
Abstract
Caffeine ingestion is associated with increases in the concentration of plasma epinephrine and epinephrine is associated with alterations in immune cell trafficking and function following intensive exercise. Therefore, the purpose of this study was to investigate the effect of caffeine ingestion on plasma epinephrine concentration, lymphocyte counts and subset activation in vivo, as measured by the expression the CD69 surface antigen, before and after intensive cycling. On two occasions, following an overnight fast and 60 h abstention from caffeine containing foods and drinks, eight endurance trained males cycled for 90 min at 70% V̇O2 max 60 min after ingesting caffeine (6 mg kg−1 body mass; CAF) or placebo (PLA). Venous blood samples were collected at pre-treatment, pre-exercise, post-exercise and 1 h post-exercise. Plasma epinephrine concentrations were significantly higher in CAF compared with PLA at pre-exercise [0.28 (0.05) nmol l−1 versus 0.08 (0.03) nmol l−1, P<0.01; mean (SE)] and immediately post-exercise [1.02 (0.16) nmol l−1 versuss 0.60 (0.13) nmol l−1, P<0.01]. Compared with pre-treatment, numbers of CD4+ and CD8+ cells decreased by 54% and 55%, respectively, in CAF at 1 h post-exercise (both P<0.01) but did not significantly differ in PLA. Compared with PLA, in CAF the percentage of CD4+CD69+ cells was 5-fold higher at post-exercise (P<0.05) and 5.5-fold higher at 1 h post-exercise (P=0.01). Compared with PLA, in CAF the percentage of CD8+CD69+ cells was 2-fold higher at pre-exercise (P<0.05) and 1.7-fold higher at post-exercise (P<0.05). These findings suggest that caffeine ingestion is associated with alterations in lymphocyte subset trafficking and expression of CD69 in vivo following prolonged, intensive exercise.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Caffeine is commonly used by endurance athletes to improve performance with doses as low as 2–3 mg kg−1 body mass reported to have ergogenic effects (Graham 2001). The mechanism behind the ergogenic effect of caffeine is still to be fully resolved. However, caffeine ingestion is widely associated with stimulation of the sympathetic nervous system and with subsequent elevations in the plasma concentrations of the catecholamines epinephrine and norepinephrine (Graham and Spriet 1995; Graham et al. 2000). Recent studies have also demonstrated elevations in plasma cortisol concentration with caffeine ingestion and exercise (Laurent et al. 2000). In addition to influencing performance, these changes could also have important implications for immune cell trafficking and function. Exercise-induced increases in plasma catecholamine and cortisol concentrations are associated with the movement of immune cells to and from the circulation and with alterations in immune cell function following intensive exercise (McCarthy and Dale 1988; Pedersen et al. 1997). However, to date, any effect of caffeine ingestion on immune cell responses to exercise in healthy individuals has not been investigated. Any such influence of caffeine is of great relevance since the use of caffeine as an ergogenic aid is likely to become even more widespread following the recent removal of this substance from the World Anti-Doping Agency list of prohibited substances.
To the authors’ knowledge there are only two published studies that have directly investigated the effect of caffeine on immune cell function. These reported that the addition of pharmacological doses of caffeine to cell culture media was associated with a dose-dependent inhibition of in vitro mitogen-stimulated proliferative responses in rat (Kantamala et al. 1990), mice and human (Rosenthal et al. 1992) T and B lymphocytes. However, in vivo administration of 18 mg kg−1 day−1 of caffeine in rats was associated with a significant increase in mitogen-stimulated T cell proliferation, yet B cell proliferative responses to mitogen were significantly decreased following administration of 6 mg kg−1 day−1 of caffeine.
Acute strenuous exercise is associated with significant alterations in the circulating concentrations of total lymphocytes and subpopulations. Noticeable increases in concentration are evident during exercise, followed by a marked fall in numbers during recovery, often to values below those at baseline (Gabriel et al. 1992; Nieman et al. 1995; Shek et al. 1995). In addition, acute intensive exercise is associated with an increase in the state of lymphocyte subset activation in vivo, for example as measured by the concentration of circulating lymphocytes expressing cell surface markers of T cell activation, such as CD45RO and the HLA-DR antigen (Gabriel et al. 1993; Gray et al. 1993). More recently, the effect of intense exercise on the expression of the early activation molecule CD69 has been assessed both in vivo and following in vitro mitogenic stimulation (DuBose et al. 2003; Green et al. 2003; Ronsen et al. 2001). Resting (unstimulated) peripheral blood lymphocytes do not usually express CD69, with only a small number of circulating T lymphocytes expressing low levels of this marker (Testi et al. 1994). Nevertheless, it is induced quickly following stimulation of the T cell receptor/CD3 complex, with transcription of CD69 evident after 30–60 min and surface expression detectable after 2–3 h (Testi et al. 1994; Ziegler et al. 1993). Two studies to date have found that the in vivo expression of CD69 on CD4+ and CD8+ cells did not significantly alter in response to exercise lasting approximately 1 h (Ronsen et al. 2001; Green et al. 2003). A recent study of military recruits, however, found a significant increase in the percentage of CD8+ lymphocytes expressing CD69+ in vivo following a 1.75–2-mile training run in warm weather; this response tended to be greater in individuals with exertional heat injury (DuBose et al. 2003).
There is an association between caffeine, exercise and stress hormone release and between elevations in plasma concentrations of epinephrine and cortisol and immune cell responses. Therefore, the purpose of the present study was to investigate the effect of caffeine versus placebo ingestion on plasma stress hormone concentration, numbers of circulating lymphocytes and CD4+ and CD8+ cell expression of the early activation molecule CD69 in vivo following cycling for 90 min at 70% V̇O2 max.
Methods
Subjects
Eight endurance trained males [mean (SE): age 24 (2) years; height 184 (2) cm; body mass 76.6 (3.4) kg; V̇O2 max 65.6 (2.3) ml kg−1 min−1] volunteered to participate in the study. All subjects were informed about the rationale for the study and the nature of the exercise tests to be performed before providing written informed consent. The Ethics Committee of Loughborough University approved the protocol. Subjects were required to complete a comprehensive health-screening questionnaire prior to each exercise test and did not report any symptoms of infection and had not taken any medication in the 4 weeks prior to the study, nor were they currently on medication. Habitual caffeine consumption among the subjects varied with two very light users (ingesting ≤50 mg day−1), five moderate users (≤300 mg day−1) and one high user (>800 mg day−1), as categorised by their responses to a questionnaire administered at the beginning of the study.
Preliminary testing
Approximately 1 week before the beginning of the study each subject performed a continuous incremental exercise test on an electromagnetically braked cycle ergometer (Lode Excalibur Sport, Groningen, the Netherlands) to volitional exhaustion to determine maximal oxygen uptake (V̇O2 max). Subjects began cycling at 95 W, with increments of 35 W every 3 min until volitional fatigue. Samples of expired gas were collected in Douglas bags during the 3rd minute of each work rate increment and heart rates were measured continuously using short-range radio telemetry (Polar Beat; Polar Electro, Oy, Finland). A paramagnetic oxygen analyser (Servomex 1420B; Crowborough, UK) and an infrared carbon dioxide analyser (Servomex 1415B) were used along with a dry gas meter (Harvard Apparatus, Edenbridge, UK) for determination of V̇E, V̇O2 and V̇CO2. The work rate equivalent to 70% V̇O2 max was interpolated from the V̇O2-work rate relationship. Subjects then returned to the laboratory 2 days later at a time of their choosing in order to acquaint themselves with the exercise trials. During this familiarisation trial, subjects cycled on an electrically braked cycle ergometer for 90 min at 70% V̇O2 max. Expired air samples were obtained and analysed as described above after the first 10 min and at 20-min intervals thereafter in order to ensure that the subjects were exercising at the required intensity. If the subject was exercising at below 70% V̇O2 max or in excess of 75% V̇O2 max the work rate was adjusted accordingly. Heart rates were monitored throughout this familiarisation trial.
Experimental trial procedures
Each subject was given a comprehensive list of caffeine containing foods and drinks and instructed to abstain from these products during the 60 h preceding each exercise trial. Subjects were also instructed refrain from alcohol intake and not to participate in any sporting activity during the 24 h preceding each main experimental trial. In an effort to standardise their nutritional status, subjects were asked to eat the same foods and drinks during the 24 h prior to both experimental trials.
For the main exercise trials, on two occasions, separated by one week, subjects reported to the laboratory at 0800 hours following an overnight fast of at least 10 h and were randomly assigned to either the caffeine (CAF) or placebo (PLA) trial in a cross-over random block design. Subjects were then required to empty their bladder before body mass (in shorts only) was recorded. After sitting quietly for 10 min, an initial resting blood sample was obtained from an antecubital vein by venepuncture (pre-treatment blood sample). Following blood sampling, in the CAF trial subjects were given 6 mg kg−1 body mass of caffeine dissolved in 3 ml kg−1 body mass of artificially sweetened (aspartame) lemon flavoured water; in the PLA trial, subjects were given the same volume of the lemon flavoured water containing artificial sweetener but zero caffeine. Subjects then rested quietly in the laboratory for 1 h before a further pre-exercise venous blood sample was obtained from an antecubital vein. Immediately after this sample had been collected, subjects began cycling on an electromagnetically braked cycle ergometer (Lode Excalibur Sport, Groningen, the Netherlands) at the work rate equivalent to 70% V̇O2 max [222 (33) W] for 90 min. In order to standardise fluid intake, subjects consumed a further 2 ml kg−1 body mass of plain water at 15-min intervals throughout the exercise on both trials. Heart rates were also recorded at these times. Samples of expired air were collected into Douglas bags after 20 min of exercise and every 30 min thereafter for determination of V̇O2 and V̇CO2 to allow determination of fat and carbohydrate oxidation and energy expenditure using stoichiometric equations (Frayn 1983). A further venous blood sample was obtained at immediately post-exercise before body mass (in shorts only) was recorded. On both trials subjects then consumed 5 ml kg−1 body mass of plain water. A final venous blood sample was obtained at 1 h post-exercise. For all samples, 12.8 ml of blood was collected and all samples were obtained with the subject in a seated position. No other fluid or food intake was allowed until the blood sample had been collected at 1 h post-exercise. Laboratory conditions were 21.1 (0.8)°C and 52 (5)% relative humidity.
Total lymphocyte count and plasma volume
Blood samples were collected into three separate monovette tubes (evacuated blood collection tubes; Sarstedt, Leicester, UK), one containing K3EDTA (1.6 mg EDTA ml−1 blood) and two containing lithium heparin (1.5 IU heparin ml−1 blood). Blood taken into the K3EDTA monovette (2.7 ml) was used for haematological analysis including haemoglobin, haematocrit and total lymphocyte counts using a Sysmex SE9000 cell counter (Sysmex UK, Milton Keynes, UK) at the Chemical Pathology laboratories of Leicester Royal Infirmary NHS Trust. All cell counts were corrected for plasma volume changes relative to values from the first (pre-treatment) blood sample, which were estimated from the haemoglobin and haematocrit values according to Dill and Costill (1974).
Assessment of lymphocyte subsets and CD69 expression
Expression of CD4, CD8 and CD69 by peripheral blood cells was analysed by flow cytometry, using Pharmingen monoclonal and isotype control antibodies purchased from Becton Dickinson Biosciences, Oxford, UK. Whole blood drawn directly into a 2.6-ml lithium heparin monovette was placed on ice and regularly mixed by hand before performing staining and analysis later the same day. Aliquots of whole blood were labelled with a cocktail of the following monoclonal antibodies against human lymphocyte cell surface markers: fluorescein isothiocyanate (FITC) conjugated anti-CD4, R-phycoerythrin-Cy5 (PE-Cy5) conjugated anti-CD8, and phycoerythrin (PE) conjugated anti-CD69. Labelling was carried out on ice and the cells subsequently washed once in ice-cold PBS containing 0.1% bovine serum albumin (BSA) and 2 mM EDTA (PBS/BSA/EDTA), after which the erythrocytes were lysed with FACSLyse (Becton Dickinson Biosciences, Oxford, UK), and the leukocytes resuspended in PBS/BSA/EDTA. Three-colour flow cytometric analysis was carried using a FACScan flow cytometer with CellQuest analysis software (Becton Dickinson, Oxford, UK). Side scatter versus forward scatter plots were used to gate on the lymphocyte population by morphology, and 30,000 lymphocyte events were acquired per analysis. Cells incubated with appropriate fluorescent-labelled isotype control antibodies were used to define the threshold of positive staining for CD4, CD8 and CD69, respectively. The percentage of T cells expressing CD4 and CD8 was derived from quadrant analysis of FL1 (CD4 FITC) versus FL3 (CD8 PE-Cy5) dot plots, and estimation of absolute CD4+ and CD8+ numbers derived from the total lymphocyte count. CD4 and CD8 positive cells were gated into separate regions, and CD69-PE histogram plots of the cells in each of these regions were used to calculate the percentage of the CD4+ and CD8+ cells expressing CD69.
Plasma hormones and blood-borne metabolites
Heparinised plasma was obtained from blood collected into a further lithium heparin monovette (7.5 ml). This was spun at 1,500 g for 10 min in a refrigerated centrifuge (4°C) within 5 min of sampling. Of the plasma obtained, 2 ml was immediately added to chilled tubes containing 200 μl of preservative (pH 6.5) containing EGTA (100 mM) and glutathione (100 mM) for later determination of norepinephrine and epinephrine concentrations. The tubes were mixed and then immediately frozen at −80°C. Plasma levels of catecholamines were determined by HPLC with electrochemical detection as previously described (Forster and Macdonald 1999). Plasma catecholamine concentrations were determined in seven of the eight subjects due to a technical problem concerning the samples from one subject in both the CAF and PLA trials.
The remaining heparinised plasma was immediately stored at −80°C for later analysis. Plasma cortisol was determined by 125I radioimmunoassay (ICN Pharmaceuticals, Costa Mesa, Calif., USA). Plasma lactate was determined in deproteinised plasma using a standard spectrophotometric method, as described by Fink and Costill (1995). Commercially available kits were used to determine plasma concentrations of glucose (GOD-PAP method; Randox Laboratories, Co. Antrim, N. Ireland) and free fatty acids (FFA) (Wako Chemicals, Neuss, Germany) for an automated system (COBAS Mira Plus; Roche Diagnostic Systems, Switzerland).
The intra-assay co-efficient of variation was 1.9% and 6.6% for norepinephrine and epinephrine, respectively. In addition, the intra-assay co-efficient of variation was 1.8% for cortisol, 2.8% for lactate, 1.6% for glucose and 1.4% for FFA.
Statistical analysis
Data in the text, tables and figures are presented as mean (SE). The data were examined using a two-factor (trial×time of measurement) ANOVA with repeated measures design. If a data set was not normally distributed, statistical analysis was performed on the logarithmic transformation of the data. Assumptions of homogeneity and sphericity in the data were checked and, where appropriate, adjustments in the degrees of freedom for the ANOVA were made using the Huynh-Feldt method of correction. Any significant F ratios subsequently shown were assessed using Student’s paired t-tests with Bonferroni correction for multiple comparisons applied to the unadjusted P value. Where significant interactions between trial and time of measurement have been found, these are reported. If the interaction between trial and time was non significant but a significant main effect of trial or main effect of time was found, the main effects only are reported. Single comparisons between trials for overall exercise intensity, fat and carbohydrate oxidation rates, rate of energy expenditure and percentage contribution of substrate to energy expenditure were made using Student’s paired t-tests. Statistical significance was accepted at P<0.05.
Results
Exercise intensity, heart rate and indirect calorimetry
Exercise intensity did not differ between the trials; mean % V̇O2 max during exercise was 74.8 (0.6)% and 73.9 (0.5)% in CAF and PLA, respectively. Likewise, heart rates were similar between trials throughout the exercise [CAF: 157 (3) beat min−1, PLA: 155 (3) beat min−1; mean of all recordings]. Respiratory exchange ratio (RER) values were significantly lower in the CAF trial compared with PLA [0.92 (0.01) and 0.95 (0.01) on CAF and PLA, respectively, t=3.4, P=0.01]. Similarly, rates of fat oxidation were significantly higher during exercise in CAF than PLA [CAF: 0.46 (0.06) g min−1, PLA: 0.32 (0.04) g min−1; t=3.7, P<0.01] but there were no significant differences in rates of carbohydrate oxidation during the exercise [3.4 (0.3) g min−1 and 3.6 (0.2) g min−1 on CAF and PLA, respectively, t=2.2, P=0.07]. Energy expenditure was similar in both trials [CAF: 76 (3) kJ min−1, PLA 74 (3) kJ min−1] but the percentage contribution of fat oxidation was significantly higher in the CAF trial compared with PLA [24 (3)% versus 17 (3)%, t=3.2, P=0.02].
Changes in body mass and plasma volume
After exercise changes in body mass (corrected for fluid intake) were similar in both trials [−2.6 (0.3) kg and −2.4 (0.1) kg on CAF and PLA, respectively]. There was no significant time×trial interaction for changes in plasma volume relative to the pre-treatment sample; after exercise plasma volume had decreased by 11.2 (1.1)% and 11.0 (1.5)% in the CAF and PLA trials, respectively.
Plasma hormones and blood-borne metabolites
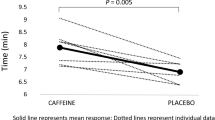
A significant time×trial interaction was found for plasma epinephrine concentration, which was higher in the CAF trial compared with PLA at pre- and immediately post-exercise (F2,12=12.02, both P<0.01; Fig. 1). A significant main effect of time only was found for plasma norepinephrine levels, with values elevated above pre-treatment levels at pre-exercise and immediately post-exercise independently of the trial followed (F2,12=55.1, both P<0.01, Table 1). There was a main effect of trial only for plasma cortisol with concentrations higher in CAF compared with PLA (F1,7=6.2; P<0.05; Table 1). A significant time×trial interaction was found for plasma FFA concentration, with values increasing from pre-treatment to pre-exercise in the CAF trial only (F3,21=3.1; P<0.05, Table 1). At 1 h post-exercise, plasma FFA concentration was significantly higher in CAF than PLA (P<0.05). There was no significant trial×time interaction or significant main effects for plasma glucose concentration (Table 1). A significant main effect of time only was found for plasma lactate with levels higher after exercise compared with pre-exercise and pre-treatment (F2,14=55.2, both P<0.01, Table 1).

Plasma epinephrine concentration during the caffeine (CAF) and placebo (PLA) trials. Values are mean (SE), n=7. Time −60, pre-treatment; time 0, pre-exercise; time 90, post-exercise. Asterisk Significantly different from pre-treatment within trial (P<0.01); cross significantly higher than PLA at that time point (P<0.01)
Lymphocyte concentrations and expression of CD69
There was a significant trial×time interaction for numbers of circulating lymphocytes, which were higher on CAF compared with PLA at pre-exercise (F3,21=5.3, P<0.01; Fig. 2). A significant time×trial interaction was also found for numbers of CD4+ cells, with the CD4+ cell count lower at pre-exercise and 1 h post-exercise compared with pre-treatment on the CAF trial only (F3,21=7.0, both P<0.01; Fig. 3a). CD4+ cell count did not change significantly over the sample time points in PLA. There was significant interaction between trial and time for numbers of circulating CD8+ cells, which were higher in CAF than in PLA at pre-exercise (F3,21=6.5, P<0.01; Fig. 3b). A significant fall in CD8+ cell number was observed at 1 h post-exercise in the CAF trial only (P<0.01, compared with pre-treatment). A significant time×trial interaction was found for the percentage of CD4+ cells expressing CD69, which were higher in CAF than PLA at pre-exercise, post-exercise and 1 h post-exercise (F3,21=5.4, P<0.05 except 1 h post-exercise, P=0.01; Fig. 4a). A significant time×trial interaction was also found for the percentage of CD8+ cells expressing CD69, which were higher on CAF than PLA at pre-exercise and post-exercise (F3,21=3.5, both P<0.05; Fig. 4b).

Circulating concentrations of lymphocytes during the CAF and placebo PLA trials. Values are mean (SE), n=8. Time −60, pre-treatment; time 0, pre-exercise; time 90, post-exercise; time +60, 1 h post-exercise. Asterisk Significantly different from pre-treatment within trial (P<0.01); cross significantly different from pre-exercise within trial (P<0.01); double cross: significantly higher than PLA at that time point (P<0.01)

Circulating concentrations of CD4+ (a) and CD8+ cells (b) during the caffeine (CAF) and placebo (PLA) trials. Values are mean (SE), n=8. Time −60, pre-treatment; time 0, pre-exercise; time 90, post-exercise; time +60, 1 h post-exercise. Asterisk Significantly different from pre-treatment within trial (P<0.01); cross significantly higher than PLA at that time point (P<0.01)

Percentage of CD4+ (a) and CD8+ (b) cells expressing CD69 during the CAF and placebo PLA trials. Values are mean (SE), n=8. Time −60, pre-treatment; time 0, pre-exercise; time 90, post-exercise; time +60, 1 h post-exercise. Asterisk Significantly different from pre-treatment within trial (P<0.05); cross significantly higher than PLA at that time point (P<0.05)
Discussion
The findings of the present study suggest that caffeine ingestion 1 h prior to exercise is associated with greater elevations is plasma epinephrine and larger perturbations in the circulating concentration of total lymphocytes and CD4+ and CD8+ lymphocyte subsets both pre-exercise and 1 h post-exercise. Furthermore, caffeine ingestion was associated with an increase in the natural state of lymphocyte activation in vivo, as assessed by the increased percentage of CD4+ and CD8+ cells expressing the early activation marker, CD69, both before and after exercise.
The main finding of the study is an increase in the natural state of activation of CD4+ and CD8+ cells both before and after exercise with pre-exercise caffeine ingestion only. Previous studies that have determined cell surface expression of CD69 on CD4+ and CD8+ cells following exercise lasting approximately 1 h have found that exercise alone has little influence on this marker of early cell activation (Green et al. 2003; Ronsen et al. 2001). The findings in the PLA trial in the present study are consistent with this. However, a recent study reported a significant increase in the percentage of CD8+CD69+ cells in vivo following a 1.75- to 2-mile training run in warm weather in military recruits that lasted less than 15 min (DuBose et al. 2003). Reasons for these inconsistent findings are not immediately apparent, although differences in exercise duration, ambient conditions or overall exercise intensity may be responsible.
In vivo CD69 is expressed rapidly following engagement of the T cell receptor (Testi et al. 1994) and expression of this molecule is associated with subsequent T cell proliferation and cytotoxic activity (Mueller et al. 2002). In the present study, the increased percentage of CD4+ and CD8+ cells expressing CD69 with caffeine ingestion and exercise could be interpreted in two ways, which may occur simultaneously. On one hand, it might be that the increase in the proportion of circulating CD4+ and CD8+ cells expressing CD69 with exercise and caffeine ingestion simply indicates that caffeine enhances the recruitment of a subpopulation activated cells into the circulation, perhaps via catecholamine influences on cell adhesion molecules and enhanced shear stress. At pre-exercise, plasma epinephrine was markedly elevated in the CAF versus PLA trial and this could explain why the concentration of total lymphocytes was higher in the CAF trial compared with PLA at this time. Although lymphocytes exhibit a circadian rhythm, the fall in the total lymphocyte count in the PLA trial at this time is greater than the reported diurnal changes in the circulating concentration of these cells (Cannon 1993). The reason for this relatively large decline in total lymphocyte count is not clear. However, this cannot be an effect of hemodilution since all cell counts were adjusted for changes in plasma volume.
The elevation in total numbers of circulating lymphocytes in the CAF trial at pre-exercise was reflected in the numbers of CD8+, but not CD4+ cells (which actually fell to below pre-treatment values). This is most likely because CD8+ cells express a greater density of β-receptors than CD4+ cells (Maisel et al. 1990; Murray et al. 1992). Therefore, while increased recruitment of CD8+ cells into the circulation may account for the increased proportion of circulating CD8+CD69+ cells in the CAF trial at pre-exercise, it does not easily explain the more marked increase in the proportion of circulating CD4+CD69+ cells with caffeine ingestion. Furthermore, at 1 h post-exercise the percentage of CD4+ cells expressing CD69 remained markedly above pre-treatment values, although the circulating concentration of CD4+ cells had decreased below pre-treatment values at this time. These findings suggest that any epinephrine-mediated recruitment of cell subpopulations cannot completely explain the observed changes in CD4+ and CD8+ expression of CD69 associated with caffeine ingestion and exercise.
Alternatively, it could also be argued that the recruitment of cells expressing the CD69+ phenotype into the circulation was induced by a stimulus, other than the exercise. For example, an antigen challenge may have occurred prior to, or during, the exercise trials. However, any subjects with symptoms of infection or taking medication during the 4 weeks prior to the study were excluded from the trials, with the aim of reducing the likelihood of this possibility. Furthermore, none of the subjects demonstrated symptoms of infection during the week following the trials, suggesting that the subjects were not incubating an infectious agent during the trials.
A further explanation for the higher percentage of CD4+ and CD8+ cells expressing CD69 in the CAF trial might be that in addition to some influence on the redistribution of cells between the tissues and circulation, caffeine has the ability to induce the activation of CD4+ and CD8+ cells. It could be speculated that this might be via the effect of caffeine on intracellular cAMP concentration since alterations of intracellular cAMP levels have been shown to be involved in the regulation of lymphocyte activation (Grader-Beck et al. 2002; Kammer 1988). Caffeine might modify intracellular levels of cAMP in a number of ways including via catecholamine stimulation of β2-adrenergic receptors (Ganong 1993) or via adenosine receptor antagonism (Greer et al. 2000). Nevertheless, intracellular cAMP levels would need to be determined to lend any support to this speculation. It is also important to acknowledge that the increase in the natural state of activation of CD4+ and CD8+ cells observed here does not necessarily suggest enhanced effector function. These pathways require many other co-stimulatory signals, including specific antigen encounters, without which the cells may enter a state of anergy (Roitt and Delves 2001).
One limitation of the present study was that plasma caffeine levels were not explicitly measured. However, the lower RER values, higher rates of fat oxidation and greater epinephrine and FFA responses in the CAF trial compared with PLA are suggestive of enhanced plasma caffeine levels (Greer et al. 2000; Laurent et al. 2000) and that the dose administered in the present study design was effective in causing altered metabolic and hormonal responses. Furthermore, in a follow-up study, we have since measured serum caffeine concentration in response to the same protocol in a similar group of subjects: Mean serum caffeine concentration was <0.05 μmol l−1 at rest in both trials and increased to ~60 μmol l−1 in the caffeine trial 1 h after ingestion. Serum caffeine concentration remained at this level at completion of the 90 min exercise, before beginning to decline (~40 μM) at 1 h post-exercise. Values remained at <0.05 μM at all sample collection times on the placebo trial (unpublished data). Although not directly linked to the findings of this particular study, these data do provide support for the success of the caffeine supplementation in elevating circulating levels of caffeine in this study.
In conclusion, this study has demonstrated that caffeine compared with placebo ingestion 1 h before a bout of intensive endurance exercise was associated with elevated concentrations of epinephrine before and after exercise and greater perturbations in numbers of circulating lymphocytes, CD4+ and CD8+ cells. Moreover, caffeine ingestion was associated with an increased percentage of CD4+ and CD8+ cells expressing the early activation marker CD69 in vivo before and after exercise. Although these findings suggest that caffeine ingestion prior to intensive exercise influences lymphocyte recruitment and natural state of activation, they now raise the question of whether these effects initiate altered lymphocyte responsiveness to mitogenic and antigenic stimuli both at rest and in response to strenuous endurance exercise.
References
Cannon JG (1993) Exercise and resistance to infection. J Appl Physiol 74:973–981
Dill DB, Costill DL (1974) Calculation of percentage changes in volumes of blood, plasma and red cells in dehydration. J Appl Physiol 37:247–248
DuBose DA, Wenger CB, Flinn SA, Judy TA, Dubovtsev AI, Morehouse DH (2003) Distribution and mitogen response of peripheral blood lymphocytes after exertional heat injury. J Appl Physiol 95:2381–2389
Fink WJ, Costill DL (1995) Analytical methods for the measurement of human performance. Ball State University Press, Indiana, pp 71–72
Forster CD, Macdonald IA (1999) The assay of the catecholamines content of small volumes of human plasma. Biomed Chromatogr 13:209–215
Frayn KN (1983) Calculations of substrate oxidation rates in vivo from gaseous exchange. J Appl Physiol 55:628–634
Gabriel H, Schwarz L, Born P, Kindemann W (1992) Differential mobilisation of leucocyte and lymphocyte subpopulations into the circulation during endurance exercise. Eur J Appl Physiol 65:529–534
Gabriel H, Schmitt B, Urhausen A, Kindermann W (1993) Increased CD45RA+CD45RO+ cells indicate activated T cells after endurance exercise. Med Sci Sports Exerc 25:1352–1357
Ganong WF (1993) Review of medical physiology, 16th edn. Prentice-Hall, London, pp 326
Grader-Beck T, Puijenbroek AAFL van, Nadler LM, Boussiotis VA (2002) cAMP inhibits both Ras and Rap1 activation in primary human T lymphocytes, but only Ras inhibition correlates with blockade of cell cycle progression. Blood 101:998–1006
Graham TE (2001) Caffeine, coffee and ephedrine: impact on exercise performance and metabolism. Can J Appl Physiol 26 [Suppl]: S203–S119
Graham TE, Spriet LL (1995) Metabolic, catecholamine and exercise performances to various doses of caffeine. J Appl Physiol 78:867–874
Graham TE, Helge JW, MacLean DA, Keins B, Richter EA (2000) Caffeine ingestion does not alter carbohydrate of fat metabolism in human skeletal muscle during exercise. J Physiol (Lond) 529:837–847
Gray AB, Telford RD, Collins M, Baker MS, Weidemann MJ (1993) The response of leukocyte subsets and plasma hormones to interval exercise. Med Sci Sports Exerc 25:1252–1258
Green KJ, Rowbottom DG, Mackinnon LT (2003) Acute exercise and T-lymphocyte expression of the early activation marker CD69. Med Sci Sports Exerc 35:582–588
Greer F, Friars D, Graham TE (2000) Comparison of caffeine and theophylline ingestion: exercise metabolism and endurance. J Appl Physiol 89:1837–1844
Kammer GM (1988) The adenylate cyclase-cAMP-protein kinase A pathway and regulation of the immune response. Immunol Today 9:222–229
Kantamala D, Vongsakul M, Satayavivad J (1990) The in vivo and in vitro effects of caffeine on rat immune cell activities: B, T and NK cells. Asian Pac J Allergy Immunol 8:77–82
Laurent D, Schneider KE, Prusacyzk WK, Franklin C, Vogel SM, Krssak M, Petersen KF, Gofrth HW, Shulman GI (2000) Effects of caffeine on muscle glycogen utilization and neuroendocrine axis during exercise. J Clin Endocrinol Metab 85:2170–2175
Maisel AS, Harris T, Rearden CA, Michel MC (1990) β-Adrenergic receptors in lymphocyte subsets after exercise. Circulation 82:2003–2010
McCarthy DA, Dale MM (1988) The leucocytosis of exercise. A review and model. Sports Med 6:333–363
Mueller SN, Jones CM, Smith CM, Heath WR, Carbone FR (2002) Rapid cytotoxic T lymphocyte activation occurs in the draining lymph nodes after cutaneous herpes simplex virus infection as a result of early antigen presentation and not the virus. J Exp Med 195:651–656
Murray DR, Irwin M, Rearden CA, Ziegler M, Motulsky H, Maisel AS (1992) Sympathetic and immune interactions during dynamic exercise: mediation via β2-adrenergic-dependent mechanism. Circulation 86:203–213
Nieman DC, Simandle S, Henson DA, Warren BJ, Suttles J, Davis JM, Buckley KS, Ahle JC, Butterworth DE, Fagoaga OR, Nehlsen-Cannarella SL (1995) Lymphocyte proliferative response to 2.5 hours of running. Int J Sports Med 16:404–408
Pedersen BK, Bruunsgaard H, Klokker M, Kappel M, MacLean DA, Nielsen HB, Rohde T, Ullum H, Zacho M (1997) Exercise-induced immunomodulation—possible roles of neuroendocrine and metabolic factors. Int J Sports Med 18 [Suppl 1]: S2–7
Roitt IM, Delves PJ (2001) Roitt’s Essential immunology, 10th edn. Blackwell Science, Oxford, pp 164–176
Ronsen O, Pedersen BK, Oritsland RT, Bahr R, Kjeldsen-Kragh J (2001) Leukocyte counts and lymphocyte responsiveness associated with repeated bouts of strenuous endurance exercise. J Appl Physiol 91:425–434
Rosenthal LA, Taub DD, Moors MA, Blank KJ (1992) Methylxanthine-induced inhibition of the antigen- and superantigen-specific activation of T and B lymphocytes. Immunopharmacology 24:302–217
Shek PN, Sabiston BH, Buguet A, Radomski MW (1995) Strenuous exercise and immunological changes: a multiple-time-point analysis of leukocyte subsets, CD4/CD8 ratio, immunoglobulin production and NK cell response. Int J Sports Med 16: 466–474
Testi R, D’Ambrosio D, De Maria R, Santoni A (1994) The CD69 receptor: a multipurpose cell-surface trigger for hematopoietic cells. Immunol Today 15:479–483
Ziegler SF, Ramsdell F, Hjerrild KA, Armitage RJ, Grabstein KH, Hennen KB, Farrah T, Fanslow WC, Shevach EM Alderson MR (1993) Molecular characterization of the early activation antigen CD69: a type II membrane glycoprotein related to a family of natural killer cell activation antigens. Eur J Immunol 23:1643–1648
Acknowledgements
We would like to thank Karen Turner and Sujata Dissanayake at the School of Biomedical Sciences, University of Nottingham Medical School for performing the catecholamines analysis.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Bishop, N.C., Fitzgerald, C., Porter, P.J. et al. Effect of caffeine ingestion on lymphocyte counts and subset activation in vivo following strenuous cycling. Eur J Appl Physiol 93, 606–613 (2005). https://doi.org/10.1007/s00421-004-1271-6
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00421-004-1271-6