
Abstract
The purpose of this study was to determine for the first time by repeated non-invasive 13C-NMR spectrometry whether blood lactate concentration affects glycogen reduction in non-exercising muscle during prolonged (6 h) physical exercise in healthy adult males. Such an effect would indirectly show that glycogenolysis independent of nervous activation occurs in non-exercising muscle. After an overnight fast, 12 subjects performed alternating one-leg cycle exercise and arm cranking exercise at an average work load of 106 (SD 26) W [63 (9)% maximum oxygen consumption for one-leg exercise] and 69 (13) W [61 (10)% maximum oxygen consumption for arm cranking exercise], respectively. During the 6-h exercise test, glycogen concentration of the non-exercising calf muscle decreased by 17 (7)% while the glycogen concentration in the exercising calf muscle decreased by 45 (8)%. In a resting control group (n=6), the glycogen concentration did not decrease significantly. The higher the exercise intensity and therefore blood lactate concentration, the smaller was the glycogen reduction in the non-exercising calf muscles. We conclude that during prolonged physical exercise glycogenolysis in non-exercising human muscles decreases as exercise intensity increase contrary to exercising muscles. This observation might be an indirect evidence for a non-exercise induced glycogenolysis in inactive muscles.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Glycogen is an important fuel for physical exercise. Although glycogenolysis and glycogen (gly) synthesis in exercising muscle have been studied intensively, little is known about the influence of physical exercise on the gly stores of non-exercising muscles. In vitro studies have shown that glycogenolysis without nervous activation occurs in epinephrine-perfused, denervated rat muscle (Jones et al. 1994). At present, there is no firm evidence of activation-independent glycogenolysis in humans. Bergström and Hultman (1967) were the first to study muscle gly concentration ([gly]) in exercising as well as in non-exercising human muscle during physical exercise. They concluded: “The glycogen concentration in resting muscle remains unchanged when other muscle groups in the same subject have been emptied of glycogen by exercise”. It is now known that the method of gly determination used by Bergström and Hultman (1967) may underestimate [gly] in muscle (Jansson 1981). Moreover, Bergström and Hultman’s (1967) conclusion conflicts with more recent studies showing that glycogenolysis does occur in non-exercising muscles during physical exercise in animals (Jones et al. 1994; McDermott et al. 1987, 1991) and humans (Bonen et al. 1985; Krssak et al. 2000). It is difficult to prove the absence of nervous activation in non-working muscle during in vivo experiments. Some studies used electromyography (EMG) to show that muscles were not activated (Bonen et al. 1985; McDermott et al. 1987, 1991). However, there is always some activity in human skeletal muscles even when they are not exercising. Therefore, one cannot exclude that the gly loss observed in non-exercising muscle was due to activation in vivo, even though the EMG showed little activity.
What could be responsible for [gly] reduction in non-exercising muscle besides activation-induced glycogenolysis? Unlike the liver, human skeletal muscle lacks the enzyme glucose-6-phosphatase and cannot produce free glucose (glu) from gly (Koolman and Röhm 1996). Some researchers have suggested that lactate (lac) may be released from the non-exercising muscles (Ahlborg 1985; Jones et al. 1994). This seems to be a paradox because the non-exercising muscles are known to take up lac during physical exercise (Ahlborg et al. 1975; Freyschuss and Strandell 1968). On the other hand, lac uptake occurs only at the beginning of exercise. After more than 2 h of exercise, lac uptake of non-exercising muscle is followed by lac release (Ahlborg 1985; Ahlborg and Felig 1982). Thus, the short duration of exercise could be another reason why Bergström and Hultman (1967) did not observe a [gly] reduction in non-exercising human muscle during their 1-h exercise protocol. Physical exercise of more than 1 h with repeated gly measurements is more helpful for investigating the proposed glycogenolysis in non-exercising muscles. Nuclear magnetic resonance (13C-NMR) spectroscopy is the only method that allows repetitive [gly] measurements of the same volume.
If “activation-independent” glycogenolysis in non-exercising muscle breaks gly down to lac, glycogenolysis in non-exercising muscle could be inhibited by high blood [lac]: a high blood [lac] diminishes the lac release from the non-exercising muscles, resulting in a smaller reduction of [gly]. Therefore, we hypothesized that glycogenolysis in non-exercising muscle is dependent on blood [lac]. It was the purpose of this study to determine for the first time non-invasively and repeatedly, whether the reduction of [gly] of non-exercising human skeletal muscle during long-term (6 h) exercise is smaller when blood [lac] is increased.
Methods
Subjects
Twelve subjects [32.0 (SD 5.4) years, 77.1 (7.3) kg, 182 (6) cm] performed the exercise protocol and six subjects [34.8 (8.4) years, 71.5 (6.4) kg, 175 (10) cm] served as controls. Written informed consent was obtained from all subjects after the procedures and potential risks of the study have been explained to them. Subjects were free to withdraw from the study at any time. The ethics committee of the Swiss Federal Institute of Technology in Zurich approved the study. All experiments were in compliance with the laws of Switzerland, where the study was performed.
13C-NMR-spectroscopy
Measurements of [gly] were performed with a 4.7 T 13C-NMR spectrometer (Varian, Palo Alto, Calif.) with a 25-cm bore as described in detail previously (Rico-Sanz et al. 1999). The repetition time was 0.231 s and the acquisition time was 51 ms. To minimize electric noise, 4,096 samples were summed up. The spectrum was phased and baseline corrected. The setting of integral areas was carried out by a standardized macro. For quantification, a 2-l bottle, 15 cm in diameter, containing a solution of 100 mmol l−1 of oyster glycogen was used as phantom. To match the electrical conductivity to that of human muscle tissue at the resonance frequency of the 13C nuclei, the phantom solution was buffered to a pH of 7.2. In comparison to the commonly used method of muscle biopsy sampling, NMR spectroscopy is more advantageous. NMR spectroscopy allows repeated measurements of the same muscle volume. This is in principle not possible with biopsy techniques. An important point for the subjects is that NMR spectrometry does not cause any muscle damage contrary to muscle biopsy sampling. Additionally, 13C-NMR spectroscopy is at least as reliable as muscle biopsy sampling for the determination of [gly] in human skeletal muscles (Taylor et al. 1992).
Exercise and EMG monitoring
Mixed exercise (alternating one-leg cycling exercise and arm cranking exercise) was used because preliminary tests had shown that most subjects could not sustain one-leg cycling or arm cranking alone for more than 3 h. During one-leg cycling, the heel of the resting leg was placed on a platform 25 cm above ground. With this arrangement, only minor calf muscle activity of the resting leg was possible. The activity of the resting calf muscles was monitored by EMG (Biovision, Wehrheim, Germany). A monitor with the EMG signals was shown to the subjects during the whole exercise protocol. This made it possible for the subjects to maintain a foot position, which resulted in almost no activity in the non-exercising calf muscles.
Preliminary test
Maximal workload and the rate of maximum oxygen consumption (V̇O2max) for both types of exercise were determined separately in two preliminary tests [maximum oxygen consumption for one-leg exercise (V̇O2max,one-leg) and maximum oxygen consumption for arm cranking exercise (V̇O2max,arm)]. Both ergometers (ergoline 800, Bitz, Germany) were electrically braked and the workload was independent of the pedaling or cranking rate. Arm cranking exercise started at 30 W, followed by workload increments of 10 W every 2 min. A cranking rate of at least 50 rpm had to be maintained. One-leg exercise started at 50 W, followed by workload increments of 12.5 W every 2 min. Similar to arm cranking exercise, the pedaling rate was at least 50 rpm. The subjects were free to choose the leg with which to exercise. The main test was performed with the same leg as the preliminary test. A spring connected the pedal of the exercising leg to the seat to assist the leg upstroke during exercise. A clipless pedaling system was used.
Main test
Each subject came to the NMR lab at 7:00 a.m. after an overnight fast. Before exercise started, [gly] of the exercising and the non-exercising calf muscle was measured and blood samples of 10 and 20 µl were collected from the ear lobe to determine blood [lac] and blood [glu]. Blood [lac] was determined enzymatically (Biosen 5040, EKF, Hamm, Germany). Blood [glu] was determined photospectrometrically (Dr. Lange Miniphotometer 2, Dr. Lange, Berlin, Germany).
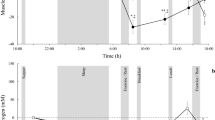
The main test consisted of three similar exercise blocks (Fig. 1). Each block comprised one bout of one-leg cycling and one bout of arm cranking. Each bout lasted 1 h. There was a pause of 5 min between the two bouts of one exercise block. After each exercise block, [gly] of the non-exercising calf was determined, this took about 20 min. After the last bout, [gly] of the exercising calf was also determined. Blood samples to determine [glu] and [lac] were collected after one-leg cycling (n=10) and after arm cranking (n=12) as well as 1 h after the end of exercise. Without complications exercise was finished at 2:40 p.m. The initial workload for both bouts in the first exercise block was between 60 and 80%V̇O2max. Gas exchange was determined with an ergospirometric system (Quark b2, Cosmed, Rome, Italy) during a 5-min period starting in the 45th minute of each bout. Subjects were fasted during the whole test but were encouraged to drink sufficient water. Whenever a subject could not maintain a minimal pedaling or cranking rate of 50 rpm, the workload was decreased by 10 W. This was repeated as often as necessary. If blood [glu] fell below 3 mmol l−1 the main test was terminated before all three exercise blocks were finished. This occurred in three subjects.

Exercise protocol
Control
After an overnight fast, [gly] was also determined in six non-exercising control subjects. During the test period, subjects were fasted and drank only water. Blood [lac], blood [glu], and [gly] in one calf muscle were determined at 7:30 a.m., 12 noon, and 4:30 p.m.
Statistics
Statistics were performed using repeated measures ANOVA, Pearson product moment correlation coefficients, and Fisher’s r to z P values. Statistical significance was set at P<0.05.
Results
Glycogen
Changes of [gly] are defined as Δ[gly]=[gly]after exercise−[gly]before exercise. Values were related to [gly]before exercise. The Δ[gly] value in the non-exercising calf was −17 (SD 7)% (P<0.01, Table 1) while Δ[gly] in the exercising calf was −45 (8)% (P<0.01). Although [gly] in the calf of the control subjects has slightly decreased after 4.5 h, no significant changes were measured after the 9-h resting period (Table 2).
Lac, glu, and exercise intensity
Blood [lac] reached a maximum after the first exercise block (Table 3). After the second and third exercise blocks, blood [lac] was almost unchanged but still significantly higher than resting blood [lac]. One hour after the last exercise bout, blood [lac] had returned to pre-exercise concentrations. Blood [glu] reached a maximum after the first exercise bout and decreased significantly below resting concentrations by the end of exercise (Table 3). Blood [glu] fell significantly during the control test (P<0.05, Table 2). No significant changes in blood [lac] were observed in the control subjects (P>0.05, Table 2).
Correlations
Higher blood [lac] after 6 h of exercise was associated with a lower loss of gly in the non-exercising calf (Fig. 2C), as shown by a significant positive correlation between Δ[gly] in the non-exercising calf muscles and blood [lac]. However, this relationship was not observed after 2 and 4 h of exercise (Fig. 2A, B). A significant positive correlation was also found between exercise intensity and Δ[gly] in the non-exercising muscles after 6 h of exercise (Fig. 3C), i.e. higher exercise intensity was associated with lower Δ[gly] in the non-exercising calf muscles. This correlation also evolved over time (Fig. 3A, B). As expected, the exercising muscles showed a significant negative correlation between exercise intensity and Δ[gly] (Fig. 4), i.e. higher exercise intensity was associated with a greater reduction of [gly]. The same relationship was observed between exercise intensity and blood [lac]: higher exercise intensity was associated with higher blood [lac] (Fig. 5). No significant correlation was found between blood [glu] and Δ[gly] or [lac] (results not shown).

Changes of glycogen concentration (Δ[gly]) during exercise in the non-exercising calf plotted against averaged blood lactate concentration (n=12). A After 2 h of exercise (r=0.28, P>0.05, n.s.), B after 4 h of exercise (r=0.53, P>0.05, n.s.), C after 6 h of exercise (r=0.73, P<0.01)

Values for Δ[gly] during exercise in the non-exercising calf plotted against averaged exercise intensity (n=12). A After 2 h of exercise (r=0.14, P>0.05, n.s.), B after 4 h of exercise (r=0.42, P>0.05, n.s.), C after 6 h of exercise (r=0.73, P<0.05). V̇O2max Maximum rate of oxygen consumption

Values for Δ[gly] in the exercising calf plotted against exercise intensity during 6 h of exercise (n=10, r=0.64, P<0.05)

Relationship between lactate concentration and average exercise intensity during 6 h of exercise (n=12, r=0.71, P<0.05)
Although workloads had to be decreased from each exercise block to the next, the rate of oxygen consumption decreased only during the last arm cranking exercise bout (Table 4). Respiratory gas exchange ratio was always higher during arm cranking exercise compared to one-leg cycle exercise (Table 4).
Discussion
Our results confirm previous observations that glycogenolysis occurs in non-exercising muscle during prolonged physical exercise in humans (Bonen et al. 1985; Krssak et al. 2000). However, it was not clear before the present study whether or not the decrease is due to a small degree of nervous activation. In exercising muscle, high exercise intensity results in high gly utilization (Fig. 4; Bergström and Hultman 1967). If high muscle activity during intensive exercise causes co-activation in the non-exercising muscles and affects by this way the non-exercising muscles despite low EMG activity, the reduction of [gly] in the non-exercising muscles should also increase with the intensity. In other words, a higher exercise intensity would be expected to cause a greater [gly] reduction in non-exercising muscles, reflected in a negative correlation with Δ[gly]. Since we only observe a significant positive correlation between exercise intensity and Δ[gly] in the non-exercising calf muscles, nervous co-activation is unlikely to be a major glycogenolytic stimulus. Nevertheless, there was a trend toward a positive correlation between glycogenolysis and intensity in the non-exercising muscles during the first 2 h of exercise (Fig. 3A). Although no significant correlation was found, we cannot entirely exclude that some nervous activation occurred in the non-exercising muscles during the initial 2 h of exercise. When the workload was reduced after 2 h, the correlation between intensity and [gly] reduction was reversed (Fig. 3B, C). A similar correlation was found between blood [lac] and glycogenolysis in the non-exercising muscles (Fig. 2). This is not surprising as blood [lac] depends on exercise intensity and, in turn, determines the rate of lac release from non-exercising muscle. The positive correlation between [gly] degradation in the non-exercising calf and the blood [lac] is the best—albeit indirect—indication to date for the existence of anaerobic glycogenolysis in non-exercising human muscle in the absence of nervous activation. However, since the greatest [gly] reduction was found after the first 2 h of exercise where exercise intensity was highest, the degree of such glycogenolysis without nervous activation is rather small. During the first 2 h, activation-driven glycogenolysis occurred most likely as discussed above.
If not nervous activation, what else might cause glycogenolysis in non-exercising muscle? The lac producing glycogenolysis in non-exercising muscle may be stimulated by epinephrine. Blood epinephrine concentration increases during prolonged physical exercise (Ahlborg and Felig 1982; Lehmann et al. 1986). Epinephrine is known to stimulate glycogenolysis in exercising human muscle (Febbraio et al. 1998; Fryburg et al. 1995; Spriet et al. 1988; Watt et al. 2001) as well as in non-exercising muscles of rats (McDermott et al. 1987, 1991). The following observation indicates that epinephrine may also drive glycogenolysis in non-exercising human muscle: lac release from non-exercising forearms decreases when β receptors are blocked by propranolol (Ahlborg 1985).
The positive correlation between blood [lac] and Δ[gly] in the non-exercising calf muscles after 6 h is consistent with our hypothesis that gly is converted to lac in non-exercising muscle during prolonged physical exercise: high blood [lac] makes the lac efflux more difficult, resulting in a higher cellular [lac] and a therefore lower rate of [gly] reduction. Low blood [lac] has the opposite effect.
Our results make it obvious that EMG cannot reliably show whether or not glycogenolysis is due to nervous activation. Despite low EMG activity, glycogenolysis driven by nervous co-activation can occur in non-exercising muscle during intensive exercise. We suggest that the correlation between glycogenolysis and intensity (or blood [lac]) may be useful in determining, whether glycogenolysis during prolonged exercise is due to nervous activation (negative correlation) or passive breakdown (positive correlation).
The intercept of the regression line between Δ[gly] of the non-exercising calf muscles and blood [lac] is at about 4 mmol l−1 blood [lac] (Fig. 2). A blood [lac] greater than 4 mmol l−1 could result in an accumulation of gly, as it was observed by McLane and Holloszy (1979) in lac-perfused, non-exercising skeletal muscle of rats. Whether this also occurs in humans, remains to be investigated.
Conclusions
We conclude that during prolonged physical exercise glycogenolysis in non-exercising human muscles decreases as exercise intensity increase contrary to exercising muscles. This observation might be an indirect evidence for a non-exercise induced glycogenolysis in inactive muscles.
References
Ahlborg G (1985) Mechanism for glycogenolysis in nonexercising human muscle during and after exercise. Am J Physiol 248: E540–E545
Ahlborg G, Felig P (1982) Lactate and glucose exchange across the forearm, legs, and splanchnic bed during and after prolonged leg exercise. J Clin Invest 69:45–54
Ahlborg G, Hagenfeldt L, Wahren J (1975) Substrate utilization by the inactive leg during one-leg or arm exercise. J Appl Physiol 39:718–723
Bergström J, Hultman E (1967) A study of the glycogen metabolism during exercise in man. Scand J Clin Lab Invest 198:218–228
Bonen A, Ness GW, Belcastro AN, Kirkby RL (1985) Mild exercise impedes glycogen repletion in muscle. J Appl Physiol 58:1622–1629
Febbraio MA, Lambert DL, Starkie RL, Proietto J, Hargreaves M (1998) Effect of epinephrine on muscle glycogenolysis during exercise in trained men. J Appl Physiol 84:465–470
Freyschuss U, Strandell T (1968) Circulatory adaptation to one- and two-leg exercise in supine position. J Appl Physiol 25:511–515
Fryburg DA, Gelfand RA, Jahn LA, Oliveras D, Sherwin RS, Sacca L, Barrett EJ (1995) Effect of epinephrine on human muscle glucose and protein metabolism. Am J Physiol 268:E55–E59
Jansson E (1981) Acid soluble and insoluble glycogen in human skeletal muscle. Acta Physiol Scand 113:337–340
Jones JP, MacLean PS, Winder WW (1994) Correlation between fructose 2,6-bisphosphate and lactate production in skeletal muscle. J Appl Physiol 76:2169–2176
Koolman J, Röhm K (1996) Color atlas of biochemistry. Georg Thieme, Stuttgart, p 150
Krssak M, Petersen KF, Bergeron R, Price T, Laurent D, Rothman DL, Roden M, Shulman GI (2000) Intramuscular glycogen and intramyocellular lipid utilization during prolonged exercise and recovery in man: A 13C and 1H nuclear magnetic resonance spectroscopy study. J Clin Endocrinol Metab 85:748–754
Lehmann M, Berg A, Keul J (1986) Sex-related differences in free plasma catecholamines in individuals of similar performance ability during graded ergometric exercise. Eur J Appl Physiol 55:54–58
McDermott JC, Elder GCB, Bonen A (1987) Adrenal hormones enhance glycogenolysis in nonexercising muscle during exercise. J Appl Physiol 63:1275–1283
McDermott JC, Elder GCB, Bonen A (1991) Non-exercising muscle metabolism during exercise. Pflugers Arch 418:301–307
McLane JA, Holloszy JO (1979) Glycogen synthesis from lactate in the three types of skeletal muscle. J Biol Chem 254:6548–6553
Rico-Sanz J, Zehnder M, Buchli R, Kühne G, Boutellier U (1999) Noninvasive measurement of muscle high-energy phosphates and glycogen concentrations in elite soccer players by 31P- and 13C-MRS. Med Sci Sports Exerc 31:1580–1586
Spriet LL, Ren JM, Hultman E (1988) Epinephrine infusion enhances muscle glycogenolysis during prolonged electrical stimulation. J Appl Physiol 64:1439–1444
Taylor R, Price TB, Rothman DL, Shulman RG, Shulman GI (1992) Validation of 13C-NMR measurement of human skeletal muscle glycogen by direct biochemical assay of needle biopsy samples. Magn Reson Med 27:13–20
Watt MJ, Howlett, Febbraio MA, Spriet LL, Hargreaves M (2001) Adrenaline increases skeletal muscle glycogenolysis, pyruvate dehydrogenase activation and carbohydrate oxidation during moderate exercise in humans. J Physiol (Lond) 534:269–278
Acknowledgements
We acknowledge the cooperation of the subjects and the great amount of time and sweat they dedicated to the study. We are grateful to Guido Kühne from the Paul Scherrer Institute and Reto Buchli for their technical support before and during this study. We thank the Paul Scherrer Institute for providing the NMR spectrometer. Financial support was provided by Wander AG, Neuenegg, and by the Swiss Federal Institute of Technology (special grant).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kohler, G., Boutellier, U. Glycogen reduction in non-exercising muscle depends on blood lactate concentration. Eur J Appl Physiol 92, 548–554 (2004). https://doi.org/10.1007/s00421-004-1109-2
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00421-004-1109-2