
Abstract
One purpose of this study was to characterize the facial skin temperature and cold-induced vasodilation (CIVD) response of 12 subjects (six males and six females) during exposure to cold wind (i.e., −10 to 10°C; 2, 5, and 8 m/s wind speed). This study found that at each wind speed, facial skin temperature decreased as ambient temperature decreased. The percentage of subjects showing facial CIVD decreased significantly at an ambient temperature above −10°C. A similar CIVD percentage was observed between 0°C dry and 10°C wet (face sprayed with fine water mist) at each wind speed. No CIVDs were observed during the 10°C dry condition at any wind speed. The incidence of CIVD response was more uniform across facial sites when there was a greater cold stress (i.e., −10°C and 8 m/s wind). Another objective of the study was to examine the effect of the thermal state of the body (as reflected by core temperature) on the facial skin temperature response during rest and exercise. This study found that nose skin temperature was significantly higher in exercising subjects with an elevated core temperature even though there was no significant difference in face skin temperature between the two conditions. Therefore, this finding suggests that acral regions of the face, such as the nose, are more sensitive to changes in the thermal state of the body, and hence will stay warmer relative to other parts of the face during exercise in the cold.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Unlike the vast amount of data available for the cold-induced vasodilation (CIVD) response in the extremities, there is limited CIVD data for the face, even though the face is also commonly exposed bare to the cold wind and is also a region of the body with a high risk of frostbite (Lehmuskallio 2000). Numerous past studies have examined the effects of cold wind exposure on facial cooling (Siple and Passel 1945; LeBlanc et al. 1976; Virokannas and Anttonen 1994; Makinen et al. 2000, 2001). However, very few of these studies examined the CIVD response in the face. Gavhed et al. (2000) speculated that CIVDs could be beneficial to individuals exposed to the cold because they “reduce the risk of frostbite, enhance the nutritional skin blood flow, and possibly reduce pain sensation.”
A few studies did examine the CIVD response in the face, but they did so by examining the effect of cooling by directly applying crushed ice or an “ice candle” to a small region of the face (Lewis 1930; Fox and Wyatt 1962) as opposed to exposing the face to cold wind, which is more representative of the type of situation most people would find themselves in while working or pursuing leisure activities outdoors. Gavhed et al. (2000) and Steegmann (1972) did examine the effect of cold wind exposure on facial CIVD response. Gavhed et al.’s (2000) study did not go into any great depth with regard to a presentation and analysis of CIVD data (only nose skin temperature during exposure to −10°C and 5 m/s wind was provided). Steegmann (1972) did present data on how often CIVDs were observed for different regions of the face, the number of CIVD waves, and the temperature of the skin, but the data was only based on an exposure to 0°C and a 3 m/s wind.
One objective of this study is to characterize the facial temperature and CIVD response of subjects exposed to cold wind over a wider range of ambient conditions (i.e., −10 to 10°C; 2–8 m/s wind speed) relative to past studies.
Another objective is to examine the effect of the thermal state of the body (as reflected by core temperature) in relation to facial skin temperature response. The tips of the fingers are the first region of the hand to cool down in response to body cooling, and they are the first to re-warm in response to active body heating (Rapaport et al. 1949). Therefore, much like the sensitivity of the fingers to changes in the thermal state of the body (Daanen et al. 1997; Daanen and Ducharme 1999), it is hypothesized that the acral regions of the face, such as the nose, are also more sensitive to changes in the thermal state of the body, and hence will stay warmer relative to other parts of the face during exercise in the cold.
Methods
Subjects
Six male and six female healthy, non-smoking volunteers with the following characteristics were recruited (mean ± S.D.): age 33±8 years, height 174±9 cm, weight 76±16 kg, body surface area 1.89±0.22 m2, and body fat of 20±4%. Body surface area was estimated using the formula of Dubois and Dubois (1916). Percentage body fat was estimated from skin-fold measurements on five body sites (triceps, scapula, suprailiac, abdomen, and front thigh) and calculated according to Forsyth et al. (1984). All subjects were medically screened by a physician at Defence Research and Development Canada—Toronto (DRDC Toronto) before being asked for their written consent. The study was approved by the Human Research Ethics Committee at DRDC Toronto.
Experimental protocol
Subjects walked comfortably (4.8 km/h) on a treadmill during exposure to four 90-min tests, each at a different environmental condition (10°C dry, 10°C wet, 0°C, and −10°C) on four separate occasions held 1 week apart. The ambient conditions were given in balanced order to avoid any ordering effect. During the 10°C wet condition, a fine mist of cold water (5°C) was sprayed from a distance of 1 m on the subject’s face every 15 s for 1 s duration. The mist was controlled by a solenoid valve (Model Red-Hat II 8210G2, Ascolectric Ltd., Brantford, ON, Canada). During each test, the wind speed was set at 2 m/s from time 0 to 30 min, 5 m/s from time 30 to 60 min, and 8 m/s after 60 to 90 min. As the subjects walked on a treadmill, they faced directly into the wind. It should be noted that subjects were always exposed to a 2 m/s wind, followed by 5 m/s wind and 8 m/s wind (in that order). That is, the wind speeds were not balanced over the experimental conditions. However, this does not negate the validity of the CIVD and facial skin temperature results at the 5 and 8 m/s wind speeds (see Discussion for more details).
Another experiment was done to examine the effect of the thermal state of the body (as reflected by core temperature) on facial skin temperatures. This was done by comparing facial skin temperature responses in exercising and resting subjects during exposures to −10 and 0°C air. More specifically, mean facial skin temperature (based on average chin, cheek, and forehead skin temperatures) and nose tip skin temperature were compared in exercising (walking on a treadmill at 4.8 km/h) and resting (sitting in a chair) subjects. The mean facial and nose skin temperatures compared between groups were based on steady-state temperatures observed in last 10 min of each condition, with each condition lasting 60 min. The exercising group participated in 60 min of exercise in the cold (time 0–30 min with a 2 m/s wind, followed by time 30–60 min with a 5 m/s wind), whereas the resting group sat for 60 min [outside the cold chamber at 22°C (no wind) from time 0 to 30 min, followed by sitting in the cold with a 4.5 m/s wind from time 30 to 60 min]. Subjects faced directly into the wind at all times. No data was collected from time 0 to 30 min, but data was collected from time 30 to 60 min. In addition, rectal temperature was measured 5 min prior to each 60-min experimental session to establish a baseline reading (time −5 to 0 min on Fig. 9). The clothing worn inside the cold chamber at each ambient temperature is described under the heading “Clothing worn.”
The exercising group consisted of 12 subjects (six male and six females) with the following characteristics (mean±SD): age 33±8 years, height 174±9 cm, weight 76±16 kg, body surface area 1.89±0.22 m2, and body fat of 20±4%. The resting group consisted of nine subjects (seven males and two females) with the following characteristics (mean±SD): age 34±6 years, height 177±6 cm, weight 81±15 kg, body surface area 1.97±0.20 m2, and percent body fat of 17±4.
There was a significant difference (P<0.05) between the 4.5±0.2 and 5.0±0.2 m/s wind speed measured during the exercising and resting conditions, respectively. However, a comparison was still made between the two data sets.
Clothing worn
The clothing worn by the subjects varied with each ambient temperature. During exposure to 10°C dry and 10°C wet, subjects wore a pair of uninsulated ski pants, wool socks, and hiking boots for the lower-half of the body, and for the upper body, the following insulation was worn: a long, tight-fitting, cotton, honeycomb shirt; a thin, wind-resistant nylon shell; an acrylic ski hat (if requested by the subject), and a thin pair of gloves (if requested by the subject). The objective in all ambient environments was to allow the subject to add or remove articles of clothing as they saw fit, in order to maintain body comfort. Subjects were asked to adjust clothing requirements if they reported a value below 6 (cool, but fairly comfortable) or above 8 (warm, but fairly comfortable) on the McGinnis 13-point thermal comfort scale (Hollies and Goldman 1977), where 7 is the rating for “comfortable.” For each ambient temperature, body-subjective comfort data was collected using the thermal comfort scale at time 2, 15, and 27 min of each 30-min session at 2, 5, and 8 m/s wind speed. Maintaining body comfort is important because even though the CIVD response serves as protective mechanism by decreasing the chances of cold injury, this protective physiological response is affected by body heat content (Goldman 1980; Daanen et al. 1997). However, it should be noted that thermal comfort measurements in the present study were not used to evaluate body heat content, but rather, thermal comfort was used as a tool to assess general subjective comfort, in an attempt to prevent the subject from shivering or sweating.
Differences in body heat content were established by creating two experimental conditions (exercising versus resting group) in which there was a significant difference in rectal temperature after 30 min of exercise. Body heat content was not directly measured, but significant differences in rectal temperature were used as an indication that body heat content was different between groups. During exposure to 0°C, the clothing worn was identical to the 10°C condition, except that a pair of long, tight-fitting, cotton, honeycomb underwear was also worn under the uninsulated ski pants, a fleece top was worn over the honeycomb shirt, Arctic mitts were worn over the hands instead of thin gloves, and a dickey insulated the neck.
During exposure to −10°C, the clothing worn was identical to the 0°C condition, except that instead of a pair of honeycomb underwear under the uninsulated ski pants, a pair of fleece pants were worn underneath the uninsulated ski pants. In addition, the thin, wind-resistant nylon shell was replaced with a thicker uninsulated jacket.
Selection of ambient temperature
Fox and Wyatt (1962) suggested that if local cooling is severe, local freezing may occur before CIVD vasodilation has had time to develop, even when the body is warm. Therefore, since the goal of the study was to characterize the CIVD response during exposure to cold wind, past studies were examined to determine the appropriate lower ambient temperature that would elicit a CIVD response, yet still minimize the risk of frostbite.
Wilson and Goldman (1970) found that there is a small risk for finger freezing when the ambient temperature is −10°C or above (even at high wind speeds), but at −15°C or below the risk increases substantially with increasing wind speeds. In a paper by Danielsson (1996), previously unpublished data of Wilson and Goldman (1970) was reported, which indicated that observed frostbite frequency in the fingers was 63% when the ambient temperature was −11.5°C with a 10 m/s wind, whereas the frostbite frequency was 0% during exposure to −9.5°C with a 10 m/s wind. Finally, studies on occupational cold injuries have shown that temperatures below −10°C significantly increased the chances of frostbite as wind temperature exceeded 4.5 m/s (Brahdy 1935; Sinks et al. 1987). Therefore, based on all these past studies, we made the assumption that a lower ambient limit of −10°C would meet our goals. The lower limit was established based on studies that examined the extremities because of the limited information available for the development of facial frostbite.
With regard to establishing an upper ambient temperature, Steegmann (1979) observed CIVD at all regions of the face (nose, cheek, chin, forehead) during a 70-min exposure to 0°C and a 3 m/s wind. But there was no facial CIVD data during exposures to an ambient greater than 0°C. In the present study, it was of interest to determine the environmental conditions at which CIVDs are first observed. It was hypothesized that at an ambient temperature of 10°C (with no wind), very little, if any, CIVD response would be observed.
Therefore, based on this information, the ambient conditions for the present experiment ranged between −10 and 10°C.
Physiological variables measured
During the experimental trials skin temperatures of the nose, cheek, chin, and forehead were measured using fine, insulated thermocouples (Model 5SC, Type T, Omega Engineering Inc., Laval. QC, Canada) made from 40-gauge wire. The tip of the thermocouples were bare. A 40-gauge wire was chosen to minimize response time by keeping the thermal mass low. The thermocouple on the nose was placed 1 cm proximally from the tip of the nose. The thermocouple on the cheek was placed in the middle of the right cheek, defined as the middle of the triangular area formed by an imaginary line joining the top of the cheekbone, the corner of the mouth, and the proximal portion of the mandible. The chin thermocouple was placed on the most prominent part of the chin, and the thermocouple on the forehead was placed 1–2 cm above the right eyebrow in-line with the middle of the eye. Mean facial skin temperature was measured by averaging the nose, cheek, chin, and forehead skin temperatures for the last 10 min of each 30-min session for each wind speed (i.e., at time 20–30, 50–60, and 80–90 min). In the present study, the ears were not included, even though they are most susceptible to frostbite (Steegmann 1967, 1979; Lehmuskallio 2000), because the ears are easy to protect from the cold by wearing a hat, whereas many individuals do not wear a balaclava or scarf to cover the face. Therefore, the focus of the present study was to only examine the CIVD response of the face.
A piece of surgical tape (Blenderm, 3M Health Care, St. Paul, MN, USA) was used to hold the sensors on the face. The thermocouple wire was covered with tape for a distance of 3 cm to help minimize the effect of the ambient air on the reading. The skin temperature data was collected every 5 s using a data acquisition system (model 3497A data acquisition/control unit; Hewlett Packard). Rectal temperature (T re) was measured via a thermistor (Pharmaseal 400 series, Baxter, Valencia, CA, USA) inserted 15 cm beyond the anal sphincter.
Criteria for termination of session inside cold chamber
The experiment was terminated if: (1) the subject requested to stop, (2) the investigator or physician stopped the experiment for safety reasons, (3) any facial skin temperature reached 0°C, or (4) the 90-min exposure period elapsed.
CIVD parameters
In the present study, a CIVD response was defined as a minimum 1°C change in skin temperature within a maximum time span of 10 min when the absolute skin temperature was 15°C or lower. Hirai et al. (1970) found no CIVD response when the fingers were immersed in 15°C water. Finger skin temperature will cool to within a degree of the water temperature (except when there is a CIVD response) and therefore using an upper CIVD skin temperature limit of 15°C was supported by Hirai et al.’s (1970) finding. There is a well-established direct relationship between blood flow and skin temperature (Daanen and Ducharme 2000) and skin temperature is the most commonly used measure of CIVD (Daanen 2003). Therefore, in the present study, the facial CIVD response was inferred from changes in skin temperature. The CIVD parameters measured in examining facial CIVD response are explained next.
-
CIVD onset time: the time from the start of exposure to the cold (time 0 min) to start of the CIVD phase.
-
CIVD peak time: the time from the start of the CIVD phase to the maximum facial skin temperature value reached in the CIVD phase.
-
CIVD amplitude: the change in temperature from the start of the CIVD phase to the maximum facial skin temperature value reached in the CIVD phase.
-
Minimum temperature: the minimum facial skin temperature observed during the CIVD phase.
-
Maximum temperature: the maximum facial skin temperature observed during the CIVD phase.
The nose was not included in examining the CIVD response because the high temperatures (above the mentioned threshold) maintained on the nose excluded it from being considered a CIVD (see Results section for details).
Statistical analyses
An one-way ANOVA for repeated measures was used to compare the four ambient conditions (10°C dry, 10°C wet, 0°C, −10°C) for each wind speed (2, 5, 8 m/s) in examining mean facial temperature for all 12 subjects. Results were considered statistically significant at P≤0.05 (using the Greenhouse–Geisser adjustment for repeated measures). A Newman-Keuls post hoc test was used to determine if there was a significant difference between ambient conditions for each wind speed. An unpaired Student’s t test was done to compare nose skin temperature during sitting (n=9) and walking (n=12) during exposure to 0°C and −10°C. An unpaired Student’s t test was also used to compare mean facial skin temperature (average of cheeks, forehead, and chin) during sitting and walking. All values are presented as mean ± SE. Statistical analyses was not done for the CIVD parameters because CIVD occurred very infrequently or did not occur at all in some conditions and therefore the results were only presented using descriptive statistics.
Results
Mean facial temperature
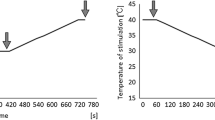
Mean facial temperature was based on the average skin temperatures of the forehead, cheek, nose, and chin for each ambient temperature during the last 10 min of each 30-min exposure at a wind speed of 2, 5, and 8 m/s. Using cheek skin temperature as an example, Fig. 1 shows the typical steady-state temperatures achieved at times 20–30 min, 50–60 min, and 80–90 min. At each wind speed, the mean facial temperature increased as the ambient temperature increased (see Fig. 2). Wetting the skin during the 10°C exposure significantly decreased the mean facial temperature. It is interesting to note that at each wind speed, the facial skin temperature during the 10°C wet condition was less than or equal to the facial skin observed during the 0°C condition.

Cheek skin temperature for each 30 min exposure at a wind speed of 2, 5, and 8 m/s, respectively, during exposures to the 10°C dry, 10°C wet, 0°C, and −10°C ambient air. Mean facial skin temperature (see Fig. 2) was based on the steady state skin temperatures measured in the last 10 min of each 30 min exposure. Figure 1 shows the typical steady state conditions achieved at times 20–30, 50–60, and 80–90 min. The values graphed are the mean ± SE for 12 subjects

Mean facial temperature based on the average skin temperatures of the forehead, cheek, nose, and chin for each ambient temperature during the last 10 min of each 30 min exposure at a wind speed of 2, 5, and 8 m/s. The values graphed are the mean±se for 12 subjects. Single Asterisk indicates a significant increase in mean facial temperature relative to that observed at an ambient temperature of −10°C. Double Asterisk indicates a significant increase in mean facial temperature relative to that observed at an ambient temperature of 0°C
During the 2-m/s wind exposure, the facial skin temperatures for the −10, 0, 10°C wet, and 10°C dry conditions were: 15.2±0.5, 19.5±0.6, 17.0±0.4, and 23.7±0.4°C, respectively.
During the 5-m/s wind exposure, the facial skin temperatures were: 11.8±0.4, 15.4±0.8, 14.4±0.4, and 20.8±0.4°C, respectively.
During the 8-m/s wind exposure, the facial skin temperatures were: 11.2±0.5, 14.4±0.7, 14.3±0.3°C, and 20.0±0.5°C, respectively.
Overall percent of subjects showing CIVD response
At each wind speed, the percentage of subjects showing a facial CIVD response decreased significantly as the ambient temperature increased (see Fig. 3). The CIVD response during the 10°C wet condition was similar to the CIVD response during the 0°C ambient condition. There was a noticeable increase in the CIVD response from the 0°C to the −10°C condition during all wind speeds.

Percentage of subjects showing facial CIVD at each ambient temperature/wind speed combination. A total of 12 subjects participated in each condition
During the 2-m/s wind exposure, the percentage of subjects showing a CIVD response (based on 12 subjects) was 42, 8, 8, and 0% during exposures to the −10, 0, 10°C wet, and 10°C dry conditions, respectively.
During the 5-m/s wind exposure, the percentage of subjects showing a CIVD response (based on 12 subjects) was 83, 33, 25, and 0%, respectively.
During the 8-m/s wind exposure, the percentage of subjects showing a CIVD response (based on 12 subjects) was 100, 33, 33, and 0%, respectively.
Percentage of subjects showing CIVD response at individual facial sites
During the 2-m/s wind exposure, the CIVD occurred mainly during the −10°C ambient condition and was observed more often on the cheek and chin, rather than on the forehead (see Fig. 4). During the 5-m/s wind exposure, CIVDs were observed on the forehead during the −10 and 10°C wet conditions, although CIVDs at the cheek and chin were more readily observed than at the forehead during exposure to −10°C air. During the 8 m/s wind exposure, CIVDs were generally observed more often on the cheek and chin, except during the −10°C condition when the CIVD occurrence on the face was more uniform between the three sites.

Percentage of subjects showing facial CIVD at each ambient temperature/wind speed combination for each of the individual facial sites. A total of 12 subjects participated in each condition
Amplitude of CIVD response at individual facial sites
During all wind exposures, the CIVD amplitude was generally between 2 and 4°C at all three facial sites, except during the −10°C condition (5 and 8 m/s wind conditions) when the CIVD amplitude was between 5 and 8°C at the cheek and/or chin (see Fig. 5).

CIVD amplitude (Mean ± SE) during each ambient temperature/wind speed combination for each of the individual facial sites. For each facial location and wind speed combination, there are a series of four numbers. The four numbers represent the number of subjects showing a CIVD response during exposures to −10, 0, 10°C wet, and 10°C dry ambient air, respectively
Minimum and maximum CIVD facial temperatures
During the 2-m/s wind exposure, the minimum and maximum CIVD temperatures ranged between 10 and 18°C for the −10, 0 and 10°C wet conditions (see Fig. 6). During the 5 and 8 m/s wind exposures, the minimum and maximum CIVD temperatures ranged between 7 and 15°C and 5 and 14°C, respectively, for the −10, 0 and 10°C wet conditions.

Mean minimum and maximum CIVD facial temperatures (Mean ± SE; based on average of cheek, chin, and forehead) at each ambient temperature/wind speed combination. For each facial location and wind speed combination, there are a series of four numbers. The four numbers represent the number of subjects showing a CIVD response during exposures to −10, 0, 10°C wet, and 10°C dry ambient air, respectively
CIVD onset time
During the 2-m/s wind exposure, the CIVD onset times during the −10, 0, and 10°C wet conditions were 18.0±2.7, 28.0, and 23.0 min (see Fig. 7). No CIVDs were observed during the 10°C dry condition, regardless of the wind speed.

CIVD onset time (Mean ± SE) for each ambient temperature/wind speed combination. Onset time is the time it takes for the first CIVD to be observed. For each facial location and wind speed combination, there are a series of four numbers. The four numbers represent the number of subjects showing a CIVD response during exposures to −10, 0, 10°C wet, and 10°C dry ambient air, respectively
During the 5-m/s wind exposure, the CIVD onset times during the −10, 0, and 10°C wet conditions were 7.9±1.5, 8.2±1.4, and 8.7±2.2 min.
During the 8-m/s wind exposure, the CIVD onset times during the −10, 0, and 10°C wet conditions were 6.8±0.8, 5.4±1.2, and 3.9±0.9 min.
CIVD peak time
During the 2-m/s wind exposure, the CIVD peak times during the −10, 0, and 10°C wet conditions were 2.9±0.7, 2.0, and 1.0 min (see Fig. 8). No CIVDs were observed during the 10°C dry condition, regardless of the wind speed.

CIVD peak time (Mean ± SE) for each ambient temperature/wind speed combination. Peak time is the time required to reach the maximum CIVD value once a CIVD is initiated. For each facial location and wind speed combination, there are a series of four numbers. The four numbers represent the number of subjects showing a CIVD response during exposures to −10, 0, 10°C wet, and 10°C dry ambient air, respectively
During the 5-m/s wind exposure, the CIVD peak times during the −10, 0, and 10°C wet conditions were 3.7±0.3, 4.3±0.6, and 2.8±0.8 min.
During the 8-m/s wind exposure, the CIVD peak times during the −10, 0, and 10°C wet conditions were 5.1±0.4, 6.3±1.8, and 5.6±0.6 min.
Rectal temperature
Rectal temperature was compared during time 30–60 min in the exercising and resting subjects during exposure to −10 and 0°C air (see Fig. 9a, b). There was no significant difference in baseline rectal temperature (time −5–0 min) between the exercising and resting groups at the start of each 60-min exposure. During the −10°C exposure, rectal temperature from time −5 to 0 min exposure was 37.31±0.03 and 37.07±0.11°C for the exercising and resting groups, respectively, whereas during the 0°C exposure, rectal temperature was 37.32±0.04 and 36.99±0.08°C for the exercising and resting groups, respectively. Time 0–30 min was used to establish a core temperature difference between the exercising and resting groups by time 30 min, however no data was collected during this time. The rectal temperature was significantly greater in the exercising group from time 30 to 60 min.

Rectal temperature (Mean ± SE) in exercising (walking on a treadmill at 4.8 km/h) and resting (sitting in a chair) subjects during exposure to −10°C (a) and 0°C (b) air. Baseline rectal temperatures (time −5 to 0 min) for the exercising and resting groups were obtained prior to the start of each 60 min exposure. Time 0–30 min was used to establish a core temperature difference between the exercising and resting groups by time 30 min, however no data was collected during this time. The rectal temperature was significantly greater in the exercising group from time 30 to 60 min
During exposure to −10°C air, rectal temperature in the resting group was stable at 36.97±0.12°C during time 30–60 min, whereas during the same time, it increased significantly from 37.79 ±0.03 to 37.93±0.05°C in the exercising group. During exposure to 0°C air, rectal temperature in the resting group was stable at 36.93±0.08°C during time 30–60 min, whereas during the same time, it increased significantly from 37.74 ±0.04 to 37.90 ±0.04°C in the exercising group.
Nose and facial skin temperatures
At an ambient temperature of −10 and 0°C, nose skin temperature was significantly higher during exercise compared with nose skin temperature at rest (see Fig. 10a). During −10°C, nose skin temperature was 9.7±1.0 and 18.1±1.5°C during rest and exercise, respectively. During 0°C, nose skin temperature was 12.3±0.6 and 21.1±1.9°C during rest and exercise, respectively.

a Steady state nose tip skin temperature (Mean ± SE) in exercising (walking on a treadmill at 4.8 km/h) and resting (sitting in a chair) subjects during exposure to −10 and 0°C air. The steady state temperatures were based on last 10 min of each 60 min exposure. The exercising group participated in 60 min of exercise in the cold (time 0–30 min with a 2 m/s wind, followed by time 30–60 min with a 5 m/s wind), whereas the resting group sat for 60 min (outside the cold chamber at 22°C (no wind) from time 0 to 30 min, followed by sitting in the cold with a 4.5 m/s wind from time 30 to 60 min). Subjects faced directly into the wind at all times. Asterisk represents a significant (P<0.05) difference between conditions. b Steady state mean facial skin temperature (based on average of chin, cheek, and forehead temperatures; Mean ± SE) in exercising (walking on a treadmill at 4.8 km/h) and resting (sitting in a chair) subjects during exposure to −10 and 0°C air. The exercise conditions described in (a), also apply to (b). The steady state temperatures were based on last 10 min of each cold exposure. There was no significant difference (P≥0.05) between the exercising and resting conditions for both ambient conditions
Mean facial temperature did not show any significant differences between the exercise and resting conditions at both ambient temperatures (see Fig. 10b). During −10°C, mean facial skin temperature was 9.0±0.8 and 10.3±0.6°C during rest and exercise, respectively. During 0°C, mean facial temperature was 12.4±0.6 and 13.8±1.7°C during rest and exercise.
Discussion
At a given wind speed, CIVD in the face was observed with an ambient air temperature as warm as 10°C when the skin was wet, but it was more common to see a response during exposure to −10°C air. It is interesting to observe that the percentage of subjects showing a facial CIVD response was similar between the 10°C wet and 0°C condition at all wind speeds. This illustrates the effect of evaporative cooling on the CIVD response.
CIVD response of different regions of the face
The incidence of CIVD response is quite uniform across facial sites, once the cold stress is severe enough (i.e., −10°C and 8 m/s wind). This would make sense when one considers that at an ambient temperature between −10 and −15°C, the likelihood of frostbite increases dramatically (at least in fingers) when there is a wind (5–15 m/s) (Wilson and Goldman 1970). That is, if the CIVD response is a physiological mechanism that protects the skin from cold injury, then one can expect the CIVD response to be most prevalent for ambient conditions presenting some risk of cold injuries [i.e., based on Wilson and Goldman’s (1970) finger temperature data, for conditions ≤ −10 to −15°C with wind speed 5–15 m/s]. However, more research is needed to determine whether the ambient temperature and wind speed at which frostbite and CIVD are likely to occur in the fingers also apply to the skin of the face.
The nose was not included in the comparison of CIVD responses for different regions of the face because its temperature ranged between 16 and 26°C during the cold exposures from −10 to 10°C. The exclusion of the nose in the comparisons was based the establishment of an upper CIVD skin temperature limit of ≤15°C based on the work of Hirai et al. (1970) (see Methods for details).
One possible explanation for the differences in the CIVD response observed between facial sites, at a given wind speed, may be due to a difference in subcutaneous fat between sites. LeBlanc et al. (1976) suggested that the forehead cools less because it is well vascularized and has a uniform surface with a thin layer of subcutaneous fat. LeBlanc (1954) found that the skin temperature on the face is lower in locations where subcutaneous fat is more abundant. Fat acts as an insulator that limits heat transfer from the deep tissues to the skin.
Another possible explanation for the observed differences in CIVD response between facial sites, at a given wind speed, is that despite the fact that subjects sat in a cold chamber with laminar wind flow, the flow over the certain regions of the face may have been turbulent due to wind deflection at the protruding points of the face. Fox and Wyatt (1962) found a similar CIVD response in comparing the cheek, forehead, and nose, which may be explained by the different methodology they used to elicit the CIVD response. That is, they locally cooled each region of the face using an “ice candle” without wind exposure, and therefore local cooling was more identical between sites.
Effect of thermal state of body on facial skin temperature
Steegmann (1979) did a field study in which he compared the nose temperatures of two groups of subjects exposed to cold air. One group of ten soldiers was exposed to −24.5°C air (no wind) while at a camp, not exercising (control group) while another group of 24 soldiers was exposed to −21°C air (no wind) and exercised (by marching or snowshoeing for several miles). Despite the air movement caused by marching, nose temperature was higher in the exercising group compared with the control group. He suggested that the increased nose temperature was a result of a higher volume of blood flow through the open facial vascular beds and that exercise may enhance frostbite resistance. Steegmann (1979), however, did not measure core temperature, whereas in the present study, core temperature was measured (see Fig. 9). In addition, this paper not only examined the effects of exercise on nose temperature, but it also compared mean facial temperatures (in regions other than the nose) in resting and exercising subjects, all of which was done in a more controlled environment relative to Steegmann’s study.
The present study found that nose skin temperature was significantly higher in exercising subjects when compared with resting subjects (see Fig. 10a), even though there was no significant difference in face temperature (excluding the nose) between conditions (see Fig. 10b). This finding supports our hypothesis that the acral regions of the face, such as the nose, are more sensitive to changes in the thermal state of the body, and hence will stay warmer relative to other parts of the face during exercise in the cold. However, there is the possibility that the increased ventilation due to exercise may have affected the expired air temperature and caused an increase in nose skin temperature. More research will be required to determine whether our finding may be extended to subjects with a higher heat content caused by passive heating.
Gavhed et al. (2000) found that the nose was cooler relative to other regions of the face and they suggested that the differences observed may be explained by the greater surface-to-mass ratio of the nose. In the present study, subjects were also exposed to −10°C air with similar wind intensities, but nose temperature was the warmest site, not the coldest site. However, unlike Gavhed’s study, subjects in the present study were performing exercise. The arteriovenous anastomoses (AVAs) in the nose most likely opened up in response to an increase in body heat content that resulted from exercising. Past studies have shown that a local cold stress acting on the fingers and toes can be overcome if sufficient heat is generated by the body from exercise (Wyndham and Wilson-Dickson 1951; Rintamaki et al. 1992) or by actively heating the body using auxiliary heat (Brajkovic et al. 1998; Brajkovic et al. 2001).
During cold exposure at rest, the tip of the nose cools more quickly as supported by the study of Gavhed et al. (2000), but the present study provides evidence that the nose is also the first region of the face to re-warm during exercise in the cold. Therefore, even though it is known that sympathetic activity increases with exercise, which is reflected in skin vasoconstriction in areas with AVAs such as the nose (Seals and Victor 1991); as body heat content increases, the same vasoconstricted areas will become vasodilated (Wyndham and Wilson-Dickson 1951). Hence, the local effects of the cold and exercise on peripheral vasoconstriction in the extremities can be overcome, provided that there is not only sufficient metabolic heat generated by the exercise, but that the length of the exercise session is long enough so that there is net positive heat storage (Wyndham and Wilson-Dickson 1951; Brajkovic and Ducharme 2001, 2003).
With regard to this comment that the AVAs in the nose most likely opened up in response to an increase in body heat content, it should be noted that that AVAs are not present in all locations where the CIVD response has been found to occur on the head (Lewis 1930; Fox and Wyatt 1962). Bergersen (1993), for example, found that AVAs are not present in the skin of the forehead, whereas they are present in the nose. This would explain why the nose skin temperature would increase before the forehead skin temperature, in response to an increase in body heat content.
A possible link between the presence of AVAs and differences in facial temperature response between facial sites may also be supported by the findings of Makinen et al. (2001). They did an experiment, which examined forehead skin temperature response in individuals exercising at two different metabolic rates during exposure to −10°C air (wind of 0.1, 1, and 5 m/s). They found that forehead skin temperature was not significantly different at the higher exercise intensity relative to the lower intensity for each wind condition, even though rectal temperature was significantly different between exercise intensities. But, they did find a significant difference in finger skin temperature between the two exercise intensities. This suggests that the forehead skin temperature is not as sensitive as finger skin temperature to changes in body heat content, and likely not as sensitive as nose temperature as suggested by the present study.
Effect of pre-cooling the skin on absolute facial skin temperature
Makinen et al. (2000) found that pre-cooling the body and face had no effect on the final skin temperature of the face observed during a 30-min exposure to −10°C air (at 0.2, 1, and 5 m/s wind) relative to a condition in which the body and face were kept thermoneutral prior to the 30-min cold exposure. Makinen et al. (2000) stated that the differences caused by pre-cooling disappeared within the first few minutes of exposure to cold wind. Therefore, this study found that the initial face temperature did not have any significant effect (i.e., is not a confounding factor) on the overall face temperature during the cold exposure, if the first few minutes of data were excluded. For this reason, the facial skin temperatures reported in the present study were based on steady-state values (i.e., the last 10 min of each 60-min exposure), to minimize any possible effect of a difference in initial facial skin temperature between the exercising and resting groups. Despite the evidence provided by Makinen et al.’s (2000) results and the precautions taken in the present study, one might hypothesize that the facial skin temperatures observed in the exercising group may have been warmer, if those subjects had been exposed to a 30-min thermoneutral exposure prior to 30 min inside the cold chamber, instead of being in the cold chamber for the entire 60-min session. If this was the case, then the difference observed between the exercising and resting subjects would have been greater than observed. In other words, if one accepts this hypothesis, our results would be conservative. The same reasoning applies to the CIVD data. At wind speeds of 5 and 8 m/s, the CIVD data presented may be considered conservative, relative to a condition in which no facial pre-cooling had taken place prior to being exposed to each of these two wind speeds.
It should be noted that the study of Makinen et al. (2000) only exposed subjects to a −10°C ambient environment, therefore conclusions about the effect of precooling on the facial skin temperatures and CIVD responses for the 0 and 10°C ambient temperatures used in the current study are speculative. However, since the other precooling ambient temperatures (0 and 10°C) were milder, the effect of precooling should be less compared with the −10°C condition.
Conclusion
One objective of this study was to characterize the facial temperature and CIVD response of subjects exposed to cold wind over a wider range of ambient conditions (i.e., −10 to 10°C; 2, 5, and 8 m/s wind speed) relative to past studies. This study found that for each wind speed, face temperature increased as the ambient temperature increased. Wetting the skin during the 10°C exposure significantly decreased the mean facial skin temperature to a value similar to the facial skin temperature observed during the 0°C condition. In addition, at each wind speed, the percentage of subjects showing a facial CIVD response decreased significantly as the ambient temperature increased. The incidence of CIVD response was more uniform across facial sites when there was a greater cold stress (i.e., −10°C and 8 m/s wind).
Another objective of the study was to examine the effect of the thermal state of the body (as reflected by core temperature) in relation to facial skin temperature response. This study found that nose skin temperature was significantly higher in exercising subjects when compared to resting subjects, even though there was no significant difference in face temperature (excluding the nose) between conditions. Therefore, this finding suggests that acral regions of the face, such as the nose, are more sensitive to changes in the thermal state of the body, and hence will stay warmer relative to other parts of the face during exercise in the cold.
References
Bergersen TK (1993) A search for arteriovenous anastomoses in human skin using ultrasound Doppler. Acta Physiol Scand 147(2):195–201
Brahdy L (1935) Frostbites among employees of the city of New York. JAMA pp 529–532
Brajkovic D and Ducharme MB (2001). Maintaining finger dexterity in the cold: a comparison of passive, direct and indirect hand heating methods. In: NATO human factors and medicine panel symposium on blowing hot and cold: protecting against climatic extremes, Dresden, Germany, October 8–10 proceedings RTO-MP-076 AC/323 (HFM-061) TP/40, p 20
Brajkovic D, Ducharme MB (2003) Finger dexterity, skin temperature, and blood flow during auxiliary heating in the cold. J Appl Physiol 95:758–770
Brajkovic D, Ducharme MB, Frim J (1998) Influence of localized auxiliary heating on hand comfort during cold exposure. J Appl Physiol 85(6):2054–2065
Brajkovic D, Ducharme MB, Frim J (2001) Relationship between body heat content and finger temperature during cold exposure. J Appl Physiol 90(6):2445–2452
Daanen HA (2003) Finger cold-induced vasodilation: a review. Eur J Appl Physiol 89(5):411–426
Daanen HA, Ducharme MB (1999) Finger cold-induced vasodilation during mild hypothermia, hyperthermia and at thermoneutrality. Aviat Space Environ Med 70(12):1206–1210
Daanen HA, Ducharme MB (2000) Axon reflexes in human cold exposed fingers. Eur J Appl Physiol 81(3):240–244
Daanen HA, Van de Linde FJ, Romet TT, Ducharme MB (1997) The effect of body temperature on the hunting response of the middle finger skin temperature. Eur J Appl Physiol Occup Physiol 76(6):538–543
Danielsson U (1996) Windchill and the risk of tissue freezing. J Appl Physiol 81(6):2666–2673
DuBois D, DuBois EF (1916) A formula to estimate the approximate surface area if height and weight be known. Arch Inter Med 17:863–871
Forsyth RD, Plyley MJ, Shephard RJ (1984) Estimation of body fatness of Canadian Forces. Can J Appl Sport Sci 9(4):5
Fox RH, Wyatt HT (1962) Cold-induced vasodilatation in various areas of the body surface of man. J Physiol 162:289–297
Gavhed D, Makinen T, Holmer I, Rintamaki H (2000) Face temperature and cardiorespiratory responses to wind in thermoneutral and cool subjects exposed to −10°C. Eur J Appl Physiol 83(4–5):449–456
Goldman RF (1980) Protection against cold injury. Contemp Orthop 2(3):263–266
Hirai K, Horvath SM, Weinstein V (1970) Differences in the vascular hunting reaction between Caucasians and Japanese. Angiology 21(8):502–510
Hollies NRS, Goldman RF (1977) Psychological scaling in comfort assessment. Clothing comfort: interaction of thermal, ventilation, construction, and assessment factors. Ann Arbor Science Publishers Inc., Ann Arbor, pp 107–120
LeBlanc J (1954) Subcutaneous fat and skin temperature. Can J Biochem Physiol 32:354–358
LeBlanc J, Blais B, Barabe B, Cote J (1976) Effects of temperature and wind on facial temperature, heart rate, and sensation. J Appl Physiol 40(2):127–131
Lehmuskallio E (2000) Emollients in the prevention of frostbite. Int J Circumpolar Health 59(2):122–130
Lewis T (1930) Observations upon the reactions of the vessels of the human skin to cold. Heart 15:177–208
Makinen T, Gavhed D, Holmer I, Rintamaki H (2000) Thermal responses to cold wind of thermoneutral and cooled subjects. Eur J Appl Physiol 81(5):397–402
Makinen TT, Gavhed D, Holmer I, Rintamaki H (2001) Effects of metabolic rate on thermal responses at different air velocities in −10°C. Comp Biochem Physiol A Mol Integr Physiol 128(4):759–768
Rapaport SI, Fetcher ES, Shaub HG, Hall JF (1949) Control of blood flow to the extremities at low ambient temperatures. J Appl Physiol 2:61–71
Rintamaki H, Hassi J, Oksa J, Makinen T (1992) Rewarming of feet by lower and upper body exercise. Eur J Appl Physiol Occup Physiol 65(5):427–432
Seals DR, Victor RG (1991) Regulation of muscle sympathetic nerve activity during exercise in humans. Exer Sport Sci Rev 19:313–349
Sinks T, Mathias T, Halperin W, Timbrook C, Newman S (1987) Survaillance of work-related cold injuries using workers’ compensation claims. J Occup Med 26(6):504–509
Siple PA, Passel CF (1945) Measurements of dry atmospheric cooling in subfreezing temperatures. Proc Am Philos Soc 89(1):177–199
Steegmann AT (1967) Frostbite of the human face as a selective force. Human Biol 39(2):131–144
Steegmann AT (1972) Cold response, body form, and craniofacial shape in two racial groups of Hawaii. Am J Phys Anthrop 37:193–222
Steegmann AT Jr (1979) Human facial temperatures in natural and laboratory cold. Aviat Space Environ Med 50(3):227–232
Virokannas H, Anttonen H (1994) Thermal responses in the body during snowmobile driving. Arctic Med Res 53(Suppl 3):12–18
Wilson O, Goldman RF (1970) Role of air temperature and wind in the time necessary for a finger to freeze. J Appl Physiol 29(5):658–664
Wyndham CH, Wilson-Dickson WG (1951) Physiological responses of hands and feet to cold in relation to body temperature. J Appl Physiol 4:199–207
Acknowledgements
We acknowledge the technical support of Robert Limmer and Debbie Kerrigan-Brown.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Brajkovic, D., Ducharme, M.B. Facial cold-induced vasodilation and skin temperature during exposure to cold wind. Eur J Appl Physiol 96, 711–721 (2006). https://doi.org/10.1007/s00421-005-0115-3
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00421-005-0115-3