
Abstract
Matrix metalloproteases (MMPs) in the circulation are thought to modulate the activation of growth factors, cytokines, and angiogenesis, facilitating physiological adaptations to exercise training. The purpose of this work was to characterize serum MMP-1, MMP-2, MMP-3, and MMP-9 concentrations pre- and post-eight weeks of exercise training. We tested the hypothesis that exercise training would influence serum MMP concentrations in response to an acute resistance exercise test (ARET). Participants were randomized into an 8-week training program (5 days per week) that emphasized callisthenic (CT, N = 8) or resistance (RT, N = 8) exercise. Serum MMP concentrations (MMP-1, -2, -3, -9) were assessed in men (N = 16) in response to an acute bout of high-intensity resistance exercise (six sets of 10-RM squats with 2-min inter-set rest periods) both before and after 8 weeks of training. Training resulted in a temporal shift in the peak MMP-1 concentration from post-ARET to mid-ARET in both groups. Post-training, MMP-9 concentrations were increased immediately after the ARET in the CT group as compared to pre-training ARET concentrations. RT did not alter MMP-3 and -9 concentrations. These data suggest that the mode of exercise training influences the MMP response to an acute bout of exercise, revealing a possible role of MMPs in initiating training-specific adaptations.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The matrix metalloprotease (MMP) family of enzymes contribute to both normal and pathological tissue remodeling. Each MMP targets a specific substrate, thus, the appropriate MMP must be released in a time- and location-specific manner to orchestrate membrane remodeling and adaptation. Of the MMPs that have been characterized thus far, MMP-1 (Collagenase 1), MMP-2 (Gelatinase A), MMP-3 (Stromelysin 1), and MMP-9 (Gelatinase B) play critical roles in cleaving muscle-specific proteins and assisting in extracellular matrix formation, remodeling, and regeneration in skeletal and cardiac muscle, as well as the surrounding vasculature (Carmeli et al. 2005; Hashimoto et al. 2002; Kjaer 2004; Ribbens et al. 2002; Rullman et al. 2007; Visse and Nagase 2003; Woessner 1991).
Certain stimuli, particularly those that induce high levels of mechanical stress such as eccentric (Heinemeier et al. 2007; Koskinen et al. 2001) or high-impact exercise (Carmeli et al. 2005, 2007; Rullman et al. 2007) activate the local production of MMPs in skeletal muscle. It is generally accepted that MMPs function in skeletal muscle to process extracellular matrix (ECM) proteins, assisting in matrix degradation and repair, while those released into the circulation facilitate angiogenesis (Giannelli et al. 2005; Kjaer 2004; Suhr et al. 2007). MMPs in the circulation are also thought to modulate the activation of growth factors and cytokines through degradation of their precursors, binding proteins, and inhibitors (Hashimoto et al. 2002; Nakamura et al. 2005).
Although investigators have explored the effects of an acute bout of exercise on MMP concentrations in skeletal muscle (Carmeli et al. 2005; Rullman et al. 2007) and plasma (Saenz et al. 2006; Tayebjee et al. 2005), the effects of exercise training on circulating MMP concentrations have not been elucidated. Since serum concentrations of MMPs are reported to peak within a relatively short time period following a single bout of exercise, it is possible that post-training serum concentrations of MMPs represent the effects of repeated bouts of exercise that have initiated adaptive responses in skeletal muscle. To this end, it is not known whether different exercise training programs, to include one that incorporates machine-based resistance exercises and one composed of aerobic and bodyweight exercises such as pull-ups, push-ups and sit-ups, promote different MMP responses. Such information would be valuable in understanding whether the type of exercise and the specific MMP response plays a role in mediating physiological adaptations to exercise training. Additionally, previous investigations have only focused on one or two MMPs, and the effects of exercise on circulating concentrations of the various MMPs have not been elucidated.
Therefore, the primary objective of this study was to characterize serum MMP-1, MMP-2, MMP-3, and MMP-9 concentrations pre- and post-eight weeks of exercise training. To maximize the practical application of our exercise model, a second objective of this study was to examine the effects of two different exercise training programs on serum concentrations of the MMPs: a callisthenic-based training program (CT) that emphasized bodyweight exercises, or a resistance training program (RT) that emphasized high-intensity training with free-weights and machines with the thought that high force exercises in the RT group might enhance serum concentrations of specific MMPs. We hypothesized that exercise training would influence serum basal MMP concentrations suggesting their role in mediating adaptations to exercise stress.
Materials and methods
Subjects
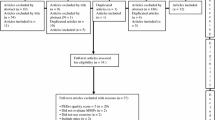
All methods were reviewed and approved by the Human Use Review Committee of the U.S. Army Research Institute of Environmental Medicine before the start of the study. Similar to Harman et al. (2008) entering Cohen’s tables with the SDs of the tests employed, the desired effect size of 1 SD, a power of 0.80, and a two-tailed α of 0.05, it was determined that the needed sample size was 15 per group. Twenty-one untrained men (non-military, 19–35 years) per group were initially recruited to account for attrition. Sixteen men completed the study. Participants had all experimental methods explained to them, and participated in this experiment after giving their free and voluntary informed consent. Subjects were recreationally active, defined as participating in less than 3 h of structured physical activity per week for the previous 6 months. All were pre-screened via a health history questionnaire and an examination by a physician. Investigators adhered to the policies for protection of human subjects as described in Army Regulation 70-25, and research was conducted in adherence with the provisions of 32 CFR Part 219 and in compliance with the principles enunciated in the Helsinki Declaration. Subjects were randomly, but equally assigned into two training groups: a callisthenic-specific training program (CT; age 29.6 ± 0.7 years, height 181.3 ± 1.2 cm) and a resistance exercise-specific training program (RT; age 26.6 ± 0.7 years, height 176.7 ± 0.5 cm), both designed to improve military performance. There were no differences in subject demographics between the two training groups at baseline.
Experimental design
One week prior to the start of the training programs, each subject participated in an acute resistance exercise test (ARET) and a series of exercises designed to assess physical performance (maximal oxygen consumption [VO2 max], one repetition maximum [1-RM] squat, and 1-RM bench press). The ARET is a resistance exercise test comprised of six sets of the individual’s 10-RM squat, separated by 2-min inter-set rest periods. The initial 10-RM squat weight used was approximated as 75% of the subject’s 1-RM measured during baseline testing sessions. Verbal encouragement was provided to ensure maximal effort and proper form. If a subject could not successfully perform ten repetitions, the weight was reduced to facilitate completion of ten full range-of-motion repetitions. One week after the completion of baseline testing, subjects began 8 weeks of exercise training of either CT or RT. The nature of the exercises depended on the group to which they were randomized (CT or RT) (Harman et al. 2008). Briefly, both groups performed a variation of warm-up and stretching exercises and trained on 5 days per week. Following the initial warm-up, the CT group had calisthenics, conditioning drills, and distance running stressed, while the RT group had agility drills, load carriage road marching, and weight training stressed. Both groups performed interval sprinting and both programmes were progressive in nature. The exercise programmes and performance measures of the CT and RT groups has recently been described in detail by Harman et al. (2008). An overview of the training programmes and performance measures is provided in Tables 1 and 2. After the eighth week of training, subjects completed a post-training ARET and VO2 max, 1-RM squat, and 1-RM bench press assessment to draw pre-training comparisons in performance changes.
Performance assessment and body composition
VO2 max was measured on a Trackmaster® TMX425C treadmill (Fullvision Inc., Newton, KS) with a ParvoMedics (Salt Lake City, UT) TrueMax 2400 metabolic gas analyzer system and cart, using a continuous, uphill, stepwise modified Bruce protocol (Volkov et al. 1975). To assess 1-RM squat strength, participants first warmed up with three sets of increasing sub-maximal loads using a standard Olympic style bar and a squat rack. The 1-RM was determined according to ACSM guidelines as the last weight used for a successful, but not repeated, lift (ACSM 2005). A similar protocol was used to assess 1-RM bench press strength using a standard Olympic style bar.
Body composition was assessed in all subjects at baseline and following the last training session using Dual Energy X-ray Absorptiometry (DEXA) (LUNAR Prodigy, GE Lunar Corporation, Madison, WI). Total body scans were performed and analyzed according to manufacturer recommendations (Total Body Analysis, version 3.6, Lunar Corp., Madison, WI). Data were obtained for fat mass and fat-free mass (Table 2).
Exercise training
Participants completed exercise training 5 days per week for a period of 8 weeks. The standardized Army physical training (CT group) consisted of moderate distance running, intervals, and calisthenics. The calisthenics included body-weight supported exercises to failure, such as push-ups, sit-ups, pull-ups and other exercises from U.S. Army Field Manual No. 21-20, the guide to which all formal physical training of the U.S. Army is conducted. The RT group performed resistance training on Monday and Thursday. Typical RT training was performed using standard Olympic-style bars and equipment and consisted of three sets of exercises for each of the four major muscle groups (chest, back, arms, and legs). Subjects performed one set of each exercise, progressing to three sets by the end of the 8-week training program. The goal was to perform eight repetitions during each set, which approximated an intensity of 80% of the participant’s 1-RM. When eight repetitions could be completed, the resistance was increased. Rest between each exercise was ~30 s and rest between each group of exercises was 2–3 min. The weight training was completed in approximately 1 h, excluding warm-up. After each weight training day, volunteers in the RT group ran 3.2 km at their own pace. The programs were similar in daily duration and approximate intensity, allowing us to attribute any training group differences to program type rather than duration or intensity of exercise training. A typical week of training for the CT and RT groups are depicted in Table 1 (Pierce et al. 2009).
Blood sampling
Basal blood draws were collected at baseline, mid-, and post- training via venipuncture between 0700 and 0900 hours after an overnight fast (1900 hours the night prior). Blood samples were also collected during the ARET using an indwelling venous catheter (pre-, mid-, immediately post-, 15 min post-, and 30 min post-ARET) at baseline (0 weeks) and post-training (9 weeks). Serum concentrations of MMPs were corrected for albumin to account for plasma volume shifts.
MMP multiplexed analysis
Circulating serum MMP concentrations were analyzed using a commercially available multiplex bead-based antibody sandwich assay (R&D Systems, Inc., Minneapolis, MN) which combined color-coded microparticles (coded for each analyte) with lasers and flow cytometry to quantify analyte concentrations in 15 μl of serum. Color-coded microspheres were identified by one laser, and streptavidin–phycoerythrin conjugate bound to the biotinylated detection antibodies on the spheres was excited by a second laser which quantified the amount of antigen present in the samples. Median fluorescence intensity from each bead set was calculated and translated to a concentration. The MMP kit was reported to have sensitivities of 4.4, 25.4, 1.3, and 7.4 pg/ml for MMP-1, -2, -3, and -9, respectively. Samples were run in duplicate and intra- and inter-assay coefficient of variations (CVs) for the MMP panel were <10%. All samples were analyzed on a Luminex 200 System (Luminex Corporation, Austin, TX) using Masterplex QT Software version 2.5 (MiraiBio, Inc., Alameda, CA).
Data analysis
Data were analyzed using repeated measures ANOVA with time (each time blood was drawn) as the within-subjects factor and group (CT or RT) as the between-subjects factor. When the ANOVA revealed a significant F ratio, a Tukey’s HSD post hoc test was employed to determine statistical differences. There was one ANOVA ran for the exercise-induced MMP response, and another ANOVA ran for the basal MMP concentrations. Statistical analyses were performed using SPSS (SPSS, v. 15.0; Chicago, IL). All data are presented as mean ± SE. An alpha level of P ≤ 0.05 was considered statistically significant for all data.
Results
Effects of training
Results for total body, lean, and fat mass are presented in Table 2. There were no changes in body mass over the 8 weeks of training in the RT or CT groups. Over the training period, there was a 3% increase in lean mass (P ≤ 0.01); however, this increase was independent of exercise group. A group × time interaction was observed for fat mass (P ≤ 0.05), and indicated that as a result of training, fat mass decreased in the RT group (pre: 17.1 ± 2.7 kg vs. post: 14.4 ± 2.9 kg; P ≤ 0.01), but not in the CT group (pre: 20.0 ± 3.3 kg vs. post: 19.2 ± 3.2 kg; P ≥ 0.05).
Results for VO2 max and 1-RM for the squat and bench press are presented in Table 2. VO2 max increased 10% as a result of training in both groups (P ≤ 0.01) with no differences in VO2 max between groups over time. For the bench press, the subjects experienced a 12% increase in 1-RM strength (P ≤ 0.01) with no group differences. However, there was a group × time interaction for 1-RM squat. Tukey’s post hoc analysis revealed that the increase in 1-RM squat strength was greater for the RT (21%) versus CT (10%), respectively (P ≤ 0.05).
Exercise-induced MMP concentrations
Exercise-induced MMP-1
There was a significant interaction effect for MMP-1 responses during the ARET when examined pre- to post-training (P ≤ 0.01); however, there were no differences between the RT and CT groups (data not shown; group data collapsed; Fig. 1a). Tukey’s post hoc testing revealed that pre-training, MMP-1 concentrations were highest at the immediate post-ARET time point (5.1 ± 0.6 ng/mL). Post-training, MMP-1 concentrations were highest mid-ARET (5.1 ± 0.9 ng/mL) compared to other time points, as well as compared to the mid-ARET time point pre-training (post-training: 5.1 ± 0.9 ng/mL vs. pre-training: 4.1 ± 0.7 ng/mL; P ≤ 0.05, Fig. 1a).

MMP-1 and MMP-2 concentrations in response to exercise. Serum MMP-1 and MMP-2 concentrations pre-, mid- and post-ARET (acute resistance exercise test: six sets of 10-RM barbell squats). a represents MMP-1, groups collapsed [callisthenic training (CT) + resistance training (RT)]; b represents MMP-2, groups collapsed (CT + RT). Values are mean ± SE. (*) P < 0.05, significantly different from pre-training at the same time point. There were no differences between groups
Exercise-induced MMP-2
The ARET-induced MMP-2 response was altered as a consequence of exercise training, but was not different between the RT and CT groups (data not shown; group data collapsed; Fig. 1b). There were no group interaction effects for MMP-2 concentrations in response to the ARET, but the main time effect demonstrated that MMP-2 concentrations in response to the ARET were highest immediately post-ARET pre-training and highest mid-ARET post-training (pre-training, immediately post-ARET: 236.2 ± 19.8 ng/mL vs. post-training, mid-ARET 230.8 ± 18.3 ng/mL).
Exercise-induced MMP-3
The MMP-3 response during the ARET was different as a result of training and also dependent on the mode of exercise. Figure 2a illustrates that prior to the 8 weeks of exercise training, MMP-3 concentrations increased in the CT group during the ARET to peak at the post-exercise time point (28.9 ± 4.7 ng/mL, P ≤ 0.05). Following exercise training, however, MMP-3 concentrations did not change during the ARET in the CT group. No changes were observed in the RT group pre- or post- training (Fig. 2c).

MMP-3 and MMP-9 concentrations in response to exercise. Serum MMP-3 [a callisthenic training (CT), c resistance training (RT)] and MMP-9 (b CT, d RT) concentrations pre-, mid- and post-ARET (acute exercise test: six sets of 10-RM barbell squats). Values are mean ± SE. (*) P < 0.05, significantly different from pre- (MMP-3) or post- (MMP-9) training
Exercise-induced MMP-9
The ARET-induced MMP-9 response demonstrated a divergent response between the two exercise training groups and was altered as a result of exercise training (Fig. 2b, d). Prior to training, MMP-9 concentrations in the CT group decreased during the ARET (n.s.), then increased for the duration of the recovery (Fig. 2b). Following training, however, MMP-9 concentrations in the CT group increased during the ARET, then decreased for the duration of the recovery (Fig. 2b). Alterations in the acute MMP-9 response did not occur in the RT group (Fig. 2d).
Basal MMP concentrations
Basal MMP-1
A group × time interaction indicated that in the RT group, basal MMP-1 concentrations increased 24.4% from pre- to mid-training (P ≤ 0.05, Table 3). No further increases were documented from mid- to post-training.
Basal MMP-2
A group × time interaction indicated that in the CT group, basal MMP-2 concentrations decreased by 35% from pre- to mid-training (pre-training: 296.1 ± 37.4 ng/mL vs. mid-training: 192.5 ± 12.4 ng/mL; P ≤ 0.05, Table 3). In the RT group, there was no effect of training on basal MMP-2 concentrations.
Basal MMP-3
A group × time interaction indicated that in the CT group, basal MMP-3 concentrations decreased 39% from pre- to mid- training (pre-training: 25.2 ± 3.1 ng/mL vs. mid-training: 15.3 ± 2.0 ng/mL; P ≤ 0.01, Table 3). Post hoc testing revealed that MMP-3 concentrations were not altered in the RT group as a result of training.
Basal MMP-9
Basal MMP-9 concentrations were altered in both exercise groups as a result of exercise training. However, the responses of the RT and CT groups were different (Table 3). In the CT group, there was a 130% increase from mid- to post-training (P ≤ 0.05), with no differences between pre- and post-training. In the RT group, basal MMP-9 concentrations increased throughout the 8 weeks of training and post-training concentrations were higher than pre-training values (pre-training: 128.0 ± 38.2 ng/mL vs. post-training: 256.0 ± 38.6 ng/mL; P ≤ 0.05).
Discussion
This study has demonstrated that the pattern of MMP release in response to a single bout of resistance exercise was altered as a result of the 8 weeks of callisthenic-type exercise training. Specifically, MMP-1 and MMP-3 concentrations increased during the ARET pre-training in both groups; however, following 8 weeks of training, this response was only different in the CT group. Furthermore, despite the absence of an increase in MMP-9 concentrations pre-training in response to a single bout of exercise, peak MMP-9 concentrations were higher after a single bout of exercise in the CT group post-training. Additionally in the CT group, MMP-3 and MMP-9 concentrations were higher 30 min into recovery post-training, as compared to pre-training. Thus, the circulating MMP response to a single bout of high-intensity exercise appears to be dependent on the mode of exercise training and may facilitate training-specific adaptations (Koskinen et al. 2001; Mackey et al. 2006; Rullman et al. 2007).
In a study by Rullman et al. (2007), the authors characterized the MMP response in human skeletal muscle biopsies taken immediately after a single bout of moderate-intensity cycling exercise and 120 min into recovery. Skeletal muscle mRNA and protein for MMP-9 increased exponentially immediately following exercise until 120 min thereafter, while no changes were observed in MMP-2 concentrations. Likewise, in humans, Koskinen et al. (2001) reported a slight increase in serum MMP-9 concentrations following a single bout of downhill running, with no measurable changes in MMP-2. Conversely, in humans, Mackey et al. (2006) reported that serum MMP-2 and MMP-9 concentrations were not different 24 h through 10 days following a 10 km run or after 50 min of deep water running (Mackey et al. 2006). Taken together, along with the current findings, these data provide important information regarding the MMP response to exercise in humans. First, it is likely that the serum MMP response is transient, with peak alterations occurring either during or within the first few hours following an exercise bout. Second, the mechanism of induction might be related to the mode of exercise training, and this response may impact specific remodeling and regenerative cascades in the vasculature (e.g. in response to aerobic-based training) or skeletal muscle (e.g. resistance-based training), depending on the nature and intensity of the exercise training. However, in interpreting these data and respective comparisons, it is critical to consider the data from the current investigation represent systemic responses, and may not be a good reflection of local skeletal muscle adaptation.
Basal MMP concentrations were also assessed at baseline, after 4 weeks, and upon the completion of the exercise training programs. In addition to the acute changes in MMP concentrations, recent data suggests that circulating MMPs play an integral role in growth factor bioavailability, capillary growth, cytokine regulation, and atherosclerotic plaque disruption (Coppock et al. 2004; Fowlkes et al. 1995, 2004; Hashimoto et al. 2002; Kai et al. 1998; Kasahara et al. 1997; Roberts et al. 2006; Tayebjee et al. 2005). Previously, Roberts et al. (2006) examined the effects of a three week exercise intervention on circulating MMP-9 concentrations in obese men diagnosed with metabolic syndrome. Aerobic exercise similar in mode, though not intensity, to that prescribed in the present study, resulted in a decrease in resting serum MMP-9 concentrations (Roberts et al. 2006). Roberts et al. (2006) attribute this decrease to an improved cardiovascular profile, with a reduced risk of atherosclerotic plaque destabilization.
Interestingly, in regards to basal MMP concentrations in the present study, the CT intervention had no effect on serum MMP-9 concentrations, while the RT intervention resulted in an increase in MMP-9 concentrations. An explanation for these contrasting results is evident when analyzing the specific MMP-9 concentrations in our subject population as compared to those in the study by Roberts et al. (2006). Primarily, the serum MMP-9 concentrations that we report here were ~25% of those reported by Roberts et al. (2006) in patients with coronary syndrome (~750 ng/mL vs. 200 ng/mL). Thus, we suggest that unless a pathological condition is present, MMP-9 concentrations are not likely to decrease as a result of training.
In the RT group, the observed increases in serum MMP concentrations may provide evidence to support the role of serum MMPs in regulating specific adaptations in skeletal muscle as a result of exercise training. In the present study, the RT group, which incorporated resistance-type exercises that are more likely to provide mechanical stressors resulting in extracellular matrix remodeling and an up-regulation of local growth factors, basal MMP concentrations (MMP-1, -2, -3 and -9) in the serum were higher post-training. An increased level of circulating MMP-1 and MMP-2 has been shown to facilitate growth factor bioavailability via IGFBP proteolysis (Fowlkes et al. 1995, 2004). If this is the case, increased growth factor bioavailability would be a reasonable mechanism through which circulating MMPs in the serum stimulate anabolic functions through IGF-associated downstream tissue remodeling. Alternatively, based on the specific tissue remodeling roles associated with individual MMPs, local release of MMPs from the muscle into the serum are indicative of specific structural alterations to the extracellular matrix. MMP-3 and MMP-9 have specific roles in degrading components of the basal lamina and type IV collagen, respectively (Kjaer 2004; Koskinen et al. 2001; Mackey et al. 2006), suggesting that they each serve specific roles in contributing to training-specific adaptations in muscle. Of particular significance is the evidence provided regarding the importance of MMP-3 in facilitating satellite cell migration through the basal lamina (Nishimura et al. 2008), as satellite cells contribute to hypertrophy by adding their nuclei to growing muscle fibers. Thus, our observations that serum concentrations of MMP-3 and 1-RM squat strength increased, while fat mass decreased in the RT group, as compared to the CT group, provides additional evidence to support a training specific adaptation mediated in part by MMP activation.
In summary, our work demonstrates that an acute bout of high-intensity resistance exercise results in transient increases in several of the MMPs, and this increase is still present following a second bout of exercise after 8 weeks of exercise training. However, this work shows that exercise training results in a temporal shift in MMP concentrations, such that peak MMP concentrations occur earlier in the post-training acute exercise bout. These results imply that the MMP system is activated in response to acute, high-intensity resistance exercise and exercise training does not attenuate this response. Thus, the MMP response is likely a critical component in skeletal muscle adaptation to exercise and the initiation of remodeling cascades. Finally, because we observed differential responses of the MMP system to different exercise training programs, we suggest that training-specific adaptations may be partially facilitated by the MMP response. Due to the purely systemic nature of these data, we view these results as preliminary and find it prudent to follow-up the current findings with an investigation examining the effects of these exercise training programs on transcriptional and translational adaptations in the MMP system in skeletal muscle.
References
ACSM (2005) ACSM’s guidelines for exercise testing and prescription. Lippincott Williams & Wilkins, Philadelphia
Carmeli E, Moas M, Lennon S, Powers SK (2005) High intensity exercise increases expression of matrix metalloproteinases in fast skeletal muscle fibres. Exp Physiol 90:613–619. doi:10.1113/expphysiol.2004.029462
Carmeli E, Haimovitz T, Nemcovsky EC (2007) Cathepsin D and MMP-9 activity increase following a high intensity exercise in hind limb muscles of young rats. J Basic Clin Physiol Pharmacol 18:79–86
Coppock HA, White A, Aplin JD, Westwood M (2004) Matrix metalloprotease-3 and -9 proteolyze insulin-like growth factor-binding protein-1. Biol Reprod 71:438–443. doi:10.1095/biolreprod.103.023101
Fowlkes JL, Thrailkill KM, Serra DM, Suzuki K, Nagase H (1995) Matrix metalloproteinases as insulin-like growth factor binding protein-degrading proteinases. Prog Growth Factor Res 6:255–263. doi:10.1016/0955-2235(95)00017-8
Fowlkes JL, Serra DM, Bunn RC, Thrailkill KM, Enghild JJ, Nagase H (2004) Regulation of insulin-like growth factor (IGF)-I action by matrix metalloproteinase-3 involves selective disruption of IGF-I/IGF-binding protein-3 complexes. Endocrinology 145:620–626. doi:10.1210/en.2003-0636
Giannelli G, De Marzo A, Marinosci F, Antonaci S (2005) Matrix metalloproteinase imbalance in muscle disuse atrophy. Histol Histopathol 20:99–106
Harman EA, Gutekunst DJ, Frykman PN, Nindl BC, Alemany JA, Mello RP, Sharp MA (2008) Effects of two different eight-week training programs on military physical performance. J Strength Cond Res Natl Strength Cond Assoc 22:524–534
Hashimoto G, Inoki I, Fujii Y, Aoki T, Ikeda E, Okada Y (2002) Matrix metalloproteinases cleave connective tissue growth factor and reactivate angiogenic activity of vascular endothelial growth factor 165. J Biol Chem 277:36288–36295. doi:10.1074/jbc.M201674200
Heinemeier KM, Olesen JL, Haddad F, Langberg H, Kjaer M, Baldwin KM, Schjerling P (2007) Expression of collagen and related growth factors in rat tendon and skeletal muscle in response to specific contraction types. J Physiol 582:1303–1316. doi:10.1113/jphysiol.2007.127639
Kai H, Ikeda H, Yasukawa H, Kai M, Seki Y, Kuwahara F, Ueno T, Sugi K, Imaizumi T (1998) Peripheral blood levels of matrix metalloproteases-2 and -9 are elevated in patients with acute coronary syndromes. J Am Coll Cardiol 32:368–372. doi:10.1016/S0735-1097(98)00250-2
Kasahara A, Hayashi N, Mochizuki K, Oshita M, Katayama K, Kato M, Masuzawa M, Yoshihara H, Naito M, Miyamoto T, Inoue A, Asai A, Hijioka T, Fusamoto H, Kamada T (1997) Circulating matrix metalloproteinase-2 and tissue inhibitor of metalloproteinase-1 as serum markers of fibrosis in patients with chronic hepatitis C. Relationship to interferon response. J Hepatol 26:574–583. doi:10.1016/S0168-8278(97)80423-0
Kjaer M (2004) Role of extracellular matrix in adaptation of tendon and skeletal muscle to mechanical loading. Physiol Rev 84:649–698. doi:10.1152/physrev.00031.2003
Koskinen SO, Hoyhtya M, Turpeenniemi-Hujanen T, Martikkala V, Makinen TT, Oksa J, Rintamaki H, Lofberg M, Somer H, Takala TE (2001) Serum concentrations of collagen degrading enzymes and their inhibitors after downhill running. Scand J Med Sci Sports 11:9–15. doi:10.1034/j.1600-0838.2001.011001009.x
Mackey AL, Donnelly AE, Swanton A, Murray F, Turpeenniemi-Hujanen T (2006) The effects of impact and non-impact exercise on circulating markers of collagen remodelling in humans. J Sports Sci 24:843–848. doi:10.1080/02640410500231470
Nakamura M, Miyamoto S, Maeda H, Ishii G, Hasebe T, Chiba T, Asaka M, Ochiai A (2005) Matrix metalloproteinase-7 degrades all insulin-like growth factor binding proteins and facilitates insulin-like growth factor bioavailability. Biochem Biophys Res Commun 333:1011–1016. doi:10.1016/j.bbrc.2005.06.010
Nishimura T, Nakamura K, Kishioka Y, Kato-Mori Y, Wakamatsu J, Hattori A (2008) Inhibition of matrix metalloproteinases suppresses the migration of skeletal muscle cells. J Muscle Res Cell Motil 29:37–44. doi:10.1007/s10974-008-9140-2
Pierce JR, Tuckow AP, Alemany JA, Rarick KR, Staab JS, Harman EA, Nindl BC (2009) Effects of acute and chronic exercise on disulfide-linked growth hormone variants. Med Sci Sports Exerc, pp 581–587. doi:10.1249/MSS.0b013e31818c6d93
Ribbens C, Martin y Porras M, Franchimont N, Kaiser MJ, Jaspar JM, Damas P, Houssiau FA, Malaise MG (2002) Increased matrix metalloproteinase-3 serum levels in rheumatic diseases: relationship with synovitis and steroid treatment. Ann Rheum Dis 61:161–166. doi:10.1136/ard.61.2.161
Roberts CK, Won D, Pruthi S, Kurtovic S, Sindhu RK, Vaziri ND, Barnard RJ (2006) Effect of a short-term diet and exercise intervention on oxidative stress, inflammation, MMP-9, and monocyte chemotactic activity in men with metabolic syndrome factors. J Appl Physiol 100:1657–1665. doi:10.1152/japplphysiol.01292.2005
Rullman E, Rundqvist H, Wagsater D, Fischer H, Eriksson P, Sundberg CJ, Jansson E, Gustafsson T (2007) A single bout of exercise activates matrix metalloproteinase in human skeletal muscle. J Appl Physiol 102:2346–2351. doi:10.1152/japplphysiol.00822.2006
Saenz AJ, Lee-Lewandrowski E, Wood MJ, Neilan TG, Siegel AJ, Januzzi JL, Lewandrowski KB (2006) Measurement of a plasma stroke biomarker panel and cardiac troponin T in marathon runners before and after the 2005 Boston marathon. Am J Clin Pathol 126:185–189. doi:10.1309/D7QUF0HJMCYYYY5A
Suhr F, Brixius K, de Marees M, Bolck B, Kleinoder H, Achtzehn S, Bloch W, Mester J (2007) Effects of short-term vibration and hypoxia during high-intensity cycling exercise on circulating levels of angiogenic regulators in humans. J Appl Physiol 103:474–483. doi:10.1152/japplphysiol.01160.2006
Tayebjee MH, Lip GY, Blann AD, Macfadyen RJ (2005) Effects of age, gender, ethnicity, diurnal variation and exercise on circulating levels of matrix metalloproteinases (MMP)-2 and -9, and their inhibitors, tissue inhibitors of matrix metalloproteinases (TIMP)-1 and -2. Thromb Res 115:205–210. doi:10.1016/j.thromres.2004.08.023
Visse R, Nagase H (2003) Matrix metalloproteinases and tissue inhibitors of metalloproteinases: structure, function, and biochemistry. Circ Res 92:827–839. doi:10.1161/01.RES.0000070112.80711.3D
Volkov NI, Shirkovets EA, Borilkevich VE (1975) Assessment of aerobic and anaerobic capacity of athletes in treadmill running tests. Eur J Appl Physiol Occup Physiol 34:121–130. doi:10.1007/BF00999924
Woessner JF Jr (1991) Matrix metalloproteinases and their inhibitors in connective tissue remodeling. FASEB J 5:2145–2154
Conflict of interest statement
None.
Author information
Authors and Affiliations
Corresponding author
Additional information
The opinions or assertions contained herein are the private views of the author(s) and are not to be construed as official or as reflecting the views of the Army or the Department of Defense. Citations of commercial organizations and trade names in this report do not constitute an official Department of the Army endorsement or approval of the products or services of these organizations.
Rights and permissions
About this article
Cite this article
Urso, M.L., Pierce, J.R., Alemany, J.A. et al. Effects of exercise training on the matrix metalloprotease response to acute exercise. Eur J Appl Physiol 106, 655–663 (2009). https://doi.org/10.1007/s00421-009-1063-0
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00421-009-1063-0