
Abstract
Quantitative data on muscle volume (MV) are important for estimating maximal muscle power. The objective of this study was to determine the correlation between anatomical cross-sectional areas (ACSAs) and the MV in thigh muscles (extensors, flexors, adductors, and sartorius) in perimenopausal women, and to identify at which proximal-to-distal level a single-slice ACSA measurement with magnetic resonance imaging (MRI) displays the highest correlation in each of these. Axial MRIs of the thigh were acquired in 41 perimenopausal women aged 50.8 ± 3.2 years. Segmentation of the extensors, flexors, adductors, and the sartorius was performed between the femoral neck (0%) and the distal end of the intermediate vastus (100%). MVs were determined by numerical integration, and the ACSA was calculated from three-dimensional reconstructions at 10% intervals from proximal to distal. The extensors contributed 50%, the flexors 19%, the adductors 28%, and the sartorius 3% of the total thigh MV. Maximal correlations between ACSA and MV were observed at the 20–40% proximal-to-distal level in the extensors (R 2 = 0.73), at 30% in the adductors (R 2 = 0.82), and at 70% in the flexors (R 2 = 0.72) and sartorius (R 2 = 0.85), respectively. ACSA at 50% displayed the highest overall correlations (R 2 ≥ 0.69) with MV for all muscle groups. Single-slice ACSAs from MRI displayed high correlations with MVs. Although the (proximal to distal) measurement locations with the highest correlation varied between the muscle groups, a single slice at the 50% location achieved the best compromise in terms of correlation between ACSA and MV across extensors, flexors, adductors and the sartorius.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Dynamic load transmission in synovial joints, limb movement, and locomotion are made possible by moments exerted by the relevant muscle groups, and the total muscle power generated by them. The maximal power exerted by a muscle is reflected best by the muscles’ volume (MV) that can be understood as the sum of sarcomeres arranged both in parallel and in series in the muscles’ architecture (Maganaris et al. 2006). Fukunaga et al. (2001) and Akagi et al. (2009) reported that measurement of MVs is associated with joint moments generated by the upper arm extensors and flexors. They also reported that these relationships were stronger than those achieved by measurement of the ACSA. Blazevich et al. (2009) showed that MV was best for estimating the in vivo knee joint extension moments under slow-speed concentric muscle contraction, whereas the combination of the physiological cross-sectional area and muscle fiber length provided the best result for high-speed contraction.
Since MV varies largely between individuals, depending on factors such as age, sex, body height, physical training and disease status (Abe et al. 1998, 2000; Kubo et al. 2003; Kanehisa et al. 1994; De Ste et al. 2003), however, there is need for measuring MV quantitatively or for estimating MV across subjects from alternative (simpler) measures. The gold standard for measuring MV is the segmentation of muscles from a series of contiguous magnetic resonance images (MRI), acquired perpendicular to a muscular region of interest (ROI). This method has been validated by comparison with cadaver muscle (Narici et al. 1992), but it is time-consuming because many slices (of different muscle groups) need to be segmented to cover the entire dimension of an anatomical ROI.
Morse et al. (2007) reported that, in young male adults, ACSA measurements from single MR images acquired at 60% of the femoral length (distal to proximal) had an error of less than 10% in estimating quadriceps MV. This study was confined to the quadriceps and did not encompass other thigh muscle groups such as the flexors, adductors, and the sartorius that are equally important for lower limb load transmission. Moreover, the authors did not determine the MV from contiguous MR images of the thigh muscles, but from 11 (equidistant) 5 mm slices along the femoral length.
In the current study, we examined the MV and ACSAs of all thigh muscle groups from contiguous MR images of the thigh in perimenopausal women. A reason for choosing perimenopausal women was that they have been understudied in the past, and that they represent an interesting group for investigating muscle exercise programs in longitudinal studies, because women at this age may profit from such exercise intervention to prevent sarcopenia.
The objective of the current analysis in perimenopausal women was:
-
1.
to determine the proportions of the total thigh MV taken up by the extensor, flexor, adductor, and the sartorius thigh MV, respectively;
-
2.
to elucidate the size of the ACSA in each muscle group from proximal to distal;
-
3.
to explore the correlations between single-slice ACSAs and MVs of the quadriceps, flexors, adductors and the sartorius, and to determine at which proximal-to-distal level the ACSAs provide the highest correlation with the total MV in each of these muscle groups;
-
4.
to determine the one single location (proximal to distal) in the thigh with the highest overall correlation across all thigh muscle groups from a single-slice MRI measurement.
Materials and methods
Forty-one female participants from the region of Salzburg, Austria, were recruited as described previously (Ring-Dimitriou et al. 2009). The inclusion criteria were 45–55 years of age, a self-reported regular physical activity level of less than 1 h/week, low cardiorespiratory fitness (measured by VO2-peak values measured by gas-exchange method completing an incremental cycle-ergometer test), no chronic illness and no surgery within the last 6 months (assessed by questionnaire). Exclusion criteria were general contraindications to MRI, claustrophobia, or unwillingness to participate in the thigh MRI component of the study. Written information was given to the participants, explaining the nature of the examination and written consent was obtained from all subjects. The study was approved by the Ethics Committee of the University of Salzburg, Austria (2 October 2006). Demographics (age, body height and body mass index) of the study participants are given in Table 1.
Magnetic resonance imaging of the dominant leg (being defined as the stronger leg when both legs were tested by maximal voluntary isometric contraction) was performed with a 1.5 T scanner and a circularly polarized transmit-receive knee-coil (NT Interna, Phillips Medical Systems, Best, Netherlands). A T1-weighted turbo-spin-echo sequence (repetition time = 1,541 ms, echo time = 15 ms, flip angle = 90°, section thickness = 10 mm, no inter-slice gap, in-plane resolution = 0.78 mm2, acquisition time = 1.57 min) was used to acquire contiguous axial sections of the entire thigh. Participants were in supine position for at least 15 min before the scan was started, in order to allow completion of fluid shifts during changing position from upright to supine (Berg et al. 1993).
Because identification of the muscles becomes more difficult at the proximal and distal ends, we used a proximal and distal landmark in order to analyze a consistent ROI in each participant. Proximally, the analysis was started at the distal end of the femoral neck. Distally, the analysis was completed with the last slice showing the muscular portion of the intermediate vastus (transition to the patellar tendon). In dependence of the participant’s body height and femoral ROI, 22 ± 1.3 slices were analyzed in each participant.
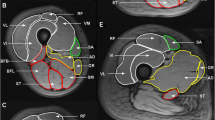
In each of the transverse slices within the above ROI, the outline of the extensor, flexor, adductor and the sartorius muscle(s) were delineated manually in order to obtain the ACSA (Fig. 1). The MV of each of the four above muscle groups and of the total thigh was determined by numerical integration of the segmented voxels. In a next step, the segmented muscles were three-dimensionally reconstructed and the ACSA was analyzed at 10% intervals of the total length of the ROI, obtaining 11 equidistant measuring points from proximal (0%) to distal (100%) independent of the original MRI slices. Three-dimensional reconstruction of each of the four muscle groups (pink color, extensors; red color, adductors; green color, flexors; blue color, sartorius muscle) and the 10% intervals from proximal to distal are shown in Fig. 2.

Segmented (R) and unsegmented (L) single MR slice of the thigh showing the anatomical cross-sectional area (ACSA) at level of 50% of the femoral region of interest (ROI). 1 extensors, 2 flexors, 3 adductors, 4 sartorius muscle

Three-dimensional reconstruction of the femoral region of interest (ROI) with the 10% intervals ranging from 0% (proximal) to distal (100%) for the different muscle groups: 1 extensors, 2 flexors, 3 adductors, 4 sartorius muscle (view from medial–distal)
Statistical analyses were performed using SPSS (version 17.0). Descriptive statistics were performed after ensuring that all variables were normally distributed. Means, standard deviations (SD), coefficients of variation (CV %), and minimal and maximal values were presented for all variables. Correlations were computed using Pearson’s rho and the coefficient of determination (coefficient of correlation squared, R 2) will be reported.
Results
The total thigh MV varied from 1,566 to 2,476 cm3 (mean 2,087 cm3) amongst the 41 perimenopausal participants. The extensors occupied 50%, the flexors 19%, and adductors 28% and the sartorius 3% of the total thigh MV within the ROI (Table 1). The extensors also displayed the largest (mean) ACSA followed by the adductors, flexors and the sartorius (Table 1).
The maximal ACSA for all thigh muscles taken together was observed at the 40% (proximal to distal) level of the ROI (Table 2). The maximum for the extensors was found at 50%, for the flexors at 70%, for the adductors at 30%, and for the sartorius at 60% (Table 2; Fig. 3a–d).

a Extensors: mean anatomical cross-sectional area (mean ACSA) at levels of percentage of the femoral region of interest (ROI). Error bar displays ±1 standard deviation. Correlations between mean ACSA and muscle volume (MV) were calculated as R2 at each level of the 10% intervals. b Flexors: mean anatomical cross-sectional area (mean ACSA) at levels of percentage of the femoral region of interest (ROI) for the flexors. Error bar displays ±1 standard deviation. Correlations between mean ACSA and muscle volume (MV) were calculated as R2 at each level of the 10% intervals. c Adductors: mean anatomical cross-sectional area (mean ACSA) at levels of percentage of the femoral region of interest (ROI) for the adductors. Error bar displays ±1 standard deviation. Correlations between mean ACSA and muscle volume (MV) were calculated as R2 at each level of the 10% intervals. d Sartorius: mean anatomical cross-sectional area (mean ACSA) at levels of percentage of the femoral region of interest (ROI) for the sartorius. Error bar displays ±1 standard deviation. Correlations between mean ACSA and muscle volume (MV) were calculated as R2 at each level of the 10% intervals
The correlation (R 2 values) between the ACSA and MV ranged from 0.39 to 0.73 for the extensors, from 0.07 to 0.72 for the flexors, from 0.20 to 0.82 for the adductors and from 0.71 to 0.85 for the sartorius (Fig. 3a–d), depending on the proximal-to-distal level investigated. The highest coefficients were found at 20–40% (proximal-to-distal level) for the extensors, at 70% for the flexors, at 30% for the adductors, and at 70% for the sartorius (Fig. 4).

Relationship between thigh muscle volume (MV) and anatomical cross-sectional area (ACSA) at the proximal-to-distal level of 40% for the extensors, at the 70% level for the flexors, at the 30% level for the adductors and at the 70% level for the sartorius muscle. Correlation of determination (R 2) is given for each model
For correlating the MVs of all four muscle groups to a single MRI slice, the 50% level of the ROI was identified as the location from which the highest correlation (R 2 ≥ 0.69) across all muscle groups was available (R 2 = 0.70 for extensors, 0.69 for flexors, 0.71 for adductors, and 0.83 for the sartorius).
Discussion
The objective of this MRI-based analysis was to provide data on the relative size of thigh muscle volumes (MVs) and ACSAs in perimenopausal women, and to explore the correlations between single-slice ACSAs at various proximal-to-distal levels with the MV in the extensors, flexors, adductors, and sartorius. The maximal coefficients of determination between ACSA and MV were 73% for the quadriceps, 72% for the flexors, 82% for the adductors, and 85% for the sartorius. The proximal-to-distal level of the ACSA with the highest correlation varied from 30 to 70% for the various muscle groups. The highest “average” correlation (between ACSA and MV) for all four thigh muscle groups (≥69%) was available from the 50% slice.
We have studied perimenopausal women because these have been understudied in the past, and because they represent an interesting group for investigating muscle exercise programs in longitudinal studies, as women at this age may particularly profit from such exercise intervention to prevent sarcopenia. It is known that MV varies between individuals differing in age, sex, body height, physical training and disease status (Abe et al. 1998, 2000; Kubo et al. 2003; Kanehisa et al. 1994; De Ste et al. 2003). Therefore, the results presented here are complementary to previous studies in young males (e.g. Maganaris et al. 2006; Fukunaga et al. 2001; Morse et al. 2007; Narici et al. 1989).
In perimenopausal populations it has been reported that factors like sarcopenia, motor neuron death, decreased physical activity, altered hormonal status, decreased caloric and protein intake, inflammatory mediators, and altered protein synthesis are related to reduction in maximal muscle power and affecting locomotion in daily life (Doherty 2003; Narici et al. 2008; Macaluso et al. 2004; Raj et al. 2010). The results reported here may therefore be specific to the relatively homogeneous group of perimenopausal women studied and cannot be readily extrapolated to other cohorts. However, it has not been documented that age-related changes affect the correlations between single-slice ACSA and MV. For the quadriceps, there are similar correlations between ACSA and MV as found in earlier studies of young men, but these relationships may not be dependent on the age and sex of the selected sample.
A limitation of the method applied is that the most proximal and distal ends of the muscles were not included in the volumetric measurement. However, the accurate differentiation between various muscular components and connective or adipose tissue was difficult in these regions; therefore this was concluded that elimination of these (relatively small) regions is a better choice than introducing potential error.
Narici et al. (1989) reported that the maximal ACSA of the thigh muscles was not necessarily located at the mid-length of each muscle. Our data confirm these findings as the extensors have their maximum ACSA roughly in the middle, whereas the adductors have a more proximal and the flexors a more distal maximum. We found that the highest correlation of the ACSAs with the MVs was observed at or near the location of the maximum ACSA in each thigh muscle group. These findings are in principle accordance with those of Morse et al. (2007) in the quadriceps, although they found somewhat higher coefficients of determination (R 2 = 0.84–0.93). Morse et al. (2007), however, studied young male students, which likely had more variable ACSAs than the physically inactive and rather homogeneous perimenopausal women studied here. The remaining variability of MV (not explained by variability in ACSA measured at a single slice) may be due to variability in the muscle length and specific muscle form between individuals.
The results of this study show that if information on the MV of the thigh musculature is required, a single MRI slice is able to provide a relatively high correlation. Depending on whether all or just one muscle group in the thigh is of interest, the “optimal” slice can be varied with regard to its proximal-to-distal location. Based on the correlation coefficients found in this study, single-slice ACSAs potentially allow one to estimate the maximal power of muscles (Maganaris et al. 2006) in context of biomechanical modeling of the load transmission in joints, or when assessing form-function relationships. These measurements can be combined with ultrasonic measurements of the pennation angle of different thigh muscles, in order to provide information of physiological cross-sectional areas and as suggested previously on high-speed muscular contraction (Fukunaga et al. 1996; Kawakami et al. 1993, 1995; Blazevich et al. 2009).
In conclusions, this study provides quantitative information on muscle volume (MV) and ACSA in thigh muscles of perimenopausal women, as measured by MRI. We found high correlations between ACSA and MV in the extensors, flexors, adductors and the sartorius. The optimal proximal-to-distal location with highest correlation between ACSA and MV varied between the thigh muscle groups (extensors, flexors, adductors, and sartorius), but acquisition of a single MR slice at the 50% location achieves the best overall correlation with MV across all muscle groups.
References
Abe T, Brechue WF, Fujita S, Brown JB (1998) Gender differences in FFM accumulation and architectural characteristics of muscle. Med Sci Sports Exerc 30:1066–1070
Abe T, Kumagai K, Brechue WF (2000) Fascicle length of leg muscles is greater in sprinters than distance runners. Med Sci Sports Exerc 32:1125–1129
Akagi R, Takai Y, Ohta M, Kanehisa H, Kawakami Y, Fukunaga T (2009) Muscle volume compared to cross-sectional area is more appropriate for evaluating muscle strength in young and elderly individuals. Age Ageing 38(5):564–569
Berg HE, Tedner B, Tesch PA (1993) Changes in lower limb muscle cross-sectional area and tissue fluid volume after transition from standing to supine. Acta Physiol Scand 148:379–385
Blazevich AJ, Coleman DR, Horne S, Cannavan D (2009) Anatomical predictors of maximum isometric and concentric knee extensor moment. Eur J Appl Physiol 105:869–878
De Ste CM, Deighan M, Armstrong N (2003) Assessment and interpretation of isokinetic muscle strength during growth and maturation. Sports Med 33:727–743
Doherty TJ (2003) Invited review: aging and sarcopenia. J Appl Physiol 95:1717–1727
Fukunaga T, Roy RR, Shellock FG, Hodgson JA, Edgerton VR (1996) Specific tension of human plantar flexors and dorsiflexors. J Appl Physiol 80:158–165
Fukunaga T, Miyatani M, Tachi M, Kouzaki M, Kawakami Y, Kanehisa H (2001) Muscle volume is a major determinant of joint torque in humans. Acta Physiol Scand 172:249–255
Kanehisa H, Ikegawa S, Tsunoda N, Fukunaga T (1994) Strength and cross-sectional area of knee extensor muscles in children. Eur J Appl Physiol Occup Physiol 68:402–405
Kawakami Y, Abe T, Fukunaga T (1993) Muscle-fiber pennation angles are greater in hypertrophied than in normal muscles. J Appl Physiol 74:2740–2744
Kawakami Y, Abe T, Kuno SY, Fukunaga T (1995) Training-induced changes in muscle architecture and specific tension. Eur J Appl Physiol Occup Physiol 72:37–43
Kubo K, Kanehisa H, Azuma K, Ishizu M, Kuno SY, Okada M, Fukunaga T (2003) Muscle architectural characteristics in young and elderly men and women. Int J Sports Med 24:125–130
Macaluso A, De Vito G (2004) Muscle strength, power and adaptations to resistance training in older people. Eur J Appl Physiol 91:450–472
Maganaris CN, Baltzopoulos V, Tsaopoulos D (2006) Muscle fibre length-to-moment arm ratios in the human lower limb determined in vivo. J Biomech 39:1663–1668
Morse CI, Degens H, Jones DA (2007) The validity of estimating quadriceps volume from single MRI cross-sections in young men. Eur J Appl Physiol 100:267–274
Narici MV, Roi GS, Landoni L, Minetti AE, Cerretelli P (1989) Changes in force, cross-sectional area and neural activation during strength training and detraining of the human quadriceps. Eur J Appl Physiol Occup Physiol 59:310–319
Narici MV, Landoni L, Minetti AE (1992) Assessment of human knee extensor muscles stress from in vivo physiological cross-sectional area and strength measurements. Eur J Appl Physiol Occup Physiol 65:438–444
Narici MV, Maffulli N, Maganaris CN (2008) Ageing of human muscles and tendons. Disabil Rehabil 30:1548–1554
Raj IS, Bird SR, Shield AJ (2010) Aging and the force-velocity relationship of muscles. Exp Gerontol 45:81–90
Ring-Dimitriou S, Steinbacher P, von Duvillard SP, Kaessmann H, Muller E, Sanger AM (2009) Exercise modality and physical fitness in perimenopausal women. Eur J Appl Physiol 105:739–747
Acknowledgments
We would like to thank the Paracelsus Medical University Forschungsfond for supporting this study and the participants who volunteered to take part in this MRI study.
Author information
Authors and Affiliations
Corresponding author
Additional information
Communicated by Arnold de Haan.
Rights and permissions
About this article
Cite this article
Cotofana, S., Hudelmaier, M., Wirth, W. et al. Correlation between single-slice muscle anatomical cross-sectional area and muscle volume in thigh extensors, flexors and adductors of perimenopausal women. Eur J Appl Physiol 110, 91–97 (2010). https://doi.org/10.1007/s00421-010-1477-8
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00421-010-1477-8