, were acquired from Sigma (Madrid, Spain). TMA-DPH was obtained from Molecular Probes (Eugene, USA).
The isolation of RBC membranes was carried out according to the protocol of Hanahan and Ekholm (1974) with minor modifications. To sum up, the hemolyzed RBC was centrifuged at 30,000×g for 20 min. The pellet was resuspended 1:5 w/v in 10 mM TRIS buffer and washed twice more. The final pellet was resuspended in 1:1 w/v and kept at −80°C until membrane fluidity assay.
Fluidity was monitored from triplicate determinations using TMA-DPH as fluorescent probe. Its incorporation into the RBC membrane and the determination of membrane fluidity were carried out according to that described elsewhere (Yu et al. 1992). RBC membranes (0.5 mg protein/mL) were re-suspended in 50 mM TRIS (3 mL final volume) and mixed with TMA-DPH (66.7 nM). After stirring vigorously on a vortex for 1 min, the preparation was incubated for 30 min at 37ºC. Fluorescence measurements were performed in a Perkin-Elmer LS-55 Luminescence Spectrometer equipped with a circulatory water bath to maintain the temperature at 22 ± 0.1°C. Excitation and emission wavelengths of 360 and 430 nm were used, respectively. The emission intensity of vertically polarized light was detected by an analyzer oriented parallel (Ivv) or perpendicular (IvH) to the excitation plane. A correction factor for the optical system, G, was used. Polarization (P) was calculated by the equation:
An inverse relationship exists between membrane fluidity and polarization (Yu et al. 1992); thus, membrane fluidity is expressed as 1/P. Protein concentration was determined by the Bradford method using bovine serum albumin as standard (Bradford 1976).
The content of protein carbonyls was measured according to the method of Levine et al. (1990). To the plasma, 100 μL of 50 mM TRIS buffer and 200 μL of 10 mM 2,4-dinitrophenylhydrazine (DNPH) solution was added and the mixture was vortexed followed by incubation at 37°C for 1 h. Ice-cold trichloroacetic acid (325 μL) was added to the mixture. The pellet obtained after centrifugation at 3,000×g for 10 min was washed three times with 1 mL ethanol/ethyl acetate (1:1, v:v). The last pellet was dissolved in 6 M guanidine (700 μL) and incubated again at 37°C for 15 min. After centrifugation at 12,000×g for 10 min, the absorbance of the supernatant was measured spectrophotometrically at 375 nm, and its concentration was expressed as μM carbonyl groups. Guanidine was used as a blank.
MDA + 4-HDA concentrations (μM) were used as an index of the oxidative breakdown of lipids in the plasma (Janero 1990). In the assay, MDA + 4-HDA react with N-methyl-2-phenylindole, yielding a stable chromophore with a maximum peak absorbance at 586 nm; 1,1,3,3-tetramethoxypropane was used as a standard.
Statistical analysis
The data were expressed as arithmetic mean and standard error (SE) values. Mean differences were determined using a paired t test, with a level of significance at p ≤ 0.05.
Results
The effects of RBC membrane fluidity of a single bout of maximal and submaximal exercises, performed according to our study design, are illustrated in Fig. 1. Continuous progressive exercise was followed by a decrease of the erythrocyte membrane fluidity levels (3.52 ± 0.30) in comparison to pre-exercise values (3.59 ± 0.31). The strenuous exercise until exhaustion and the submaximal workload (70% MWC) for 30 min produced a dramatic drop in the RBC membrane fluidity as compared to the resting period (3.42 ± 0.32 and 3.43 ± 0.42, respectively). No significant changes were observed after strenuous and moderate exercise.

Membrane fluidity in erythrocytes isolated from 34 male healthy subjects during basal (A) and immediately after a continuous progressive exercise test (B), a strenuous test performed until exhaustion (C) and a submaximal exercise (70% of the expected maximum workload) for 30 min (D). Data (mean ± SE) are expressed as the inverse of polarization. *Statistical differences (p ≤ 0.05) versus pre-exercise, **p < 0.05 versus continuous progressive exercise
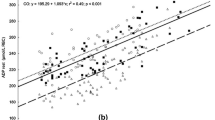
With regard to protein carbonyl concentrations in plasma (Fig. 2), immediately following the continuous progressive exercise and the strenuous exercise until exhaustion (B: 2.76 ± 0.08 μM, and C: 2.99 ± 0.09 μM, respectively), protein carbonylation increased significantly as compared to carbonyl concentrations during resting time (A: 2.76 ± 0.08 μM), However, there were no significant changes just after the submaximal one (2.86 ± 0.09 vs. 2.76 ± 0.08 μM).

Effect of acute exercise on plasmatic protein carbonylation (μM) in 34 male healthy subjects at resting time (A) and immediately post-exercise (B, C and D). Data is expressed as mean ± SE. *Statistical differences (p < 0.05) versus pre-exercise
Combined MDA + 4-HDA concentrations have been used as an index of lipid peroxidation in biological samples. Statistical analysis of plasmatic MDA + 4-HDA levels for oxidative damage to lipids did not reveal significant effects for either maximal or submaximal exercise protocols (A = 3.09 ± 0.26 μM, B = 2.97 ± 0.29 μM, C = 3.19 ± 0.32 μM, D = 3.23 ± 0.33 μM) (Fig. 3). The apparent rise in plasma MDA + 4-HDA levels at the end of the strenuous exercise performed until exhaustion and the submaximal cycloergometric tests compared to the basal were not significant (p = 0.646 and 0.621, respectively).

Plasmatic concentrations (μM) of malondialdehyde (MDA) and 4-hydroxyalkenals (4-HDA) in 34 male healthy subjects during rest (A) and immediately post-exercise (B, C and D). Data is expressed as mean ± SE
Discussion
Our study demonstrates that an acute period of exhausting or submaximal controlled exercise results in a decrease in the RBC membrane fluidity. To the best of our knowledge, this is the first report showing that acute physical exercise affects the membrane fluidity of erythrocytes in healthy human males using measurements of the membrane fluidity assessed by fluorescence spectroscopy. The principle of the fluorescence spectroscopy studies is based on the intercalation into the membrane of a fluorescent molecule, in this case TMA-DPH, which, when illuminated by polarized light, emits a fluorescence signal. The degree of polarization depends on the state of mobility of the TMA-DPH, which reflects motion in the membrane lipid environment (Yu et al. 1992). Our results are in agreement with the rigidity detected in mitochondrial membranes isolated from skeletal muscle immediately after exhausting exercise in Sprague–Dawley rats (Li et al. 1999). These authors labeled the membranes with DPH. TMA-DPH is a DPH derivative, which incorporates a trimethylammonium substituent to improve its localization in the membrane. Therefore, TMA-DPH is intercalated parallel to the long molecular axis of the phospholipids with the cationic residue oriented at the surface (Prendergast et al. 1981).
Previous observations have been reported using another technical procedure to measure membrane fluidity, electron paramagnetic resonance spectroscopy. Membrane fluidity of RBC obtained from competition horses decreased immediately after a standardized exercise, which included a final step at maximal velocity performed on a race track (De Moffarts et al. 2007). Similar observations, rigidity in erythrocyte membranes, were found in four sedentary dogs after submaximal exercise in a study attempting to elucidate the role of vitamin E supplementation in preventing the effects of submaximal exercise-induced oxidative damage over a long period of time (Motta et al. 2009). Finally, Brzeszczynska et al. (2008) detected erythrocyte rigidity 1 h after an exhaustive incremental cycling test performed in 11 healthy untrained males. These authors employed three spin labels, 5-, 12- or 16-doxylstearic acids to provide information of changes in the microenvironment in the nearest region of different depths of membrane bilayers. Since an increase in the order was detected only for the 5-doxylstearic acid spin label, they concluded that exercise-induced decreases in erythrocyte membrane fluidity were located in the polar region of the membranes (Brzeszczynska et al. 2008). To measure fluidity changes in this specific region of the membrane, we chose TMA-DPH because the polar region of this probe is anchored at the lipid–water interface, while the hydrocarbon moiety enters the lipid part of the membrane. The length of the hydrophobic part of the TMA-DPH molecule is approximately equivalent to that of a 10-carbon aliphatic chain (Kuhry et al. 1983) and will thus provide information on this more superficial region including the surface and glycerol side chain region of the plasma membrane (Prendergast et al. 1981).
On the other hand, several studies suggested that regular exercise increased fluidity and improved the membrane viscosity of human RBC (Cazzola et al. 2003; Kamada et al. 1993; Tsuda et al. 2003). Since erythrocytes are essential for rapid and homogeneous perfusion of oxygen in the microcirculation (Dutta-Roy et al. 1985), increasing membrane fluidity and lowering the microviscosity, both provoked by aerobic training, may play an important role in erythrocyte diffusion in the microcirculation (Tsuda et al. 2003).
Several structural reasons have been proposed as the cause of the RBC membrane rigidity. Firstly, these may be disturbances in the lipid membrane composition, e.g., a drop in the polyunsaturated/saturated fatty acid ratio in the membrane (Curtis et al. 1984; Shinitzky 1984). It is well documented that exercise results in free radical and other reactive oxygen species overproduction (Bloomer and Fisher-Wellman 2008; Powers and Jackson 2008). Since the polyunsaturated fatty acids are particularly sensitive to the aggressive behavior of free radicals (Gutteridge 1995), it seems reasonable that oxidative damage to the erythrocyte lipid bilayer may be involved in the RBC rigidity due to acute exercise. Secondly, oxidative stress in a biological membrane induces the formation of cross-linking of lipid–lipid and lipid–protein moieties (Chen and Yu 1994). Thirdly, membrane proteins may be modulators of membrane fluidity (Shinitzky 1984). The thiol groups of these proteins are easily oxidized by free radicals (Nakazawa et al. 1996), and it has even been suggested that acute physical exercise may result in aggregation of the spectrin–actin cytoskeletal protein complex, which leads to a decrease in the membrane dynamics (Brzeszczynska et al. 2008).
Membrane fluidity is a physicochemical feature of cell membranes that plays an important role in modulating RBC functions such as permeability, transport of ions or oxygen, membrane-associated enzyme activities and osmotic fragility (Derby and Gleeson 2007; Shinitzky 1984; Sudhahar et al. 2008). Thus, maintaining adequate erythrocyte membrane fluidity levels is essential for optimal cell physiology. During exercise, RBC are highly exposed to mechanical and oxidative stress, even more than other cells, especially considering that RBC continuously produce free radicals and also because of their limited repair mechanisms (Cimen 2008; Petibois and Deleris 2005). Several studies have claimed that vigorous exercise acutely impairs RBC deformability (Eichner 1985; Szygula 1990), and oxidative stress results in lipid and protein oxidation in the membrane, which may destabilize the lipid bilayer and the cytoskeleton, thereby compromising cell survival (Dumaswala et al. 1999). The RBC membrane rigidity due to acute exercise detected during our study is consistent with these findings.
In addition to RBC membrane rigidity, we detected increased oxidative damage in the plasma due to acute exercise, although these effects were detected in a biomolecule-specific manner; that is, plasmatic protein oxidation increased following exercise, whereas plasmatic lipid oxidation was minimally affected.
Protein oxidation due to oxidative stress results in a loss of its biological function and structural modifications, e.g., the addition of carbonyl groups to its amino acid residues (Davies and Goldberg 1987; Levine and Stadtman 2001). In this way, plasmatic protein carbonylation increased acutely in resistance trained men following a single set of anaerobic exercise (Bloomer et al. 2007; Bloomer and Fisher-Wellman 2008). However, the magnitude of protein damage resulting from aerobic exercise depends on its intensity. It has recently been proposed that a single bout of exercise for 40 min elevated protein carbonyl groups in plasma of trained men in a workload-dependent manner (Lamprecht et al. 2008). Thereby, these authors observed that oxidative damage to the plasmatic proteins occurs after exercises performed at 75 and 80% of VO2max; however, these alterations were only statistically significant when reading 80% of VO2max. In agreement with these previous studies, we found significant rises in protein carbonylation when the untrained volunteers performed maximal exercises (B and C); however, we were unable to notice a significant change in the oxidation of plasmatic protein at submaximal workloads of 70% of the expected maximum VO2 for 30 min.
Finally, acute exercise has been proved to elevate MDA concentrations or several reactive products of lipid peroxidation in the active muscle (Alessio et al. 2000; Davies et al. 1982; Ji and Fu 1992; Li et al. 1999) as well as other tissues and plasma (Brzeszczynska et al. 2008; Motta et al. 2009). In contrast to these observations, but in accordance with our results, other researchers have found that exercise minimally modifies or even reduces the degree of lipid peroxidation, presumably by increasing the capacity of the antioxidant system (Bloomer et al. 2007; Groussard et al. 2003; Kim et al. 1996) or due to increased clearance or distribution throughout the body (Leaf et al. 1997).
In conclusion, our study shows that erythrocyte membranes in untrained healthy males were less fluid after an acute period of maximal or submaximal exercise. Based on the elevation of protein carbonylation in the plasma, a marker of systemic oxidative damage, as well as the previously reported pro-oxidative effects of physical exercise, it seems reasonable that the disturbances in the dynamics of the RBC lipid bilayers may be attributed, to some extent, to the overproduction of free radicals.
References
Alessio HM, Hagerman AE, Fulkerson BK, Ambrose J, Rice RE, Wiley RL (2000) Generation of reactive oxygen species after exhaustive aerobic and isometric exercise. Med Sci Sports Exerc 32:1576–1581
Ashton T, Rowlands CC, Jones E, Young IS, Jackson SK, Davies B, Peters JR (1998) Electron spin resonance spectroscopic detection of oxygen-centred radicals in human serum following exhaustive exercise. Eur J Appl Physiol Occup Physiol 77:498–502
Asmussen E, Christensen EH, Nielsen M (1939) Die O2-Aufnahme der Ruhenden und der Arbeitenden Skelettmuskein. Skan Arch Physiol 82:212
Bloomer RJ, Fisher-Wellman KH (2008) Blood oxidative stress biomarkers: influence of sex, exercise training status, and dietary intake. Gend Med 5:218–228
Bloomer RJ, Falvo MJ, Fry AC, Schilling BK, Smith WA, Moore CA (2006) Oxidative stress response in trained men following repeated squats or sprints. Med Sci Sports Exerc 38:1436–1442
Bloomer RJ, Davis PG, Consitt LA, Wideman L (2007) Plasma protein carbonyl response to increasing exercise duration in aerobically trained men and women. Int J Sports Med 28:21–25
Bradford MM (1976) A rapid and sensitive method for the quantitation of microgram quantities of protein utilizing the principle of protein–dye binding. Anal Biochem 72:248–254
Brzeszczynska J, Pieniazek A, Gwozdzinski L, Gwozdzinski K, Jegier A (2008) Structural alterations of erythrocyte membrane components induced by exhaustive exercise. Appl Physiol Nutr Metab 33:1223–1231
Caputo F, Denadai BS (2004) Effects of aerobic endurance training status and specificity on oxygen uptake kinetics during maximal exercise. Eur J Appl Physiol 93:87–95
Carta P, Aru G, Barbieri MT, Mele M (1991) Bicycle ergometry exercise tests: a comparison between 3 protocols with an increasing load. Med Lav 82:56–64
Cazzola R, Russo-Volpe S, Cervato G, Cestaro B (2003) Biochemical assessments of oxidative stress, erythrocyte membrane fluidity and antioxidant status in professional soccer players and sedentary controls. Eur J Clin Invest 33:924–930
Chen JJ, Yu BP (1994) Alterations in mitochondrial membrane fluidity by lipid peroxidation products. Free Radic Biol Med 17:411–418
Cimen MY (2008) Free radical metabolism in human erythrocytes. Clin Chim Acta 390:1–11
Curtis MT, Gilfor D, Farber JL (1984) Lipid peroxidation increases the molecular order of microsomal membranes. Arch Biochem Biophys 235:644–649
Davies KJ, Goldberg AL (1987) Oxygen radicals stimulate intracellular proteolysis and lipid peroxidation by independent mechanisms in erythrocytes. J Biol Chem 262:8220–8226
Davies KJ, Quintanilha AT, Brooks GA, Packer L (1982) Free radicals and tissue damage produced by exercise. Biochem Biophys Res Commun 107:1198–1205
De Moffarts B, Portier K, Kirschvink N, Coudert J, Fellmann N, van Erck E, Letellier C, Motta C, Pincemail J, Art T, Lekeux P (2007) Effects of exercise and oral antioxidant supplementation enriched in (n-3) fatty acids on blood oxidant markers and erythrocyte membrane fluidity in horses. Vet J 174:113–121
Derby MC, Gleeson PA (2007) New insights into membrane trafficking and protein sorting. Int Rev Cytol 261:47–116
Dumaswala UJ, Zhuo L, Jacobsen DW, Jain SK, Sukalski KA (1999) Protein and lipid oxidation of banked human erythrocytes: role of glutathione. Free Radic Biol Med 27:1041–1049
Dutta-Roy AK, Ray TK, Sinha AK (1985) Control of erythrocyte membrane microviscosity by insulin. Biochim Biophys Acta 816:187–190
Eichner ER (1985) Runner’s macrocytosis: a clue to footstrike hemolysis. Runner’s anemia as a benefit versus runner’s hemolysis as a detriment. Am J Med 78:321–325
García JJ, Reiter RJ, Guerrero JM, Escames G, Yu BP, Oh CS, Muñoz-Hoyos A (1997) Melatonin prevents changes in microsomal membrane fluidity during induced lipid peroxidation. FEBS Lett 408:297–300
Groussard C, Rannou-Bekono F, Machefer G, Chevanne M, Vincent S, Sergent O, Cillard J, Gratas-Delamarche A (2003) Changes in blood lipid peroxidation markers and antioxidants after a single sprint anaerobic exercise. Eur J Appl Physiol 89:14–20
Gutteridge JM (1995) Lipid peroxidation and antioxidants as biomarkers of tissue damage. Clin Chem 41:1819–1828
Halliwell B (1991) Reactive oxygen species in living systems: source, biochemistry, and role in human disease. Am J Med 91:14S–22S
Hanahan DJ, Ekholm JE (1974) The preparation of red cell ghosts (membranes). Methods Enzymol 31:168–172
Janero DR (1990) Malondialdehyde and thiobarbituric acid-reactivity as diagnostic indices of lipid peroxidation and peroxidative tissue injury. Free Radic Biol Med 9:515–540
Ji LL, Fu R (1992) Responses of glutathione system and antioxidant enzymes to exhaustive exercise and hydroperoxide. J Appl Physiol 72:549–554
Kamada T, Tokuda S, Aozaki S, Otsuji S (1993) Higher levels of erythrocyte membrane fluidity in sprinters and long-distance runners. J Appl Physiol 74:354–358
Kim JD, Yu BP, McCarter RJ, Lee SY, Herlihy JT (1996) Exercise and diet modulate cardiac lipid peroxidation and antioxidant defenses. Free Radic Biol Med 20:83–88
Kuhry JG, Fonteneau P, Duportail G, Maechling C, Laustriat G (1983) TMA-DPH: a suitable fluorescence polarization probe for specific plasma membrane fluidity studies in intact living cells. Cell Biophys 5:129–140
Lamprecht M, Greilberger JF, Schwaberger G, Hofmann P, Oettl K (2008) Single bouts of exercise affect albumin redox state and carbonyl groups on plasma protein of trained men in a workload-dependent manner. J Appl Physiol 104:1611–1617
Leaf DA, Kleinman MT, Hamilton M, Barstow TJ (1997) The effect of exercise intensity on lipid peroxidation. Med Sci Sports Exerc 29:1036–1039
Levine RL, Stadtman ER (2001) Oxidative modification of proteins during aging. Exp Gerontol 36:1495–1502
Levine RL, Garland D, Oliver CN, Amici A, Climent I, Lenz AG, Ahn BW, Shaltiel S, Stadtman ER (1990) Determination of carbonyl content in oxidatively modified proteins. Methods Enzymol 186:464–478
Li JX, Tong CW, Xu DQ, Chan KM (1999) Changes in membrane fluidity and lipid peroxidation of skeletal muscle mitochondria after exhausting exercise in rats. Eur J Appl Physiol Occup Physiol 80:113–117
Motta S, Letellier C, Ropert M, Motta C, Thiebault JJ (2009) Protecting effect of vitamin E supplementation on submaximal exercise-induced oxidative stress in sedentary dogs as assessed by erythrocyte membrane fluidity and paraoxonase-1 activity. Vet J 181:288–295
Nakazawa H, Genka C, Fujishima M (1996) Pathological aspects of active oxygens/free radicals. Jpn J Physiol 46:15–32
Petibois C, Deleris G (2005) Evidence that erythrocytes are highly susceptible to exercise oxidative stress: FT-IR spectrometric studies at the molecular level. Cell Biol Int 29:709–716
Pialoux V, Mounier R, Rock E, Mazur A, Schmitt L, Richalet JP, Robach P, Coudert J, Fellmann N (2009) Effects of acute hypoxic exposure on prooxidant/antioxidant balance in elite endurance athletes. Int J Sports Med 30:87–93
Ponizovsky AM, Barshtein G, Bergelson LD (2003) Biochemical alterations of erythrocytes as an indicator of mental disorders: an overview. Harv Rev Psychiatry 11:317–332
Portier K, de Moffarts B, Fellman N, Kirschvink N, Motta C, Letellierw C, Ruelland A, van Erck E, Lekeux P, Couder J (2006) The effects of dietary N-3 and antioxidant supplementation on erythrocyte membrane fatty acid composition and fluidity in exercising horses. Equine Vet J Suppl: 279–284
Powers SK, Jackson MJ (2008) Exercise-induced oxidative stress: cellular mechanisms and impact on muscle force production. Physiol Rev 88:1243–1276
Prendergast FG, Haugland RP, Callahan PJ (1981) 1-[4-(Trimethylamino)phenyl]-6-phenylhexa-1, 3, 5-triene: synthesis, fluorescence properties, and use as a fluorescence probe of lipid bilayers. Biochemistry 20:7333–7338
Shinitzky M (1984) Membrane fluidity in malignancy. Adversative and recuperative. Biochim Biophys Acta 738:251–261
Singer SJ, Nicolson GL (1972) The fluid mosaic model of the structure of cell membranes. Science 175:720–731
Stubbs CD, Smith AD (1984) The modification of mammalian membrane polyunsaturated fatty acid composition in relation to membrane fluidity and function. Biochim Biophys Acta 779:89–137
Sudhahar CG, Haney RM, Xue Y, Stahelin RV (2008) Cellular membranes and lipid-binding domains as attractive targets for drug development. Curr Drug Targets 9:603–613
Szygula Z (1990) Erythrocytic system under the influence of physical exercise and training. Sports Med 10:181–197
Tsuda K, Yoshikawa A, Kimura K, Nishio I (2003) Effects of mild aerobic physical exercise on membrane fluidity of erythrocytes in essential hypertension. Clin Exp Pharmacol Physiol 30:382–386
Yu BP, Suescun EA, Yang SY (1992) Effect of age-related lipid peroxidation on membrane fluidity and phospholipase A2: modulation by dietary restriction. Mech Ageing Dev 65:17–33
Acknowledgments
This work was supported by the Gobierno de Aragón (Aging and Oxidative Stress Physiology, Grant No. B40) and by F.I.S. from Instituto de Salud Carlos III (Grant No. RD06/0013/1017).
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Additional information
Communicated by Susan Ward.
Rights and permissions
About this article
Cite this article
Berzosa, C., Gómez–Trullén, E.M., Piedrafita, E. et al. Erythrocyte membrane fluidity and indices of plasmatic oxidative damage after acute physical exercise in humans. Eur J Appl Physiol 111, 1127–1133 (2011). https://doi.org/10.1007/s00421-010-1738-6
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00421-010-1738-6