
Abstract
The purpose of this study is to compare a mechanical property of bone in world-class female athletes with different loading histories. Bone bending stiffness or EI (E is the modulus of elasticity and I, the moment of inertia) was measured noninvasively with the mechanical response tissue analyzer, that analyzes the response of bone to a vibratory stimulus. We evaluated the ulna, ulnar width, wrist density and tibia in 13 synchronized swimmers (SYN), eight gymnasts (GYM) and 16 untrained women (UNT) of similar age. Muscle strength in the flexors and extensors at elbows and knees was measured in the athletes. SYN were taller than GYM or UNT (168±0.7 vs. 152±1.1 or 157±1.2 cm, P< 0.01). Ulnar EI, Nm2, was similar in SYN and GYM (41±5.4 vs. 42±4.2, NS) and 50% higher than in UNT (27±2.1, P<0.05). Ulnar EI, Nm2 was related to ulnar width (r=0.497, P<0.002, n=37) but not to wrist density. Tibial EI, Nm2, in SYN and GYM (270±42 vs. 285±49, NS) was similar and more than twice as high as in UNT (119±6; p<0.05). Knee flexor strength measured at 60° s−1 and elbow extensor strength at 200° s−1 correlated with tibial EI (r=0.44 and 0.41, P<0.05). In spite of different loading histories, the tibiae and ulnas of world-class athletes showed similar high values for bending stiffness that exceeded values in untrained women. EI in the ulna could be related to bone width and in the tibia, to muscle strength.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
There is a great deal of information on the bone densities of athletes with different loading histories, but little information on the effect of different sports on the structure and mechanical properties of bone. Athletes whose bones are exposed to high-impact loads such as gymnasts are known to have high mineral density (Fehling et al. 1995), whereas athletes such as swimmers and synchronized swimmers, who train with low-impact loads in a buoyant environment have low or normal bone densities (Helge and Kanstrup 2002; Risser et al. 1990). Theoretically, there is the expectation that the higher density bones of gymnasts will have greater strength than the bones of synchronized swimmers because mineral content is a major determinant of bone strength (Weinstein 2000). This concept and bone density measurements fail to take into account the architecture, organization of tissue, mechanical properties and other factors that impart strength to bone (Martin and Ishida 1989), all of which can be collectively assessed in a single long bone (tibia or ulna) by a novel instrument we have shown previously to measure bone bending stiffness.
A direct noninvasive measurement of long bone strength that uses the response of a long bone to a low-frequency vibratory stimulus was invented for NASA to evaluate bone strength in astronauts after space flight (Young et al. 1979). Young et al. (1979) called the instrument the mechanical response tissue analyzer (MRTA). The analysis of the response produced by a vibration, was based on beam theory that could be related to long bone extrinsic stiffness or EI where E is equal to Young’s modulus of elasticity and I is the cross-sectional moment of inertia (Steele et al. 1988). The technique was biologically validated in the monkey tibia where it could be demonstrated that an in vivo measurement with the MRTA was highly correlated with the three-point bending in the same bones (see Fig. 1) (Roberts et al. 1996). The measurement was also validated in the human ulna by determining EI in the ulnas of patients with type 1 osteogenesis imperfecta, the classic fragile bone disease due to a genetic defect of collagen. Ulnas of normal bone density in patients showed decreased bending stiffness (Smith et al. 1994). The principle of the test, that is, the analysis of resonant frequencies produced by a vibration and its relation to torsional stiffness of long bones based on a simple beam model, was confirmed in other species (Lowet et al. 1991).

(With permission from the editors of the Journal of Medical Primatology.) A validation study in the tibias of Rhesus monkeys that shows the relationship of EIMRTA in the same bone in vivo to EIInstron in the excised tibia (r2=0.95, P<0.0001). Values from the MRTA were obtained in the tibias of live animals through skin and soft tissue and analyzed by a 6-parameter algorithm. Values of EIInstron were obtained in the same bones by three point bending after storage at −20°C, thawing and warming to 37°C. EIMRTA is consistently twice as high as EIInstron due to differences in the support systems for the test
The capability of the MRTA instrument to distinguish differences in the ulnas of men who exercised more or less than 6 h a week (Myburgh et al. 1993) suggested an application to a study in athletes. Our interest was to compare the effect of rigorous training in the water, a buoyant environment, to “high-impact” training on the ground in the bones of world-class athletes. We selected synchronized swimmers (SYN) and gymnasts (GYM) as the athletes for comparison of long bone bending stiffness. The purpose of this study is to determine bending stiffness, a mechanical property and index of strength, in the long bones of elite athletes trained in physical environments that would impose different types of loads on bone. We hypothesized that GYM would have higher bending stiffness than SYN. The second purpose of this study is to examine the role of muscle strength as a determinant of bending stiffness.
Methods
Subjects
Thirteen US Olympic female SYN were recruited from Stanford University Synchronized Swim Team and the Santa Clara Swim Club Aquamaids Team, and eight US National competitive female GYM from Stanford University Women’s Gymnastic Team to participate as study subjects. A control group of 16 sedentary women (UNT) were recruited on the basis of similar age with the two elite athletic groups. All subjects were screened by a health and physical activity questionnaire. All subjects were eumenorrheic. Each subject provided information on the level of physical activity (UNT), the number of years and yearly schedule (hours/day, days/week and weeks/year) of training in their major sport (GYM and SYN). GYM had a longer history of participation than SYN (13.9±0.57 vs. 10.4±0.51 year, P=0.05). The average training schedule (excluding competition time) in GYM was 4 h/day, 5 day/week, for 50 week/year or approximately 1,000 h/year, and in SYN, 6 h/day, 6 day/week for 47 week/year or approximately 1,690 h/year. Seven of the SYN reported a few hours a week of gymnastics for 2–3 years; two participated in ballet for 5 or 9 years a few hours each month, one played softball and one engaged in running a few hours a week for the past 2 years. The control group did not participate in any formal physical training. All subjects were briefed by the investigators about the benefits and risks of the experimental procedure, and provided informed written consent before participating in this study. The study protocol was approved by the Human Research Institutional Review Board at NASA Ames Research Center, Moffett Field, CA and the Institutional Review Board at California State Polytechnic University, Pomona, CA, USA.
Procedures
Average cross-sectional bending stiffness
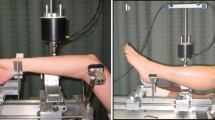
Average cross-sectional bending stiffness was determined by an instrument (MRTA) originally manufactured by Gaitscan, Inc, NJ and modified by NASA for use in human adults (see Fig. 2). Bending stiffness is EI in Nm2, where E is Young’s modulus of elasticity and I is the cross-sectional bending moment of inertia (Steele et al. 1988). EI is determined by analysis of the response to a low-frequency vibration generated by a mechanical shaker through a small probe placed on the skin surface over the center of the ulna or tibia. Force and acceleration are measured at the probe and transformed to a frequency response that is analyzed by a curve-fitting algorithm to determine the physical parameters of skin, bone and muscle. The results of this algorithm are highly correlated with breaking strength in long bones (Roberts et al. 1996; Hutchinson et al. 2001). The mathematical model for the ulna was modified for the analysis of the more complex curve from the human tibia by adding mass, stiffness and damping elements at both ends of the bone, where a firm support is difficult to achieve (Roberts and Steele 1995). This 12 parameter algorithm was used to analyze the tibial data in this study. The load carrying capacity of the bone is estimated from the maximum axial load or Pcr=EI(πL−1)2 divided by the body weight, a measurement termed “sufficiency” (S) to denote the number of body weights that can be supported by the bone.

A line drawing of the mechanical response tissue analyzer. For a test, the subject lies down on an exercise table. The tibia is supported by the two metal cylinders at the proximal end and the medial and lateral malleoli by the adjustable cylinders at the distal end of the support. The medial and lateral epicondyles at the elbow rest on the proximal cylinders and the wrist (radial side down) rests on the metal plate below the cylinders. The probe is automatically centered between proximal and distal supports and rests on the skin surface covering the tibia or ulna. Wires connecting the impedance head and magnetic shaker to the computer are not shown
Quality control (QC) of the instrument was determined by measurement of an aluminum rod with a known EI of 28.7 Nm2 . QC estimates were within 3.5% of the calculated EI [mean±SD: 27.7±1.3, coefficient of variance (CV) 4.8%]. The relocation of the instrument for the control group required a second QC estimate that was within 9% of the calculated EI (mean±SD: 31.7±1.2, CV 3.8%). Reproducibility was tested by repeated measures in the same individual. Based on the 7-parameter algorithm the CV of ulnar EI was 3.2% and on the 9-parameter algorithm 5.6%. Based on the 12-parameter algorithm, the CV of tibial EI was 10.8%.
Anthropomorphic measurements
Weight (kg), height (cm), ulnar and tibial lengths (cm) were measured. Body mass index (BMI = weight/(height)2) was calculated for each group. For ulnar length, the forearm is flexed at 90° at the elbow and a metal tape measure was placed at the tip of the ulna at the wrist and extended to the tip of the olecranon process. For tibial length, the subject is asked to sit on the exercise table and dangle the left leg so that the groove at the top of the tibia is easily palpable. The metal tape is extended from the groove at the knee to the distal edge of the medial malleolus at the ankle.
Ulnar bending stiffness
The subject lies down on an exercise table, head toward the MRTA instrument, and raises the forearm above the head, resting the epicondyles of the distal humerus on the top of the two small metal cylinders (attached to the proximal supports of the MRTA instrument). The wrist, radial side down, rests on the metal plate at the distal supports (Fig. 2). The distance between proximal and distal supports is adjustable, as is the height of the distal plate and proximal cylinders. The forearm is placed so that the ulna is uppermost, and the probe can be lowered and rested on the center of the bone. Centering between proximal and distal supports is automatic. A brief (10 s) vibration is given and then the resonant response is recorded, and analyzed by a computer program. The operator then evaluates the curve-fitting response using a 7-parameter algorithm originally developed by Gaitscan Inc. or a 9-parameter algorithm improved by one the investigators (CS). The root mean square error (RMSE) for the 3–5 ulnar EI tests on the same individual using the 9-parameter algorithm was between 3% and 7%.
Bone density of the wrist and ulnar width
Bone density of the left distal forearm was measured using a single photon densitometer (PIXI, Lunar Corporation, Madison, WI, USA). The CV of the BMD based on phantoms for the wrist was 3.45% and based on repeated measures of the same individual was 1.2%. A tennis ball was placed in the hand of each subject to ensure correct position of the wrist. The printed image of the distal forearm was used to estimate ulnar width. A caliper (Manostat Corporation, Geneva, Switzerland) was used to measure the width of the ulna 30 mm from the junction of the ulna and radius.
Tibial bending stiffness
The subject lies down on an exercise table and places the left tibia on the proximal supports, and the distal end of the tibia (the medial and lateral malleoli) on the distal supports so that the tibia is suspended. Then, the probe is lowered and placed on the center of the tibia, a brief (10 s) vibration is given and then the resonant response is recorded and analyzed. The operator then evaluates the curve-fitting response using the 12-parameter algorithm expanded from the original 7-parameter algorithm by one of the investigators (CS). The RMSE for the tibia EI measurement on the same individual using the 12-parameter algorithm was between 7% and 9.3%.
Skinfold thickness
The skinfold thickness over the triceps, subscapular, suprailiac, mid-thigh and medial calf muscles were measured by the same investigator with a caliper (Lange, Cambridge Scientific, Cambridge, MD, USA) according to the Anthropometric Standardization Reference Manual (Lohman et al. 1988).
Muscular isokinetic strength
The same investigator used a protocol that tested the strength (N-m) of knee and elbow flexors and extensors at the velocity of 60, 120 and 200° s−1 (Cybex Norm, Dallas, TX, USA). Average power (watt) of the elbow and knee flexor and extensor were determined, respectively, with 15 repetitions (elbow flexion and extension) or 30 repetitions (knee flexion and extension) at 120° s−1 . Due to software failure while the subjects (4 GYM) were performing the 120° s−1 knee flexion/extension measurement this isokinetic contractile velocity was not used for data analysis. Subjects were instructed to provide a maximum effort with a standard “cheering on” approach. Because of the high intensity of muscular dynamic strength required to perform the isokinetic test and to prevent muscular injury the UNT group was not tested.
Statistical analysis
All data are presented as means ± SE. Data were analyzed using one-way ANOVA and independent (two-sided) t-test statistics. Pearson correlation statistics was applied to examine the relationship between bone bending stiffness (ulna and tibia EI), muscular strength of the elbow and knee, ulnar EI and width or wrist density. The Student–Newman–Keuls test was used to evaluate the individual group differences after significant differences were established by ANOVA. All tests of statistical significance were set at P<0.05. Either a statistical software program SPSS version 10.0 (SPSS, Inc., Chicago, IL, USA) or a program developed by S.A. Glantz (Primer of Biostatistics, copyright 1988 by McGraw Hill, Inc.) was used for data analysis.
Results
Physical characteristics and history
Subjects’ physical characteristics are presented in Table 1. The age and weight of these two groups of athletes were nearly equal. However, SYN averaged 16 cm taller than GYM, and UNT averaged were 5 cm taller than GYM. The years of training in GYM exceeded those in SYN by 3.5 years (P<0.05). The sums of five skin fold thicknesses between these two groups of athletes were similar. As shown in Table 2, the average length of the tibia was 3.3 cm longer in SYN than GYM but similar in UNT and GYM. Ulnar lengths of the SYN, GYM and UNT were similar.
Ulnar and tibial bending stiffness
As shown in Table 2, EI obtained from the ulna and tibia in each group of athletes was greater than in UNT (P<0.05). EI in the ulna correlated with EI in the tibia in athletes (r=0.654, P=0.001, n=21, Fig. 3) but not in UNT. Average tibial EI cm−1, expressed per centimeter of bone to adjust for the longer tibia in SYN than GYM was similar in both groups (7.6±0.04 in SYN vs. 8.13±0.46 Nm2 /cm in GYM, NS). When EI in the ulna is adjusted to body weight for sufficiency (S), the highest values are shown in GYM compared to SYN and UNT (P=0.056). S in the tibia is similar in both athletic groups and greater than in UNT (P=0.001).

The relationship of bending stiffness in the ulna and in the tibia in 21 athletes (filled diamond) (r=0.654 P=0.001)
Ulnar width and wrist density
As enumerated in Table 2, the widths of the ulnas in each group were different from one another with GYM showing the highest, SYN slightly lower and UNT the lowest diameter (P=0.001). The widths in GYM were greater than in SYN. BMD in the wrist was greatest in GYM, intermediate in UNT and lowest in SYN. Ulnar width was correlated with EI in the athletes (r=0.546, P=0.05) and in all 37 subjects (r=0.497, P=0.002, Fig. 4). BMD was barely related to width in the athletes (r=0.427, P=0.053, n=21) but not in UNT or all 37 subjects. BMD was unrelated to EI in athletes (r=0.027, NS) and/or UNT (r=0.159, NS).

The relationship of bending stiffness in the ulna to width of the bone in SYN (filled triangle), GYM (filled square) and UNT (filled circle). Width was measured with calipers on the image of a bone record, 30 mm from the junction of the ulna and radius (r=0.497, P=0.002)
Muscle strength
The isokinetic strength measurements for the elbow and knee flexors and extensors for both groups of athletes are listed on Table 3. GYM had higher elbow flexor strength than SYN measured at the 60 (P<0.05) and 120° s−1 (P<0.01). SYN had stronger knee extensor and flexor strength (P<0.05) than GYM measured at 200° s−1 . Peak torque of knee extensor and flexors measured at a slower isokinetic velocities (i.e. at 60° s−1) and average power measured at 30-repetitions with 120° s−1 flexion/extension were not statistically different between the groups. Tibia EI values correlated with knee flexor strength measured at 60° s−1 (r=0.44, P<0.02) and elbow extensor strength at 200° s−1 (r=0.41, P<0.05). However, ulna EI was unrelated to any measurement of muscular strength.
Discussion
The most interesting result in our study was the similarity of bending stiffness in the long bones of GYM and SYN in spite of differences in muscular loading histories. Bending stiffness in the ulna and the tibia of the athletes was more than twice as high as in UNT, an indication of greater bone strength of the athletes than the untrained females. Training initiated during the growing years and continued at maximum effort during growth probably accounted for the differences in athletes and UNT (Courteix et al. 1998). Taafe et al. (1997) did not think earlier training influenced bone parameters in collegiate swimmers and runners, but the type and duration (i.e. hours per day) of training undertaken by world-class athletes in our study undoubtedly had some effect on their bone and muscle strength. Training for synchronized swimming involves long hours of highly repetitive exercises that use a variety of arm and leg sculling actions to accelerate, decelerate, rotate, turn, propel and lift the body out of the water. Synchronized swimmers develop a great deal more muscle strength in the lower extremities than regular distance swimmers who develop upper body strength (Elmslander et al. 1998). On the other hand, gymnastics is a sport with high-impact loading activity involving acceleration, deceleration, pushing and pulling movements with more muscle strength in the upper than lower extremities in a gravitational environment.
We expected higher BMD and EI values in GYM than SYN because of the well-known effect of high-impact exercise on bone mass (Snow-Harter et al. 1990; Taafe et al. 1997) and the well-known relationship of bone mass and strength (Weinstein 2000). Bone density of the distal ulna was higher in GYM than in SYN but there was no relationship between bending stiffness and bone density in the ulna. The lowest EI values were found in the UNT group with an intermediate bone density value relative to SYN and GYM. The important determinant of bending stiffness in the ulna in this study was the bone width, greater in athletes than UNT. There was a trend for width to be related to bone density in the athletes (P=0.053), but clearly no relationship between bone density and EI. If ulnar EI is adjusted for body weight, the maximal axial load capacity of the bone in terms of body weights (sufficiency) can be estimated. The highest value is in the GYM group, that is, a GYM ulna could support nearly 12 times her body weight, more than the 9.5 or 8.2 body weights supported by SYN or UNT, respectively. Although the EI values were similar in GYM and SYN, it is clear that the GYM ulna had the greatest strength in reference to body weight when compared to the other groups. Myburgh et al. (1993) found the greater width of the ulna to be a significant predictor of EI in men who were highly active compared to less or moderately active individuals. Duncan et al. (2002a, 2002b) found the medullary cavity cross-sectional areas in femurs to be wider in athletes exposed to low rather than high-load sports, a structural difference that would enhance the mechanical strength of bone. An increase in bone width is an adaptation in bone remodeling to compensate for mineral loss with age and maintain strength in the human radius (Burr and Martin 1983).
The magnitude and distribution of the strain generated in bone by synchronized swimming is clearly different than that induced by gymnastics (Rubin and Lanyon 1987). Gymnastics provides a high-impact- load that is a well-known osteogenic stimulus for the accrual of bone mineral (the “E” component of bending stiffness) in the ulna and tibia. In synchronized swimming, the nature of the stimulus that influences the architecture of bone is not yet identified. We speculate that the stimulus to bone must come from repetitive high-velocity muscular contractile force since two of our muscle strength measurements correlated with EI in the tibia.
Differences in muscular strength between these well-trained gymnasts and synchronized swimmers may be explained by differences in training techniques, training activities or volume and cross-training activity during the off-season. The exposure to some cross-training that used strength training devices or running activity in synchronized swimmers and in gymnasts is a possible explanation for the non-significant difference in ulna and tibia bending stiffness. Our study showed greater knee flexion and extension strength of high velocity (i.e. 200° s−1) in the synchronized swimmers than the gymnasts. This is because synchronized swimmers exert an equal amount of “moderate to high” velocity muscular contractile force from the upper and lower limbs. The greater high-velocity muscle strength in knee extensors and flexors in SYN than GYM may well have influenced the EI of the tibia. The observed relationship between tibia EI and muscle tensile force in elbow extensor at 200° s−1 and knee flexor at 60° s−1 suggest that high muscle tension may contribute to an osteogenic stimulus for bone growth or remodeling. The width of the ulnas in SYN and GYM was clearly greater than in UNT. There is little information on bone strength development in synchronized swimming.
The methodology we used to quantify bending stiffness may not have been sensitive enough to detect fine structural differences in the long bones of athletes exposed to different types of training even though there was a clear separation of EI in UNT and the athletes. We were also limited by group size and the rarity of world-class athletes. EI was similar in both groups of athletes in spite of such different loading histories and a slightly higher ulnar width in GYM than SYN. The technique is well validated not only by us in the non-human primate (Roberts et al. 1996; Hutchinson et al. 2001) but also by others (Lowet et al. 1991). There are significant differences in ulnar EI in right and left handed men (Arnaud et al. 1991). McCabe et al. (1991) reported lower EI in ulnas of older than young women and Kiebzak et al. (1999) reported low ulnar EI in women with osteoporosis. There is greater EI in highly active men compared to moderately active men (Myburgh et al. (1993).
We were interested in acquiring information on young females with training in different environments required to become national and Olympic level synchronized swimmers and gymnasts. One cannot rule out genetic influences on bone structure despite differences in muscular loading histories and length of training in their respective sport events. Genetics is recognized to be a major determinant in the development of the skeleton with genes that regulate not only bone mass but also structural and material properties (Blank 2001). Individual biological variation of genetic origin in our data for bending stiffness is suggested by the correlation of EI in the ulna and tibia in both athletic groups (Fig. 3).
To summarise we have found similarities in bending stiffness of two long bones in national and Olympic level competitive synchronized swimmers chronically exposed to a buoyant environment and in gymnasts who trained with high-impact loading activity. World-class athlete’s values in bending stiffness of the ulna and tibia were more than twice those determined in untrained controls. Whether bending stiffness in the bones of the synchronized swimmers was related to their genetic history or to the physical training for their sport is uncertain. Nevertheless, it is clear that bone strength similar to that in gymnasts can be generated by vigorous physical training of the type used in synchronized swimming.
References
Arnaud SB, Steele CR, Zhou L-Z, Hutchinson T, Marcus R (1991) A direct non-invasive measure of long bone strength. Proc Ann Int Cong IEEE Eng Int Med Biol Soc 13:1984–1985
Blank RD (2001) Breaking down bone strength: a perspective on future skeletal genetics. J Bone Miner Res 16:1207–1211
Burr DB, Martin RB (1983) The effects of composition, structure and age on the torsional properties of the human radius. J Biomech 16:603–608
Courteix DE, Lespessailes E, Peres SL, Obert P, Germain P, Benhamou CL (1998) Effect of physical training on bone mineral density in prepubertal girls: a comparative study between impact loading and non-impact loading sports. Osteoporosis Int 8:152–158
Duncan CS, Blimkie CJR, Kemp A, Cowell CT, Burke ST, Brody JN, Howman-Giles R (2002a) Bone mineral density in adolescent female athletes: relationship to exercise type and muscle strength. Med Sci Sports Exerc 34:286–294
Duncan CS, Blimkie CJR, Kemp A, Higgs W, Cowell CT, Woodhead H, Brody JN, Howman-Giles R (2002b) Mid-femur geometry and biomechanical properties in 15- to 18-yr-old female athletes. Med Sci Sports Exerc 34:673–681
Elmslander HC, Sinaki M, Muhs JM, Chao EY, Wahner HW, Bryant SC, Riggs BL, Eastell R (1998) Bone mass and muscle strength in female college athletes (runners and swimmers). Mayo Clin Proc 73:1151–1160
Fehling PC, Alekel L, Clasey J, Rector A, Stillman RJ (1995) A comparison of bone mineral densities among female athletes in impact loading sports. Bone 17:206–210
Helge EW, Kanstrup JL (2002) Bone density in female elite gymnasts: impact of muscle strength and sex hormones. Med Sci Sports Exerc 34:174–180
Hutchinson TM, Bakulin AV, Rakhmanov AS, Martin RB, Steele CR, Arnaud SB (2001) Effects of chair restraint on the strength of the tibia in rhesus monkeys. J Med Primatol 30:313–321
Kiebzak GM, Box JH, Box P (1999) Decreased ulnar bending stiffness in osteoporotic Caucasian women. J Clin Densitom 2:143–152
Lohman TG, Roche AF, Martorell R (1988) Anthropometric standardization reference manual, Human Kinetics Books, Champaign, pp 55–70
Lowet G, Van Audekercke R, Vander P, Geusans P, Dequejers J, Lammens J (1991) The relation between resonant frequencies and torsional stiffness of long bones in vitro. Validation of a simple beam model. J Biomech 26:689–696
Martin RB, Ishida J (1989) The relative effects of collagen fiber orientation, porosity, density, and mineralization on bone strength. J Biomech 22:419–426
McCabe F, Zhou L-Z, Steele CR, Marcus R (1991) Noninvasive assessment of ulnar bending stiffness in women. J Bone Miner Res 6:53–59
Myburgh K, Charette S, Zhou L-Z, Steele CR, Arnaud SB, Marcus R (1993) Influence of recreational activity and muscle strength on ulnar bending stiffness in healthy men. Med Sci Sports Exerc 25:592–596
Risser WL, Lee EJ, LeBlanc A, Pointdexer JM, Risser JM, Schneider V (1990) Bone density in eumenorrheic female college athletes. Med Sci Sports Exerc 33:570–574
Roberts SG, Steele CR (1995) End flexibility incorporated into a model of a vibrating human tibia for non-invasive measurement of bone properties. Ad In Bioeng Proc Intl Mech Eng Congr Expo 31:345–346
Roberts SG, Hutchinson T, Arnaud SB, Kiratli BJ, Martin RB, Steele CR (1996) Noninvasive determination of bone mechanical properties using vibration response: a refined model and validation in vivo. J Biomech 29(1):91–98
Rubin CT, Lanyon LE (1987) Osteoregulatory nature of mechanical stimuli: function as a determinant for adaptive remodeling in bone. J Orthop Res 5:300–310
Smith SR, Burshell A, Bober M, Smetherman D (1994) Adaptation of bone in a kindred with osteogenesis imperfecta. J Bone Miner Res 9:S424
Snow-Harter CM, Bouxsien M, Lewis B, Charette S, Weinstein P, Marcus R (1990) Muscle strength as a predictor of bone mineral density in young women. J Bone Miner Res 5(6):589–595
Steele CR, Zhou L-Z, Guido D, Marcus R, Heinrichs WL, Cheema C (1988) Noninvasive determination of ulnar stiffness from mechanical response—in vivo comparison of stiffness and bone mineral content in humans. J Biomech Eng 110:87–96
Taafe DR, Robinson TL, Snow CM, Marcus R (1997) High impact exercise promotes bone gain in well trained female athletes. J Bone Miner Res 12:255–260
Weinstein RS (2000) True strength. J Bone Miner Res 15:621–625
Young DR, Howard WH, Cann C, Steele CR (1979) Noninvasive measures of bone bending rigidity in the monkey (M. Nemestrina). Calcif Tissue Int 27:109–115
Acknowledgements
We gratefully acknowledge the generosity of the coaches and athletes who took the time to participate in our study. This study is partially supported by a NIH grant No. 5 S0 GM053933-06 and NASA No. SAA2-401535
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Liang, M.T.C., Arnaud, S.B., Steele, C.R. et al. Ulnar and tibial bending stiffness as an index of bone strength in synchronized swimmers and gymnasts. Eur J Appl Physiol 94, 400–407 (2005). https://doi.org/10.1007/s00421-005-1351-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00421-005-1351-2