
Abstract
The rhythmic components of heart rate variability (HRV) can be separated and quantitatively assessed by means of power spectral analysis. The powers of high frequency (HF) and low frequency (LF) components of HRV have been shown to estimate cardiac vagal and sympathetic activities. The reliability of these spectral indices, as well as that of LF/HF ratio as a marker of autonomic interaction at rest and during exercise, is briefly reviewed. Modifications in autonomic activities induced by different physiological conditions, e.g. hypoxia exposure, training, and water immersion, have been found in HRV power spectra at rest. The changes in HF and LF powers and in LF/HF ratio observed during exercise have been shown not to reflect the decrease in vagal activity and the activation of sympathetic system occurring at increasing loads. HF peak was recognised in power spectra in the entire range of relative intensity, being responsible for the most part of HR variability at maximal load. LF power did not change during low intensity exercise and decreased to negligible values at medium–high intensity, where sympathetic activity was enhanced. There was no influence from factors such as fitness level, age, hypoxia, and blood distribution. In contrast, a dramatic effect of body position has been suggested by the observation that LF power increased at medium–high intensities when exercising in the supine position. The increased respiratory activity due to exercise would be responsible of HF modulation of HR via a direct mechanical effect. The changes in LF power observed at medium–high intensity might be the expression of the modifications in arterial pressure control mechanisms occurring with exercise. The finding of opposite trends for LF rhythm in supine and sitting exercises suggests that different readjustments might have occurred in relation to different muscular inputs in the two positions.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
"Spontaneous variability of heart rate has been related to three major physiological originating factors: quasi-oscillatory fluctuations thought to arise in blood-pressure control, variable frequency oscillations due to thermal regulation, and respiration; frequency selective analysis of cardiac interbeat interval sequences allows the separate contributions to be isolated." This sentence from the paper "Analysis of heart rate variability" by Sayers (1973) clearly indicates the physiological relevance of the variations of instantaneous heart rate (HR).
Beat-to-beat fluctuations in HR or variations in consecutive R-R intervals are conventionally described with the term HR variability (HRV). During the 1980s the characteristics of the rhythmic fluctuations of cardiovascular parameters, particularly of HR, could be evaluated and quantitatively assessed in numerous physiological and pathological conditions due to the development of automated techniques for measurements, including power spectral analysis.
Three components can be found in HRV power spectrum: (1) a peak at respiratory frequency that corresponds to respiratory sinus arrhythmia (high frequency, HF, >0.15 Hz); (2) a peak centred at about 0.1 Hz that is related to arterial pressure control (low frequency, LF 0.04–0.15 Hz); (3) a component at very low frequency (VLF, <0.04 Hz; sometimes as a peak) considered to be expression of the peripheral vasomotor regulation. The amplitude and to a lesser extent the frequency of the fluctuations have been shown to continuously change as responses of cardiovascular control systems via autonomic nerves. Fluctuations above 0.15 Hz are due to vagal activity only, whereas fluctuations below 0.15 Hz are mediated by both cardiac vagal and sympathetic nerves. Thus, quantitative information on the autonomic control of the heart can be obtained from HRV power spectral analysis related to the separation of the different components in various physiological conditions (see: Saul 1990; Kamath and Fallen 1993; Camm et al 1996).
On this basis, in the late 1980s, our group adopted HRV power spectral analysis as a tool to evaluate the sympathetic and vagal roles in the study of HR control during muscular work. This paper is a brief review of the most relevant results on the topic obtained in the Laboratory of Physiology of the University of Brescia. The reliability of spectral indices in assessing cardiac autonomic activities at rest will be illustrated by few examples of HRV power spectrum distributions in some peculiar physiological conditions. Data of HRV power spectral analysis during muscular work will also be reviewed; these lead to the conclusion that spectral components do not estimate sympatho–vagal interaction during exercise. The changes in HR rhythmic fluctuations, and thus in spectral peaks during exercise, as expressions of the responses of control systems will be discussed.
HRV and autonomic activity at rest
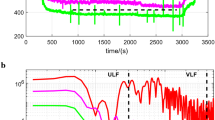
In Fig. 1 (top panels) HRV power spectra are shown for a young subject at rest both in supine and sitting positions. Total power of HRV, i.e. the variance of R-R intervals (thick line), is distributed over the three previously mentioned components: the HF peak is centred at 0.19 Hz , the LF peak at 0.09 Hz, and the VLF component is below 0.04 Hz (no peak; not labelled in the figure). The amplitude of the components is different in the two body positions, in particular, the LF peak is sharper and higher in sitting than in supine position. Large changes in HRV total power can be found in the same subject between different conditions, e.g. body position, and also between subjects. As a consequence, the comparison of spectral components as expressions of responses in control systems is improved by calculating the relative value of each component in proportion to the total power. An increase in LF peak power from 20% to 50% of total power and a decrease in HF peak power from 36% to 12% was found in the subject of Fig. 1 after passing from supine to sitting position. VLF is the remaining power in both positions. These changes in peak powers are the expression of the different contributions of the LF and HF rhythms to HRV in the two body positions via changes in autonomic activities. Agreement exists that the HF peak is a good index of vagal activity (Camm et al. 1996), thus the decrease in HF per cent observed when assuming sitting position reflects the decrease in vagal activity induced by the orthostatic load. More controversial is the interpretation of LF peak power as an expression of sympathetic activity because of the role of both branches in mediating fluctuations below 0.15 Hz. Nevertheless, an increase in LF normalised power has been shown to occur when assuming the upright position, during both tilt and mental stress, i.e. when sympathetic activity is increased (Camm et al. 1996). According to this, the LF increase found in the above example suggests that an increase in sympathetic activity was induced by sitting position. Similar information can be obtained by the ratio between LF and HF powers (LF/HF), as an estimate of the sympatho–vagal interaction (Pagani et al 1986). This ratio increased from 0.4 in supine to 4.1 in sitting position in the subject of Fig. 1, i.e. autonomic interaction shifted toward sympathetic dominance. However, agreement on the concept of autonomic balance or interaction does not exist and criticism can be found in the literature (Eckberg 1997).

The power spectrum distribution of heart rate variability at rest in supine and sitting positions in a young male in control conditions at sea level (top panels) and after 32 days at high altitude [5,050 m above sea level (asl)]. Continuous lines represent total power of HRV in the 0–0.5 Hz range. Spectral components are shown as low frequency [0.04–0.15 Hz; (◫) LF] and high frequency [>0.15 Hz; (■) HF]. The component below 0.04 Hz (very low frequency, (□) VLF) is also shown in control condition power spectra. (Modified from Perini et al. 1996)
In the lower panels of Fig. 1, HRV power spectra are reported for the same subject after a 32-day sojourn at 5,050 m above sea level (asl; Perini et al. 1996). At high altitude, in the supine position, a well-defined LF peak coupled with a reduced HF peak was observed, whereas in sitting position power distribution was similar to that at sea level. However, both LF and HF peaks were less evident as a result of the decreased total power, and the HF peak was shifted to the right of the spectrum. At arrival at high altitude and for the entire 1-month sojourn, LF per cent did not change (mean value 36%) and HF per cent decreased by half (11%) in the supine position, whereas in sitting position both LF and HF per cent had similar values to those at sea level (34% and 6%, respectively). As a consequence, LF/HF ratios were about 2.5 times higher at altitude than at sea level in supine position (4.8 vs 1.7), but they were unchanged in sitting position (6.9). Autonomic spectral indices seem to suggest that hypoxia augmented the sympathetic activity and decreased the vagal activity in supine but not in sitting position. It is of note that similar HR increases in both positions were found at high altitude, and after 1 month HR was still about 12 beats·min−1 higher than at sea level.
The powers of the spectral peaks have not been considered to be direct measures of the activities of autonomic nerves (Kamath and Fallen 1993; Camm et al. 1996), but as suggested by Saul (1990) "it is most appropriate to interpret HR spectral peaks as quantifiers of autonomic responsiveness than autonomic tone". Thus, the decrease in HF per cent and the increase in LF/HF ratio found in supine position by us and by others (Hughson et al 1994) have to be considered as indicative of the shift of the autonomic interaction from the vagal dominance occurring in this position at sea level to the sympathetic dominance induced by hypoxia. On the other hand, as orthostatism per se induces a sympathetic dominance in autonomic interaction, it was hypothesised that no additional effect due to hypoxia could be retrieved in HRV power spectra in sitting position.
Lack of shift in autonomic interaction due to orthostatism has also been shown in elderly subjects whose LF and HF powers and LF/HF ratio did not change after assuming upright or sitting position (Lipsitz et al. 1990; Perini et al. 2000). We observed, however, that VLF power represented more than 50% of total power in subjects over 70 years of age, both in supine and sitting positions. Moreover, in most cases a peak centred at about 0.03 Hz was found. Even though caution must be used in interpreting the VLF component for short recordings, as in our study, the hypothesis has been made that the augmented sympathetic activity occurring with ageing (Lakatta 1993) might have induced the shift of the spectra toward the lowest frequencies (Jasson et al. 1997). As a consequence, the sympathetic dominance occurring in supine position might have prevented the observed change in autonomic interaction after the change in body position in elderly subjects, as has been previously described for hypoxia exposure.
As enhanced vagal tone is expected to be found in trained subjects, HRV power spectra were calculated in a group of professional cyclists [maximum oxygen uptake (V̇O2max) 72.0 (6.4) ml·kg−1 ·min−1] at rest while sitting on the cycle ergometer. These subjects have been compared with a group of age-matched sedentary subjects [V̇O2max: 44.4 (3.4) ml·kg−1·min−1; Baselli et al. 1989]. No significant differences were found in the percentage powers of both LF and HF, even though a tendency for LF power to be lower in cyclists than in sedentary subjects was observed (mean values 34% and 49%, respectively), suggesting a lower level of sympathetic activity. Spectral component powers very simlilar to those found in cyclists have been measured in a group of tri-athletes [V̇O2max 59.9 (2.2) ml·kg−1·min−1; unpublished data]. Thus no clear influence of training on HRV parameters was observed. It cannot be excluded that our results might have been affected by the experimental conditions. While sitting on the cycle ergometer before exercise, as in our protocol, even greater values of LF power have been described in athletes than in sedentary subjects (Bernardi et al. 1990). Moreover, HF power has been shown to be higher in long-distance runners (Dixon et al. 1992) and cyclists (Macor et al. 1996) than in sedentary subjects in supine, but not in upright position (Dixon et al. 1992). Thus, the observed lack of differences between trained and untrained groups might be related to the sitting position, when the effect of training on vagal activity might have been masked by the sympathetic dominance in autonomic interaction. Nevertheless, the modifications in autonomic HR control induced by prolonged and intense training could be detected by the LF/HF ratio. It was significantly lower in cyclists [3.7 (0.7)] and tri-athletes [3.4 (0.6)] than in sedentary subjects [7.6 (3.0)], thus clearly reflecting the differences in sympatho–vagal interaction between the groups.
The relation between physical fitness and/or level of activity has not been completely defined; recently it has been pointed out that "HRV does not appear to be increased in a dose-dependent manner with increasing levels of physical activity" (Melanson 2000). Many discrepancies can be found in the effect of aerobic training programmes on HRV; changes in autonomic indices have been described in some but not in other studies (see references in Melanson 2000 and Perini et al 2002). We recently showed that 8 weeks of aerobic training induced an increase in V̇Opeak (17% on average), a decrease in resting HR and arterial pressures, but no change in HRV parameters in elderly subjects (Perini et al. 2002). Thus an increase in aerobic power per se does not imply modifications in HRV parameters.
Head-out immersion in almost neutral water has been shown to induce a slight decrease in HR and no change in LF and HF powers when compared with the same position in air (Perini et al. 1998), thus suggesting that there is not a major effect of blood distribution on cardiac autonomic activities; however, HRV total power was about three times higher in water than in air. As vagal nerves modulate HR in the entire range of frequencies, the possibility has been suggested that the increased pressure on the body due to immersion might have increased vagal activity via direct and indirect mechanisms, thus leading to enhanced modulation of both LF and HF rhythms.
HRV and autonomic activity during muscular exercise
Autonomic HR control during muscular work has traditionally been studied by means of pharmacological blockade, leading to the conclusion that the increase in HR due to vagal withdrawal is at most 30 beats min−1, while further increments are sustained by enhanced sympathetic activity (Robinson et al. 1966). Our group approached this topic by analysing the time courses of HR and plasma noradrenaline concentration, as expression of sympathetic activity, in the rest–exercise transition of different intensities (Orizio et al. 1988). When the HR kinetic was monoexponential, i.e. up to 30% V̇O2max, no increment in noradrenaline concentration was found, thus indicating that a single mechanism could be responsible for the HR increase, i.e. the vagal withdrawal. In contrast, when a second-order exponential function described the HR increase, significant increments in noradrenaline concentration took place. Moreover, a close relationship was found between the increments in noradrenaline concentration and the increments in HR values due to the slow exponential component. Thus, at medium–high intensity, it has been suggested that the sympathetic drive acted as a second mechanism and overlapped vagal withdrawal to cause the further HR increase up to steady-state values.
HRV spectral analysis is an additional tool used to evaluate the autonomic HR control during exercise. The increase in HR occurring with the increase in metabolic demand has been found to be coupled with the decrease in HRV total power, and thus with the decrease in absolute power of each spectral component, as the result of the reduction in vagal activity during exercise (Arai et al. 1989). The main role of vagal activity in HR modulation was further indicated by the observation that the largest drop in total power, more than 60% of the resting value, occurred within 25–30% V̇O2max (Perini et al. 1990). As previously mentioned this level corresponds to the upper limit for the contribution of vagal activity in HR increase. The largest decrease in HRV total power has been reported to occur during low-intensity exercises in cyclists (Baselli et al. 1989) and elderly males and females (Perini et al. 2000), while supine (Perini et al. 1993) and during water-immersed pedalling (Perini et al. 1998).
HRV power spectra, and thus autonomic spectral indices, have been calculated at steady states of submaximal exercises. In Fig. 2 data from the first study on HRV during exercise by our group (Perini et al. 1990) are reported together with other observations obtained in similar experimental conditions in our laboratory. LF and HF per cent are reported as a function of exercise intensity expressed as a percentage of V̇O2max. LF per cent remained unchanged in the low intensity range, where only a tendency to increase could be observed. Beyond about 30% V̇O2max, there was an almost linear decrease in LF power toward very low values. On the other hand, HF peak was constantly found in HRV power spectra and its power showed a tendency to slightly increase above resting values. As a consequence of these changes in peak powers, the LF/HF ratio did not change significantly during exercise of low–medium intensity and it decreased at the highest loads when compared with rest.

The powers of LF and HF spectral components as a percentage of total power (mean values and SEM) as a function of relative exercise intensity [per cent maximum oxygen uptake (%V̇O 2max )]. Each symbol represents the values observed at steady states of constant load exercises in various groups of sedentary young subjects. The values for a group of professional cyclists (□) are also reported. Symbols to the left of the dotted line represent resting values in sitting position
HF power as spectral vagal index was expected to progressively decrease in the range of intensities examined, particularly from rest to low intensity exercise when HR increase is due mainly to vagal withdrawal. In contrast, HF power was substantially unchanged from rest up to 70% V̇O2max. On the other hand, LF power significantly decreased at medium–high intensities that are known to elicit sympathetic activation. Thus, during exercise, no relation between LF power and sympathetic activity was observed. The consequence was that the LF/HF ratio failed as an estimate of autonomic interaction. The conclusion of this study was that HRV power spectral analysis did not allow us to estimate the autonomic activities during dynamic muscular work.
Other studies have confirmed that HF and LF peaks do not reflect vagal and sympathetic activities during exercise. The persistence of HR fluctuations in the HF bandwidth has been described during moderate exercise (Dixon et al. 1992; Perini et al. 1993; Hagerman et al. 1996) as well as at maximal intensity (Bernardi et al. 1990; Casadei et al. 1995; Perini et al. 1998, 2000). As far as LF peak power is concerned, unchanged values at medium intensity (Kamath et al. 1991; Dixon et al. 1992) and decreased values from medium–high intensity have been reported (Bernardi et al. 1990; Perini et al. 1993; Hagerman et al. 1996). During low intensity tasks, some authors have stated that a shift of autonomic interaction occurred toward sympathetic dominance, as indicated by the reduced HF power with a concomitant increase in LF power and thus an increase in LF/HF ratio (Bernardi et al. 1990; Rimoldi et al. 1992). In both these studies spectral component powers have been expressed in normalised units, nu, i.e. as a percentage of total power after discarding the VLF component (Pagani et al. 1986). The different procedure of normalisation adopted in our studies might explain the discrepant findings at low intensities.
Nevertheless, Casadei et al. (1995) clearly showed that the changes in LF and HF powers during exercise are independent of the unit of measurements and, in agreement with us, they concluded that "the evidence suggests that spectral analysis of R-R interval variability is unable to provide an adequate measurement of sympathetic and parasympathetic activities during exercise". Our group presented the results in more recent studies both in terms of percentage power and nu, further confirming the lack of influence of the normalisation procedure (Perini et al. 1998, 2000).
At high exercise intensity the accuracy of the estimation of spectral components might be affected by the very low total power values. Adopting coarse-graining spectral analysis to overcome this limitation, Yamamoto et al. (1991) claimed that an increase in LF/HF ratio could be observed beyond ventilatory threshold, thus reflecting the high level of sympathetic system activity. However, it is noteworthy that the same authors reported that "at higher intensities the peak at 0.1 Hz disappeared"; this is consistent with the observation of negligible values of LF peak by us and by other authors. The increased ratio reported by Yamamoto et al. (1991) might be attributed to increased power in the lowest frequencies of the spectra. This would be in agreement with the finding of augmented VLF powers at high exercise intensity as the result of the enhanced sympathetic activity (Perini et al. 1990, 1993; Nakamura et al. 1993; Casadei et al. 1995). It has been found that LF peak is shifted to lower frequencies during moderate exercises (Dixon et al. 1992; Perini et al. 1993).
In Fig. 2, LF per cent and HF per cent of the professional cyclists previously mentioned are also reported (open squares). No difference could be seen between the power values observed in the two groups at comparable intensities, thus indicating no effect of training on HR modulation during exercise. Nevertheless, a tendency for HF power to increase was observed in cyclists but not in sedentary subjects during the highest load. The higher relative intensity reached by trained rather than sedentary subjects (80% and 70% V̇O2max, respectively) might explain the augmented HR modulation at respiratory frequency, in agreement with the observation that HF power represents a large part of HRV at high intensity (Bernardi et al. 1990; Casadei et al. 1995).
At the end of exercise, HR returns exponentially to control values. The prompt restoration of vagal tone induces a decrease in HR of 30–35 beats·min−1 observed in the first minute of recovery independent of exercise intensity. The further decrease in HR after medium–high intensity exercises has been ascribed to the progressive decrease of sympathetic activity that has been found to start after about 1 min of recovery (Perini et al. 1989).
HRV spectral analysis showed that autonomic control of HR returned to control conditions within 5 min of recovery from submaximal exercise (Perini et al. 1990). A tendency for LF per cent and HF per cent to be higher and lower than pre-exercise, respectively, has been found only after exercise of medium and high intensity. Nevertheless the finding of a LF/HF ratio 2.5 times higher than at rest after high intensity exercise clearly indicated that sympathetic dominance occurred in autonomic interaction, which is in agreement with the aforementioned observations of a slow return of sympathetic drive to resting level. Similar findings have been reported in the recovery from 50% maximal-load exercise in sedentary subjects (Kamath et al. 1991), and athletes who showed a more complete restoration of peak spectral powers (Dixon et al. 1992). Recently, we observed that 7–8 min were sufficient for the recovery of HRV power distribution in elderly (over 70 years of age) subjects (Perini et al. 2002). When submaximal exercise is prolonged up to 20 min, however, almost 1 h is needed to completely recover cardiac autonomic control (Terziotti et al. 2001). As a whole these data indicate that HRV spectral analysis does estimate the autonomic activity during recovery as well as in resting conditions, due to the return of cardiovascular control mechanisms to pre-exercise conditions.
HR fluctuations as expressions of the responses to muscular exercise
In Fig. 3 mean values (for the sake of clarity, SDs are not shown) of LF and HF per cent are reported as a function of exercise intensity (%V̇O2max) for three groups of subjects. These data have been obtained during incremental cycle exercises up to V̇O2max, thus adding to the previous observations on the effects of exercise on HRV power spectra data in the upper part of the intensity range. Filled circles represent the control conditions for a group of sedentary subjects who have also been evaluated after a 3-week sojourn at high altitude (5,050 m asl, open circles; unpublished results). Filled triangles represent data for subjects whose lower-limb motion was taking place in a horizontal plane (HP pedalling) at right angles with the trunk axis (Perini et al. 1998). It is evident that independent of the experimental condition, LF peak power decreased and finally disappeared from moderate–high exercise intensity. HF peak was recognised in the entire range and an almost linear increase in per cent power, that we had not previously described, was observed beyond 65–70% V̇O2max. These changes in LF and HF powers are comparable in the three groups when allowance is made for minor differences. Thus the modification in HR fluctuations induced by the exercise seemed to be mainly affected by the exercise intensity, thus reflecting specific responses to muscular work.

The powers of LF and HF components as percentages of total power as a function of %V̇O2max. Each symbol represents a group of subjects exercising up to exhaustion: ● sedentary subjects in control conditions and ○ at high altitude (5,050 m asl; 3-week sojourn); ▲ sedentary subjects pedalling with lower limbs motion in a horizontal plane. Symbols to the left of the dotted line represent the resting values in sitting position. For the sake of clarity, mean values only are reported. Values of SEM are comparable for both LF and HF per cent power with those reported in Fig. 3
The LF rhythm has been related to arterial pressure fluctuations via baroreceptor mechanisms (Saul 1990; Camm et al. 1996). The lack of change in LF peak during low-intensity exercise suggests that the 0.1 Hz rhythm is substantially unaffected when cardiovascular adjustment depends mainly on vagal withdrawal. When, however, the activity of the sympathetic system is enhanced as a function of exercise intensity, the modulation of HR at 0.1 Hz is progressively reduced and ultimately disappears. This phenomenon might reflect the modifications in arterial pressure control mechanisms, particularly the reset of baroreflex occurring during muscular work (Rowell and O'Leary 1990). LF decrease occurred at lower intensities for constant-load tasks than for incremental tests (25–30% and 40–45 % V̇O2peak, respectively; see Figs. 2, 3). Inputs from active muscles have been shown to play a main role in cardiocirculatory responses to exercise (O'Leary 1996). Therefore, the different experimental protocol might have influenced both the sympathetic activation and baroreceptor reset, which in turn affected LF rhythm. The tendency of LF to decrease at a slower rate than in control conditions for subjects HP pedalling and those at high altitude could be similarly attributed to the modulating effects of muscular inputs (Rowell and O'Leary 1990).
Similar changes in LF power during exercise have been found in elderly subjects (Perini et al. 2000). The threshold for LF decrease, however, was higher in elderly females than in elderly males [80% vs 40% peak rate of oxygen uptake (V̇O2peak)], probably reflecting the lower sympathetic activity (Seals et al. 1994) and the attenuated baroreflex responsiveness observed in middle-aged and elderly females than in age-matched males (Huikiri et al. 1996). Both these factors might be affected by physical fitness, as suggested by the shift of the level for LF reduction from 60% to 40% V̇O2peak after a training programme in elderly (over 70 years of age) subjects (Perini et al. 2002).
Due to the persistence of the respiratory rhythm during exercise in healthy as well as in heart transplant recipients (Bernardi et al. 1990), it was hypothesised that mechanisms other than neural mechanisms could be involved in respiratory modulation of HR. The mechanical effect of increased respiratory activity has been suggested to be responsible for HF fluctuations during exercise (Bernardi et al. 1990; Casadei et al. 1996). The finding of increased HF powers above 60–65% V̇O2 seems to indicate that this mechanism is particularly relevant at high intensity, where a large increase in pulmonary ventilation occurs. Data at V̇O2max in Fig. 3 show that mean value of HF per cent power was 55 in control conditions and "only" 27 at 5,050 m asl for the same subjects whose V̇O2max decreased from 3,500 ml·min−1 at sea level to 2,250 ml·min−1 at altitude. Moreover, the HP pedalling subjects showed at maximal intensity both V̇O2max and HF per cent very similar to control subjects. Therefore, it can be suggested that the amplitude of HF modulation could be related to the absolute value of V̇O2. This indication is further supported by the observation that elderly males and females showed similar increases in HF per cent power in the common range of metabolic demand; the males, however, reached higher values than the females due to their higher V̇O2 peak (Perini et al. 2000).
The strict relation between HF peak and respiratory activity is demonstrated by the almost linear increase in HF central frequency as a function of exercise intensity (Perini et al. 1990). The slope of the relation seems to be influenced by factors other than metabolic demand. Exercise in supine position (Perini et al. 1993) and in water (Perini et al. 1998) induced a steeper increase in HF central frequency, related to the influence of the experimental conditions on the respiratory activity. When a group of subjects performed the same power output pedalling at different rates, a tendency for HF central frequency to increase more at 100 rpm than at 25 rpm was observed (unpublished results), probably as the result of coupling between the rhythm of the movements and the respiratory rate.
In Fig. 4, data obtained during exercise in water (open circles) and in air in the same position (control; filled circles) are shown (Perini et al. 1998). The powers of LF and HF, expressed in nu, are reported as a function of metabolic demand up to maximum oxygen uptake.

Mean values and SEM of powers of LF and HF components expressed in normalised units as a function of metabolic demand during exercises up to exhaustion in air (●) and head-out water immersion (○). (From Perini et al. 1998)
Exercise in water induced changes in LF and HF powers that were not different to those found in control conditions. The lack of influence of water immersion on the changes in LF rhythm during exercise seems to exclude a main role of blood distribution on HR modulation at 0.1 Hz. On the other hand, both in water and air, HF power decreased from rest to about 2,000 ml·min−1 V̇O2 (corresponding to 55% V̇O2max); thereafter it increased linearly. The similar ventilation observed in the two conditions might justify the comparable value of HF observed at maximal intensity in water and air. However, the different respiratory pattern due to the pressure of water on the chest induced a larger increase in HF central frequency while immersed than when in air, as previously reported.
The effects of body position on HRV power spectra during exercise are illustrated in Fig. 5 (Perini et al. 1993). The meaning of power spectra reported in the higher panels of the figure has been previously commented on in the section on HRV and autonomic activity at rest. When observing the power spectra at the different loads it is clear that an influence of body position on HRV occurred also during exercise. While pedalling in the sitting position, the changes previously described for the LF component could be seen, the peak being lower and enlarged from 50 W to 150 W. The HF peak was consistently apparent, shifting at higher frequencies at increasing loads. In supine position, in contrast, LF peak was well-defined at each intensity and at 150 W it was particularly high and sharp. The changes in HF peak were similar to those found in sitting position. It is of note that at the highest exercise intensity HRV total power was comparable in the two positions. This allows us to state that: (1) the accuracy of the method was maintained at very low values of total power, and (2) the finding of very low LF powers in sitting position only was not due to technical limitations.

Power spectrum distributions of HRV at rest and at steady states of submaximal constant load exercises in supine (left panels) and sitting (right panels) positions in a representative young sedentary subject. Spectral components are shown as low frequency (◫), high frequency (■) and very low frequency (□). Note the different scale of y-axes decreasing with exercise intensity. (From Perini et al. 1993)
When peak powers have been expressed as a function of exercise intensity, no change in LF per cent was observed in either sitting or supine position within 30% V̇O2max, i.e. 50 W in both body positions. This further confirmed that no effect was found on LF modulation at these intensities when cardiovascular responses are mainly driven by vagal withdrawal. In contrast, LF power increased from a mean value of 32% to–54% in supine and decreased to 8% in sitting position in the range between 30% and 70% V̇O2max, i.e. at the intensities where sympathetic activation and major changes in cardiocirculatory control occurred. On the other hand, body position failed to affect HF per cent power; it was similar in both supine and sitting positions at medium–high intensities as a result of comparable metabolic demand and ventilation.
The suggestion that the different blood distribution could explain the diverse trends for LF power in supine and sitting exercises has to be ruled out when the lack of effect of water immersion on LF peak during exercise is taken into account. As a result of the major role of muscular input in cardiocirculatory control at medium–high intensity (O'Leary 1996), it can be hypothesised that baroreceptor mechanisms, and thus HR modulation at 0.1 Hz, could have been modified to different extents in the two positions. Reduced muscle vasodilatation and lower blood flow in leg muscles have been described in supine as compared with sitting exercises at comparable intensities (Folkow et al. 1971). The influence of muscular afferents is reinforced by the observation that a similar large decrease in total power was found during zero intensity exercises in both body positions. This occurred even when HR was significantly increased in supine but unchanged in sitting position.
Further studies are needed to clarify the importance of both mechanical and chemical muscle inputs in HR control during exercise. The simultaneous analysis of both HR and arterial pressure variabilities and their correlation could improve the comprehension of the mechanisms at the basis of the changes in LF rhythm at the different intensities and in the different positions. The few data on arterial pressure variability during exercise show that both variance (Macor et al. 1996; Gonzales-Camarena et al. 2000) and LF nu power (Rimoldi et al. 1992) increase during exercises of low intensity, which suggests augmented vascular sympathetic activity. No data are available on the effect of higher intensity exercises.
In conclusion, quantitative assessment of cardiac autonomic activities can be obtained from HRV power spectral analysis in numerous physiological conditions. Spectral indices, however, fail to reflect the changes in vagal and sympathetic activities occurring during exercise. HR fluctuations during muscular work have to be interpreted as expressions of the re-adjustment of the control mechanisms.
References
Arai Y, Saul JP, Albrecht P, Hartley LH, Lilly LS, Cohen RJ, Colucci WS (1989) Modulation of cardiac autonomic activity during and immediately after exercise. Am J Physiol 256:H132–H141
Baselli G, Cerutti S, Interdonato T, Orizio C, Perini R, Veicsteinas A (1989) Heart rate variability during exercise in sedentary subjects and athletes. In: Proceedings of Computers in Cardiology. IEEE Computer Society, Washington, D.C., pp 319–322
Bernardi L, Salvucci F, Suardi R, Soldà PL, Calciati A, Perini S, Falcone C, Ricciardi L (1990) Evidence for an intrinsic mechanism regulating heart rate variability in the transplanted and in the intact heart during submaximal dynamic exercise? Cardiovasc Res 24:969–981
Camm AJ, Malik M, Bigger JT, Brethardt G, Cerutti S, Cohen RJ, Coumel P, Fallen EL, Kennedy HL, Kleiger RE, Lombardi F, Malliani A, Moss AJ, Rottman JN, Schmidt G, Schwartz PJ, Singer D (1996) Heart rate variability. Standards of measurements, physiological interpretation, and clinical use. Circulation 93:1043–1065
Casadei B, Cochrane S, Johnston J, Conway J, Sleight P (1995) Pitfalls in the interpretation of spectral analysis of the heart rate variability during exercise in humans. Acta Physiol Scand 153:125–131
Casadei B, Moon J, Johnston J, Caiazza A, Sleight P (1996) Is respiratory sinus arrhythmia a good index of cardiac vagal tone in exercise? J Appl Physiol 81:556–564
Dixon EM, Kamath MV, McCartney N, Fallen EL (1992) Neural regulation of heart rate variability in endurance athletes and sedentary controls. Cardiovasc Res 26:713–719
Eckberg DL (1997) Sympatho-vagal balance. A critical appraisal. Circulation 96:3224–3232
Folkow B, Haglund U, Jodal M, Lundgren O (1971) Blood flow in the calf muscle of man during heavy rhythmic exercise. Acta Physiol Scand 81:157–163
Gonzales-Camarena R, Carrasco-Sosa S, Roman-Ramos R, Gaitan-Gonzales MJ, Medina-Banuelos V, Azpiroz-Leehan J (2000) Effect of static and dynamic exercise on heart rate and blood pressure variabilities. Med Sci Sports Exerc 32:1719–1728
Hagerman I, Berglund M, Lorin M, Nowak J, Sylven C (1996) Chaos-related deterministic regulation of heart rate variability in time and frequency domains: effects of autonomic blockade and exercise. Cardiovasc Res 31:410–418
Hughson RL, Yamamoto Y, McCullough RE, Sutton JR, Reeves JT (1994) Sympathetic and parasympathetic indicators of heart rate control at altitude studied by spectral analysis. J Appl Physiol 77:2537–2542
Huikiri HV, Pikkujamsa SM, Airaksinen KEJ, Ikaheimo MJ, Rantala AO, Kauma H, Lilja M, Kesaniemi A (1996) Sex-related differences in autonomic modulation of heart rate in middle-aged subjects. Circulation 94:122–125
Jasson S, Medigue C, Maison-Blanche P, Montano N, Meyer L, Verneiren C, Mansier P, Coumel P, Malliani A, Swynghedauw B (1997) Instant power spectrum analysis of heart rate variability during orthostatic tilt using a time/frequency-domain method. Circulation 96:3521–3526
Kamath MV, Fallen EL (1993) Power spectral analysis of heart rate variability: a non invasive signature of cardiac autonomic function. Crit Rev Biomed Eng 21:245–311
Kamath MV, Fallen EL, McKelvie R (1991) Effects of steady state exercise on the power spectrum of heart rate variability. Med Sci Sports Exerc 23:428–434
Lakatta EG (1993) Cardiovascular regulatory mechanisms in advanced age. Physiol Rev 73:413–467
Lipsitz LA, Mietus J, Moody GB, Goldberger AL (1990) Spectral characteristics of heart rate variability before and during postural tilting. Relation to aging and risk of syncope. Circulation 81:1803–1810
Macor F, Fagard R, Amery A (1996) Power spectral analysis of RR interval and blood pressure short-term variability at rest and during dynamic exercise: comparison between cyclists and controls. Int J Sports Med 17:175–181
Melanson EL (2000) Resting heart rate variability in men varying in habitual physical activity. Med Sci Sports Exerc 32:1894–1901
Nakamura Y, Yamamoto Y, Muraoka I (1993) Autonomic control of heart rate during physical exercise and fractal dimension of heart rate variability. J Appl Physiol 74:875–881
O'Leary DS (1996) Heart rate control during exercise by baroreceptors and skeletal muscle afferents. Med Sci Sports Exerc 28:210–217
Orizio C, Perini R, Comandè A, Castellano M, Beschi M, Veicsteinas A (1988) Plasma catecholamines and heart rate at the beginning of muscular exercise in man. Eur J Appl Physiol 57:644–651
Pagani M, Lombardi F, Guzzetti S, Rimoldi O, Furlan R, Pizzinelli P, Sandrone G, Malfatto G, Dell'Orto S, Piccaluga E, Turiel M, Baselli G, Cerutti S, Malliani A (1986) Power spectral analysis of heart rate and arterial pressure variabilities as a marker of sympatho–vagal interaction in man and conscious dog. Circ Res 59:178–193
Perini R, Orizio C, Comandè A, Castellano M, Beschi M, Veicsteinas A (1989) Plasma norepinephrine and heart rate dynamics during recovery from submaximal exercise in man. Eur J Appl Physiol 58:879–883
Perini R, Orizio C, Baselli G, Cerutti S, Veicsteinas A (1990) The influence of exercise intensity on the power spectrum of heart rate variability. Eur J Appl Physiol 61:143–148
Perini R, Orizio C, Milesi S, Biancardi L, Baselli G, Veicsteinas A (1993) Body position affects the power spectrum of heart rate variability during dynamic exercise. Eur J Appl Physiol 66:207–213
Perini R, Milesi S, Biancardi L, Veicsteinas A (1996) Effects of high altitude acclimatisation on heart rate variability in resting humans. Eur J Appl Physiol 73:521–528
Perini R, Milesi S, Biancardi L, Pendergast DR, Veicsteinas A (1998) Heart rate variability in exercising humans: effect of water immersion. Eur J Appl Physiol 77:326–332
Perini R, Milesi S, Fisher NM, Pendergast DR, Veicsteinas A (2000) Heart rate variability during dynamic exercise in elderly males and females. Eur J Appl Physiol 82:8–15
Perini R, Fisher N, Veicsteinas A, Pendergast DR (2002) Aerobic training and cardiovascular responses at rest and during exercise in older men and women. Med Sci Sports Exerc 34:700–708
Rimoldi O, Furlan R, Pagani MR, Piazza S, Guazzi M, Pagani M, Malliani A (1992) Analysis of neural mechanisms accompanying different intensities of dynamic exercise. Chest 101 [Suppl 5]:226S–230S
Robinson BF, Epstein SE, Beiser GD, Braunwald E (1966) Control of heart rate by the autonomic nervous system. Studies in man on the interrelation between baroreceptor mechanisms and exercise. Circ Res 19:400–411
Rowell LB, O'Leary DS (1990) Reflex control of the circulation during exercise: chemoreflexes and mechanoreflexes. J Appl Physiol 69:407–418
Sayers BM (1973) Analysis of heart rate variability. Ergonomics 16:17–32
Saul JP (1990) Beat-to-beat variations of heart rate reflect modulation of cardiac autonomic outflow. News Physiol Sci 5:32–37
Seals DR, Taylor JA, Ng AV, Esler MD (1994) Exercise and aging: autonomic control of the circulation. Med Sci Sports Exerc 5:568–576
Terziotti P, Schena F, Gulli G, Cevese A (2001) Post-exercise recovery of autonomic cardiovascular control: a study by spectrum and cross-spectrum analysis in humans. Eur J Appl Physiol 84:187–194
Yamamoto Y, Hughson RL, Peterson JC (1991) Autonomic control of heart rate during exercise studied by heart rate variability spectral analysis. J Appl Physiol 71:1136–1142
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Perini, R., Veicsteinas, A. Heart rate variability and autonomic activity at rest and during exercise in various physiological conditions. Eur J Appl Physiol 90, 317–325 (2003). https://doi.org/10.1007/s00421-003-0953-9
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00421-003-0953-9