
Abstract
Velocity at VO2 max (vV̇O2 max) and peak treadmill velocity (PTV) are variables highly predictive of endurance performance. However, how these variables are affected by the menstrual cycle is unknown. The aim of this study was to assess the effect of the menstrual cycle on vV̇O2 max and PTV. Ten, female runners were studied across three menstrual cycles. Training, menstrual history and mood states were assessed for 2 months, with daily salivary samples taken to detect menstrual phases. During the third menstrual cycle, participants completed a maximal test to determine V̇O2 max, vV̇O2 max and PTV in the early follicular phase, late follicular phase, early luteal phase, late luteal phase and menses. Progesterone increased at the onset of the luteal phase [mean (SEM); 490 (73.6) pmol l−1] compared to the follicular phase [344.6 (59.7) pmol l−1). No significant differences in the psychological mood states between the phases of the menstrual cycle were found (P>0.05). No significant differences in vV̇O2 max (P=0.611), or PTV (P=0.472) were found between the phases of the menstrual cycle. Thus, vV̇O2 max and PTV are not affected by the monthly menstrual cycle in female endurance runners.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
There is a plethora of research that has utilised laboratory-based tests to obtain information on the relationships of selected physiological variables and endurance running performance (Birch and Reilly 1997; Janse de Jonge 2003). These illustrate that many factors influence endurance running performance, including running economy (Davies et al. 1997), maximal oxygen uptake (Chang et al. 1998), submaximal VO2 (Williams and Krahenbuhl 1997), training intensity (Heitkamp et al. 1991), recovery (Quinn et al. 1994), and metabolic and substrate factors (Giacomoni et al. 2000). The athlete and coach need to assess such variables associated with performance and try to combine them within a suitable training program to enhance performance. Indeed, prediction of physical performance from laboratory-based measurements has been a frequent concern for exercise physiologists and as such the physiology of the female athlete has received considerable attention over the last few decades. Within this topic, particular attention has been paid to the possible effects of the menstrual cycle phase on the physiological predictors of endurance running performance. However, whilst some of these aspects of the female athlete have been fairly extensively researched and reviewed in the past, recent developments in our understanding of the athlete’s physiology have revealed new areas of interest that need to be assessed with specific reference to the female. In particular, recent studies are finding that the physiological variables velocity at V̇O2 max (vV̇O2 max) and peak treadmill velocity (PTV) may be more highly predictive of endurance running performance than variables such as V̇O2 max and blood lactate (Billat et al. 2003; Noakes et al. 1990). However, many studies have focused solely on the physiological variables of V̇O2 max, blood lactate and submaximal and maximal heart rate (Giacomoni et al. 2000; Marsh and Jenkins 2002; Sunderland and Nevill 2003). No one study has as yet focused on these more recent variables suggested to be important predictors of performance. In addition, these specific variables have not been assessed in a group of homogenous highly trained athletes where any small variations in such physiological variables could significantly impact on training and performance. As such, the question as to how the variables could be affected by the sex hormone fluctuations across the monthly menstrual cycle remains unanswered. Therefore, the purpose of this study was to assess the menstrual cycle phase effects on vV̇O2 max and PTV in a homogenous group of highly trained female endurance runners.
Methods
Ten highly trained, eumenorrhoeic female endurance runners volunteered to participate in the present study. To be accepted on the study participants had to fulfil the following criteria: female, aged 18–40 years (to minimise any age related variability/alterations within the menstrual cycle), currently competing at distances of 1,500 m to marathon with current times within 40% of the national best recorded times for their event, and non-oral contraceptive users. Participants were recruited from UK athletic clubs.
Prior to participation in the study all participants signed a voluntary informed consent form and health questionnaire. The protocol was explained fully to each participant, highlighting the possible risks and benefits associated with participation. The study was approved by the University Ethics Committee.
For 2 months prior to laboratory-based testing, each participant completed a training and menstrual cycle diary. The training diaries reported the type, duration and intensity of each session, along with any occurrence of illness. The menstrual cycle diary recorded the onset and cessation of menses with any changes in the regularity of menses noted. A validated prospective mood state questionnaire was also completed prior to every training session to assess mood states such as irritability, fatigue, physical symptoms, negative and positive moods (Choi and Salmon 1995), to assess if they were altered across the menstrual cycle phases and thus impacting on the physiological variables (Warner and Bancroft 1988). Luteal phase onset was determined by participants collecting daily morning salivary samples across the two menstrual cycles prior to laboratory testing and throughout the period of laboratory-based testing, following a strict protocol using the salivette method of saliva collection which has been reported to decrease the possibility of gingival bleeding that is associated with the chewing and spitting methods of saliva collection (Kruger et al. 1996). All participants were instructed to collect the saliva samples prior to the brushing of teeth, application of make-up and after hand washing to avoid contamination. The mouth was rinsed with water a few times and the participant swallowed two to three times to remove old saliva. Subsequently participants remained at rest for a few minutes prior to taking the sample. One, unstimulated cotton swab (plain cotton swab not containing citric acid), was removed from the salivette (Salivette cotton swab without preparation; Sarstedt, Leicester, UK), and placed under the tongue for 2 min. After 2 min the swab was removed from the mouth and placed back into the salivette. Samples were labelled with participant identification, immediately frozen, and stored in domestic freezers. When the menstrual cycles were complete, the frozen samples were delivered to the laboratory in a frozen state, and stored in a freezer at −21°C for later analysis of salivary progesterone by means of a RIA (Coat-A-Count; DPC, USA) with a coefficient of variation (CV) <10%. The RIA has been previously validated by O’Rorke et al. (1995). Prior to analysis the frozen cotton swabs were thawed and centrifuged at 3,000 rev min−1 for 10 min to extract the saliva to be utilised in the assay (approximately 1–2 g of saliva was collected). The lower detection limits of the assay have been reported to be 20.7 pmol l−1. The intra-assay CVs ranged from 7.8% to 3.8% for the low to high pools, and the inter-assay CVs ranged from 9.1% to 3.8%, respectively. Recovery of the hormone from saliva has been assessed at 94.3%. The specificity of the antiserum used gives 23% cross-reactivity with 5α-pregnandione; all other steroids have less than 1.2% cross-reactivity. A modified detection limit of 20 pmol l−1 was utilised.
Participants were randomly divided into two groups of five to form a counter-balanced testing design to account for any possible order effects. Prior to commencing the study participants were familiarised with all the test procedures. Following familiarisation, all participants were tested in the early follicular phase (within 2–3 days post-menses=F1); late follicular phase (within 4–5 days pre-ovulation=F2); early luteal phase (within 1–2 days post-ovulation=L1); late luteal phase (within 1–2 days pre-menses=L2); and during two consecutive menses (M1 and M2). Thus, all participants completed 6 tests. Group 1 members were tested in the following sequence; L1 and L2, M1, F1 and F2, M2, whilst athletes in group 2 were tested in the sequence; M1, F1 and F2, L1 and L2 and M2. Times for the physiological testing were arranged to incorporate two tests within each phase of the cycle with at least 72 h between each test. Testing took place at the same time of day to minimise the effects of circadian rhythms (Atkinson and Reilly 1996).
On each test occasion participants entered the laboratory and were weighed (wearing lightweight T-shirt, shorts, and socks) to the nearest 0.1 kg (Balance Beam Scale; Seca, Germany). Height was recorded (stadiometer attached to balance beam scale; Seca, Germany) and the sum of four skinfolds was assessed using the four-site method of Durnin and Womersley (1974). Skinfold measures were performed in triplicate taking the average values, utilising Harpenden skinfold calipers (British Indicators, Luton, UK). Participants completed an individualised warm up before commencement of the treadmill tests. Participants retained the same warm-up for each session which consisted of approximately10 min slow jogging (9–10 km h−1), followed by 5–10 min stretching.
Following the warm-up participants completed a maximal test to exhaustion to determine V̇O2 max, vV̇O2 max and PTV. The maximal test commenced at a speed selected to elicit a test duration of approximately 8–12 min, with the treadmill speed increased every minute by 0.5 km h−1 until volitional exhaustion (Billat et al. 1994). All participants ran on a previously calibrated motorised treadmill (Woodway XELG70; Weil-am-Rhein, Germany) set at 1% gradient to simulate outdoor running (Jones and Doust 1996). Gaseous exchange (V̇O2) was measured using the COVOX microlab on-line gas analyser and recorded over 30-s intervals (Fitness research systems, Exeter, UK). Velocity at V̇O2 max (vV̇O2 max) was determined using the method of Billat et al. (1994), whilst PTV was taken as the highest speed (km h−1) maintained for a whole minute during the maximal test (Noakes et al. 1990). Maximal oxygen uptake (V̇O2 max) was assessed utilising a plateau in V̇O2 (increased <2.1 ml kg−1 min−1), respiratory exchange ratio >1.1, blood lactate levels >8 mmol l−1, and a heart rate >90% of the predicted maximum heart rate.
Throughout the experimental period all participants were asked not to perform any strenuous exercise within 48 h and no exercise 24 h prior to the tests. They were also requested not to consume food within 4 h of the test; no alcohol within 24 h; no caffeine within 6 h; to wear identical lightweight clothing for each test; and to maintain their regular diets throughout the test procedures.
Group 1 and group 2 were combined to produce a larger sample size for ANOVA analysis. As groups 1 and 2 had small sample sizes the assumptions of normality and homogeneity of variance for parametric tests could not be met, so the data were subjected to a non-parametric Mann-Whitney U-test to assess whether the two groups had a different population distribution in the participant summary statistics. This demonstrated that as well as no order effect of testing, there were no significant differences between the physical, gynaecological, and training profiles of group 1 (n=5) and group 2 (n=5) (P>0.05). Thus, groups 1 and 2 were combined (n=10) for all further data analysis.
A two-way ANOVA with repeated measures (phase×time) was utilised to compare differences between vV̇O2 max, PTV and mood states across the menstrual cycle phases (SPSS, version 11.0). An alpha level of P<0.05 was selected to identify significant differences. ANOVA assumption of spherificity was assessed in SPSS (version, 11.0), and all physiological and psychological data met the assumption. Mean (SEM) and 95% CIs were reported for vV̇O2 max and PTV. Effect size for the study was also calculated (Cohen 1977).
Results
The current study showed an effect size of 0.2 for vV̇O2 max and PTV indicating a small effect size for this study.
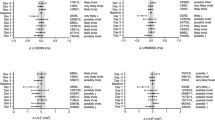
Hormonal analysis of salivary progesterone confirmed the expected hormonal profiles and timing of the menstrual cycle phases, with increases in progesterone at the onset of the luteal phase [490 (73.6) pmol·l−1; 340–640 pmol·l−1] compared to the follicular [344.6 (59.7) pmol·l−1; 223–466 pmol·l−1], and menstrual [305.5 (60.5) pmol·l−1;180–430 pmol·l−1] phases. The CUSUM method (Lebenstedt et al. 1999) was utilised to identify an increase in individual progesterone values above the follicular baseline and thus the onset of the luteal phase (Fig. 1). The data were combined with the menstrual cycle diaries to detect any shortened luteal phases (luteal phase <10 days). All cycles were regular, with no occurrence of shortened luteal phases or oligomenorrhoea.

Luteal phase data are normalised around day 1, which is the day of a significant rise in progesterone concentrations (analysed by CUSUM). Average follicular phase values are taken from the longitudinal mean of four samples of the follicular phase (days 2–7)
The participant characteristics are shown in Table 1. No statistically significant differences in any of the psychological mood states (positive, irritability, fatigue, physical symptoms, or negative mood states; P>0.05) were found between the phases of the menstrual cycle (Fig. 2).

Mood states are averaged over all days of each menstrual phase; Menses (black); follicular (hatched); luteal (cross-hatched). Values are mean (SEM)
No statistically significant differences in vV̇O2 max [M1=14.7 (0.6) km·h−1; M2=15 (0.8) km·h−1; F1=14.5 (0.7) km·h−1; F2=14.4 (0.8) km·h−1; L1=14.7 (0.6) km·h−1; L2=14.8 (0.7) km·h−1; F5,35=0.72; P=0.611], or PTV [M1=15.3 (0.7) km·h−1; M2=15.6 (0.8) km·h−1; F1=15.4 (0.7) km·h−1; F2=15.7 (0.8) km·h−1; L1=15.7 (0.6) km·h−1; L2=15.5 (0.8) km·h−1; F5,35=0.93; P=0.472] were found within or between the menstrual, follicular, or luteal phases of the menstrual cycle (Table 2). In addition, no significant difference in body mass was found within or between the phases of the menstrual cycle (P>0.05).
Discussion
The results of this study indicate that vV̇O2 max and PTV in highly trained female endurance runners were not altered within or across the phases of the menstrual cycle. The fact that no variation in the performance predictors were observed over the menstrual cycle phases in the present study could be due to the highly trained status of the participants and the controlled pre-testing training and dietary habits (Maughan et al.1997).
Mood states
Mood states have often been linked to performance with negative moods, such as anxiety, reported to decrease performance (Reilly 1977). Warner and Bancroft (1988) reported positive feelings to increase pre-ovulation and to decrease thereafter with negative moods (irritability, depression and anxiety), increasing post-ovulation, pre-menstrually and menstrually. As such, if one wishes to study the effects of the menstrual cycle on the physiological variables associated with performance, and not the psychological variables associated with performance, mood states need to be assessed to ensure that any changes seen in physiological variables are attributed to the phases of the menstrual cycle and not the alterations in mood states alone. This study found no significant changes in irritability, positive, negative and fatigue mood states, or physical symptoms across the menstrual cycle phases. As such, these mood states should not be affecting the physiological variables measured across the menstrual cycle. This finding is in agreement with past research that has reported that female mood fluctuations are less over the menstrual cycle than those observed on a day-to-day basis (McFarlane et al. 1988).
Velocity at V̇O2 max
vV̇O2 max is a useful variable that combines V̇O2 max and running economy into a single factor (Jones 1998). Since it is theoretically the minimal velocity needed to elicit V̇O2 max, it should describe the ideal training intensity for middle and long distance training (Billat et al. 2003). It is therefore reasoned that any change in vV̇O2 max during the menstrual cycle could have a corresponding impact on endurance running performance. The present study found no significant changes in vV̇O2 max across or within the menstrual phases, even though an increase in progesterone during the luteal phase was shown. Thus suggesting that the luteal phase has little effect on this variable of performance. With an increase in progesterone levels an increased circulatory and aerobic—metabolic strain has been proposed (Hessemer and Bruck 1985) and would suggest that vV̇O2 max would alter across the menstrual phases. However, such early studies had serious methodological flaws, such as not using hormonal identification of the luteal phase and not controlling for extraneous variables such as mood states and diet. Indeed, those studies using hormonal documentation in a well-controlled study design have shown a dissociation of the metabolic and thermoregulatory responses associated with the menstrual cycle (Lebrun 1994; Lynch and Nimmo 1998). As such, this would support the no change in vV̇O2 max found in this study.
Peak treadmill velocity
Noakes et al. (1990) showed that PTV is a better predictor of running performance than V̇O2 max alone, particularly for distances between 10 and 90 km. As such, this variable is highly related to endurance performance and needs to be assessed to determine if it is affected by the hormonal fluctuations present across the menstrual cycle. PTV has been suggested to be related to the muscle capacity for high cross-bridge cycling and respiratory adaptations (Noakes 1986). Thus, if the higher levels of progesterone in the luteal phase of the menstrual cycle affect cross bridge cycling and respiratory variables, PTV may also be affected, impinging on endurance performance. However, the present study found no significant difference in PTV across and within the menstrual phases suggesting that the luteal phase has little effect on this variable of running performance. Although, to the author’s knowledge, no previous published studies have assessed this variable across the menstrual cycle, studies have measured various respiratory variables (Williams and Krahenbuhl 1997) and muscle strength (Janse de Jonge et al. 2001; Fridan et al. 2003) across the menstrual cycle. Those studies which have been well controlled have found no significant difference in respiratory variables and muscle strength across the phases, thus providing some indirect support and evidence for why there would be no significant change in PTV.
The present study failed to show evidence of any differences in the physiological variables measured within and between the menstrual cycle phases. It seems that due to the stability of the cardiovascular and respiratory systems across the menstrual cycle no attempt to compensate for metabolic acidosis was required. Thus, the physiological predictors were stable across the six menstrual phases assessed. However, it is acknowledged that the sample size was small. Since there is little data concerning the changes expected in vV̇O2 max and PTV across the menstrual cycle, a statistical power analysis prior to the study was problematic. In light of the current study’s data, to get a power of 0.80 for a difference of 0.5 km h−1, with α=0.05 would require 64 participants.
As this study only had ten participants there is potential for the study to be underpowered. However, the small SEM and stable within-subject variation in vV̇O2 max and PTV across the phases lends support for the results found. This analysis is valuable for researchers considering subsequent studies in this area. Particularly as more research needs to be completed looking at these variables across the menstrual cycle using the wide range of methodologies employed to predict them. In addition, research is needed to assess other important variables being recognised as good predictors of endurance running performance i.e., time to exhaustion at vV̇O2 max.,to assess if they are affected by the sex hormone fluctuations across the menstrual cycle. The testing needs to be completed over a range of days within the cycle to ascertain the relationship between the hormonal fluctuations within each menstrual phase and their concomitant effect on endurance running performance. The status of the participants also needs to be verified by hormonal documentation with data on anovulatory females required to elucidate if their responses are similar to ovulatory females.
References
Atkinson G, Reilly T (1996) Circadian variation in sports performance. Sports Med 21:292–312
Billat V, Renoux JC, Pinoteau J, Petit B, Koralsztein JP (1994) Reproduability of running time to exhaustion at VO2 max in sub-elite runners. Med Sci Sports Exerc 26:254–257
Billat LV, Lepretre PM, Heugas AM, Laurtence MH, Salim D, Koralsztein P (2003) Training and bioenergetic characteristics in elite male and female Kenyan runners. Med Sci Sports Exerc 35:297–304
Birch KM, Reilly T (1997) The effects of eumenorrhoeic menstrual cycles on physiological responses to a repetitive lifting task. Can J Appl Physiol 22:148–160
Chang R, Lambert G, Mosely P, Chapler F, Gisolfi C (1998) Effects of estradiol supplementation on exercise thermoregulation in premenopausal females. J Appl Physiol 85:2082–2086
Choi PY L, Salmon P (1995) Symptom changes across the menstrual cycle in competitive sportswomen, exercisers and sedentary women. Br J Clin Psychol 34:447–460
Cohen J (1977) Statistical power analysis for the behavioural science. Academic Press, London
Davies MJ, Mahar MT, Cunningham LN (1997) Running economy: comparison of body mass adjustment methods. Res Q Exerc Sport Sci 68:177–181
Durnin JVGA, Womersley J (1974) Body fat assessed from total body density and its estimation from skinfold thickness: measurements on 481 men and women aged from 16 to 72 years. Br J Nutr 32:77–97
Friden C, Hirschberg A, Saartok T (2003) Muscle strength and endurance do not significantly vary across 3 phases of the menstrual cycle in moderately active premenopausal women. Clin Sports Med 13:238–241
Giacomoni M, Bernard T, Gavarry O, Altare S, Falgairette G (2000) Influence of the menstrual cycle phase and menstrual symptoms on maximal anaerobic performance. Med Sci Sports Exerc 32:486–492
Heitkamp H, Holdt M, Scheib K (1991) The reproducibility of the 4 mmol l−1 lactate threshold in trained and untrained women. Int J Sports Med 12:363–368
Hessemer V, Bruck K (1985) Influence of menstrual cycle on thermoregulatory, metabolic, and heart rate responses to exercise at night. J Appl Physiol 59:1911–1917
Janse de Jonge XAK (2003) Effects of the menstrual cycle on exercise performance. Sports Med 33:833–851
Janse de Jonge XAK, Boot CRL, Thom JM, Ruell PA, Thompson MW (2001) The influence of menstrual cycle phase on skeletal muscle contractile characteristics in humans. J Physiol (Lond) 530:161–166
Jones AM (1998) A five year physiological case study of an Olympic runner. Br J Sports Med 32:39–43
Jones AM, Doust JH (1996) A comparison of three treadmill protocols for the determination of maximal aerobic power in runners. J Sports Sci 14:89–94
Kruger C, Ulrike B, Jutta BS, Helmuth GD (1996) Problems with salivary 17-hydroxyprogesterone determinants using the salivette device. Eur J Clin Chem Biochem 34:927–929
Lebenstedt M, Platte P, Pirke KM (1999) Reduced resting metabolic rate in athletes with menstrual disorders. Med Sci Sports Exerc 31:1250–1256
Lebrun CM (1994) The effect of the phase of the menstrual cycle and the birth control pill on athletic performance. Clin J Sports Med 13:419–441
Lynch NJ, Nimmo MA (1998) Effects of menstrual cycle phase and oral contraceptive use on intermittent exercise. Eur J Appl Physiol 78:565–572
Marsh SA, Jenkins DG (2002) Physiological responses to the menstrual cycle: implications for the development of heat illness in female athletes. Sports Med 32:601–614
Maughan RJ, Greenhaff PL, Leiper JB (1997) Diet composition and the performance of high-intensity exercise. J Sports Sci 15:265–275
McFarlane J, Martin CL, Williams TM (1988) Mood fluctuations: women versus men and menstrual versus other cycles. Psychol Women Q 12:201–223
Noakes TD (1986) Lore of running. Oxford University Press, Cape Town, South Africa
Noakes TD, Myburgh KH, Schall R (1990) Peak treadmill velocity during the VO2 max test predicts running performance. J Sports Sci 8:35–45
O’Rorke A, Kane MM, Gosling JP, Tallon DF, Fotrell PF (1995) Development and validation of a monoclonal antibody enzyme immunoassay for measuring progesterone in saliva. Clin Chem 40:454–458
Quinn TJ, Vroman NB, Kertzer R (1994) Post exercise oxygen consumption in trained females: effect of exercise duration. Med Sci Sports Exerc 26:908–913
Reilly T (1977) Pre-start moods of cross-country runners and their relationship to performance. Int J Sports Psychol 8:210–217
Sunderland C, Nevill M (2003) Effect of the menstrual cycle on performance of intermittent, high intensity shuttle running in a hot environment. Eur J Appl Physiol 88:345–352
Warner P, Bancroft J (1988) Mood, sexuality, oral contraceptives and the menstrual cycle. J Psychol Res 32:417–427
Williams TJ, Krahenbuhl GS (1997) Menstrual cycle phase and running economy. Med Sci Sports Exerc 29:1609–1618
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Burrows, M., Bird, S.R. Velocity at V̇O2 max and peak treadmill velocity are not influenced within or across the phases of the menstrual cycle. Eur J Appl Physiol 93, 575–580 (2005). https://doi.org/10.1007/s00421-004-1272-5
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00421-004-1272-5