
Abstract
The objective of this study was to assess the effects of acupuncture applied at Hegu (LI 4) points and Neiguan (PC6) points on heart rate variability (HRV) in normal subjects under fatigue and non-fatigue states using power spectral analysis. Twenty-nine normal male subjects were randomly divided into three groups. Subjects in Group A and Group B performed a simulated driving task for 3 h and acupuncture needles were then inserted perpendicularly into the LI 4 points in the middle of the dorsal thenar muscle and PC 6 points situated between the tendons of the palmaris longus and carpi radialis muscles for 15 min for Group A but inserted subcutaneously to the acupuncture points for Group B as a control. Acupuncture needles were directly inserted perpendicularly into the LI 4 points and PC 6 points for 15 min for Group C. Stimulations of the acupuncture points induced a significant decrease in heart rate (HR), HRV total power (TP), low frequency (LF) power and ratio of low frequency to high frequency (LF/HF), and a significant increase in the HF power in normalized units (NU) during the post stimulation period in fatigue state (P<0.05). Stimulation of acupuncture points resulted in a significant increase both in the LF power and HF power in absolute units (AU) (P<0.05) but no significant change in NU was found during the post stimulation period in non-fatigue state. It was concluded that the modulating effect of acupuncture on heart rate variability not only depended on the points of stimulation such as acupuncture or non-acupuncture points but also on the functional state of the subject, namely whether the subjects are in a state of fatigue or not.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
When humans were under various kinds of stress, disturbances in the autonomic nervous system (ANS) were frequently induced, which could involve suppressed vagal and/or enhanced sympathetic functions (Wang et al. 2002). Driving is often stressful (Langford and Glendon 2002) and professional drivers are at higher risk for stress and fatigue related disease (Raggatt 1991). Long duty driving may cause higher blood pressure and thus cardiovascular risk as a result (Kobayashi et al. 2002). Appropriate restoration of the ANS functions would be beneficial to maintain a healthy life. Unfortunately, there are few effective and safe maneuvers to enhance the vagal output while suppressing the sympathetic functions.
The rationale for using acupuncture to modify behaviours associated with stress and feelings of distress are based on the untested assumption that acupuncture reduces the sympathetic nerve activity associated with arousal and stress (Knardahl et al. 1998). Some supports for the assumption that somatic afferent stimulation may decrease sympathetic nerve activity come from animal experiments (Chao et al. 1999). In hypertensive rats, direct electrical stimulation of the sciatic nerve produces hypoalgesia and profound reductions in arterial pressure and activity in the splanchnic sympathetic nerve lasting for several hours (Yao et al. 1982).
Frequency-domain analysis of heart rate variability (HRV) is a sophisticated noninvasive tool for the detection of ANS regulation of the heart. Spectral analysis of HRV in a normal subject during resting controlled conditions is characterized by three major components that account for almost all the power (i.e., variance, total power (TP) of the variability signal (Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology 1996). Two major oscillatory components at low (LF: 0.04–0.15 Hz) and high (HF: 0.15–0.40 Hz) frequency are usually detectable (Pagani et al. 1986). The LF component, which corresponds to the 0.10 Hz slow fluctuations of arterial pressure, mainly reflects sympathetic modulation of sinus node, whereas the HF component, which is a measure of respiratory sinus arrhythmias, can be considered an index of vagal (parasympathetic) modulation (Pagani et al. 1986; Malliani et al. 1991). The LF/HF ratio is considered to mirror sympathovagal balance (Montano et al. 1994) or to reflect the sympathetic modulations (Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology 1996; Pagani et al. 1997).
In human studies, the effect of acupuncture on the ANS has been varying. The most studied acupuncture points were the Hegu point (LI 4) in the middle of the dorsal thenar muscle (Suter and Kistler 1994) and Neiguan (PC6) points situated between the tendons of the palmaris longus and carpi radialis muscles (Li et al. 2004). Haker et al. (2000) reported that stimulation of Hegu point (LI 4) resulted in a significant increase in the sympathetic and the parasympathetic nerve activity during the stimulation period. Middlekauff et al. (2001) reported that acupuncture at PC6 and LI 4 attenuated the blood pressure response to mental stress in normal humans and the sympatho-excitation during mental stress was not attenuated by acupuncture. Our previous studies showed magnitopuncture at Dazhui (DU14) point which is between the spinous process of the seventh cervical vertebra and that of the first thoracic vertebra and Neiguan (PC6) points resulted in reduced sympathetic nerve activity and increased parasympathetic nerve activity at the end of driving task (Li et al. 2003). It was also reported that needle insertions in the vagal innervated area of the ear to induce reduced narcotic and alcoholic withdrawal symptoms and the underlying physiological mechanisms have been described as increased parasympathetic nerve activity (Mendelson 1978). Sugiyama et al. (1995) reported that sympathetic nerve activity increased during manual needle stimulation at the Tsusanli point (ST36) which is one finger breadth lateral to the inferior (distal) end of the tibial tuberosity, followed by a return of sympathetic nerve activity to basal levels after removal of the needle.
Since the temporary change of ANS activity is associated with the functional state of human body such as mental stress or fatigue (Pagani et al. 1989, 1994), it would be reasonable to hypothesize that the effects of acupuncture on ANS activity are associated with the functional state of human body. In this study, the effect of acupuncture at Hegu (LI 4) points and Neiguan (PC6) points on HRV was tested in normal subjects under fatigue and non-fatigue state.
Materials and methods
Subjects
The experimental procedures were approved by the University’s Ethics Committee and were performed in accordance with the ethical standards laid down in the 1964 Helsinki Declaration. Written informed consent was obtained from each subject before participating in the study. To avoid the influence of gender and age on HRV (Pagani et al. 1986; Liao et al. 1995), 29 normal male subjects aged 25.6±3.3 were recruited from staff and students within the Shanghai Jiaotong University to participate in the study. The subjects reportedly did not suffer from any illnesses nor were they taking any medication.
Driving simulator
At the driving simulator, the subject viewed a 32 inch. monitor at a distance of 2.5 m. A 3-h videotape showed the view of the road ahead, including other vehicles and roadside objects such as trees and traffic signs while driving through a scenic highway with few intersecting roads and scarcely any buildings. A speedometer was provided. In order to maintain an indicated speed of 80 km per hour, the position of the accelerator pedal was monitored. A small red light mounted in the middle of the dash stayed on when pedal pressure was kept within prescribed limits.
Procedure
The 29 normal male subjects were randomly divided into three groups, A (n=10), B (n=10) and C (n=9). All subjects were required to be well rested before the experiment. To avoid the influence of circadian fluctuations on HRV (Fauchier et al. 1998), the experiments were scheduled to be at the same time session (between 8.30 a.m. and 12.00 a.m.). All the subjects had a 10-min rest before starting their sessions. All the subjects maintained standard seating posture during the rest and test in an adjustable driving seat as described previously (Li and Wang 2001). Briefly, subjects were seated in a driving seat with knee angle and trunk-thigh angle at 120–135° and 110–120° respectively.
Test session for Group A
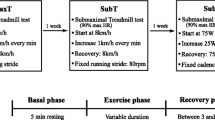
Figure 1 shows the procedure for test session for Group A. The subjects first had a 10 min rest and then performed simulated driving for 180 min. This was followed by a 2-min self-reporting for subjective fatigue. Then, acupuncture needles (Hwato,ϕ10.30×40 mm) were inserted perpendicularly into the Hegu (LI 4) points in the middle of the dorsal thenar muscle and Neiguan (PC 6) points situated between the tendons of the palmaris longus and carpi radialis muscles and manually stimulated for approximately 15 s to achieve the De-Qi sensation of heaviness, fullness, or soreness. The needles were left in place for 15 min, and then removed. Finally, the subjects rested for 10 min in the same seating posture. ECG was recorded throughout the session.

Test session for Group A. The subjects first had a 10-min rest and then performed a simulated driving for 180 min. This was followed by a 2-min self reporting, subsequently, acupuncture was administered for 15 min. ECG was recorded throughout the session
Test session for Group B
The subjects in Group B performed the same sequence as in Group A except that acupuncture needles (Hwato,ϕ10.30×40 mm) were inserted subcutaneously proximal (1.5 mm) to the acupuncture points used for the acupuncture group. No manipulation was performed.
Test session for Group C
The subjects in Group C did not perform the driving task. After a 10-min rest, acupuncture needles (Hwato,ϕ10.30×40 mm) were inserted perpendicularly into the Hegu (LI 4) points and Neiguan (PC 6) points and manually stimulated for approximately 15 s to achieve the De Qi sensation. The needles were left in place for 15 min, and then removed.
Subjective responses to the questionnaire were collected after the driving task for Group A and Group B with the Borg CR-10 scale (Borg 1982).
Measurement instrumentation and spectral analysis
During the test session, the subject was connected to an electrocardiogram (ECG) measuring system (FDP-1, Shanghai Medical University, ver 3.01) to record ECG signals for subsequent calculation of HR, HRV components. Throughout the experiment, ECG signals were collected on-line via three electrodes attached to the chest. These surface ECG signals were sampled at 250 Hz and recorded directly onto the hard disk of a computer through an A-D convertor having a 12 bits resolution. The manual editing of the R-R data was performed to ensure correct identification and classification of every QRS complex. Any R-R interval less than 0.4 sec (HR>150 bpm) or greater than 1.5 sec [HR≤40 bpm (beat per minute)] was identified and examined. Using an autoregressive (AR) model (order 12), the power spectrum of HRV was estimated from 256 R-R intervals of the heart beat (Pagani et al. 1986). For spectral analysis, the following variables were calculated (Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology 1996):
-
1.
The TP within the frequency range of 0–0.4 Hz.
-
2.
The LF power within the frequency range of 0.04–0.15 Hz.
-
3.
The HF power within the frequency range 0.15–0.4 Hz.
-
4.
The LF/HF ratio.
Spectrum components were expressed both in absolute unit (AU, ms2) and normalized unit (NU). The NU represents the relative value of each power component in proportion to the TP minus the VLF component (Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology 1996). The last 256 points of each 10-min R-R interval sequence were used for analysis.
All acupunctures were performed by the same certified acupuncturist. The skin was cleaned with alcohol.
Statistical analyses
Results were given as mean values±SD. The significance of differences within the groups was compared using one-way ANOVA with repeated-measures (SPSS version 11.5.1). The significance of differences among groups was compared using one-way ANOVA with post hoc multiple comparison procedures. Mann–Whitney rank sum test was used for subjective evaluation. P<0.05 was considered to be the level of statistical significance.
Results
Heart rate
Table 1 and Fig. 2 present the mean values of heat rate during the pre-task, end-task and post-stimulation periods. HR did not change significantly after the driving task in both Group A and control group (Group B). Stimulation of Hegu (LI 4) points and Neiguan (PC6) points produced a significant decrease in HR for both Group A and Group C in the post stimulation period (P<0.05). But subcutaneous stimulation did not produce such effect in HR for control group.

Mean heart rate during rest, end task and post stimulation periods for all test sessions
Heart rate variability
Total power
Table 1 and Fig. 3 present the mean values of TP during the pre-task, end-task and post-stimulation periods. The TP significantly increased at the end of driving task (P<0.05). Stimulation of Hegu (LI 4) points and Neiguan (PC6) points produced a significant decrease in TP during the post stimulation period for Group A (P<0.05). But the same stimulation produced a significant increase in TP for Group C (P<0.05). But subcutaneous stimulation of the same points did not induce significant change in TP for Group B. Significant differences in TP were also observed between Group A and Group B, Group A and Group C during the post stimulation period (P<0.05).

Total power (TP) during rest, end task and post stimulation periods for all test sessions
LF power
Table 1, Figs. 4 and 5 present the mean values of LF power (AU and NU) during the pre-task, end-task and post-stimulation periods. Significant increases in the LF power in AU (P<0.01) and in NU (P<0.05) were exhibited for Group A and Group B at the end of driving task. Stimulation of Hegu (LI 4) points and Neiguan (PC6) points produced a significant decrease in LF power both in AU (P<0.05) and NU (P<0.05) during the post stimulation period for Group A. However, the same stimulation produced a significant increase in LF power in AU (P<0.05) during the post stimulation period for Group C. Subcutaneous stimulation did not induce significant change in LF power during the post stimulation period for Group B.

LF power (AU) during rest, end task and post stimulation periods for all test sessions

LF power (NU) during rest, end task and post stimulation periods for all test sessions
HF power
Table 1, Figs. 6 and 7 present the mean values of HF power (AU and NU) during the pre-task, end-task and post-stimulation periods. The HF power in NU significantly decreased at the end of driving task for both Group A and Group B (P<0.05). Stimulation of Hegu (LI 4) points and Neiguan (PC6) points produced a significant increase in HF power in NU (P<0.05) during the post stimulation period for Group A. However, the same stimulation produced a significant increase in HF power in AU (P<0.05) for Group C. Subcutaneous stimulation did not induce significant change in HF power during the post stimulation period for Group B.

HF power (AU) during rest, end task and post stimulation periods for all test sessions

HF power (NU) during rest, end task and post stimulation periods for all test sessions
LF/HF ratio
Table 1 and Fig. 8 present the mean values of LF/HF ratio during the pre-task, end-task and post-stimulation periods. Stimulation of Hegu (LI 4) points and Neiguan (PC6) points produced a significant decrease in LF/HF ratio during the post stimulation period for Group A (P<0.05). However, the same stimulation did not induce significant change in LF/HF ration for Group C. Also subcutaneous stimulation did not induce significant change in LF/HF ratio during the post stimulation period for Group B.

LF/HF ratio during rest, end task and post stimulation periods for all test sessions
Subjective evaluation
Self-reporting is the most frequently used method for assessing fatigue (Milosevic 1997). It provides useful information concerning the subjective awareness of fatigue following the completion of a task. The subjective responses to the questionnaire with the Borg CR-10 scale (Table 1) were obtained before and after the simulated driving task for Group A, Group B and Group C. The scale (ranging 0–10) indicates the extent to which the subject has experienced each symptom (Borg 1982). The subjects of all groups were at non-fatigue state (rating fatigue at 0 or 0.5) at rest. The rating of subjective fatigue in the group A and group B were 5.2 and 5.1 respectively indicating evident fatigue feeling after the driving task. Significant difference was found between rest period and post driving period for Group A and Group B (P<0.05). No significant difference was found between Groups A and B after the driving task (Fig. 9).

Subjective evaluation of fatigue
Discussion
In the present study, we tried to avoid any confounding psychological and physical stress. The superficial needle insertion technique was presented in 1990 (Haker and Lundeberg 1990) and was considered as a control. Recently, a placebo acupuncture needle has been introduced to simulate an acupuncture procedure without penetrating the skin (Streitberger and Kleinhenz 1998). Kept in a tube, the placebo needle was not fixed inside the copper handle. Its tip was blunt, and when it touched the skin, a pricking sensation was felt by the subject, simulating the puncturing of the skin. Despite no skin penetration, the tip exerted a mechanical stimulation. According to the results presented by Kolzenburg and Handwerker (1994), a non-painful mechanical stimulation might induce an increase of the cutaneous blood flow and may also excite nociceptive primary afferents. No ideal method of placebo stimulation acupuncture exists at present.
According to Grandjean (1979), mental fatigue is part of functional states, which ranges from deep sleep, light sleep, drowsy, weary, hardly awake, relaxed, resting, fresh, alert, very alert, and stimulated and a state of alarm. During the rest period, no statistically significant differences in both HR and HRV were observed among the three groups indicating that all subjects were at the same functional state which can be defined as a non-fatigue state for the purpose of this study.
Heart rate (HR) has been used as a physiological measure of workload during driving conditions and used to monitor driver fatigue (Wildervanck et al. 1978). HR is sensitive to physical demand (Williams and Horvath 1995). In the present study, the non significant changes in average HR at the end of the driving task were probably the result of the small metabolic demand of the task itself. Stimulation of Hegu (LI 4) points and Neiguan (PC 6) points produced a significant decrease in HR in Group A and Group C during the post-stim period while superficial stimulation did not do so in control group C. The results suggested that acupuncture has a cardiosuppressive effect following acupuncture applied to the Hegu (LI 4) points and Neiguan (PC 6) points. Haker et al. (2000) reported similar results that stimulation of the Hegu (LI 4) points resulted in a statistically significant decrease of the HR at the end of the post-stimulation period.
The ANS provides the primary control of HR. The decreased response of HR following acupuncture could be attenuated by administration of atropine and propranolol (Nishijo et al. 1997). Therefore, the acupuncture-induced response of decrease in HR has been suggested to be a result of a reciprocal coordination of an increase in parasympathetic nerve activity and a decrease in sympathetic nerve activity (Nishijo et al. 1997). However, average HR is subject to too many control mechanisms and pathologic phenomena, and cannot be used as a reliable estimator of autonomic activity and tone (Malik and Camm 1993).
The LF power in AU and LF/HF ratio increased significantly at the end of the driving task period when compared with the pre-task period, indicating that the sympathetic nerve activity and sympatho-vagal balance became higher. The LF power in NU increased significantly and the HF power in NU decreased significantly, indicating a shift of sympathovagal balance toward a sympathetic predominance and a reduced vagal tone in the fatigue state. This was consistent with previous studies (Li et al. 2002, 2003; Jiao et al. 2004). The representation of LF and HF in NU tends to minimize the effect of the changes in TP on the values of LF and HF components and reflect the reciprocal interaction that characterizes sympathetic and vagal outflows in physiological conditions (Pagani et al. 1986; Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology 1996). Our results suggested that measures of HRV in NU have been more sensitive to mental effort and stress than has HR in laboratory tasks.
In the present study, stimulations of the LI 4 points and PC 6 points induced opposite effects to the stress and fatigue response, i.e., significant decrease in the TP, LF power (AU and NU) and LF/HF ratio, and a significant increase in the HF power (NU) in the post stimulation period in fatigue state. The same stimulation just induced a significant increase in LF power in AU and HF power in AU in non-fatigue state. The superficial stimulation did not induce significant changes in LF power and HF power in control group. Corresponding to different states (fatigue and non-fatigue), the LF and HF power were at different levels, and the acupuncture induced different effects on ANS. In fatigue state, stimulations of the LI 4 points and PC 6 points showed a significant modulation effect on the relative distribution between the two major oscillatory components [LF (NU) and HF (NU)], which indicated A shift of sympathovagal balance. In non-fatigue state, the acupuncture adopted in this study apparently induced a significant increase in activity of both the sympathetic and the parasympathetic nerve system during the post stimulation period in normal subjects, which was similar to the study by Haker et al. (2000), suggesting no modification in sympathovagal balance in non-fatigue state. The superficial stimulation did not induce significant effect on ANS in this study while the effects of the acupuncture stimulation were significant.
The mechanisms underlying the effects of acupuncture on the ANS functions have been analyzed in anesthetized animals. Acupuncture-like stimulation on the somatosensory pathway has proved to activate the sympathetic system, which is also known as the somatosympathetic reflex (Sato et al. 1996). This mechanism has been used to explain many physiological responses induced by acupuncture. However, there are some uncertainties with regard to the anatomical loci of acupuncture points, strength, and frequency of stimulation in animals. The mechanism defined in anesthetized animals may not readily be extrapolated to the effect of acupuncture observed in conscious humans.
It is important to point out that spectral analysis of R-R interval variability does not provide a direct estimate of the differential activity of either sympathetic or vagal nerves (Pagani et al. 1997). Such spectral analysis only furnishes quantitative markers of the neural modulation of the sino-atrial node, examined in closed loop conditions. It also depends upon the continuous interaction between neural and humoral factors and the target function.
In the present study, acupuncture on the Neiguan and Hegu points seemed to enhance vagal and suppress sympathetic activity. These effects on the ANS were just opposite to the stress and fatigue response, indicating that the acupuncture could reduce the effects of fatigue in a fatigue condition. The different effects of acupuncture on HRV suggested that the modulating effect of acupuncture on HRV not only depended on the points of stimulation such as acupuncture or non acupuncture points but also associated with the functional state of human body such as fatigue or non-fatigue in normal subjects. Although the relationship between acupuncture and ANS response is still ambiguous, we suggested that this acupuncture maneuver is a noteworthy adjuvant for reversing fatigue responses possibly with ANS involvement.
References
Borg G (1982) A category scale with ratio properties for intermodal and interindividual comparisons. Psychophysical judgment and the process of perception. VEB, Berlin, pp 25–34
Chao DM, Shen LL, Tjen-A-Looi S, Pitsillides KF, Li P, Longhurst JC (1999) Naloxone reverses inhibitory effect of electro-acupuncture on sympathetic cardiovascular reflex responses. Am J Physiol Heart Circ Physiol 276:H2127–H2134
Fauchier L, Babuty D, Autret ML, Poret P, Cosnay P, Fauchier JP (1998) Influence of duration and hour of recording on spectral measurements of heart rate variability. J Auton Nerv Syst 73:1–6
Grandjean E (1979) Fatigue in industry. Br J Intern Med 36:175–186
Haker E, Lundeberg T (1990) Acupuncture treatment in epicondylalgia: a comparative study of two acupuncture techniques. Clin J Pain 6:221–226
Haker E, Egekvist H, Bjerring P (2000) Effect of sensory stimulation (acupuncture) on sympathetic and parasympathetic activities in normal subjects. J Auton Nerv Syst 79:52–59
Jiao K, Li ZY, Chen M,Wang CT (2004) Effect of different vibration frequencies on heart rate variability and driving fatigue in normal drivers. Int Arch Occup Environ Health 77(3):205:212
Knardahl S, Elam M, Olausson B, Wallin BG (1998) Sympathetic nerve activity after acupuncture in humans. Pain 75(1):19–25
Kobayashi F, Watanabe T, Watanabe M, Akamatsu Y, Tomita T, Nakane T, Furui H, Takeuchi K, Okada A, Ohashi R, Hayano J (2002) Blood pressure and heart rate variability in taxi drivers on long duty schedules. J Occup Health 44(4):214–220
Kolzenburg M, Handwerker HO (1994) Differential ability of human cutaneous nociceptors to signal mechanical pain and to produce vasodilatation. J Neurosci 14:1756–1765
Langford C, Glendon AI (2002) Effects of neuroticism, extraversion, circadian type and age on reported driver stress. Work Stress 16(4):316–334
Li ZY, Wang CT (2001) Research on driver fatigue and ergonomics design of automobile. Mech Design Manufact Eng 30(138):12–14
Li ZY, Jiao K, Chen M, Wang CT (2002) Spectral analysis of heart rate variability as a quantitative indicator of driver mental fatigue, 2002-01-0090, SAE 2002. Trans J Passenger Cars Mech Sys 2003:249–254
Li ZY, Jiao K, Chen M, Wang CT (2003) Effect of magnitopuncture on sympathetic and parasympathetic activities in normal drivers during simulated driving. Eur J Appl Physiol 88: 404–410
Li ZY, Jiao K, Chen M, Wang CT (2004) Reducing the effect of driving fatigue with magnitopuncture. Accid Anal Prev 36(4):501–505
Liao DP, Barnes RW, Chambless LE, Simpson RJ, Sorlie P, Heiss G (1995) Age, race, and sex differences in autonomic cardiac function measured by spectral analysis of heart rate variability—the ARIC study. Am J Cardiol 76: 906–912
Malik M, Camm AJ (1993) Components of heart-rate-variability - what they really mean and what we really measure. American Journal of Cardiology 72(11):821–822
Malliani A, Pagani M, Lombardi F (1991) Cardiovascular neural regulation explored in the frequency domain. Circulation 84:482–492
Mendelson G (1978) Acupuncture and cholinergic suppression of the withdrawal symptoms: an hypothesis. Br J Addict 73:166–170
Middlekauff HR, Yu JL, Hui KK (2001) Acupuncture effects on reflex responses to mental stress in humans. Am J Physiol Regul Integr Comp Physiol 280:R1462–R1468
Milosevic S (1997) Drivers’ fatigue studies. Ergonomics 40(3):381–389
Montano N, Gnecchi Ruscone T, Porta A, Lombardi F, Pagani M, Malliani A (1994) Power spectrum analysis of heart rate variability to assess the changes in sympathovagal balance during graded orthostatic tilt. Circulation 90:1826–1831
Nishijo K, Mori H, Yosikawa K, Yazawa K (1997) Decreased heart rate by acupuncture stimulation in humans via facilitation of cardiac vagal activity and suppression of cardiac sympathetic nerve. Neurosci Lett 227(3):165–168
Pagani M, Lombardi F, Guzzetti S, Rimoldi O, Furlan R, Pizzinelli P, Sandrone G, Malfatto G, Dellorto S, Piccaluga E, Turiel M, Baselli G, Cerutti S, Malliani A (1986) Power spectral analysis of heart rate and arterial pressure variabilities as a marker of sympathovagal interaction in man and conscious dog. Circ Res 58:178–193
Pagani M, Furlan R, Pizzinelli P, Crivellaro W, Cerutti S, Malliani A (1989) Spectral analysis of R-R and arterial pressure variables to assess sympatho-vagal interaction during mental stress in humans. J Hypertension 7:S14–S15
Pagani M, Lucini D, Mela GS, Langewitz W, Malliani A (1994) Sympathetic overactivity in subjects complaining of unexplained fatigue. Clin Sci 87:655– 661
Pagani M, Montano N, Porta A, Malliani A, Abboud FM, Birkett C, Somers VK (1997) Relationship between spectral components of cardiovascular variabilities and direct measures of muscle sympathetic nerve activity in humans. Circulation 95:1441–1448
Raggantt PTF (1991) Work stress among long-distance coach drivers: a survey and correlation study. J Organ Behav 12:565–579
Sato A, Sato Y, Suzuki A, Uchida S (1996) Reflex modulation of catecholamine secretion and adrenal sympathetic nerve activity by acupuncture-like stimulation in anesthetized rat. Jpn J Physiol 46:411– 421
Streitberger K, Kleinhenz K (1998) Introducing a placebo needle into acupuncture research. Lancet 352:364–365
Sugiyama Y, Xue Y, Mano T (1995) Transient increase in human muscle sympathetic nerve activity during manual acupuncture. Jpn J Physiol 45:337–345
Suter B, Kistler A (1994) Does acupuncture influence the cardiovascuacupuncture system via the central nervous system?. Schweiz Med Wochenschr 124:36–38
Task Force of the European Society of Cardiology, the North American Society of Pacing Electrophysiology (1996) Heart rate variability. Standards of measurement, physiological interpretation, and clinical use. Circulation 93:1043–1065
Wang JD, Kuo TBJ, Yang CCH (2002) An alternative method to enhance vagal activities and suppress sympathetic activities in humans. Auton Neurosci-Basic Clin 100(1–2):90–95
Wildervank C, Mulder G, Michon J (1978) Mapping mental load in car driving. Ergonomics 21: 225–229
Williams R, Horvath S (1995) Recovery from dynamic exercise. Am J Physiol Heart Circ Physiol 268:H2311–H2320
Yao T, Andersson S, Thore P (1982) Long-lasting cardiovascular depression induced by acupuncture-like stimulation of the sciatic nerve in unanaesthetized spontaneously hypertensive rats. Brain Res 240:77–85
Acknowledgements
The authors would like to acknowledge Takashimaya Nippatsu Kogyo Co., Ltd. for funding this research and all the participants at Shanghai Jiaotong University and acupuncturist (Qi SH) at Zhongshan hospital for spending time and effort to help us in this study.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Li, Z., Wang, C., Mak, A.F.T. et al. Effects of acupuncture on heart rate variability in normal subjects under fatigue and non-fatigue state. Eur J Appl Physiol 94, 633–640 (2005). https://doi.org/10.1007/s00421-005-1362-z
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00421-005-1362-z